
Abstract
Background
Fractures are rare events and can occur because of a fall. Fracture counts are distinct from other count data in that these data are positively skewed, inflated by excess zero counts, and events can recur over time. Analytical methods used to assess fracture data and account for these characteristics are limited in the literature.
Methods
Commonly used models for count data include Poisson regression, negative binomial regression, hurdle regression, and zero-inflated regression models. In this paper, we compare four alternative statistical models to fit fracture counts using data from a large UK based clinical trial evaluating the clinical and cost-effectiveness of alternative falls prevention interventions in older people (Prevention of Falls Injury Trial; PreFIT).
Results
The values of Akaike information criterion and Bayesian information criterion, the goodness-of-fit statistics, were the lowest for negative binomial model. The likelihood ratio test of no dispersion in the data showed strong evidence of dispersion (chi-square = 225.68, p-value < 0.001). This indicates that the negative binomial model fits the data better compared to the Poisson regression model. We also compared the standard negative binomial regression and mixed effects negative binomial models. The LR test showed no gain in fitting the data using mixed effects negative binomial model (chi-square = 1.67, p-value = 0.098) compared to standard negative binomial model.
Conclusions
The negative binomial regression model was the most appropriate and optimal fit model for fracture count analyses.
Trial registration
The PreFIT trial was registered as ISRCTN71002650.
Similar content being viewed by others
Introduction
Reducing fractures in older people is a public health priority. Few community-based clinical trials of fracture prevention have been sufficiently powered to show reductions in fractures [1, 2]. Inevitably, sampling participants from the general population means that only a very small proportion of the target population sustain a fracture over the period of observation. For a large UK cluster randomised controlled trial (RCT) (63 general practices, n = 9803 participants) investigating a screen and treat approach offering falls prevention interventions to prevent falls and fractures, we required an appropriate statistical strategy for the trial analyses. The Prevention of Falls Injury Trial (PreFIT) methods and results have been reported in detail elsewhere [2,3,4].
Statistical methods specifically for analysing fracture counts are less common in the literature, compared to methods for the analyses of falls. Fracture data are distinct from other count data for a number of reasons, including: (a) the majority of data are positively skewed with a large proportion of zero events; (b) multiple fractures can occur at one anatomical site at the same time (e.g. hand, foot or rib fractures); (c) fracture events can be recurrent, in that some people can fracture repeatedly over a period of time, and (d) some have multiple injurious falls with multiple fracture events. A Cochrane systematic review of interventions to prevent falls in older people identified 62 trials that had used inappropriate statistical analysis methods to test intervention efficacy [5]. Some trials incorrectly assumed normality for distribution of falls data and used linear regression and t-tests, whereas other trials used analysis of variance. The number of falls or fractures over time are count data, often positively skewed with a large proportion of zeros. There are several recommended methods for analysing count data, namely, Poisson regression, generalised Poisson regression, negative binomial regression, hurdle regression, and zero-inflated regression [6]. However, it is not clear which statistical method works best when count data are positively skewed with a large proportion of zero counts.
Robertson et. al. [7] compared the performance of negative binomial regression with two different survival analysis methods (Andersen-Gill and marginal Cox proportional hazards regressions) using data from two randomised trials testing the Otago home exercise programme to prevent falls. The authors recommended using negative binomial regression to measure the efficacy of fall prevention trials. However, the research team did not compare the performance of negative binomial regression to other methods of analysing count data. The superseded Cochrane systematic review [8] identified that many trials used negative binomial regression to compare the intervention between treatment arms, as recommended by Robertson [7]. Guthrie et. [9] investigated the performance of different statistical methods for skewed counts using genetic data and showed that negative binomial regression performed well compared to the other methods for count data. However, it was unclear how well the negative binomial distribution would perform when data have more than 95% zero counts. In this study, we undertook a secondary analysis to examine the utility of different statistical models that take account of count data, using the example of fracture events. We propose these issues should be considered in future analyses of fracture outcomes in clinical trials.
The paper is organised as follows. We firstly present a brief introduction to Poisson distribution, Poisson regression, negative binomial regression, hurdle and zero-inflated regression models. We then present our analyses using the PreFIT dataset, describing the goodness-of-fit statistics and results for each statistical model. Finally, we discuss the implications of our findings.
