
Abstract
Background
The present study examines the psychometric properties of the German adaptation of the Client Attachment to Therapist Scale (CATS). The validity of the scale as originally proposed has recently been brought into question, as patients were identified as “pseudosecure”.
Methods
We examined the measure’s factorial structure, as well as reliability and validity towards related measures using a clinical sample of N = 354 participants.
Results
We found the original model, consisting of 36 items to be lacking in terms of model fit and construct validity. A shortened 12-item version exhibited markedly improved model fit and reliability. Correlations to related constructs demonstrated that none of the scale’s validity was lost by shortening it. Furthermore, we showed scalar invariance across groups of age and sex.
Conclusions
The shortened CATS-S can be recommended for future use in clinical research in German-speaking populations as a valid, reliable, and economical alternative to the longer version.
Similar content being viewed by others

Background
Bowlby [1], postulated that the psychotherapeutic relationship resembles a behavioral repertoire comparable to attachment, providing a possible explanation of the expectations and behaviors displayed by clients in the therapeutic setting. As in a parental or primary caregiver relationship, the psychotherapist provides emotional support and regulation, accessibility, comfort, sympathy, and a “secure base” promotion explorative behaviors [2]. Therefore, nourishing a therapeutic relationship can be understood as certain form of adult attachment, which is mostly coined by past relationships experiences in the client’s childhood [1]. Hence, attachment theory models foster understanding in therapeutic environments.
Although a large body of literature has used concepts of attachment theory in psychotherapy research [3,4,5,6], the therapeutic relationship was rarely conceptualized from an attachment perspective. Subscales of existing measures—for example, the “bond” subscale of the Working Alliance Inventory (WAI) [7] — capture only one aspect of this attachment relationship. Therefore, important components of the attachment theory are missing, such as clients’ feelings and attitudes toward the counselor from an attachment perspective. Furthermore, the clients’ capacity to form positive, secure attachments towards their therapists [8], the quality of the working alliance [9], the level of basic social competencies [5, 10], and clients’ secure and insecure attachment representation [1] should be assessed.
Therefore, the Client Attachment to Therapist Scale (CATS) was developed. To this end, nine experienced therapists generated items based on the description of the behavior displayed by infants of secure, ambivalent, and avoidant attachment described by Ainsworth and her colleagues [11]. The panel generated a total of 272 items. After removing redundant items and changing the wording to minimize response set bias, the initial version of the CATS contained 100 items with a 6-point response scale. After pretesting, a factor analysis based on n = 138 patients revealed one large factor, which captured client perceptions of secure attachment and two smaller factors, which captured more troubled attachments to the therapist. The subscales (Secure, Avoidant-Fearful and Preoccupied-Merger) demonstrated acceptable internal and retest reliability (α > .72; r > .63).
Clients with high scores in the CATS Secure subscale viewed their therapists as emotionally available, supportive, and encouraging exploration of an uncomfortable emotional experiences [1]. These types of clients are prone to record a positive working alliance, good object-relations capacity, and a relatively solid perception of self-efficacy. Clients with elevated scores on the CATS Preoccupied-Merger subscale, long for boundaryless affiliation to the therapist and wish a deeper and intense relationship. These clients are also characterized by a constant rumination on their therapist and are highly compliant in terms of depending on others. The relationship of the CATS Preoccupied-Merger subscale with the working alliance implies attachment to the therapists, even without a dialectical goal settlement between client and therapist. Clients who scored high on the CATS Avoidant-Fearful subscale tend to mistrust their therapists, avoided rejection, and were not compliant in open up to their therapists. Clients who scored high on the CATS Avoidant-Fearful subscale exhibited the weakest working alliances and object-relations shortcomings.
For differential validity, the CATS was applied together with social competencies, social support, and personality questionnaires [12, 13]. Furthermore, in various psychotherapy studies the CATS was used to specify the effect of the client attachment to therapist onto transference [14], depth in session [15], interpersonal process [13], WAI, and outcome [16,17,18]. In addition, the premature termination [19], session impact [4], emotion, and mood awareness [20] could be predicted by the client attachment to therapist (CATS). Recent studies also showed the influence of the therapist’s attachment and the clients’ attachment to therapist onto WAI and session exploration [21,22,23,24,25,26].
Even though the CATS was psychometrically investigated, the factorial structure of the CATS has not been yet investigated by a confirmatory factor analysis. This is of special importance since, patients were recently identified as pseudosecure attached patients [27]. Patients with pseudosecure and secure attachment to the therapist present some similar features in the early sessions such as: easily bonding, readiness to self-disclose, regard their therapist in strongly positive terms, and place high value on the therapeutic relationship [27]. The crucial difference is that patients with a pseudosecurity pattern idealize their therapist and are highly dependent of him or her. This might be explicable by the high intercorrelation between the clients’ secure attachment to the therapist (CATS-Secure) with the clients’ avoidant attachment (CATS-Avoidant-Fearful; r = −.693, p < .001). Hence, one of our aims was to identify clearly separable factors and provide a clear-cut illustration of the three-factor structure of the CATS. For this aim, the German adaptation of the original scale was implemented [24]. Such was previously translated by experts from English into German according to common translation guidelines [25,26,27,28]. Nevertheless, the psychometric properties were not primary focus of the past investigation [24]. Therefore, a further aim of the present study is to evaluate the psychometric properties of the scale and if required optimize them based on a large sample. Especially in clinical research, in which patients do not feel well, long questionnaires with 36 items such as the CATS might be a tiring and a more economic version would be highly appreciated. Consequently, the need of shorter scale in this research field may be a practical contribution for patients and therapists.
