
Abstract
Background
Many studies have compared real-world clinical outcomes of immunotherapy in patients with metastatic non-small cell lung cancer (NSCLC) with reported outcomes data from pivotal trials. However, any differences observed could be only limitedly explored further for causation because of the unavailability of individual patient data (IPD) from trial participants. The present study aims to explore the additional benefit of comparison with IPD.
Methods
This study compares progression free survival (PFS) and overall survival (OS) of metastatic NSCLC patients treated with second line nivolumab in real-world clinical practice (n = 141) with IPD from participants in the Checkmate-057 clinical trial (n = 292). Univariate and multivariate Cox proportional hazards models were used to construct HRs for real-world practice versus clinical trial.
Results
Real-world patients were older (64 vs. 61 years), had more often ECOG PS ≥ 2 (5 vs. 0%) and were less often treated with subsequent anti-cancer treatment (28.4 vs. 42.5%) compared to trial patients. The median PFS in real-world patients was longer (3.84 (95%CI: 3.19-5.49) vs 2.30 (2.20-3.50) months) and the OS shorter than in trial participants (8.25 (6.93-13.2) vs. 12.2 (9.90-15.1) months). Adjustment with available patient characteristics, led to a shift in the hazard ratio (HR) for OS, but not for PFS (HRs from 1.13 (0.88-1.44) to 1.07 (0.83-1.38), and from 0.82 (0.66-1.03) to 0.79 (0.63-1.00), respectively).
Conclusions
This study is an example how IPD from both real-world and trial patients can be applied to search for factors that could explain an efficacy-effectiveness gap. Making IPD from clinical trials available to the international research community allows this.
Similar content being viewed by others


Introduction
The treatment landscape of metastatic lung cancer patients has changed over recent years [1]. Chemotherapy used to be the cornerstone therapy for metastatic non-small cell lung cancer (NSCLC) patients, but the introduction of immunotherapy has positively changed the clinical outcomes of these patients [2,3,4]. Immunotherapy is increasingly more prescribed in the Netherlands. The Dutch Lung Cancer Audit showed that immunotherapy-based treatments consisted of 15% of all treatments in 2015 and increased to 57% in 2019 [5].
The phase-III marketing authorization trials researching immunotherapy in NSCLC patients used strict in- and exclusion criteria [4, 6, 7]. Patients treated in real-world practice can differ from these trial patients, leading to different clinical outcomes, also known as the efficacy-effectiveness (EE) gap [8]. Because of the unavailability of individual patient data (IPD) from clinical trials, a common approach for comparing trial and real-world patients is using Kaplan-Meier curves from scientific publications. These are digitized with software, such as DigitizeIt, to allow comparison between trial and real-world patients and to measure the hazard ratio (HR) between the curves [8, 9]. Previous Dutch research on immunotherapy treatment (nivolumab and pembrolizumab) also used this approach and showed differences in clinical outcomes between real-world metastatic NSCLC and trial patients [10]. However, further search for causation, for example, through multivariable regression modeling, was not put forward because of unavailable IPD from the respective trials.
Recently, for one of the pivotal trials involved in the Dutch EE gap study, the IPD have come available. The aim of the present study is to explore if individual patient data (IPD) could be helpful to identify factors that explain divergence between outcomes from the nivolumab treatment arm of the Checkmate-057 clinical trial and patients with NSCLC treated in real-world clinical practice.
Methods
Data sources
This exploratory study is an in-depth study of the study of Cramer-van der Welle et al [10]. The data from that study were re-used. The trial data from the Checkmate-057 trial were collected from the internal ICI database of the Medicines Evaluation Board database.
Patients and outcomes
The population under study consisted of metastatic nonsquamous NSCLC patients treated with second line nivolumab after prior platinum-containing chemotherapy. Real-world patients were treated with nivolumab in the years 2015 to 2018. Participants in the Checkmate-057 clinical trial were treated before marketing authorization [4]. The outcomes in this study were progression-free survival (PFS) and overall survival (OS).
Statistical analyses
Patient- and tumor characteristics of the study population were analyzed using descriptive statistics. These included age, gender, stage, Eastern Cooperative Oncology Group Performance Score (ECOG PS), the presence of brain metastases at diagnosis, tumor histology, and programmed death-ligand 1 (PD-L1) expression. Age was categorized in < 70 and ≥ 70 years, since NSCLC has a median onset at age 70 years [11].