Data
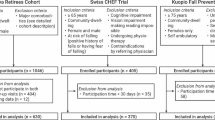
We used anonymised data from a completed, large UK-based, three-arm pragmatic cluster RCT, PreFIT [10]. The aim of the trial was to compare the clinical and cost-effectiveness of three alternative fall prevention interventions: advice only, advice with exercise, and advice with multifactorial falls prevention (MFFP), in adults aged 70 years and older. Sixty-three general practices (total 9803 participants) were randomised into three intervention arms: 21 practices [3223/9803 (33%) participants] to advice only; 21 practices [3279/9803 (33%)] to exercise, and 21 practices [3301/9803 (34%)] to MFFP. The primary outcome was fractures over 18 months, expressed as the fracture rate per person per 100 years [2]. We ascertained fractures using multiple methods, from a) UK National Health Service (NHS) Digital Hospital Episode Statistics (HES) (Admitted Patient Care and Accident and Emergency data); b) general practices using consultation codes, x-ray reports and hospital correspondence; and c) participant self-report collected by postal survey. All fracture events were independently confirmed by a panel of clinicians blinded to treatment allocation.
Overview of analytical approaches
The poisson distribution
The Poisson distribution is commonly used to model the number of events (count data) over a specified period [11]. The Poisson distribution assumes that (i) the probability of an event occurring in a distinct and non-overlapping interval of time is independent of the probability of an event occurring in other intervals, and (ii) the probability of an event occurring in an interval is proportional to the length of the interval [12]. Both the mean and the variance of Poisson distribution are equal to the only parameter of the distribution, which is calculated as the rate of the occurrence of the events.
Poisson, negative binomial, hurdle, and zero-inflated regression models
The Poisson regression, negative binomial regression, hurdle regression, and zero-inflated regression models are generalised linear models widely used to model count data. We briefly discuss the assumption of each of these models (Table 1).
The Poisson regression model assumes that the mean and variance of the outcome are the same [12], which is a very strong assumption and is unlikely to hold in practice. With count data, it is commonly observed that the variance of the outcome is greater than the mean of the outcome, known as over-dispersion. Negative binomial regression is widely used for over-dispersed count data [13, 14]. Sometimes count data contain excess zero counts relative to data from a standard Poisson distribution. For example, the number of GP (general practice) visits for seasonal flu within a population could be inflated by zero counts by those who did not have flu. In such cases, there are two types of zero counts in the data: (i) the number of GP visits is zero (certain zeros) for those who did not have flu and thus did not visit their GP, and (ii) the number of GP visits is zero (sampling zeros) for those who had flu but did not attend their GP. The zero-inflated models are used in such cases. The certain zeros, also known as structural or non-risk zeros, are due to some specific structure in the data as they will always be zero [14, 15]. A logit model is used to predict the probability of these zero counts. Sampling or at-risk zeros, with other positive counts, can be modelled using Poisson or negative binomial regression. The hurdle model assumes that all zeros are structural, that is, certain zero due to some structure of the data, and the positive values are due to sampling [16, 17].
Presence of repeated observations
In a cluster RCT, it is assumed that the observations are more likely to be similar within the same cluster compared to observations in the other clusters [18]. Ignoring such dependencies between the observations in the same cluster will underestimate the standard error of the parameter estimates and, consequently, will result in an inflated type I error rate [19]. One way to account for such intra-cluster dependencies is to include a random effect term into the model, called a mixed effects model. In cohort studies and clinical trials, it is common for participants to have variable follow-up times. In such cases, the natural logarithm of the follow-up periods is included in the model as an offset term to allow us to model counts in proportion to the variable follow-up periods. In clinical trials, individuals or clusters of individuals are randomly allocated to intervention groups. This randomisation ensures that interventions groups are balanced, on average, in terms of baseline covariates. However, this assumption might not be valid with small number of clusters in each group [20]. To account for possible imbalance between the arms, the analysis model is usually adjusted for baseline covariates, which increases the credibility of the trial findings and improves the statistical power [21].