Methods
In order to ensure the quality of the analyses, two samples were collected at two different timepoints. Thus, in the first study (Study 1), the psychometric properties of the translated scale were piloted (Sample 1). With the purpose of confirmatory validation, a second study (Study 2) was conducted to evaluate the final scale (Sample 2). The results of each study are reported in the respective results section.
Participants
The attachment representations of patients in a naturalistic inpatient were assessed. Similar to instructions given to the participants in the original CATS development study, all clients in both of our samples were reassured their therapist would never have access to ratings of their therapeutic relationship. The study was approved by the ethics committee of [masked for review] (Code of ethics: 112052007). In general, the average duration of treatment was 64.05 calendar days (SD = 28.54). In addition to a daily group therapy session with their primary therapist, patients also saw their primary therapist for individual focal therapy twice a week for 50 min. As a result, the contact with their primary therapists was intensified. The other members of the therapeutic team had patient contacts lasting merely 10 to 15 min. The psychotherapists who were asked to take part in our study had a professional background with a psychological or medical education with an additional license for practicing psychotherapeutic treatment.
In Study 1 (Sample 1 = N = 433), 79 participants were excluded due to missing data, leading to a total sample size of N = 354. Thirty-one participants in this sample had missing values of no more than three items in a scale. We substituted those missing values with the item mean. The imputation via mean values was carried out on a per-person-basis. Thus, the personal characteristics of each participant have been taken into account. Sample 2 (N = 306), no missing values were identified. The ICD-10 diagnoses confirmed by SCID [29, 30] were in Sample 1 mostly affective (F30–39; 114/32%) followed by anxiety disorders (F40-F41; 55/16%), adjustment/stress disorders (F43; 37/10%), and somatoform disorders (F45; 35/10%). In Sample 2 (N = 306), most of the diagnoses were mental, behavioral and neurodevelopmental (F01-F99; 98/32%) followed by factors influencing health status and contact with health services (Z00-Z99; 27/8.8%). The majority of the mental disorders were related to anxiety, dissociative, stress-related, somatoform and other nonpsychotic mental disorders (F40-F4; 15/5.0%), followed by mental and behavioral disorders due to psychoactive substance use (F10-F19; 10/3.3%) as well as behavioral syndromes associated with physiological disturbances and physical factors (F50-F59; 7/2.2%). The general symptom severity at admission was quite high (SCL-90-R-GSI T value at admission was M = 69.98; SD = 11.35) and had significantly decreased at discharge, even though the level was still high (M = 61.89, SD = 13.70) (t = 13.36, df = 335, p < .001; d = .65). Depression symptoms were also quite pronounced (BDI-score at admission was M = 26.61; SD = 12.36) and significantly decreased at the end of therapy (M = 16.60, SD = 12.72; t = 15.95, df = 285, p < .001; d = .79). The sociodemographic data of the participants is reported in Table 1.
Measures
For the study at hand (Study 1,2) we implemented the German-versions of each of the following measures.
A German adaptation of the Client Attachment to Therapist Scale (CATS) [5], was applied to analyze the patients’ feelings and expectations toward their therapist from an attachment point of view. The CATS encompass 36 items arranged in three sub-scales: the Secure sub-scale (14 items: e.g., ‘my counselor is dependable’), the Avoidant-Fearful sub-scale (12 items: ‘I don’t like to share my feelings with my counselor’), and the Preoccupied-Merger sub-scale (10 items: ‘I think I am my counselor’s favorite client’). High avoidance mirrors the patients’ distrust towards the therapist and disagreement whereby patients are not compliant in opening up and feel uncomfortable and disgusted when speaking in therapy. High preoccupation reflects the patient’s thoughts about the therapist and the desire for a closer the therapeutic relationship. Patients answer on a six-point-scale from strongly agree (1) to strongly disagree (6). The evidence of validity was evinced by significant correlations of the CATS sub-scale scores with scales of adult attachment, working alliance, and object relations. The internal reliabilities (Cronbach’s Alpha) for the Secure, Avoidant–Fearful and Preoccupied-Merger sub-scales were .78, .83, and .82, respectively [5]. In the current sample, the internal reliabilities (Cronbach’s Alpha) for the sub-scales ranged from .73 to .81. The characteristics of the CATS items and scales are displayed in Table 2.
The original CATS was translated by experts into German according to the translation guidelines based on the WHO protocol of translation and adaption of instruments (e.g., forward and back translation, pre-testing and final version) [28] which is in line with the procedure of translation, back-translation, and verification of suggested protocols in the past [25,26,27].
