
Abstract
Introduction
In the current systematic review and meta-analysis, we aim to analyze the existing literature to evaluate the role of inflammatory biomarkers, including neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), C-reactive protein (CRP), tumor necrosis factor-a (TNF-a), and interleukin-6 (IL-6) among individuals with cardiac syndrome X (CSX) compared to healthy controls.
Methods
We used PubMed, Web of Science, Scopus, Science Direct, and Embase to systematically search relevant publications published before April 2, 2023. We performed the meta-analysis using Stata 11.2 software (Stata Corp, College Station, TX). So, we used standardized mean difference (SMD) with a 95% confidence interval (CI) to compare the biomarker level between patients and healthy controls. The I2 and Cochran’s Q tests were adopted to determine the heterogeneity of the included studies.
Results
Overall, 29 articles with 3480 participants (1855 with CSX and 1625 healthy controls) were included in the analysis. There was a significantly higher level of NLR (SMD = 0.85, 95%CI = 0.55–1.15, I2 = 89.0 %), CRP (SMD = 0.69, 95%CI = 0.38 to 1.02, p < 0.0001), IL-6 (SMD = 5.70, 95%CI = 1.91 to 9.50, p = 0.003), TNF-a (SMD = 3.78, 95%CI = 0.63 to 6.92, p = 0.019), and PLR (SMD = 1.38, 95%CI = 0.50 to 2.28, p = 0.02) in the CSX group in comparison with healthy controls.
Conclusion
The results of this study showed that CSX leads to a significant increase in inflammatory biomarkers, including NLR, CRP, IL-6, TNF-a, and PLR.
Similar content being viewed by others


Introduction
Cardiac syndrome X (CSX) is characterized by typical or atypical anginal chest pain with no evidence of significant coronary vascular abnormalities visualized on the angiogram. The etiology of cardiovascular symptoms due to CSX has yet to be fully understood [1], and with previous studies failing to uncover specific pathophysiology of CSX, our abilities to cure and prevent this disease are limited. However, several pathogenic mechanisms have been proposed, including inflammation, neuroendocrine dysfunction, and oxidative stress [2, 3]. To further characterize immune dysregulation in CSX, many studies have evaluated levels of circulating inflammatory mediators, such as neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR), C-reactive protein (CRP), tumor necrosis factor-a (TNF-a), and interleukin-6 (IL-6) [4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32].
An emerging and unique inflammatory marker, the NLR, has more recently been investigated in the setting of human cardiac diseases like cancer, stroke, and hypertension. A population-based study on 13,732 participants published in 2024 showed that NLR was associated with coronary heart disease risk in adults [33]. Pathologically, blood neutrophils increase, and lymphocytes decrease in response to inflammatory stress, increasing the NLR. PLR, similar to NLR, is a relatively novel inflammatory marker, with recent studies showing significant elevation in several cardiac disorders [34]. For example, a recent meta-analysis published in 2024 showed that among heart failure patients, PLR was significantly lower in survived patients rather than deceased group [35]. In addition, CRP is an acute-phase protein released during times of increased stress and inflammation. Recent studies have shown that this biomarker can have some diagnostic and prognostic role in several cardiovascular disorders. For example, a 15-year prospective cohort study published in 2024 showed that CRP is associated with an increased risk of cardiovascular disease [36]. In addition, TNF-a and IL-6 are well-studied inflammatory markers released mostly by macrophages and monocytes during stressful events and have some diagnostic roles in cardiac disorders like hypertension and myocardial infarction [37,38,39,40]. While some previous studies have shown that these biomarkers were increased in CSX patients, other studies reported no association between these biomarkers and CSX; so, debate continues about the role of these biomarkers in CSX.
To better determine the association of NLR, CRP, IL-6, TNF-a, and PLR with CSX, we have conducted a meta-analysis to review the published literature examining inflammatory marker levels in these patient populations.
Materials and methods
This study follows the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) 2020 reporting guideline [41]. The PRISMA checklist of this study is shown in Supplementary File A. The protocol was registered in PROSPERO (CRD42023448843).
Eligibility criteria
Our inclusion criteria based on PICO criteria were as follows:
-
(a)
Population: Patients with CSX.
-
(b)
Control: Healthy controls.
-
(c)
Intervention/Exposure: Level of NLR, CRP, IL-6, TNF-a, and PLR in CSX.
-
(d)
Outcomes: Diagnostic significance of NLR, CRP, IL-6, TNF-a, and PLR in CSX.