The Kaplan-Meier method with log-rank test was used to compare the PFS and OS between real-world and trial patients. Survival times were calculated from the start of nivolumab treatment (real-world patients) or randomization date (trial patients). Patients not reaching the endpoint at data cut-off were censored at the last known alive date. Median follow-up duration was calculated for the study population using the reverse Kaplan-Meier method [12].
Next, analogous to identification of potential confounders, relative changes in the HR were used to identify factors that could explain the difference between real-world and trial patient outcomes. To do so, univariable and multivariable Cox proportional hazards models were used to construct HRs for real-world practice versus clinical trial patients for both outcomes. All patient- and tumor characteristics (see above) were assessed as potential explanatory factors. Theoretically, variables that result in adjustment of the HR towards 1.00 were considered as potential causative for the EE-gap. Since this study does not compare two different treatments but two groups treated similarly, we argue that the influence of long-term survivors on the proportionality of the Cox model is limited. Statistical analyses were stated significant if the p-value was < 0.05.
Data handling and statistical analyses were performed using the R software system for statistical computing [13] (version 4.1.0.; packages tidyverse, lubridate, tableone, ggplot2, survival, survminer, gtsummary, forestmodel).
Ethical statement
The Santeon Institutional Review Board reviewed and approved the original study and the need for informed consent was waived (SDB219-008). For this secondary analysis, all clinical information was provided anonymously.
Results
Patient characteristics
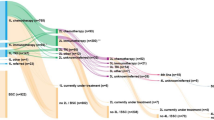
A total of 292 metastatic NSCLC patients were treated with nivolumab in the Checkmate-057 trial and 141 patients in real-world clinical practice. The median follow-up time of the real-world and trial patients was respectively 25.2 (95%CI 22.7-32.6) and 18.6 (95%CI 17.6-20.1) months. Real-world patients were older (64 (44-80) years vs 61 (37-84), p = 0.003) compared to trial patients. Five percent (n = 7) of the real-world patients had an ECOG PS of 2, compared to 0% in trial patients. The trial patients were more often treated with subsequent anti-cancer treatment compared to real-world patients (42.5% vs. 28.4%, p = 0.006). These characteristics are presented in Table 1.
ECOG PS = Eastern Cooperative Oncology Group Performance Score, PD-L1 = Programmed death-ligand 1, RCT = randomized controlled trial.
Progression-free survival
The median PFS of real-world patients was 3.84 (95%CI: 3.19-5.49) months compared to 2.30 (95%CI: 2.20-3.50) months in trial patients (p = 0.104) (Fig. 1). The unadjusted HR for real-world versus trial was 0.82 (95%CI: 0.66-1.03). Patient characteristics associated with PFS were ECOG PS 1 (p = 0.018) and PD-L1 expression > 50% (p < 0.001) (Table 2). The multivariate Cox model, including all patient characteristics, yielded an adjusted HR for real-world versus trials of 0.79 (0.63-1.00) (Fig. 2).

Kaplan-Meier estimate of the progression-free survival (PFS) of metastatic NSCLC patients treated with nivolumab in the clinical trial versus real-world. The progression-free survival time was calculated from randomization date to first progression in clinical trial patients and from start of nivolumab treatment to first progression in real-world patients

Forest plot visualizing multivariate proportional hazard cox regression model of factors associated with the progression-free survival (PFS) of metastatic NSCLC patients
CI = Confidence Interval , ECOG = Eastern Cooperative Oncology Group Performance Score, OR = Odds Ratio. Analysis from the pooled dataset including real-world and clinical trial patients.
Overall survival
The median OS was 8.25 (95%CI: 6.93-13.2) months for real-world patients and 12.2 (95%CI: 9.90-15.1) months for trial patients (p = 0.33) (Fig. 3). ECOG PS 1 (p < 0.001) and ECOG PS 2 (p = 0.001), and PD-L1 expression > 50% (p = 0.001) were significantly associated with OS (Table 3). The unadjusted and fully adjusted HR for real-world versus trials were 1.13 (95%CI: 0.88-1.44) and 1.07 (95%CI: 0.83-1.38), respectively (Fig. 4).

