
Abstract
Objective
Postoperative delirium is a common and debilitating complication that significantly affects patients and their families. The purpose of this study is to investigate whether there is an effective sedative that can prevent postoperative delirium while also examining the safety of using sedatives during the perioperative period.
Methods
The net-meta analysis was used to compare the incidence of postoperative delirium among four sedatives: sevoflurane, propofol, dexmedetomidine, and midazolam. Interventions were ranked according to their surface under the cumulative ranking curve (SUCRA).
Results
A total of 41 RCT studies involving 6679 patients were analyzed. Dexmedetomidine can effectively reduce the incidence of postoperative delirium than propofol (OR 0.47 95% CI 0.25–0.90), midazolam (OR 0.42 95% CI 0.17-1.00), normal saline (OR 0.42 95% CI 0.33–0.54) and sevoflurane (OR 0.39 95% CI 0.18–0.82). The saline group showed a significantly lower incidence of bradycardia compared to the group receiving dexmedetomidine (OR 0.55 95% CI 0.37–0.80). In cardiac surgery, midazolam (OR 3.34 95%CI 2.04–5.48) and normal saline (OR 2.27 95%CI 1.17–4.39) had a higher rate of postoperative delirium than dexmedetomidine, while in non-cardiac surgery, normal saline (OR 1.98 95%CI 1.44–2.71) was more susceptible to postoperative delirium than dexmedetomidine.
Conclusion
Our analysis suggests that dexmedetomidine is an effective sedative in preventing postoperative delirium whether in cardiac surgery or non-cardiac surgery. The preventive effect of dexmedetomidine on postoperative delirium becomes more apparent with longer surgical and extubation times. However, it should be administered with caution as it was found to be associated with bradycardia.
Similar content being viewed by others


Introduction
Postoperative delirium, also known as postoperative cognitive dysfunction (POCD), refers to delirium that occurs after surgery and is a common complication with an incidence rate of 70% [1,2,3]. It typically manifests 1–3 days after surgery and can last up to 2–5 days. While it can be completely relieved in most cases, recent studies suggest a strong association between postoperative delirium and the development of long-term cognitive and non-cognitive diseases [4], including post-traumatic stress disorder [5]. Moreover, postoperative delirium can lead to prolonged hospitalization, increased hospitalization costs, reduced quality of life, and increased mortality and complications [6], which poses a significant burden to both society and families. The incidence of delirium is higher in the elderly population, and with an aging population, postoperative cognitive dysfunction has become an increasingly hot topic [7,8,9]. Currently, there is no clear treatment for postoperative delirium, and it is generally managed through symptomatic treatment and the use of sedative adjuvants. Although some progress has been made in the diagnosis and treatment of the disease [10,11,12], there is still much debate surrounding the prevention of postoperative delirium.
Some researchers argue that sedatives, such as midazolam, may be a contributing factor in postoperative delirium [13, 14]. However, the article suggests that dexmedetomidine can help to prevent postoperative delirium [15], although the effects on circulation and heart rate remain a controversial issue. Previous studies have shown that the use of propofol and sevoflurane for preventing postoperative delirium has produced mixed results [16,17,18,19]. Given the variety of sedatives available to anesthesiologists, it is crucial to choose the appropriate one that can minimize the risk of postoperative delirium.
A meta-analysis is a powerful tool that can overcome the limitations of sample size in individual studies. Net meta-analysis takes this approach one step further by comparing different interventions through the combination of direct and indirect evidence, ultimately ranking them to identify the most effective treatment measures. The purpose of our study was to evaluate the preventive effects of four commonly used anesthetic drugs, including sevoflurane, propofol, dexmedetomidine, and midazolam, on postoperative delirium. By synthesizing the available evidence, we aimed to provide a comprehensive and robust evaluation of the relative efficacy and safety of these anesthetic drugs in preventing postoperative delirium.
Methods
Eligibility standards
To ensure the rigor and reliability of our analysis, we followed the guidelines and recommendations of PIRIMA (Preferred Reporting Items for systematic reviews and meta-Analyses). The registration ID of PROSPERO is CRD42023426641.