Data Analysis
The Prevention of Falls Injury Trial (PreFIT) dataset
In this post-hoc analysis, we applied the four regression models described in Sect. 3.2 to the PreFIT dataset. As described, the primary outcome was the rate of fractures over the 18 months period per person per time unit. The follow-up periods varied by participant. Table 2 shows the distribution of the number of fractures over 18 months by the three intervention arms. Of the 9803 participants, 9424 (96%) participants had no fractures and 379 (4%) participants had at least one fracture over the 18 month follow-up period. The distribution of the number of fractures across the intervention arms were similar. The mean and variance of the number of fractures were 0.05 and 0.07, respectively, which suggests over dispersion in the data.
People can experience multiple fractures from one fall. Instead of recording the number of fractures associated with each fall, the trial recorded the number of fall-related fracture episodes over the entire follow up period, which represents the total number of times a participant had fractures due to falling. Table 3 shows the distribution of the number of fracture episodes by three intervention arms. We observed that 9424/9803 (96%) participants had zero fracture episodes, 356/9803 (3.6%) participants had a single fracture episode only, and 23/9803 (0.3%) participants had repeated fracture episodes, that is, more than one fracture episode over 18 months follow up. The number of fracture episodes was evenly distributed across the intervention arms. It was not possible to fit a statistical model to compare fracture episodes due to the small number of participants with repeated episodes (n = 23; 0.3%).
Statistical analysis
As discussed in section Poisson, negative binomial, hurdle, and zero-inflated regression models, the zero-inflated model assumes two sources of zeros (structural and sampling) and the hurdle model assumes certain zeros in the data. In the PreFIT dataset, the zero fracture counts were sampling zeros and we, therefore, did not consider zero-inflated and hurdle models although had 96% zero counts in the data.
A series of four models were fitted: Poisson regression, negative binomial regression, mixed effects Poisson regression, and mixed effects negative binomial regression. We included an offset in each of the models to account for variable follow up periods. Models were adjusted for the baseline covariates of age, gender, GP deprivation score, and natural logarithm of baseline falls count. We adjusted for the natural logarithm of baseline falls count because the distribution of baseline falls count was highly skewed and this approach fitted the model better compared to adjusting for baseline falls count. We added 0.5 to the zero baseline falls count for mathematical convenience. To account for the possible dependency among the observations from the same general practice, we included a random effect for general practices in the mixed effects models. The rate ratios (RaRs) with 95% confidence interval (CI) were calculated to compare the effects of the active intervention arms (exercise or MFFP) versus the control arm (advice). The goodness-of-fit of the models was assessed using Akaike information criterion (AIC) and Bayesian information criterion (BIC). Lower values of AIC and BIC indicate a better fit. We also used the likelihood ratio (LR) test to test the following hypotheses: (i) there was no dispersion in the data, that is, there was no gain of using standard negative binomial regression over standard Poisson regression, (ii) the mixed effects Poisson model fitted the data better compared to the standard Poisson model, and (iii) the mixed effects negative binomial model fitted the data better compared to the standard negative binomial model. We used STATA (version 17) to analyse data.
Table 4 presents the goodness of fit statistics, AIC and BIC, for each of the four considered models. The results show that both AIC and BIC values are the lowest for the negative binomial model, which means the negative binomial model fitted the fracture data better compared with the other three models. The LR test of no dispersion in the data showed strong evidence of dispersion (chi-square = 225.68, p-value < 0.001). This indicates that the negative binomial model fitted the data better compared to the Poisson regression model. When we compared the mixed effects Poisson regression model and the standard Poisson regression, the LR test showed strong evidence (chi-square = 11.62, p-value < 0.001) that the mixed-effect Poisson model fitted the data better compared to the standard Poisson model.
Finally, we compared the standard negative binomial regression and mixed effects negative binomial models. The LR test showed no gain in fitting the data using mixed effects negative binomial model (chi-square = 1.67, p-value = 0.098) compared to standard negative binomial model. In addition, the same adjusted AIC and BIC for the standard negative binomial regression model and mixed-effect negative binomial regression model indicated that there was no clustered structured in the data although the data came from a large, multicentre trial. It is important here to note that one should fit mixed-effect negative binomial regression models first over the standard negative binomial model when data are clustered.