Psychological distress was evaluated with the German version of the Symptom Check List (SCL-90-R) [31] at the time of admission and at termination of therapy. The global severity index (GSI) of the Symptom Check List was applied as a main outcome measure from the patients’ point of view. The GSI measures general symptom distress; its reliability and validity have been shown in numerous studies. A German validation study replicated the scale’s high internal consistency of .94 to .98 and a high retest-reliability of .79 to .90 [32].
The Bielefeld Client Expectations Questionnaire (BFCE) [33] evaluates the expectations of the patients towards the therapist. The scale covers the following dimensions: Fear of Rejection, Readiness for Self-Disclosure, and Conscious Need for Care, conveyed in 11 and 10 items, accordingly. A 5-point scale ranging from (0) = “does not apply at all” to (4) = “does fully apply”. The internal consistency is respectable (α = .83–.84) [33].
The German version of the Helping Alliance Questionnaire (HAQ) [34, 35] was implemented to assess the quality of the therapeutic relationship by 22 Items, which reflect the two factors relationship satisfaction and outcome satisfaction from the patient and the therapist point of view. Answer options range from (1) = “I strongly feel it is not true.” to (6) = “I strongly feel it is true.” Reliability coefficients are α = .89 for relationship satisfaction and α = .84 for outcome satisfaction [35]. An overview of the scales in provided in Table 3.
Procedure
In both studies, the patients were instructed about the aim of the research project and about the data policies of the study (e.g., confidentiality clause). The participants were assured that neither their primary therapist nor third parties could have access to their submitted data. After submitting their informed consent for participation, the patients were included in the study. Thereafter, they filled out routine assessment questionnaires of symptoms at the beginning and the end of the treatment. To that end, participants were told to refer to their primary therapist when answering the CATS. At the end of the psychotherapeutic intervention (Sample 1,2: after approximately 63 days, 12 sessions), they filled out the German adaptation of the Client Attachment to Therapist (CATS) questionnaire.
Statistical analyses
We computed the statistical analysis using R and the packages EFAutilities, lavaan, paran, semTools, and stuart [36,37,38,39,40]. We employed an α level of .05 for tests of significance, unless noted otherwise. Our hypotheses and data-analytical plan were specified a priori. For the exploratory factor analysis (EFA), we first conducted parallel analysis (PA) [41] to establish the number of components in the data by comparing the empirical eigenvalues to those of randomly generated data sets with the same general properties. Subsequently, we applied different methods for item reduction and model generation. For these calculations, we conducted an EFA applying ordinary least squares extraction and oblique rotation. Thereafter, the item descriptive statistics were examined. Items with the following characteristics were discarded: loadings smaller than .500, cross-loadings higher than .250, item-total correlations smaller than .500, or absolute skewness and excessive kurtosis values larger than 2 or 4, respectively [42, 43], or multiple of the above-mentioned criteria. Next, we used stuart to further shorten the model and tested it in the confirmatory Sample 2. Stuart works with ant colony optimization to generate and evaluate subsets of a scale and maximize model fit. For this procedure we chose models with four items per scale. For validity purposes, we conducted Person Product Moment correlations between the CATS-S subscales and related psychological constructs (Table 8), as described in the section measures.
In Study 2, we computed a confirmatory factor analysis (CFA) with the robust weighted least square method (WLSMV in lavaan) [44]. To evaluate the model fit, we used the commonly recommended indices and cutoff values [45,46,47,48]: The χ2-statistic should ideally not be significant, but this is unlikely with larger samples [49]. The comparative fit index (CFI) should be higher than .95 for a model to be acceptable, while values higher than .97 indicate particularly good fit. Similar criteria are generally applied for the Tucker Lewis index (TLI), although this index is always lower than the CFI. The root mean square error of approximation (RMSEA) and its 90% confidence interval should be lower than .08, while values lower than .05 suggest good fit. The standardized root mean square residual (SRMR) is evaluated by similar standards as the RMSEA.
Finally, we investigated measurement invariance across age and sex groups by applying a multigroup analysis with theta parameterization. We divided participants into age groups of comparable sizes (≤39, 40–59, ≥59). For the analysis of invariance, we applied the χ2-test, the CFI, and the RMSEA. We treated a deviation of more than .01 in CFI and .015 in RMSEA between models as a sign that a measure is not invariant across the groups [50, 51]. Since the factor analysis method we employed treats our items as ordinal, we tested the following levels of invariance: configural (or pattern invariance, i.e., the number of factors and pattern of loadings is equal for both groups), metric (or weak; i.e., additionally the same magnitude of factor loadings across groups), threshold invariance (additionally the thresholds in the assumed latent response distribution are set to be equal across groups), and finally scalar invariance (or strong; additionally, the item intercepts are equated across groups). Finally, we used ω as a measure of factor score reliability [52].
Results
Item characteristics
Table 2 shows descriptive statistics such as means, standard deviations, along with values for skewness, and kurtosis for all CATS items, and its three scales. Furthermore, corrected item-total correlations are reported. As indicated by item difficulty indices and skewness values, the items of the secure-scale were evaluated in a positive manner (P = .39 to P = .69), whereas most participants disagreed with the statements proposed in the avoidant-fearful-scale (P = .25 to P = .53) and the preoccupied-merger-scale (P = .20 to P = .47). Internal consistency coefficients indicated good reliability for all three scales (ωsecure = .81; ωavoidant-fearful = .75; ωpreoccupied-merger = .86). The final scale is illustrated in Table 4.