The studies were deemed eligible for inclusion in this review only if they met the specific criteria established for this study:
-
(a)
population: we restricted our study to adult patients aged 18 years or older and excluded studies involving individuals with pre-existing brain diseases, dementia, delirium, cerebral infarction, or cerebral ischemia.
-
(b)
intervention: comparison between dexmedetomidine, sevoflurane, midazolam, and propofol, saline group. the experimental group treated with placebo or one of the the three drugs can be used as a control group. Other drugs are not included.
-
(c)
outcome: The primary outcome measure of our review was the incidence of postoperative delirium. To control for potential confounding factors, we limited our analysis to cases where delirium was diagnosed within seven days of surgery. Only studies that utilized reliable tools for diagnosing delirium, such as the Confusion Assessment Method (CAM), Mini-Mental State Examination (MMSE), Nursing Delirium Screening Scale (Nu-DESC scoring), Delirium Rating Scale (DRS), and Memorial Delirium Assessment Scale were included in our review.
-
(d)
study design: studies were RCT studies.
Search strategy
We conducted a comprehensive search on multiple databases, including PubMed, EMBASE, and Cochrane Central, for relevant literature published before the end of december 2022. Using the search terms: the Subject words and free words of postoperative delirium AND dexmedetomidine OR propofol OR sevoflurane OR midazolam. During the full-text screening process, non-random experiments are typically excluded as they may have a higher risk of selection bias and thus may affect the reliability and generalizability of study outcomes. By adopting a rigorous and systematic approach to data collection, we aimed to reduce the risk of selection bias and enhance the validity of our findings.
Study selection
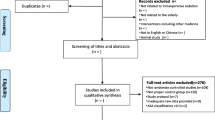
To manage the literature search process, we utilized EndNote X9 software to import and automatically remove any duplicate documents. We then organized and screened the articles based on our predetermined criteria. Case reports, letters, and records of meetings were excluded. There are two independent authors (Hjx and Zss). They performed literature searches, read titles and abstracts, and screened full texts independently, without communication with each other. If there were discrepancies or differences of opinion between the two authors, they discussed and resolved them through consensus. In cases where consensus could not be reached, a third author (Wss) was consulted to make the final decision. The flowchart of the search strategy is in Fig. 1.

The flowchart of the searching strategy
Data extraction
In our meta-analysis, two investigators (Hjx and Zss) collected and analyzed a range of data from the literature independently, including the first author’s name, publication year, patient age, sample size, study type, type of operation, timing, and duration of medication, treatment plan, method of delirium evaluation, the incidence of delirium, operation time, extubation time, and incidence of hypotension and low heart rate. By examining this wide range of variables, we aimed to conduct a comprehensive evaluation of the effects of different anesthetic drugs on postoperative delirium.
Definition of outcomes
We considered the incidence of postoperative cognitive dysfunction (POCD) as the primary index, and the incidence of hypotension, sinus bradycardia, operation time, and extubation time as secondary indicators. Hypotension was defined as a systolic blood pressure lower than 90 mmHg or diastolic blood pressure lower than 60 mmHg, while sinus bradycardia was defined as a heart rate less than 60 beats per minute.
Assessment of risk of bias
Randomized controlled trials (RCTs), considered the gold standard for verifying the effectiveness of interventions, are an integral part of producing high-quality meta-analyses. To further ensure the quality of the studies included in our meta-analysis, we utilized the Cochrane Risk of Bias (ROB) tool-2 to evaluate the risk of bias in each study. Five domains for assessing the risk of bias: random sequence generation, allocation concealment, blinding, incomplete outcome data, and selective reporting. Bias risk assessment: high, medium, or low risk of bias is assigned for each assessment item, and bias risk messages are generated accordingly. This evaluation was conducted independently by two authors (Hjx and Zss), to reduce the potential for bias in the assessment process.
Statistic analysis
For continuous variables in the outcome index, we expressed them as mean ± standard deviation. However, if the variable is expressed as median (interquartile range), and the sample size is large enough and close to the normal distribution, we can treat the median as the mean, and calculate the standard deviation by taking the quartile range and dividing it by 1.35 For dichotomous variables, we extracted the number of occurrences and the total number of the sample.