-
(e)
Study design: cohort, case-control, and cross-sectional studies.
Our exclusion criteria were as follows: (1) Those that did not compare any one of our outcomes inflammatory biomarkers (NLR, CRP, IL-6, TNF-a, OR PLR) levels between CSX patients and controls; (2) Studies that did not report their results as Mean ± standardized division (SD). There were not any limitations on language or date of publication.
Information sources
One author (ShS) searched PubMed, Web of Science, Scopus, ScienceDirect, and Embase databases to identify all studies comparing the level of inflammatory biomarkers between CSX patients and healthy controls, published before April 2, 2023. Initially, we conducted a thorough search to identify all studies on the role of inflammatory biomarkers in CSX.
Search strategy
Our search strategy was as follows: (“NLR“[All Fields] OR “neutrophil to lymphocyte ratio“[All Fields] OR “platelet to lymphocyte ratio“[All Fields] OR “PLR“[All Fields] OR “C-reactive protein“[All Fields] OR “CRP“[All Fields] OR “tumor necrosis factor“[All Fields] OR “TNF“[All Fields] OR “interleukin“[All Fields]) AND (“cardiac syndrome X“[All Fields] OR “microvascular angina“[MeSH Terms] OR “microvascular angina“[All Fields]). There was no limitation on the publication date or language of studies in our search. The exact search strategy is shown in Supplementary file B. We did not search unpublished studies.
Additionally, two authors (ShKh and ShS) reviewed the reference lists of included and relevant studies, according to the snowball method, to identify further eligible studies.
Selection process
EndNote was used for study screening [42]. Initially, duplicate studies were deleted (521). Then, two authors (PA and ShS) screened the titles and abstracts of studies found in the initial search of databases and found the closely relevant studies (N = 85). Then, the same authors obtained and screened the full texts of these studies. Then, 41 studies were deleted due to lack of data on NLR, CRP, IL-6, TNF-a, or PLR, 11 studies due to irrelevant population, four for being review articles, and one due to lack of peer review. The remaining studies were used in the meta-analysis (N = 29). The kappa statistic was used to calculate Inter-reviewer agreement for the study selection [43]. The Kappa value of > 0.6 was considered a significant agreement between the authors.
Data collection process
Supplementary file C shows our data extraction form. Two authors (MAD and PA) extracted data manually and independently using an Excel sheet.
Data items
The first author, year of publication, study design, study location, total sample size, number of patients and healthy controls, type of biomarker measured, mean and SD of biomarker level, or any data for estimating the mean and SD (median and IQR or/and range) were extracted.
Study risk of bias assessment
Two authors (MKh and MAD) conducted the quality assessment of included studies, utilizing the Newcastle–Ottawa scale (NOS) [44]. Disagreements between the authors were finally resolved via consensus and consulting with the third author(HB). Those studies with six or more points were deemed to have good quality.
Effect measures
we used standardized mean difference (SMD) with a 95% confidence interval (CI) to compare the biomarker level between patients and healthy controls. The median(Interquartile range) values were converted to mean ± SD using the method introduced by Wan et al. [45].
Synthesis methods
We performed the meta-analysis using Stata 11.2 software (Stata Corp, College Station, TX). The I2 and Cochran’s Q tests were adopted to determine the heterogeneity of the included studies. Significant heterogeneity between studies was conceived as I 2 >50% and p-value of the Q test < 0.05. In the case of significant heterogeneity, we used the random-effects model. Otherwise, the fixed-effect model was chosen. P value < 0.05 was considered significant.
Reporting bias assessment
We used the funnel plot and Egger’s test to determine the publication bias. The symmetric plot was seen in the lack of bias.
Certainty assessment
One of the authors (ShKh) utilized the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) method to evaluate the certainty of the evidence for the outcome investigated in the meta-analysis [46].
Results
Search results and included studies
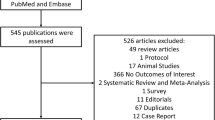
Table 1 shows the general characteristics of included studies, and Fig. 1 shows the PRISMA flow diagram, indicating the process of inclusion and exclusion in detail [4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32]. We found an almost perfect agreement between the authors concerning interrater reliability of study selection (94% agreement; kappa = 0.83; 95%CI = 0.65–1.0, P < 0.001).