Factor structure
In the initial PA, the empirical eigenvalues for the first three components were larger than the 95% confidence interval of the randomly generated ones (Table 5). Hence, it was confirmed that a three component should be extracted from the original matrix. We reported the factor loadings of the subsequent EFA in Table 2. Upon examination, the three-factor structure became evident.
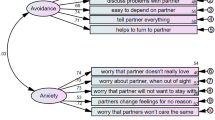
In Sample 1, the original model proposed by Mallinckrodt and colleagues [5] had moderate to unacceptable fit (see Table 6), which led us to seek for a better fitting model. To this end, we shortened the model based on item characteristics, as previously explained in the section of statical analyses. Items with low loadings (i.e., 7, 14, 17, 21, 24, 26, 31, 32, 36) and cross-loadings higher than .25 (i.e., 8,12) were excluded. In addition, items with item total correlation lower than .50 were discarded too (i.e., 7, 14, 22, 23, 26, 31, 32, 36) [42]. Finally, we used stuart on the remaining items. Among the possible 47,250 combinations, the algorithm selected the most suitable as indicated in Table 2. The aforementioned configuration was tested in Sample 2, showing excellent fit (Table 6). Correlations between the latent variables were small to moderate: rsecure, avoidant-fearful = −.363, p = .002, rsecure, preoccupied-merger = .232, p = .002, ravoidant-fearful, preoccupied-merger = .164, p = .043.
Measurement invariance
To ensure the comparability of test results across different demographic groups, we computed measurement invariance across sex and age groups in the confirmatory sample (Study 2). As reported in Table 7, there is evidence for metric, threshold, and scalar factorial invariance across sexes. For age groups, we could also confirm metric and scalar invariance, but with regard to item response thresholds deviated slightly in terms of Δχ2 and ΔCFI, indicating non-equivalence for at least some of the thresholds. In contrast, a very low ΔRMSEA indicated invariance. By releasing equality constraints for the thresholds of Items 15 (“I think my counselor disapproves of me.”) and 18 (“I don’t like to share my feelings with my counselor.”), partial threshold invariance was attained.
Validity
Convergent and discriminant validity were investigated using the HAQ, the BFKE, and the SCL-90. Zero-order correlations are reported in Table 8. To compare the predictive validity of the short scales to that of the original scales, we tested the correlations towards relevant constructs for significant differences. For the secure-scales, differences in r were never larger than .04, zs ≤ .53, ps ≥ .298. The avoidant-fearful-subscales differed with regard to their associations with two subscales: Patient-HAQ “relationship-satisfaction” (Δr = .10, z = 1.752, p = .040) and BFCE “Readiness for Self-Disclosure” (Δr = .12, z = 1.672, p = .047). These differences in r correspond to a d of .20 and .24, respectively, which are commonly interpreted as small effects. There were again no significant differences between correlations for the preoccupied-merger scales, Δr ≤ .08, zs ≤ 1.08, ps ≥ .14. It should also be mentioned that the secure- and the avoidant-fearful-scale are correlated at r = −.56, compared to r = −.71 for the original CATS; Δr = .15, z = 3.37, p < .001, d = .30.
Discussion
The CATS is widely used in psychotherapeutic research. However, the psychometric structure of the German adaption of the CATS has not yet been investigated, especially a confirmatory factor analysis is needed. This is of special importance, since patients were recently identified as “pseudosecure” attached patients due to a high intercorrelation between the clients’ secure attachment to the therapist (CATS-secure) with the clients’ avoidant attachment [27]. Therefore, the factorial structure was reevaluated in a large German-speaking sample and an item selection implemented in order to reduce this overlap of constructs.
Based on two large clinical samples, the present study demonstrated a poor fit for the CATS model proposed by Mallinckrodt and colleagues [5]. These results are consistent with and explicable by the high intercorrelation between the clients’ secure attachment to the therapist (CATS-Secure) with the clients’ avoidant attachment (CATS-Avoidant-Fearful; r = −.69, p < .001). In order to improve the model, items were eliminated based on relevant characteristics (item-total correlation, normal distribution of item scores, factor loadings). The resulting version of 12 items with 4/4/4 items per subscale showed a very good fit for this shortened model (see Table 6.). In addition, items that were eliminated also fit well the characteristic of the sample, being that our participants were inpatients. This implies that such setting represents a different type of answers and might reflect the attachment to the therapist in an inpatient environment, that might be experienced in a different way than outpatients. For example, item 16.: “I think about calling my counselor at home.” and item 22.: “I wish there was a way to spend more time with my counselor.” were excluded (Table 4). Since inpatients are constantly surrounded by the staff, either by nurses, doctors, social workers, coaches, or other room-patients the proximity seeking to the therapist is different than patients in an out-patient environment. Thus, the patient might not feel the same type of separation anxiety as an outpatient, who does not have this network of support in a daily basis.