We used I2 and p-value to estimate the statistical difference, where I2 > 50%, and p < 0.05, were considered significant heterogeneity using STATA (version 15). We created interval diagrams for all comparative and predictive confidence intervals and objectively assessed each variable using a network graph. To evaluate potential discrepancies between direct and indirect comparisons, we compared loop inconsistencies in our analysis. we also used the node splitting method and consistency model to test for consistency.
We sorted the intervention measures, and the area under the curve indicates the level of the intervention. The effect of treatment of interventions is ranked according to the area under the curve ranking SUCRA. To evaluate publication bias, we used a funnel plot.
Results
Study selection
As shown in Fig. 1, we initially identified a total of 4012 articles from three databases (PubMed, Cochrane, and EMBASE). After excluding 442 duplicates, 2059 irrelevant studies, 577 studies on other topics, 234 animal experiments, 10 non-English studies, and 604 abstracts, letters, or conference proceedings, we proceeded with the full-text screening of the remaining 86 articles.
Out of the 86 articles, we excluded 7 studies that did not involve general anesthesia, 11 that were not RCTs, 15 that did not report the incidence of delirium, 4 that had incomplete data, and 8 that were limited to a specific age group. Finally, out of the 41 studies that met the inclusion criteria, we conducted our meta-analysis.
Study characteristics
As presented in (PS: Table 1), the studies included in our meta-analysis were published between 2014 and 2022. Among the 41 studies, 12 were focused on cardiac surgery, 28 were focused on non-cardiac surgery, and 1 study included both cardiac and non-cardiac surgery. Furthermore, 6 studies were conducted in the ICU, 33 studies were conducted in the OR, and 2 studies included both OR and ICU settings. Figure 2 displays the network plot.

network plot: The relationship between delirium incidence and the overall structure of a network can be described as network geometry
Risk of bias within studies
In our assessment, we identified two studies as high-risk [20, 21], and we determined that two studies posed a potentially high risk of bias. One study lacked sufficient information regarding the implementation of a double-blind procedure. The other study reported that anesthesiologists and nurses were not blinded due to the need to adjust the timing and dosage of dexmedetomidine. In addition, we considered five studies to have a medium risk of bias [22,23,24,25,26]. The researchers and subjects may not be double-blind and There is no mention of whether there was an appropriate analysis used to estimate the effect of assignment to intervention (Fig. 3).

Literature quality evaluation Document quality is evaluated using ROB-2
Synthesis of results
Incidence of postoperative delirium and postoperative cognitive dysfunction
The pairwise comparison interval diagram (Fig. 4) presents the comparison of several interventions in terms of their effectiveness in reducing postoperative delirium and postoperative cognitive dysfunction. The diagram shows that midazolam (OR 2.40; 95% CI 1.00 to 5.79), propofol (OR 2.12; 95% CI 1.11 to 4.05), sevoflurane (OR 2.58; 95% CI 1.22 to 5.46), and saline(OR 2.36 95%CI 1.85–3.01) are less effective in reducing postoperative delirium and postoperative cognitive dysfunction when compared to dexmedetomidine. A league chart (PS Fig. 1) is also provided for further information. We have summarized a forest plot comparing multiple drugs (PS Fig. 2).

The pairwise comparison interval diagram. the comparison of several interventions in terms of their effectiveness in reducing postoperative delirium and Postoperative cognitive dysfunction
Extubation time
Several factors have been identified as potential risk factors for postoperative delirium, and the duration of extubation is one such factor. propofol was found to have a higher likelihood of causing postoperative delirium and prolonged extubation time when compared to dexmedetomidine (MD 350.58 95% CI 323.78-377.38), midazolam (MD 344.28 95%CI 316.98-371.57), and normal saline (MD 351.21 95% CI 324.32–378.10). sevoflurane with a higher incidence of postoperative delirium with longer extubation times when compared to dexmedetomidine (MD 349.58 95% CI 322.27-376.88), midazolam (MD 343.28 95% CI 315.49-371.07), physiological saline (MD 350.21 95% CI 322.82–377.60).
Operation time
A total of 30 articles were included in the study, comprising 4924 participants. Operation time is also one of the causes of delirium, but affected by many other factors, there is no significant difference in the effect of different operation times and drugs on postoperative delirium.
Results of subgroup analyses
Operation time
To identify subgroups of patients who may benefit more from measures aimed at preventing postoperative delirium, the study participants were divided into two groups based on whether their surgery lasted longer or shorter than three hours.