PRISMA 2020 Flow diagram for new systematic reviews which includes searches of databases, registers and other sources
NLR level in patients with cardiac syndrome X
A random-effect model revealed significantly higher NLR levels in the CSX group than healthy controls (SMD = 0.85, 95%CI = 0.55 to 1.15, p < 0.0001, I2 = 89.0%) (Fig. 2). However, the GRADE approach determined that the certainty of this summary estimate of effect was very low. (Table 2).

Meta-analysis of differences in NLR level between CSX patients and healthy controls
The subgroup analysis according to the study design demonstrated that there was a significantly higher NLR level among CSX patients in comparison with healthy controls in either retrospective (SMD = 0.83, 95% CI = 0.51 to 1.14, p < 0.001, I2 = 74.3%) or prospective studies (SMD = 0.98, 95% CI = 0.32 to 1.64, p = 0.004, I2 = 94.2%) (Fig. 3).

Subgroup analysis of differences in NLR level between CSX patients and healthy controls according to study design
CRP level in patients with cardiac syndrome X
CRP level was significantly higher in the CSX group than healthy controls (SMD = 0.69, 95%CI = 0.38 to 1.02, p < 0.0001). A random-effect model was used due to high heterogeneity (I2 = 92.2%, Fig. 4). However, the GRADE approach determined that the certainty of this summary estimate of effect was very low (Table 2).

Meta-analysis of differences in CRP level between CSX patients and healthy controls
IL-6 level in patients with cardiac syndrome X
Meta-analysis of four relevant articles using the random-effect model showed that IL-6 level was significantly higher in the CSX group compared to healthy controls (SMD = 5.70, 95%CI = 1.91 to 9.50, p = 0.003, I2 = 99.1%, Fig. 5). According to the GRADE approach, the certainty of this summary estimate of effect was very low (Table 2).

Meta-analysis of differences in IL-6 level between CSX patients and healthy controls
TNF-a level in patients with Cardiac Syndrome X
In this meta-analysis of four relevant articles, TNF-a level was significantly higher in the CSX group (random-effect model, SMD = 3.78, 95%CI = 0.63 to 6.92, p = 0.019, I2 = 99.1%, Fig. 6). The certainty of this summary effect estimate was very low (Table 2).

Meta-analysis of differences in TNF-a level between CSX patients and healthy controls
PLR Level in patients with cardiac syndrome X
Then we analyzed the differences in PLR level between CSX patients and healthy controls and found that compared to healthy controls, PLR level was significantly higher in the CSX group (random-effect model, SMD = 1.38, 95%CI = 0.50 to 2.28, p = 0.02, I2 = 96.3%, Fig. 7). However, the certainty of evidence was very low in this analysis (Table 2).

Meta-analysis of differences in PLR level between CSX patients and healthy controls
Publication bias
Egger’s test showed no publication bias among studies on PLR(p = 0.47) and TNF-a (p = 0.07). However, there was some evidence of potential publication bias among studies on NLR(p = 0.01), CRP (p = 0.02), and IL6 (p = 0.01). The relevant funnel plots are shown in supplementary File D.
Discussion
CSX is a significant cause of morbidity due to recurring angina events despite its favorable long-term prognosis. This condition’s pathophysiology must be understood to offer patients the best possible treatment. Although the pathophysiology of CSX is complex, inflammation is likely a key factor [2]. This meta-analysis showed a significant increase in NLR level as a new inflammatory biomarker in CSX patients compared to healthy controls. This difference remained significant in a subgroup analysis by study design. The analysis also showed significant increases in CRP, IL-6, TNF-a, and PLR levels reported in prior studies.
Neutrophils play a central role in innate immunity by enhancing pro-inflammatory reactions, while lymphocytes are integral to the adaptive immune system, modulating immune responses. When NLR is elevated, the inflammatory actions of neutrophils may surpass the regulatory effects of lymphocytes, leading to a notable escalation in peripheral inflammation [47].
Numerous original studies have been published on the role of NLR and inflammatory markers in recent literature, and there is now a need for a systematic review of the literature. For example, a recent meta-analysis indicated that an elevated pretreatment NLR could predict the risk of major adverse cardiac events (MACE) and mortality in patients who had a recent acute coronary syndrome [48]. Another meta-analysis reported that NLR could predict arrhythmia, in-stent thrombosis, angina, no-reflow, advanced heart failure, nonfatal myocardial infarction, long-term all mortality, cardiac mortality, MACE, and nonfatal myocardial infarction (MI) in patients with acute ST-segment elevation MI after percutaneous coronary intervention [49]. In addition, a meta-analysis conducted by Liu et al. has shown that elevated preoperative NLR could predict postoperative atrial fibrillation [50]. In another meta-analysis, an elevated preoperative NLR (> 5 in vascular surgery, > 3.3 in cardiac surgery) was associated with high mortality at a mean follow-up of 34.8 months, raised risk of post-operative re-intubation, amputation in vascular operations, and increased cardiac mortality [51]. In the recent meta-analysis on the association of NLR with heart failure, NLR was associated with all-cause mortality and renal dysfunction [52].