Overall, evidence for invariance across sex is strong but for age groups it is weaker and should be reassessed in additional studies, es especially because we released equality constraints for the thresholds of two Items 15 (“I think my counselor disapproves of me.”) and 18 (“I don’t like to share my feelings with my counselor.”). Based on our data, we supposed that older people (≥59) compared to younger adults (≤39) would have different attitudes toward their counselor. From the perspective of developmental and personality psychology, we assumed that older adults would have stricter judgement toward their therapist give that they tend score higher on neuroticism [53] compared to younger people.
This economic version also showed a good and improved reliability, compared to the original model proposed by Mallinckrodt and colleagues [5] with reliability values of Alpha = .81/64/.63. Based on this empirical approach, a questionnaire was gained with a good model fit. In addition, an economic version was generated, which is well applicable in the clinical settings with patients with psychological symptoms. This model was also invariant for sex and age groups.
The present study showed very little disparity between long version and short version of the CATS. In addition, the convergent validity for the new short version is given as well. This could be shown based on the convergent validity to the Helping Alliance Questionnaire (HAQ) as well as another questionnaire measuring the expected attachment to the therapist (BFCE). Specifically, clients who scored low on the insecure BFCE-scales (Fear of rejection, Conscious need of care), high on the secure BFCE-scales Readiness of self-disclosure scored also high on the CATS Secure subscale. As in the present data, these patients reported positive working alliances and tend to perceived their therapists as emotionally responsive, accepting, and promoting a “secure base” for exploration (e.g., “I feel that somehow things will work out OK for me when I am with my counselor”) [1, 54, 55]. They show a greater self-disclosure [56] and high in-session exploration [15]. It has been shown that this type of behavior strengthens the working alliance [27, 57, 58]. A strong working alliance is related to improvement in symptoms, global functioning, and interpersonal problems [59]. In this context it is worth mentioning that validity depends on making strong assurances of anonymity, as originally stated by Mallinckrodt and colleagues (1995). The authors mentioned that their participants were assured that their therapist or counselors would never have access to their assessment of the counseling relationship. Such information is crucial for the patients in order to feel comfortable and truly share their internal state with their therapist without hesitation. Otherwise, patients could question the anonymity of their data and be reluctant, which may compromise the validity of the scale.
Clients who scored high on the insecure BFCE- scales, low on the secure BFCE- scales, Readiness of self-disclosure also scored high on the CATS Preoccupied-Merger subscale and desired more frequent and intensely personal contact and long to be “at one” with the therapist. Clients with these characteristics tend to be highly willing to depend on the therapist, fear rejection, abandonment, and wish to be their therapist’s “favorite” client [5, 60]. The correlations of the CATS Preoccupied-Merger subscale with working alliance suggest a poor working alliance characterized by a bond without agreement about the therapy’s goals, as previously observed [15, 61]. According to [62] this type of behavior is related to an insecure attachment, which reflects in behavioral hyperactivation (e.g., a heightened need for proximity and desire to blur professional boundaries: “I think about calling my counselor at home”). Especially adults with a background of dysfunctional interactions with family members, memories of emotionally unavailable parents tend to develop this type of attachment [63]. Clients who scored high on the insecure BFCE- scales, low on the secure BFCE- scales Readiness of self-disclosure also scored high on the CATS Avoidant-Fearful subscale. These patients distrusted their therapists, showed fear of rejection and were reluctant with self-disclosure and reported the poorest working alliances, as previously evidenced [27, 64, 65]. It has been explained that avoidant patients typically decline requests to express their emotions and feel discomfort when getting closer to the therapist [60, 61]. In addition, the high correlations between the psychological symptom questionnaire (SCL-90R) and the avoidant-fearful as well as preoccupied-merger scale of the CATS showed that greater attachment insecurity is associated with greater psychological symptoms, which is consistent with a large body of literature [12, 66, 67].
Even though this study is based on relatively large samples of patients, there are several limitations to be considered. For example, there are differences between the original sample [5] (sample a) and our sample (sample b), that could explain why the factor analyses differed: (1) Sample b), were all inpatients, while the participants in sample a were all outpatients. (2) Sample a) had one therapist and this person was the exclusive focus of ratings; Sample a) worked with many individuals in the inpatient setting (3) Sample a) completed ratings early in the first 5–6 sessions treatment, whereas the participants in our study completed the CATS near termination after about 12 sessions and more than 60 days of continuous inpatient treatment.
Finally, the original CATS is based on an English-speaking population, while our sample is based on German-speaking participants, which may culturally differ from one another. Furthermore, we were not able to collect detailed sociodemographic variables other than age and sex in the second study (Sample 2). However, this matter did not affect any of the statistical analyses. Moreover, no interaction between therapist adult attachment and patient attachment to therapist could be investigated since the adult attachment style of the therapist was not assessed. The importance of such interactions was highlighted by Petrowski and colleagues [24], who found that therapist’s insecure adult attachment was associated with more insecure client attachment to therapist. Moreover, patient attachment to therapist was assessed only by a self-report in the present study. The effect of patient attachment to therapist should be investigated by different methods. In future studies, the patients’ representation of the therapists’ using the Patient-Therapist Adult Attachment Inventory (PT AAI) by Diamond and colleagues [68] might be promising. The PT-AAI [68, 69], is a semi-structured interview developed as an adaptation of the AAI aimed at classifying the mental state concerning patients’ attachment to their therapists, and vice versa.