Operation time < 3 h
The incidence of postoperative delirium was significantly lower among patients who underwent surgery lasting less than three hours when received dexmedetomidine (OR 2.74 95% 1.48–5.05) compared to those who received normal saline as part of the anesthesia regimen.
Operation time > 3 h
When surgical procedures lasted longer than three hours, it was found that the preventative effect of administering dexmedetomidine to reduce the incidence of postoperative delirium was significantly better than that of using another part of the anesthesia regimen (PS Fig. 3).
Extubation time
We categorized extubation time into less than 1 h and more than 5 h.
Extubation time < 1 h
It was observed that administering dexmedetomidine within the first hour after surgery was better than the usage of midazolam (OR 15.55 95%CI 1.11-218.13) and normal saline (OR 3.48 95%CI 1.75–6.94) preventing postoperative delirium.
Extubation time > 5 h
when extubation time exceeded 5 h, the use of propofol (OR 2.20 95% 1.23–3.93) and normal saline (OR 2.63 95%CI 1.09–6.31) was found to be less effective compared to the usage of dexmedetomidine in preventing postoperative delirium.
Type of surgery
During our study, we divided participants into cardiac and non-cardiac groups.
Cardiac surgery
Among the cardiac group, a total of 12 articles were included in the study and 4 drugs were compared (propofol, sevoflurane, dexmedetomidine, saline). it was observed that patients who received midazolam (OR 3.34 95%CI 2.04–5.48) and normal saline (OR 2.27 95%CI 1.17–4.39) were more likely to develop postoperative delirium compared to those who received dexmedetomidine.
Non-cardiac surgery
A total of 28 articles were included in the study, which compared 5 drugs. Our findings suggest that the use of normal saline in cardiac surgery is more likely to contribute to postoperative delirium compared to the usage of dexmedetomidine (OR 1.98 95%CI 1.44–2.71).
Results of secondary indicators
Bradycardia was reported in 12 articles that included a total of 1831 participants. The incidence rate of bradycardia was significantly lower in the saline group compared to the dexmedetomidine group (OR 0.55, 95% CI 0.37 to 0.80). However, no significant difference was observed in the incidence of heart rate among other sedatives.
Out of the 41 articles analyzed, only 12 contained records of hypotension. The rates of hypotension for several drugs were not found to be statistically significant.
SUCRA probability ranking
According to the Ranking Probabilities Diagram (Fig. 5), dexmedetomidine was ranked the highest among all the interventions, indicating that it may be the most effective among the drugs studied. The SUCRA indices were found dexmedetomidine (98.8%) > Propofol (51.4%) > saline (37.2%) > Midazolam (36.4%) > Sevoflurane (26.2%), indicating that dexmedetomidine has the highest probability of being the most effective intervention for reducing the incidence of postoperative delirium.

The Ranking Probabilities Diagram. The product map under the curve is also shown in the figure. A larger area under the curve indicates a greater possibility of the best pre-measures. Abbreviations used in the chart include Dex for Dexmedetomidine, Mid for Midazolam, N for Saline, Pro for Propofol, and Sev for Sevoflurane
Publication bias
We used funnel plots to compare the differences in the mean changes of all outcome measures between the treatment group and the placebo group. The majority of the scatter points in all funnel plots were located on both sides of the vertical line. The funnel plot (Fig. 6) shows that the distribution of each study is roughly symmetrical, which suggests the absence of publication bias or other forms of bias.

The funnel plot. a funnel chart shows that the distribution of each study is roughly symmetrical
the effect OR is plotted on the abscissa, while the reciprocal 1/SE (log OR) of the standard error of the effect is plotted on the ordinate. The dotted lines perpendicular to the horizontal axis represent the combined effect, and the dotted lines on both sides of the chart represent the 95% confidence interval
Acronym:
(Dex): dexmedetomidine; (Mid): midazolam; (N): saline; (Pro): propofol; (Sev): sevoflurane;
A:(Dex):dexmedetomidine; B:(Mid):midazolam; C:(N):saline; D:P(Pro):propofol; E(Sev):sevoflurane;
Comparison of consistency and heterogeneity
The following Stata code “network meta I (P = 0.18 P > 0.05)” indicates that a consistency model can be applied for the analysis. Additionally, the results of the node splitting map (PS Fig. 4) indicate that there is no apparent local inconsistency for both direct and indirect comparisons(all P > 0.05), demonstrating the absence of significant heterogeneity. In The ring inconsistency (PS Fig. 5), midazolam, propofol, and sevoflurane were compared with each other regarding their ability to undergo cyclization (P > 0.05), dexmedetomidine, midazolam, and propofol have the ability to form a ring structure through cyclization (P > 0.05), test also verifies that there is no obvious inconsistency between direct comparison and indirect comparison.