To the best of our knowledge, there has not been a review of research on CSX. Our findings are the first to provide a thorough and up-to-date assessment of NLR and other inflammatory marker levels in CSX patients based on a review of all publications.
Despite numerous studies investigating the correlation between NLR and CSX in the past, the findings have been inconsistent. The existing literature has shown a significant variability in the reported associations between NLR and CSX. While dissecting the results, we found that NLR has been shown in the literature to be a unique inflammatory marker that may reflect important immunologic abnormalities critical to the development of CSX [31].
The PLR is increasingly being viewed as a marker of systemic inflammation due to studies indicating that platelets have early involvement in the inflammatory response and tissue healing [53]. However, studies on the PLR are less frequent compared to studies on the NLR [54]. Platelets collaborate with different types of white blood cells and release substances that prompt leukocytes to adhere faster to endothelial surfaces, potentially causing cellular leakage. Platelets can significantly impact the inflammatory response of leukocytes, either enhancing or suppressing their activity. An increased PLR may result from chronic low-grade inflammation, and a rising PLR could indicate persistent inflammation, increasing susceptibility to various conditions like CSX, coronary artery disease, autoimmune diseases, and solid organ tumors [55].
Similar to the NLR, many studies have investigated the potential of the PLR as a diagnostic tool for determining the extent of inflammation in various cardiovascular diseases. Recently, a meta-analysis revealed that an increased PLR may indicate stable CAD and can help predict collateral circulation, severe CAD stenosis, and CSF [56]. Higher PLR predicts worse in-hospital and long-term outcomes in STEMI patients following pPCI, according to a meta-analysis published in 2021 [57]. In another study, Wang and colleagues discovered that NLR and PLR are potential biomarkers for predicting prognosis in individuals with acute pulmonary embolism (PE) since the increase of both biomarkers was linked to greater mortality rates [58]. A meta-analysis conducted in 2021 found that patients with STEMI who have higher PLR levels upon admission and receive primary PCI treatment are more likely to experience in-hospital MACE and mortality, as well as long-term MACE and mortality [59]. Lastly, Li and colleagues discovered that PLR has the potential to be an effective biomarker to predict the likelihood of poorer prognosis in patients with ACS [60]. Our study also showed significantly higher levels of PLR in CSX patients.
The positive results from different studies indicate that NLR and PLR are proper biomarkers for cardiovascular diseases, and their elevation can predict adverse outcomes. However, the specificity of NLR and PLR for these diseases is under debate as they may not differentiate two different illnesses. Aging, ethnicity, obesity, and genetic factors are other factors that can alter inflammatory biomarkers, so clinicians should be cautious when using these biomarkers for their diagnosis [61, 62].
Other investigations have shown an unequal distribution of pro-inflammatory elements and anti-inflammatory processes in individuals with CSX, suggesting that inflammation could contribute to endothelial and microvascular dysfunction, which are believed to play a role in the onset of CSX [2]. Tousoulis and colleagues found elevated levels of intercellular adhesion molecule-1 and vascular cell adhesion molecule-1 (VCAM-1) in the bloodstream of patients with CSX. These molecules are produced by activated endothelial cells in response to inflammatory triggers [63].
As for IL6 and TNF-a, similar elevation was found in our analysis of CSX patient studies.
IL-6 is a significant cytokine that has both anti-inflammatory and pro-inflammatory effects. It can be produced locally by crucial cells in the development of atherosclerosis, such as muscle cells, endothelial cells, and macrophages [26]. Therefore, it can lead to vascular inflammation by inducing the formation of foam cells in macrophages, dysfunction of the endothelium, migration of inflammatory cells into the subintima, and smooth muscle proliferation [64]. This indicates that IL-6 may contribute to the pathogenesis of CSX by promoting inflammation and initiating endothelial dysfunction, which leads to reduced vascular reactivity, specifically microvascular vasoconstriction. It may also cause myocardial ischemia in CSX by increasing diffuse atherosclerosis at the microvasculature [65].