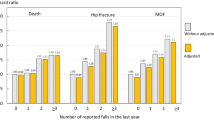
Therefore, the negative binomial regression model was the best fit for the fracture data among the considered possible models based on AIC value and LR test. Table 5 presents the adjusted and unadjusted rate ratios (RaRs) from the negative binomial regression for fractures over 18 months. The advice arm was used as the reference group in the primary analyses for PreFIT. The unadjusted and adjusted fracture RaRs (95% Cis) for the exercise group compared to those randomised to advice were 1.11 (95% CI: 0.84, 1.46) and 1.20 (95% CI: 0.91, 1.59), respectively, indicating a statistically non-significant increase in fracture rate in the exercise group compared to advice only. For the comparison of MFFP with advice only, the unadjusted and adjusted fractures RaRs were 1.27 (95% CI: 0.97, 1.66) and 1.30 (95% CI: 0.99, 1.71), respectively, also indicating a statistically non-significant increase in fracture rate in the MFFP group compared to advice only.
Discussion
We explored the utility of several statistical models to fit fracture counts recorded within a large pragmatic clinical trial. Despite being the largest UK falls prevention trial to date, recruiting almost 10,000 older people and observing outcomes over 18 months, the PreFIT dataset had a low proportion of fall-related fractures overall and thus an excess of zero events. Fracture count data have distinct properties including positively skewed distribution, potential for recurrent fracture events, and multiple fracture events at one or more anatomical sites at time of injury.
We can summarise our findings as follows. Firstly, the zero-inflated and the hurdle models were not eligible to model fracture counts although our data had excess zeros. This is because zero fracture counts equate no fracture whereas zero-inflated models assume two zero generating processes and the hurdle models assumes ‘certain’ zeros. Secondly, based on the goodness-of-fit statistics, the standard Poisson model did not fit the data well. This was because there was data over-dispersion, but the Poisson model ignored this by assuming equality between mean and variance. The negative binomial model fitted the model better compared to the standard Poisson model as it accounted for the over-dispersion. The extended Poisson model and the extended negative binomial model, incorporating a random effect term to account for possible dependence among observations, did not give any gain over standard Poisson and standard negative binomial model, respectively. This suggests that the correlation between the two observations from the same cluster are negligible. Therefore, the negative binomial model fitted the fracture count data in the PreFIT dataset very well.
In our dataset, there were no missing fracture counts due to rigorous data collection using national hospital statistics and GP/radiographic records and triangulation approaches to confirm self-reported and routinely reported fracture events across the whole recruited sample. Therefore, we did not undertake sensitivity analysis. However, in practice, it is common to have missing counts. In such cases, one needs to consider sensitivity analysis under different missingness mechanisms to check the validity of model results. Our findings are based on this sample of community-dwelling older adults recruited from primary care thus may not apply to other clinical studies with much higher fracture event rates e.g. hospitalised or screened osteoporotic populations. We therefore encourage further work to externally validate our models.
In conclusion, after comparing four alternative statistical models for the analyses of fracture counts, we found that the negative binomial regression model was the best model to fit fracture counts with excess zeros within our large trial dataset of over 9000 older people. We recommend that this analytical approach should be considered for future population based studies recording fracture events.
Availability of data and materials
All reasonable requests for data should be sent to the corresponding author. Access to the available anonymised dataset may be granted following review by the research team.
References
Shepstone L, Lenaghan E, Cooper C, Clarke S, et al. Screening in the community to reduce fractures in older women (SCOOP): a randomised controlled trial. Lancet. 2018;391(10122):741–7.
Lamb SE, Bruce J, Hossain A, Ji C, et al. Screening and intervention to prevent falls and fractures in older people. N Engl J Med. 2020;383(19):1848–59.
Bruce J, Lall R, Withers EJ, Finnegan S, et al. A cluster randomised controlled trial of advice, exercise or multifactorial assessment to prevent falls and fractures in community-dwelling older adults: protocol for the prevention of falls injury trial (PreFIT). BMJ Open. 2016;6(1):e009362.
Bruce J, Hossain A, Ji C, et al. Falls and fracture risk screening in primary care: update and validation of a postal screening tool for community dwelling older adults recruited to UK Prevention of Falls Injury Trial (PreFIT). BMC Geriatr. 2023;23:42.