Kaplan-Meier estimate of the overall survival (OS) of metastatic NSCLC patients treated with nivolumab in the clinical trial versus real-world. The overall survival time was calculated from randomization date to death in clinical trial patients and from start of nivolumab treatment to death in real-world patients

visualizing multivariate proportional hazard cox regression model of factors associated with overall survival (OS) of metastatic NSCLC patients
CI = Confidence interval, ECOG = Eastern Cooperative Oncology Group Performance Score, HR = Hazard Ratio. Analysis from the pooled dataset including real-world and clinical trial patients.
Discussion
This study with IPD from both real-world patients and trial participants showed that through the arisen possibility of multivariable modeling potential causative factors for an efficacy-effectiveness gap can be identified. For OS, the HR for real-world versus trials moved to 1.07 (0.83-1.83) after adjustment, suggesting that differences in the available characteristics between the two settings partly explain the altered OS seen in real-world practice. The latter phenomenon was not observed for PFS, suggesting that for that outcome other unmeasured factors are involved.
The median PFS of real-world patients was longer compared to trial patients, resulting in an HR for PFS below 1.00. Although ECOG PS was statistically significant in the multivariate Cox analyses, the adjusted HR between real-world and trial patients did not change. The etiology for this gap in PFS is believed to be multifactorial, with contributing factors including differences in patient populations, healthcare delivery, and variability in the experience of treating health care providers. Multiple factors which could explain differences in patient populations were measured but did not lead to a difference in HR. Unmeasured factors involving PFS could be smoking status, comorbidities, and frailty. Previous research also showed that use of corticosteroids and the number of organs with metastases are associated with PFS [14]. Healthcare delivery was different in terms of response measurement. According to the original Checkmate-057 trial study protocol, response was evaluated in week 9 after nivolumab initiation and every 6 weeks thereafter [15]. In real-world practice, response was assessed every 8 weeks. This led to visible drops in the Kaplan-Meier for PFS of trial patients, while these are less obvious in the real-world PFS (supplement 1). Furthermore, measuring progressive disease using the Response Evaluation Criteria in Solid Tumors (RECIST)- criteria can be less structured and strict in real-world than in trial patients [16]. In clinical practice, the immune responses assigned using RECIST (iRECIST) criteria are used, which include unconfirmed progression [17]. Consequently, conclusions about progressive disease might be delayed in clinical practice what could result in considering possibilities for subsequent systemic treatment later as well. Hypothetically, real-world patients remain treated with nivolumab while with progressive disease, in turn leading to further clinical deterioration reducing the tolerability of subsequent docetaxel, eventually leading to the inverse of the HR for overall survival.
In contrast to PFS, the non-significant difference in OS between real-world and trial shifted towards a null effect after adjustment for the available characteristics in the data (aHR of 1.07 (95%CI, 0.83-1.38)). This suggests that differences in ECOG PS and presence of brain metastases are linked to the observed shorter OS in real-world practice.
Apart from the beforementioned potential, this study also confirms the results using the standard approach of trial and real-world comparison using software applications. The unadjusted calculated HRs for PFS and OS in the study of Cramer-van der Welle et al are identical to the findings of this study using IPD [10].
A strength of our study we consider the quality of the real-world data. Data were manually extracted from electronic healthcare records and with very few missing data. An exception is the PD-L1 expression status which was often missing in real-world (48.9%) since it is not mandatory to measure this before nivolumab treatment in second line. We therefore could not use this factor in the multivariate analyses. Besides this, we could also not test for smoking status that in the Checkmate-057 study was an effect modifier (less effect in never smokers). On the other hand, we expect most patients to be current or past smokers. Altogether, we argue that most of the characteristics with the high prognostic value were included in the analyses [4]. A possible limitation was that the trial data only included PFS and OS calculated from the date of randomization and not from the start of nivolumab treatment as in real-world practice. However, as stated in the RCT protocol, nivolumab treatment should be initiated within three business days after randomization [15]. This very short period is unlikely to affect the outcomes of this study and will not introduce bias in the comparison with the Cramer et al. paper because that study calculated survival times similarly. Finally, we focused in this study on the relative changes in the HR and not on significancy. In case only aggregated trial data are available, a covariate balancing method analogous to propensity score weighting could be used [18].