TNF-a has been associated with the development and advancement of atherosclerosis and its related outcomes, such as acute coronary syndrome. Additionally, TNF-a has been demonstrated to hinder the generation of NO by inhibiting the production of the endothelial nitric oxide synthase enzyme in endothelial cells [66]. The most commonly accepted explanation of CSX pathogenesis suggests that this condition can induce endothelial dysfunction, leading to impaired microvascular function.
Notably, new evidence suggests that CRP may be both a marker and a mediator of cardiac syndrome X. CRP induces endothelial cells to produce cellular adhesion molecules, endothelin-1, and interleukin-6 [25]. CRP plays a role in activating monocyte chemoattractant protein-1 and enhancing the uptake of low-density lipoprotein by macrophages. Additionally, CRP inhibits angiogenesis, decreases nitric oxide synthesis, upregulates the angiotensin type 1 receptor in smooth muscle cells, and reduces prostacyclin release by endothelial cells [67]. Reducing CRP levels by using statins or aspirin could improve coronary microvascular function. However, the efficacy and safety of this approach are not definitively established and require further investigation. Indeed, since many inflammatory mediators exist, identifying inflammatory mechanisms and triggers in each specific clinical scenario and targeting therapy to the particular rate limiting or trigger stages in effector pathways looks more plausible [67].
While patients with CSX have a favorable prognosis, they frequently develop recurring angina pectoris crises. Several drugs used to treat stenotic coronary artery disease can be recommended in this clinical state; however, there is no specific treatment available due to the unknown etiology of the disease [1]. We believe future research into specific CSX treatment approaches will concentrate on novel pathways, such as targeting inflammation and NLR levels.
Limitations and strengths
We gathered all information on the association between inflammatory biomarkers and cardiac syndrome X for the current meta-analysis. Although meta-analysis often strengthens the existing evidence, there are various limitations to consider when interpreting our study results. Our study has several limitations associated with the observational nature of the included studies with all the inherited biases. In fact, the considerable heterogeneity found, which is likely due to the inclusion criteria used by the participants, as well as the study designs, diagnostic criteria, sex, and age of participants, may have led to indefinite findings. Furthermore, the results could have been biased due to publication bias. Furthermore, using the GRADE method, the GRADE approach determined that the certainty of this summary estimate of effect was very low. Another limitation was that most of the included studies were conducted in Turkey, China, and Italy. Inflammatory biomarkers may differ depending on race and other factors. As a result, further studies in other regions are needed to verify or reject the influence of race on inflammatory biomarkers. In addition, our findings are limited by the use of SMD instead of odds ratio(OR), risk ratio (RR), and hazard ratio (HR). When we extracted the data, most relevant studies reported mean ± SD. So, in our study, SMD was used. This limitation means that study findings must be interpreted cautiously because average values can prove differences but not correlations. This issue is intriguing and could be usefully explored in further research. Despite these limitations, our findings provide crucial clinical implications. To the best of our knowledge, this is the first meta-analysis that completely analyzes information addressing the relationship between inflammatory biomarkers and cardiac syndrome X. Other key strengths of our meta-analysis should also be highlighted. First, we established a repeatable and thorough search method for each database, in addition to the manual reference search of the references of the first selected papers, reviews, meta-analyses, or comments. Furthermore, various inflammatory biomarkers were carefully analyzed in this study, although further research is required to determine a cut-off value point for such biomarkers. Finally, all the included articles excluded the patients with disorders affecting inflammatory markers, such as hematological disorders, chronic or acute inflammatory or infectious diseases, malignancies, hepatic insufficiency, renal dysfunction, or steroid therapy. Regarding the fact that in several systemic disorders, the level of inflammatory markers may rise, and it can affect the results of diagnostic tests, this exclusion criterion among included studies could substantially increase our results’ validity.
Conclusion
Despite the limitations, our results showed that the levels of NLR, CRP, IL-6, TNF-a, and PLR in patients with CSX were increased compared to healthy controls. Although these biomarkers are straightforward and readily accessible, making them potentially suitable options for countries with limited healthcare resources, their ability to predict CSX needs further exploration. Additional studies are necessary to investigate the correlation between these ratios and CSX in more depth.
Data availability
The dataset supporting the conclusions of this article is included in the article.