Discussion
The incidence of postoperative delirium with dexmedetomidine was found to be lower than that of a placebo, propofol, sevoflurane, and midazolam, regardless of whether the extubation time was longer than 1 or 5 h, the operation time was less than 3 h or more than 3 h, or whether the surgery was cardiac or non-cardiac. This indicates that dexmedetomidine has a positive effect on preventing postoperative delirium. However, it should be noted that dexmedetomidine carries a higher risk of reducing heart rate than normal saline. Therefore, it is necessary to closely monitor heart rate when using dexmedetomidine and discontinue the drug promptly if necessary.
Our analysis supports previous research and guidelines [27], indicating that dexmedetomidine can play a positive role in preventing postoperative delirium [28, 29]. A large randomized study showed that dexmedetomidine does not reduce the incidence of postoperative delirium. It is possible that other side effects, such as hypotension, could contribute to the occurrence of postoperative delirium. Therefore, the conclusion can be drawn that there is no significant difference in the rate of postoperative delirium between the dexmedetomidine group and the normal group. Furthermore, it is important to acknowledge that postoperative delirium can be caused by multiple factors, which necessitates a comprehensive and dialectic evaluation. dexmedetomidine functions by inhibiting the release of norepinephrine through the activation of α2 receptors in the brain, which reduces the excitability of neurons and enhances the inhibitory effect of γ-aminobutyric acid (GABA). This mechanism can provide analgesic effects, relax patients, and reduce anxiety [30]. Dexmedetomidine can also improve postoperative sedation and sleep quality, and reduce sensory perception, nerve exhaustion, and stress response, promoting better patient recovery [31]. Finally, dexmedetomidine may have a positive effect on the prevention of postoperative delirium by regulating the inflammatory response and metabolic activity of neurons in the brain, thus exerting anti-inflammatory and neuroprotective effects [20, 32]. Therefore, the use of dexmedetomidine is effective in preventing postoperative delirium.
Our analysis found that compared to saline, midazolam, sevoflurane, and propofol, dexmedetomidine is more likely to cause bradycardia, but there was no significant difference in the incidence of hypotension among all sedatives. We identified 12 articles reporting bradycardia and 12 articles reporting hypotension among the total of 41 articles included in our analysis. However, due to the limited number of articles available on hypotension and bradycardia, we do not have sufficient evidence to establish the differences between different sedatives. Clinicians should consider the potential side effects when administering drugs to patients.
According to some guidelines, the duration of surgical procedures is recognized as one of the factors that affect the occurrence of postoperative delirium. However, different studies appear to have arrived at varying conclusions regarding the specific length of time required to increase the risk of developing this condition [33]. Some studies have suggested that the rate of postoperative delirium increases significantly if the surgical procedure takes more than 2 h [34], while others suggest that the threshold could be 3, 4, or even 5 h [35,36,37]. In our study, we observed that when the duration of surgery exceeded three hours, administering dexmedetomidine had a significantly greater effect in preventing postoperative delirium compared to the other anesthesia regimen. The incidence of postoperative delirium was significantly reduced in surgeries lasting less than three hours, where patients were administered dexmedetomidine compared to the usage of normal saline as part of the anesthesia regimen. The specific duration and threshold for postoperative delirium risk may depend on factors such as the type and location of surgery, the patient’s health status, and anesthesia-related factors. Therefore, clinicians need to consider various risk factors carefully for each patient and surgical procedure to minimize the risk of postoperative delirium.