Gillespie LD, Gillespie WJ, Robertson MC, Lamb SE, Cumming RG, Rowe BH. Interventions for preventing falls in elderly people (Cochrane review). The Cochrane Library, Issue 3, 2003.
Cameron AC, Trivedi PK. Regression analysis of count data. Cambridge university press; 2013 May 27.
Robertson M, Clare A, Campbell J, Herbison P. Statistical analysis of efficacy in falls prevention trials. J Gerontol A Biol Sci Med Sci. 2005;60(4):530–4.
Sherrington C, Fairhall NJ, Wallbank GK, Tiedemann A, Michaleff ZA, Howard K, Clemson L, Hopewell S, Lamb SE. Exercise for preventing falls in older people living in the community. Cochrane database of systematic reviews. 2019(1).
Guthrie KA, Gammill HS, Kamper-Jørgensen M, Tjønneland A, Gadi VK, Nelson JL, Leisenring W. Statistical methods for unusual count data: examples from studies of microchimerism. Am J Epidemiol. 2016;21:1–8.
Bruce J, Hossain A, Lall R, Withers EJ, et al. Fall prevention interventions in primary care to reduce falls and fractures in people aged 70 years and over: the PreFIT three-arm cluster RCT. Health Technol Assess. 2021:25:(34):1.
Agresti A, Kateri M. Categorical data analysis. Berlin Heidelberg: Springer; 2011.
Johnson NL, Kemp AW, Kotz S. Univariate discrete distributions. Wiley; 2005.
Hilbe JM. Negative binomial regression. Cambridge University Press; 2011.
Feng CX. A comparison of zero-inflated and hurdle models for modeling zero-inflated count data. J Statistic Distribut Applications. 2021;8(1):8.
Hu MC, Pavlicova M, Nunes EV. Zero-inflated and hurdle models of count data with extra zeros: examples from an HIV-risk reduction intervention trial. Am J Drug Alcohol Abuse. 2011;37(5):367–75.
Lambert D. Zero-inflated Poisson regression, with an application to defects in manufacturing. Technometrics. 1992;34(1):1–4.
Mullahy J. Specification and testing of some modified count data models. J Econometrics. 1986;33(3):341–65.
Campbell MJ, Walters SJ. How to design, analyse and report cluster randomised trials in medicine and health related research. Wiley; 2014.
Hossain A, Diaz-Ordaz K, Bartlett JW. Missing continuous outcomes under covariate dependent missingness in cluster randomised trials. Stat Methods Med Res. 2017;26(3):1543–62.
Hayes RJ, Moulton LH. Cluster randomised trials. CRC Press; 2017.
Hernández AV, Steyerberg EW, Habbema JD. Covariate adjustment in randomized controlled trials with dichotomous outcomes increases statistical power and reduces sample size requirements. J Clin Epidemiol. 2004;57(5):454–60.
Acknowledgements
We thank all participants, trial teams and healthcare practitioners who participated in the original PreFIT trial. I confirm that that all methods were carried out in accordance with relevant guidelines and regulations in the declaration section under the ethical approval and consent to participants.
Funding
This project was funded by the National Institute for Health Research (NIHR) Health Technology Assessment programme as project number 08/14/41. JB and MU are supported by NIHR Research Capability Funding via University Hospitals Coventry and Warwickshire.
Author information
Authors and Affiliations
Contributions
AH and RL conducted the full analysis and drafted the manuscript, which was revised by CJ, JB, MU, and SL. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participants
The National Research Ethics Service approved the PreFIT trial (Research Ethics Committee reference 10/H0401/36, version 3.1, 21 May 2013), which was overseen by a Trial Steering Committee and a Data and Safety Monitoring Committee. Informed, signed consent was obtained from all participants in PreFIT. I confirm that all methods were carried out in accordance with relevant guidelines and regulations in the declaration section under the ethical approval and consent of participants.
Consent for publication
Not applicable as no patient or participate information is published.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hossain, A., Lall, R., Ji, C. et al. Comparison of different statistical models for the analysis of fracture events: findings from the Prevention of Falls Injury Trial (PreFIT). BMC Med Res Methodol 23, 216 (2023). https://doi.org/10.1186/s12874-023-02040-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12874-023-02040-1