Change history
08 June 2024
A Correction to this paper has been published: https://doi.org/10.1186/s12872-024-03968-y
Abbreviations
- neutrophil to lymphocyte ratio:
-
NLR
- platelet to lymphocyte ratio:
-
PLR
- C-reactive protein:
-
CRP
- tumor necrosis factor-a :
-
TNF-a
- interleukin-6:
-
IL-6
- cardiac syndrome X:
-
CSX
- vascular cell adhesion molecule-1:
-
VCAM-1
- Standardized mean difference:
-
SMD
- 95% confidence interval:
-
95% CI
References
Piegza M, Wierzba D, Piegza J. Cardiac syndrome X-the present knowledge. Psychiatr Pol. 2021;55(2):363–75.
Mahtani AU, Padda IS, Bhatt R. Cardiac syndrome X, in StatPearls [Internet]. StatPearls Publishing; 2022.
Jarczewski J et al. Microvascular angina (Cardiac Syndrome X) from a historical overview, epidemiology, pathophysiology to treatment recommendations—a minireview. Folia Med Cracov, 2021. 61(3).
Alizade E, et al. Association of monocyte-to-HDL cholesterol ratio with cardiac syndrome X is linked to systemic inflammation. Koşuyolu Heart J. 2016;19(2):97–102.
Altiparmak IH, et al. Evaluation of thiol levels, thiol/disulfide homeostasis and their relation with inflammation in cardiac syndrome X. Coron Artery Dis. 2016;27(4):295–301.
Arroyo-Espliguero R, et al. Chronic inflammation and increased arterial stiffness in patients with cardiac syndrome X. Eur Heart J. 2003;24(22):2006–11.
Atmaca Y, et al. The association of elevated white blood cell count and C-reactive protein with endothelial dysfunction in cardiac syndrome X. Acta Cardiol. 2008;63(6):723–8.
Bolayir HA. Relationship between platelet-to-lymphocyte ratio and cardiac syndrome x. Cumhuriyet Med J. 2017;39(3):570–5.
Boyraz B, et al. Assessment of inflammatory parameters in obstructive coronary artery disease and cardiac syndrome X: an evolving value of neutrophil-lymphocyte ratio. Eur Res J. 2020;6(1):53–61.
Büyükkaya E et al. The serum pentraxin-3 is elevated in patients with cardiac syndrome X 2013.
Caglar FT, et al. Evaluation of serum vitamin D levels in patients with X syndrome. Eur Rev Med Pharmacol Sci. 2016;20(6):1155–60.
Cao G-Y, et al. The Relationship between the neutrophil to lymphocyte ratio, the platelet to lymphocyte ratio, and Cardiac Syndrome X. Risk Manage Healthc Policy. 2022;15:427.
Demir B, et al. Does inflammation have a role in the pathogenesis of cardiac syndrome X? A genetic-based clinical study with assessment of multiple cytokine levels. Angiology. 2016;67(4):355–63.
Demirkol S, et al. Neutrophils/lymphocytes ratio in patients with cardiac syndrome X and its association with carotid intima–media thickness. Clin Appl Thromb Hemost. 2014;20(3):250–5.
Dollard J, et al. A prospective study of C-reactive protein as a state marker in Cardiac Syndrome X. Brain Behav Immun. 2015;43:27–32.
Eroglu S, et al. Serum levels of C-reactive protein and uric acid in patients with cardiac syndrome X. Acta Cardiol. 2009;64(2):207–11.
Guler E, et al. Evaluation of adiponectin and lipoprotein (a) levels in cardiac syndrome X. Springer; 2015.
Karakaş MF, et al. Kardiyak Sendrom X’de Eritrosit dağılım genişliği RDW Ile hs-CRP seviyelerinin incelenmesi. Abant Tıp Dergisi. 2013;2(1):17–22.
Lanza GA, et al. Assessment of systemic inflammation and infective pathogen burden in patients with cardiac syndrome X. Am J Cardiol. 2004;94(1):40–4.
Li J-J, et al. Elevated circulating inflammatory markers in female patients with cardiac syndrome X. Cytokine. 2007;40(3):172–6.
Lin C-P, et al. Differential mononuclear cell activity and endothelial inflammation in coronary artery disease and cardiac syndrome X. Int J Cardiol. 2003;89(1):53–62.
Mahfouz RA, et al. Association of morning blood pressure surge with carotid intima-media thickness and cardiac dysfunction in patients with cardiac syndrome-X. Blood Press. 2018;27(5):297–303.
Okyay K, et al. Relationship between neutrophil-to-lymphocyte ratio and impaired myocardial perfusion in cardiac syndrome X. Eur Rev Med Pharmacol Sci. 2015;19(10):1881–7.