In general, the short version of the German-version of the CATS showed very good fit. Importantly, we included items that have moderate difficulty in order to maximize sensitivity across the broadest range of the trait. However, it is possible that extreme values cannot be capture with this short version.
For future research, the short version of the CATS has to be implemented in a large clinical sample in order to replicate the psychometric properties and the factorial structure of the CFA. Also, there are still numerous unanswered questions such as, for example, how counter-complementary attachment behavior can and should be used in therapeutic settings [70]. For clinical practice, it would be of interest whether pre-treatment and possible earned security status of the patients would further influence the therapeutic process. In addition, the therapy drop-out rate as well as disorder specific effects needs to be examined more closely in reference to the clients’ attachment to the therapists. Further research on the interaction processes between the attachment representations of the patients and the therapists assessed by using the same measures should be carried out with respect to the therapeutic outcome.
Conclusions
The present study investigated a German adaptation of the original CATS and proposed a shortened version of with improved validity. The CATS-S will be helpful in properly identifying types of client attachment, and we recommend it for medical and psychological research.
Availability of data and materials
The dataset used and analyzed during the current study is available from the corresponding author on reasonable request.
Abbreviations
- CATS:
-
Client Attachment to Therapist Scale
- SCL:
-
Symptom Check List
- BFCE:
-
Bielefeld Client Expectations Questionnaire
- HAQ:
-
Helping Alliance Questionnaire
- AAI:
-
Adult Attachment Inventory
- CMIN/DF:
-
Minimum discrepancy divided by degrees of freedom
- CFI:
-
Comparative Fit Index
- TLI:
-
Tucker Lewis Index
- RMSEA:
-
Root Mean Square Error of Approximation
- SRMR:
-
Standardized Root Mean Square Residual
- BIC:
-
Bayesian Information Criterion
- GH:
-
Gamma hat
References
Bowlby J. A secure base. Clinical applications of attachment theory. London: Routledge; 1978.
Pistole CM. Attachment: implications for counselors. J Couns Dev. 1989;68:190–3.
Horowitz LM, Rosenberg SE, Bartholomew K. Interpersonal problems, attachment styles, and outcome in brief dynamic psychotherapy. J Consult Clin Psychol. 1993;61:549–56.
Janzen J, Fitzpatrick M, Drapeau M. Process involved in client nominated relationship building incidents: client attachment, attachment to therapist, and session impact. Psychotherapy. 2008;45:377.
Mallinckrodt B, Coble HM, Gantt DL. Attachment patterns in the psychotherapy relationship: development of the client attachment therapist scale. J Couns Psychol. 1995;42:307–17.
Yotsidi V, Pezirkianidis C, Karakasidou E, Stalikas A. The client attachment to therapist scale (CATS) in a Greek clinical population: a validation study. Open J Med Psychol. 2018;7(04):59.
Horvath AO, Greenberg L. Development and validation of the working Alliance inventory. J Couns Psychol. 1989;36:223–32.
Diamond D, Blatt SJ. Internal working models and the representational world in attachment and psychoanalytic theories. In: Portions of this chapter were presented at the 100th annual convention of the American Psychological Assn. Washington, DC: Guilford Press; 1994. Aug 1992. 1992.
Henry WP, Strupp HH. The therapeutic alliance as interpersonal process (chap 3). In: Horvarth AO, Greenberg LS, editors. The working alliance: theory research and practise. New York: Wiley; 1994.
Mallinckrodt B. Childhood emotional bonds with parents, development of adult social competencies, and the availability of social support. J Couns Psychol. 1992;39:453–61.
Ainsworth MDS, Blehar MC, Waters E, Wall S. Patterns of attachment: a psychological study of the strange situation. Hillsdale: Lawrence Erlbaum; 1978.
Bachelor A, Meunier G, Laverdiére O, Gamache D. Client attachment to therapist: relation to client personality and symptomatology, and their contributions to the therapeutic alliance. Psychotherapy. 2010;47(4):454.
Mallinckrodt B. The psychotherapy relationship as attachment: evidence and implications. J Soc Pers Relat. 2010;27:262–27.
Woodhouse SS, Schlosser LZ, Crook RE, Ligiero DP, Gelso CJ. Client attachment to therapist: relations to transference and client recollections of parental caregiving. J Couns Psychol. 2003;50:395–408.
Mallinckrodt B, Porter MJ, Kivlighan DM. Client attachment to therapist, depth of in-session exploration, and object relations in brief psychotherapy. Psychother Theory Res Pract Train. 2005;42:85–10.
Taylor P, Rietzschel J, Danquah A, Berry K. Changes in attachment representations during psychological therapy. Psychother Res. 2014;25:222–38.
Sauer EM, Anderson MZ, Gormley B, Richmond CJ, Preacco L. Client attachment orientations, working alliances, and responses to therapy: a psychology training clinic study. Psychother Res. 2010;20:702–11.
Mallinckrodt B, Jeong JS. Meta-analysis of client attachment to therapist: associations with working alliance and client pre-therapy attachment. Psychotherapy. 2015;52:134–9.
Choi G. Client attachment as a predictor of therapy outcome and premature termination. Knoxville: University of Tennessee; 2014. PhD diss.