Extubation is the process of removing a breathing tube that is inserted into a patient’s airway during surgery to help them breathe. The longer the duration of extubation (the amount of time the breathing tube is in place), the higher the risk of postoperative delirium [38, 39]. This is because the tube can cause irritation and inflammation in the airways, which can trigger an inflammatory response in the body that can lead to cognitive issues [40, 41]. A study looked at the relationship between extubation duration and postoperative delirium in elderly patients undergoing cardiopulmonary bypass. The study found that patients who had a longer duration of extubation were more likely to develop postoperative delirium, compared to patients who had a shorter duration of extubation. Our study found that the extubation time for patients who received propofol and sevoflurane was longer compared to those who received dexmedetomidine, midazolam, and normal saline. Previous studies have demonstrated that the use of dexmedetomidine in intubated patients has a sedative effect, reducing restlessness and preventing postoperative delirium [42,43,44,45]. Our study further supports this finding, as we observed a positive effect of dexmedetomidine in preventing postoperative delirium regardless of the length of intubation.
Numerous studies have demonstrated that the use of dexmedetomidine can decrease the incidence of postoperative delirium [16, 46,47,48], although a few have reported otherwise [49, 50]. Postoperative delirium is associated with various factors such as the type of operation, age, the patient’s overall health status, excessive blood loss, and abnormal liver and kidney function. While dexmedetomidine has primarily been studied in the context of cardiac surgery, some research has shown that it can also be effective in preventing postoperative delirium in non-cardiac surgical procedures [51,52,53,54]. Our study provides further evidence in support of dexmedetomidine’s effectiveness, finding that it can reduce the incidence of postoperative delirium not only after cardiac surgery but also after non-cardiac surgical procedures.
This study has several strengths. First, this meta-analysis updates results from clinical studies over the past two years, thus several recently published, large-scale, and high-quality RCTs have been included. Second, to increase the credibility of the study, our study excluded clinical experiments with the number of participants in each group being less than 20. Finally, we also increased the effect of intubation time and operation time on postoperative delirium.
Our net-meta analysis has some limitations that need to be addressed. Firstly, some studies have smaller sample sizes, with only 40 subjects, which could affect the generalizability of the findings. Secondly, we only compared four sedatives, while there are likely more than four drugs used in clinical settings. Thirdly, postoperative delirium is multi-factorial and can be influenced by several variables such as age, type of operation, operation time, and intraoperative medication. Our analysis did not consider these factors. Lastly, the scale of postoperative delirium is subjective, which could influence the accuracy of the results.
Conclusion
In conclusion, our findings suggest that dexmedetomidine has a positive effect in preventing postoperative delirium. However, the limitations of our analysis in terms of the literature included and the impact of dexmedetomidine on heart rate should be considered carefully when making clinical decisions. Besides, it is important for clinicians to carefully monitor the duration of extubation and operation and consider strategies to minimize the duration of intubation when possible, especially in older patients who are at higher risk for postoperative delirium. This may include optimizing pain control, managing anxiety and agitation, and providing supportive care to minimize irritation and inflammation in the airways. Moving forward, we hope to discover more drugs that can effectively prevent postoperative delirium.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
Watne LO, et al. Increased CSF levels of aromatic amino acids in hip fracture patients with delirium suggests higher monoaminergic activity. BMC Geriatr. 2016;16:149.
Saleh AJ, et al. Preoperative cognitive intervention reduces cognitive dysfunction in elderly patients after gastrointestinal surgery: a randomized controlled trial. Med Sci Monit. 2015;21:798–805.
Lin GX, et al. Serum high-mobility group box 1 protein correlates with cognitive decline after gastrointestinal surgery. Acta Anaesthesiol Scand. 2014;58(6):668–74.
Rengel KF, Pandharipande PP, Hughes CG. Special considerations for the aging brain and perioperative neurocognitive dysfunction. Anesthesiol Clin. 2019;37(3):521–36.
Saczynski JS, et al. Cognitive trajectories after postoperative delirium. N Engl J Med. 2012;367(1):30–9.
de la Varga-Martínez O et al. Development and validation of a delirium risk prediction preoperative model for cardiac surgery patients (DELIPRECAS): an observational multicentre study. J Clin Anesth. 2021;69.
Leslie DL, Inouye SK. The importance of delirium: economic and societal costs. J Am Geriatr Soc. 2011;59(Suppl 2):S241–3.