Qing P, et al. Evaluation of red blood cell distribution width in patients with cardiac syndrome X. Dis Markers. 2013;34(5):333–9.
Rasmi Y, Raeisi S, Seyyed MH, Mohammadzad. Association of inflammation and Cytotoxin-Associated Gene a positive strains of Helicobacter Pylori in Cardiac Syndrome X. Helicobacter. 2012;17(2):116–20.
Recio-Mayoral A, et al. Inflammation and microvascular dysfunction in cardiac syndrome X patients without conventional risk factors for coronary artery disease. JACC: Cardiovasc Imaging. 2013;6(6):660–7.
Şahin DY, et al. Relationship between oxidative stress markers and cardiac syndrome X. J Clin Experimental Investigations. 2012;3(2):174–80.
Tondi P, et al. Endothelial dysfunction as assessed by flow-mediated dilation in patients with cardiac syndrome X: role of inflammation. Eur Rev Med Pharmacol Sci. 2011;15(9):1074–7.
Ungan İ, et al. Evaluation of the Epicardial Fat tissue thickness and serum omentin levels in patients with Cardiac Syndrome X. Koşuyolu Heart J. 2019;22(1):13–9.
Yaşar E, Bayramoğlu A. Systemic Immune-Inflammation Index as a Predictor of Microvascular Dysfunction in Patients With Cardiac Syndrome X Angiology, 2022: p. 00033197221087777.
Yurtdas M, et al. Heart rate recovery after exercise and its relation with neutrophil-to-lymphocyte ratio in patients with cardiac syndrome X. Coron Artery Dis. 2014;25(6):485–92.
Akın Y, et al. Predictive value of the systemic immune inflammatory index in cardiac syndrome x. BMC Cardiovasc Disord. 2023;23(1):1–7.
Wang Y, et al. The neutrophil-to-lymphocyte ratio is associated with coronary heart disease risk in adults: a population-based study. PLoS ONE. 2024;19(2):e0296838.
Cao GY, et al. The Relationship between the neutrophil to lymphocyte ratio, the platelet to lymphocyte ratio, and Cardiac Syndrome X. Risk Manag Healthc Policy. 2022;15:427–33.
Vakhshoori M, et al. The impact of platelet-to-lymphocyte ratio on clinical outcomes in heart failure: a systematic review and meta-analysis. Ther Adv Cardiovasc Dis. 2024;18:17539447241227287.
Li N, et al. The combination of high uric acid and high C-reactive protein increased the risk of Cardiovascular Disease: a 15-year prospective cohort study. Nutrition, Metabolism and Cardiovascular Diseases; 2024.
Yao Y-s, Chang W-w, Jin Y-l. Association between TNF-a promoter-308G/A polymorphism and essential hypertension in the Asian population: a meta-analysis. J Renin-Angiotensin-Aldosterone Syst. 2017;18(4):1470320317741066.
Panahi M, et al. P2861 a systematic review and meta-analysis of anti-cytokine therapies targeting IL-1 and TNF-A in myocardial infarction and heart failure. Eur Heart J. 2018;39(suppl1):ehy565.
He F, et al. Efficacy and safety of inhibiting the NLRP3/IL-1β/IL‐6 pathway in patients with ST‐elevation myocardial infarction: a meta‐analysis. Eur J Clin Invest. 2023;53(11):e14062.
Jayedi A, et al. Inflammation markers and risk of developing hypertension: a meta-analysis of cohort studies. Heart. 2019;105(9):686–92.
Page MJ, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. 2021;88:105906.
Gotschall T. EndNote 20 desktop version. J Med Libr Association: JMLA. 2021;109(3):520.
McHugh ML. Interrater reliability: the kappa statistic. Biochemia Med. 2012;22(3):276–82.
Wells GA et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. 2000, Oxford.
Wan X, et al. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14:1–13.
Group GW. Grading of recommendations assessment, development and evaluation (GRADE). 2012.
Faria SS et al. The neutrophil-to-lymphocyte ratio: a narrative review. Ecancermedicalscience, 2016. 10.
Dong C-H, Wang Z-M, Chen S-Y. Neutrophil to lymphocyte ratio predict mortality and major adverse cardiac events in acute coronary syndrome: a systematic review and meta-analysis. Clin Biochem. 2018;52:131–6.
Zhang S, et al. Predictive value of neutrophil to lymphocyte ratio in patients with acute ST segment elevation myocardial infarction after percutaneous coronary intervention: a meta-analysis. BMC Cardiovasc Disord. 2018;18(1):1–8.