In the present study we assessed the value of IPD with second line nivolumab, while Cramer-van der Welle et al. also reported a significant impaired OS in real-world with first line pembrolizumab. Unfortunately, due to unavailability of trial IPD on pembrolizumab, we could not assess what the added value of adjustment with IPD would be for that regimen. The European Medicines Agency (EMA) started an initiative to publish clinical trial data submitted to EMA as part of marketing authorization applications [19]. At the moment, trial data on COVID-19 medicines do become publicly available [20]. Hopefully, initiatives from the EMA and others like ClinicalStudyDataRequest.com will help to improve the availability of much more clinical trial data, considering the privacy of patients included in the trial, to allow better identification of factors associated with an efficacy-effectiveness gap (if any), in turn facilitating individualized prognoses and treatment planning [21,22,23].
Conclusion
This study is an example how IPD from both real-world and trial patients can be applied to search for factors that could explain an efficacy-effectiveness gap. Making IPD from clinical trials available to the international research community allows this.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Change history
27 January 2023
A Correction to this paper has been published: https://doi.org/10.1186/s12874-023-01850-7
Abbreviations
- ECOG PS:
-
Eastern Cooperative Oncology Group Performance Score
- EE:
-
Efficacy-effectiveness
- EMA:
-
European Medicines Agency
- HR:
-
Hazard Ratio
- IPD:
-
Individual patient data
- NSCLC:
-
Non-small cell lung cancer
- OS:
-
Overall survival
- PD-L1:
-
Programmed death-ligand 1
- PFS:
-
Progression-free survival
- RCT:
-
Randomized controlled trial
- RECIST:
-
Response Evaluation Criteria in Solid Tumors
References
Yuan M, Huang L, Chen J, Wu J, Xu Q. The emerging treatment landscape of targeted therapy in non- small-cell lung cancer. Signal Transduct Target Ther. 2019. https://doi.org/10.1038/s41392-019-0099-9.
Reck M, Rodriguez-Abreu D, Robinson AG, Hui R, Csöszi T, Fülöp A, et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung Cancer. N Engl J Med. 2016;375:1823–33. https://doi.org/10.1056/NEJMoa1606774.
Gettinger SN, Redman MW, Bazhenova L, Hirsch FR, Mack PC, Schwartz LH, et al. Nivolumab Plus Ipilimumab vs Nivolumab for Previously Treated Patients With Stage IV Squamous Cell Lung Cancer The Lung-MAP S1400I Phase 3 Randomized Clinical Trial JAMA Oncol. 2021;06520. doi:https://doi.org/10.1001/jamaoncol.2021.2209.
Borghaei H, Paz-Ares L, Horn L, Spigel DR, Steins M, Ready NE, et al. Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. N Engl J Med. 2015;373:1627–39. https://doi.org/10.1056/NEJMoa1507643.
Ismail RK, Schramel FMNH, Van DM, Hilarius DL, De BA, Wouters M, et al. Lung Cancer The Dutch Lung Cancer Audit : Nationwide quality of care evaluation of lung cancer patients. 2020;149:68–77. https://doi.org/10.1016/j.lungcan.2020.08.011.
Herbst RS, Baas P, Kim DW, Felip E, Pérez-Gracia JL, Han JY, et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): a randomised controlled trial. Lancet. 2016;387:1540–50. https://doi.org/10.1016/S0140-6736(15)01281-7.
Rittmeyer A, Barlesi F, Waterkamp D, Park K, Ciardiello F, von Pawel J, et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): a phase 3, open-label, multicentre randomised controlled trial. Lancet. 2017;389:255–65. https://doi.org/10.1016/S0140-6736(16)32517-X.
Phillips CM, Parmar A, Guo H, Schwartz D, Isaranuwatchai W, Beca J, et al. Assessing the efficacy-effectiveness gap for cancer therapies: a comparison of overall survival and toxicity between clinical trial and population-based, real-world data for contemporary parenteral cancer therapeutics. Cancer. 2020;126:1717–26. https://doi.org/10.1002/cncr.32697.
DigitizeIt. DigitizeIt n.d. https://www.digitizeit.xyz/ (accessed August 25, 2021).
Cramer-Van Der Welle CM, Peters BJM, Schramel FMNH, Klungel OH, Groen HJM, Van De Garde EMW. Systematic evaluation of the efficacy-effectiveness gap of systemic treatments in metastatic nonsmall cell lung cancer. Eur Respir J. 2018:52. https://doi.org/10.1183/13993003.01100-2018.
Vora N, Reckamp KL. Non-small cell lung Cancer in the elderly: defining treatment options. Semin Oncol. 2008;35:590–6. https://doi.org/10.1053/j.seminoncol.2008.08.009.