Woodhouse SS, Gelso CJ. Volunteer client adult attachment, memory for in-session emotion, and mood awareness: an affect regulation perspective. J Couns Psychol. 2008;55:197–208.
Black S, Hardy G, Turpin G, Parry G. Self-reported attachment styles and therapeutic orientation of therapists and their relationship with reported general alliance quality and problems in therapy. Psychol Psychother. 2005;78:363–77.
Mallinckrodt B, Choi G, Daly KD. Pilot test of a measure to assess therapeutic distance and its association with client attachment and corrective experience in therapy. Psychother Res. 2015;25:505–17.
Petrowski K, Joraschky P, Buchheim A. Matching the patient to the therapist: the roles of the attachment status and the helping alliance. J Nerv Ment Dis. 2011;199:839–44.
Petrowski K, Pokorny D, Nowacki K, Buchheim A. The therapist’s attachment representation and the patient’s attachment to the therapist. Psychother Res. 2013;23:25–34.
Brislin RW. Back-translation for cross-cultural research. J Cross-Cult Psychol. 1970;1:185–216 Romano V, Fitzpatrick M, Janzen J. The secure-base hypothesis: global attachment, attachment to counselor and session exploration in psychotherapy. J Couns Psychol 2008;55:495–504.
Brislin, R. W. Translation and content analysis of oral and written material. In H. C. Triandis; & J. W. Berry (Eds.), Handbook of crosscultural psychology. Boston: Allyn & Bacon; 1980, 2. 389–444. Wiseman H, Tishby O. Client attachment, attachment to therapist and client-therapist attachment match: how do they relate to change in psychodynamic psychotherapy? Psychother Res 2014;24:392–406.
Brislin RW, Lonner WJ, Thorndike RM. Cross-cultural research methods. New York: Wiley; 1973. Mallinckrodt B, Anderson MZ, Choi G, Levy KN, Petrowski K, Sauer EM, Tishby O, Wiseman H. Pseudosecure vs. individuated-secure client attachment to therapist: implications for therapy process and outcome. Psychother Res 2016;24:1–15
World Health Organization. Processs of translation and adaption of instruments: WHO; 2010. Available online at: https://www.who.int/substance_abuse/research_tools/translation/en/; Accessed 26 Feb 2021
Spitzer RL, Williams JB, Gibbon M, First MB. User's guide for the structured clinical interview for DSM-III-R: SCID. 1990.
Wittchen HU, Zaudig M, Fydrich T. SKID. Strukturiertes Klinisches Interview für DSM-IV. Achse I und II. Handanweisung. [Structured clinical interview for DSM-IV. Axis I and II. User’s guide.] Göttingen: Hogrefe; 1997.
Franke GH. SCL-90-R. The Symptom-Checklist by Derogatis. Weinheim: Beltz; 1995.
Hessel A, Schumacher J, Geyer M, Brähler E. Symptom-checklist SCL-90-R: validation and standardization based on a representative sample of the German population. Diagnostica. 2001;47:27–39.
Der HD. Bielefelder Fragebogen zu Klientenerwartungen (BFKE). Psychotherapeut. 1999;44:159–66.
Alexander LB, Luborsky L. The Penn helping Alliance scales. In: Greenberg LS, Pinsof W, editors. The psychotherapeutic process: a research handbook. New York: Guilford; 1986. p. 325–66.
Bassler M, Potratz B, Krauthauser H. Der “Helping Alliance Questionnaire”(HAQ) von Luborsky. Möglichkeiten zur Evaluation des therapeutischen Prozesses von stationärer Psychotherapie. Psychotherapeut. 1995;40:23–32.
Dinno A. Paran: horn’s test of principal components/factors. R package version 1.5. 1; 2012.
Rosseel Y. Lavaan: an R package for structural equation modeling and more. Version 0.5–12 (BETA). J Stat Softw. 2012;48(2):1–36.
Contributors S. semTools: Useful tools for structural equation modeling. R Package Version 0.4-14. 2016.
Schultze M. Stuart: subtests using algorithmic rummaging techniques (R package version 0.7. 3) [computer software].; 2018.
Zhang G, Jiang G, Hattori M, Trichtinger L. EFAutilities: Utility functions for exploratory factor analysis. R package version, 2(0). 2019.
Horn JL. A rationale and test for the number of factors in factor analysis. Psychometrika. 1965;30(2):179–85.
Croom Helm Hair JF, Black WC, Babin BJ, Anderson RE, Tatham RL. J Multivar Data Anal. 2007.
Kim H-Y. Statistical notes for clinical researchers: assessing normal distribution (2) using skewness and kurtosis. Restor Dent Endod. 2013;38(1):52.
Muthén B, du Toit SHC, Spisic D. Robust inference using weighted least squares and quadratic estimating equations in latent variable modeling with categorical and continuous outcomes. 1997. Available at https://www.statmodel.com/download/Article_075.pdf
Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model. 1999;6:1–55.
Hu L, Bentler PM. Fit indices in covariance structure modeling: sensitivity to Underparameterized model misspecification. Psychol Methods. 1998;3:424–53.