Liu Z, et al. The prognostic value of elevated perioperative neutrophil-lymphocyte ratio in predicting postoperative atrial fibrillation after cardiac surgery: a systematic review and meta-analysis. Heart Lung Circulation. 2020;29(7):1015–24.
Tan TP, et al. Neutrophil–lymphocyte ratio as predictor of mortality and morbidity in cardiovascular surgery: a systematic review. ANZ J Surg. 2015;85(6):414–9.
Wang X, et al. Prognostic value of neutrophil to lymphocyte ratio in heart failure patients. Clin Chim Acta. 2018;485:44–9.
Etulain J. Platelets in wound healing and regenerative medicine. Platelets. 2018;29(6):556–68.
Dasgupta R, et al. Platelet-lymphocyte ratio as a novel surrogate marker to differentiate thyrotoxic patients with graves disease from subacute thyroiditis: a cross-sectional study from South India. Endocr Pract. 2020;26(9):939–44.
Özdemir E et al. Correlation between the severity of coronary artery ectasia and monocyte/lymphocyte, platelet/lymphocyte, and HDL/LDL ratios 2020.
Qiu Z, et al. Relationship between platelet to lymphocyte ratio and stable coronary artery disease: meta-analysis of observational studies. Angiology. 2020;71(10):909–15.
Dong G, Huang A, Liu L. Platelet-to‐lymphocyte ratio and prognosis in STEMI: a meta‐analysis. Eur J Clin Invest. 2021;51(3):e13386.
Wang Q, et al. Prognostic value of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in acute pulmonary embolism: a systematic review and meta-analysis. Int Angiol. 2017;37(1):4–11.
Willim HA, Harianto JC, Cipta H. Platelet-to-lymphocyte ratio at admission as a predictor of in-hospital and long-term outcomes in patients with St-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention: a systematic review and meta-analysis. Cardiol Res. 2021;12(2):109.
Li W, Liu Q, Tang Y. Platelet to lymphocyte ratio in the prediction of adverse outcomes after acute coronary syndrome: a meta-analysis. Sci Rep. 2017;7(1):1–9.
Meng X, et al. Determinant roles of gender and age on SII, PLR, NLR, LMR and MLR and their reference intervals defining in Henan, China: a posteriori and big-data‐based. J Clin Lab Anal. 2018;32(2):e22228.
Bahadır A, et al. Is the neutrophil-to-lymphocyte ratio indicative of inflammatory state in patients with obesity and metabolic syndrome? Anatol J Cardiol. 2015;15(10):816.
Tousoulis D, et al. Vascular cell adhesion molecule-1 and intercellular adhesion molecule‐1 serum level in patients with chest pain and normal coronary arteries (syndrome X). Clin Cardiol. 2001;24(4):301–4.
Arroyo-Espliguero R, Kaski JC. Microvascular dysfunction in cardiac syndrome X: the role of inflammation. CMAJ. 2006;174(13):1833–1833.
Taqueti VR, Ridker PM. Inflammation, coronary flow reserve, and microvascular dysfunction: moving beyond cardiac syndrome X. 2013, American College of Cardiology Foundation Washington, DC. pp. 668–671.
Li J-J, et al. Inflammation: a possible pathogenic link to cardiac syndrome X. Med Hypotheses. 2006;66(1):87–91.
Lanza GA. Cardiac syndrome X: a critical overview and future perspectives. Heart. 2007;93(2):159–66.
Acknowledgements
We would like to thank all those who have helped in carrying out the research, particularly Amirhossein Maleki from Shiraz University of Medical Sciences, Shiraz, Iran.
Funding
No funding was received to undertake this systematic review.
Author information
Authors and Affiliations
Contributions
ShKh contributed to the conception of the study and performed the data analyses; ShS searched the articles and reviewed all identified articles for eligibility; PA reviewed all identified articles for eligibility; SAN assessed the quality of studies; AGh reviewed all identified articles for eligibility; MKh assessed the quality of studies; BLW wrote the manuscript; HB Assisted in judging disputed articles; JC wrote the manuscript; NJ helped perform the analysis with constructive discussions. Y.Z and M.A.D helped in the revision process.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised: the affilaition of Yuexia Zhao has been updated.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhao, Y., Ghaedi, A., Azami, P. et al. Inflammatory biomarkers in cardiac syndrome X: a systematic review and meta-analysis. BMC Cardiovasc Disord 24, 276 (2024). https://doi.org/10.1186/s12872-024-03939-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-024-03939-3