Schemper M, Smith TL. A note on quantifying follow-up in studies of failure time. Control Clin Trials. 1996;17:343–6. https://doi.org/10.1016/0197-2456(96)00075-X.
RStudio Team. RStudio: integrated development for R n.d.
Hendriks LEL, Henon C, Auclin E, Mezquita L, Ferrara R, Audigier-valette C. Outcome of patients with non – small cell lung Cancer and brain metastases treated with checkpoint inhibitors. J Thorac Oncol. 2019;14:1244–54. https://doi.org/10.1016/j.jtho.2019.02.009.
BMS. Clinical Protocol CA209057; 2012. https://doi.org/10.1056/NEJMoa1507643.
Feinberg BA, Zettler ME, Klink AJ, Lee CH, Gajra A, Kish JK, et al. Comparison of solid tumor treatment response observed in clinical practice with response reported in clinical trials. JAMA Netw Open. 2021;4:2–11. https://doi.org/10.1001/jamanetworkopen.2020.36741.
Seymour L, Bogaerts J, Perrone A, Ford R, Schwartz LH, Mandrekar S, et al. iRECIST: guidelines for response criteria for use in trials testing immunotherapeutics. Lancet Oncol. 2017;18:e143–52. https://doi.org/10.1016/S1470-2045(17)30074-8.
Tan K, Bryan J, Segal B, Bellomo L, Nussbaum N, Tucker M, et al. Emulating control arms for Cancer clinical trials using external cohorts created from electronic health record-derived real-world data. Clin Pharmacol Ther. 2022;111:168–78. https://doi.org/10.1002/cpt.2351.
European Medicines Agency (EMA). Clinical data publication n.d. https://ema.europe.eu/en/human-regulatory/marketing-authorisation/clinical-data-publication (accessed 7 Sept 2021).
European Medicines Agency (EMA). Online access to clinical data for medicinal products for human use n.d. https://clinicaldata.ema.europa.eu/web/cdp (accessed 7 Sept 2021).
ClinicalStudyDataRequest.com n.d. https://www.clinicalstudydatarequest.com/ (accessed 17 Aug 2021).
Kuntz RE, Antman EM, Califf RM, Ingelfinger JR, Krumholz HM, Ommaya A, et al. Individual patient-level data sharing for continuous learning: a strategy for trial data sharing. NAM Perspect. 2019. https://doi.org/10.31478/201906b.
Tucker K, Branson J, Dilleen M, Hollis S, Loughlin P, Nixon MJ, et al. Protecting patient privacy when sharing patient-level data from clinical trials. BMC Med Res Methodol. 2016;16. https://doi.org/10.1186/s12874-016-0169-4.
Acknowledgements
Not applicable.
Funding
This study was not funded.
Author information
Authors and Affiliations
Contributions
RI: Conception and design study, data acquisition, data analysis and interpretation of data, drafting the article, revising critically for important intellectual content. FS: Interpretation of data, revising the article critically for important intellectual content, Final approval of the version to be submitted. MvD: Interpretation of data, revising the article critically for important intellectual content, Final approval of the version to be submitted. AP: Interpretation of data, revising the article critically for important intellectual content, Final approval of the version to be submitted. CC: Data acquisition, revising the article critically for important intellectual content, Final approval of the version to be submitted. DH: Interpretation of data, revising the article critically for important intellectual content, Final approval of the version to be submitted. AdB: Interpretation of data, revising the article critically for important intellectual content, Final approval of the version to be submitted. MW: Interpretation of data, revising the article critically for important intellectual content, Final approval of the version to be submitted. EvdG: Conception and design study, interpretation of data, revising the article critically for important intellectual content, Final approval of the version to be submitted.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study reuses observational data from a previous study. There were no experiments on humans and/or human tissue samples. All methods were carried out in accordance with relevant guidelines and regulations. The original study was reviewed and approved by the Santeon institutional review board, and all clinical information was provided anonymously, and informed consent was waived (SDB219-008) by this review board.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised: the authors requested to correct the word “first-line” to “second-line” in the article title.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ismail, R.K., Schramel, F.M.N.H., van Dartel, M. et al. Individual patient data to allow a more elaborated comparison of trial results with real-world outcomes from second-line immunotherapy in NSCLC. BMC Med Res Methodol 23, 1 (2023). https://doi.org/10.1186/s12874-022-01760-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12874-022-01760-0