MacCallum RC, Browne MW, Sugawara HM. Power analysis and determination of sample size for covariance structure modeling. Psychol Methods. 1996;1:130–49.
Schermelleh-Engel K, Moosbrugger H, Müller H. Evaluating the fit of structural equation models: tests of significance and descriptive goodness-of-fit measures. Methods Psychol Res Online. 2003;8:23–74.
Jöreskog KG, Sörbom D. Lisrel 8: structural equation modeling with the SIMPLIS command language. Hillsdale: Erlbaum; 1993.
Cheung GW, Rensvold RB. Evaluating goodness-of-fit indexes for testing measurement invariance. Struct Equ Model. 2002;9:233–55.
Wu H, Estabrook R. Identification of confirmatory factor analysis models of different levels of invariance for ordered categorical outcomes. Psychometrika. 2016;81(4):1014–45.
Green SB, Yang Y. Reliability of summed item scores using structural equation modeling: an alternative to coefficient alpha. Psychometrika. 2009;74(1):155–67.
Herzberg P., Roth M. (2014) Persönlichkeit: Stabil oder Veränderbar?. In: Persönlichkeitspsychologie. Basiswissen Psychologie. Springer VS, Wiesbaden. https://doi.org/10.1007/978-3-531-93467-9_8.
Ainsworth MDS. Object relations, dependency and attachment: a theoretical view of the mother-infant relationship. Child Dev. 1969;40:969–1025.
Ainsworth MDS. Some considerations regarding theory and assessment relevant to attachments beyond infancy. Attach Preschool Years. 1990;IV:463–88.
Mikulincer M, Nachshon O. Attachment styles and patterns of self-disclosure. J Pers Soc Psychol. 1991;61(2):321.
Eames V, Roth A. Patient attachment orientation and the early working alliance-a study of patient and therapist reports of alliance quality and ruptures. Psychother Res. 2000;10(4):421–34.
Diener MJ, Monroe JM. The relationship between adult attachment style and therapeutic alliance in individual psychotherapy: a meta-analytic review. Psychotherapy. 2011;48(3):237.
Lilliengren P, Falkenström F, Sandell R, Mothander PR, Werbart A. Secure attachment to therapist, alliance, and outcome in psychoanalytic psychotherapy with young adults. J Couns Psychol. 2015;62(1):1.
Wallin DJ. Attachment in psychotherapy. New York: Guilford press; 2007.
Talia A, Miller-Bottome M, Wyner R, Lilliengren P, Bate J. Patients' Adult Attachment Interview classification and their experience of the therapeutic relationship: are they associated?. Res Psychother. 2019;22(2):361. https://doi.org/10.4081/ripppo.2019.361.
Mikulincer M, Shaver PR. Boosting attachment security to promote mental health, prosocial values, and inter-group tolerance. Psychol Inq. 2007;18(3):139–56.
King JL, Mallinckrodt B. Family environment and alexithymia in clients and non-clients. Psychother Res. 2000;10(1):78–86.
Bernecker SL. Patient Interpersonal and Cognitive Changes in Relation to Outcome in Interpersonal Psychotherapy for Depression; 2013.
Elliot AJ, Reis HT. Attachment and exploration in adulthood. J Pers Soc Psychol. 2003;85(2):317.
Levy KN, Ellison WD, Scott LN, Bernecker SL. Attachment style. J Clin Psychol. 2011;67:193–203.
Muller RT. Trauma and dismissing (avoidant) attachment: intervention strategies in individual psychotherapy. Psychotherapy. 2009;46(1):68.
Diamond D, et al. “Scoring system for the patient-therapist adult attachment interview.” 2001.
George C, Kaplan N, Main M. Adult Attachment Interview. University of California; 1985.
Mallinckrodt B. Attachment, social competencies, social support and interpersonal process in psychotherapy. Psychother Res. 2000;10:239–66.
Acknowledgements
We acknowledge support by the Open Access Publication Fund of the University of Dresden.
Title: We note that the title in the system, is different from the title in the manuscript. Please ensure that the title in the system match the title in the manuscript. We changed the title of the paper as recommended by Reviewer 1, as in is in the manuscript stated.
Permission was granted to use and modify the scales described in the submission by the owners/copyright holders.
Funding
Open Access funding enabled and organized by Projekt DEAL. The authors received no funding for the reported research.
Author information
Authors and Affiliations
Contributions
All listed authors have made substantial contributions to the present research in one way or another. KP contributed to conceptualization, design, and data collection, analysis as well as writing of the manuscript. IS and BS contributed to the and analysis as well as writing of the manuscript. EO and JR contributed to the data collection and correction of the manuscript. All authors agree to be accountable for the content of the work. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The present study was conducted in accordance with the Declaration of Helsinki. The study was approved by the local ethics committee of TU-Dresden (Code of ethics: 112052007) Participants gave their informed consent before they were allowed to participate in the study. Participants under the age of 18 were not recruited.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Petrowski, K., Schmalbach, B., Ronel, J. et al. Evaluating the psychometric properties of the German adaptation of the client attachment to therapist scale. BMC Med Res Methodol 22, 96 (2022). https://doi.org/10.1186/s12874-022-01548-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12874-022-01548-2