Al Tamimi L, et al. Intraoperative xenon for prevention of delirium after on-pump cardiac surgery: a randomized, observer-blind, controlled clinical trial. Br J Anaesth. 2020;124(4):454–62.
Al-Radeef MY, et al. Comparing the effect of dexamethasone, normal saline, and metoclopramide on prevention of postoperative nausea, vomiting, and pain in a patient undergoing laparoscopic cholecystectomy or open appendectomy: a randomized clinical trial. Open Access Macedonian J Med Sci. 2020;8(B):139–44.
Campbell AM, et al. Melatonin for the prevention of postoperative delirium in older adults: a systematic review and meta-analysis. BMC Geriatr. 2019;19(1):272.
Yoshitaka S, et al. Association of plasma melatonin levels with delirium after general anesthesia. J Neurosurg Anesthesiol. 2012;24(4):514–5.
Konkayev AK, Bekmagambetova NV. Comparison of sedation with dexmedetomidine and haloperidol in patients with delirium after femoral neck fractures. Anesteziol Reanimatol. 2015;60(1):8–11.
Aydogan MS, et al. Pain, fentanyl consumption, and delirium in adolescents after scoliosis surgery: dexmedetomidine vs midazolam. Pediatr Anesth. 2013;23(5):446–52.
Mansouri N, Nasrollahi K, Shetabi H. Prevention of cognitive dysfunction after cataract surgery with intravenous administration of midazolam and dexmedetomidine in elderly patients undergoing cataract surgery. Adv Biomed Res. 2019;8:6.
Chen J, Yan J, Han X. Dexmedetomidine may benefit cognitive function after laparoscopic cholecystectomy in elderly patients. Experimental Therapeutic Med. 2013;5(2):489–94.
Djaiani G, et al. Dexmedetomidine versus propofol sedation reduces delirium after cardiac surgery: a randomized controlled trial. Anesthesiology. 2016;124(2):362–8.
Duan GY, et al. Cognitive function and delirium following sevoflurane or propofol anesthesia for valve replacement surgery: a multicenter randomized controlled trial. Kaohsiung Journal of Medical Sciences. 2022.
Guo L, et al. Impact of sevoflurane versus propofol anesthesia on post-operative cognitive dysfunction in elderly cancer patients: a double-blinded randomized controlled trial. Med Sci Monit. 2020;26:e919293.
Li WX, et al. Effects of propofol, dexmedetomidine, and midazolam on postoperative cognitive dysfunction in elderly patients: a randomized controlled preliminary trial. Chin Med J. 2019;132(4):437–45.
Lee C, et al. The effect of the timing and dose of dexmedetomidine on postoperative delirium in elderly patients after laparoscopic major non-cardiac surgery: a double-blind randomized controlled study. J Clin Anesth. 2018;47:27–32.
Tang S, et al. Comparison of effects of propofol versus sevoflurane for patients undergoing cardiopulmonary bypass cardiac surgery. Pakistan J Med Sci. 2019;35(4):1072–5.
Xu G, et al. Effects of dexmedetomidine on postoperative cognitive dysfunction and serum levels of β-amyloid and neuronal microtubule-associated protein in orthotopic liver transplantation patients. Ann Transplant. 2016;21:508–15.
Gao Y, et al. Effect of dexmedetomidine on the neuroglobin expression in elderly patients with minimally invasive coronary artery bypass graft surgery. Heart Surg Forum. 2021;24(5):pE776–E780.
Li Z et al. Effects of dexmedetomidine doses on postoperative cognitive dysfunction and serum β- amyloid and cytokine levels in elderly patients after spine surgery: a randomized controlled trial. Nan Fang Yi Ke Da Xue Xue bao [Journal of Southern Medical University]. 2021;41(4):600–6.
Mengmeng Liu XX, Li H, Qi F. The effects of dexmedetomidine in general anesthesia on the perioperative hemodynamics and postoperative cognitive functions of patients with sleep apnea syndrome in the perioperative period of uvulopalatopharyngoplasty. Int J Clin Exp Med. 2020;13(3).
MIcha g, zalonIs PtI, KotsIs K, Papadopoulos g, arnaoutoglou E. Propofol vs sevoflurane anesthesia on postoperative cognitive dysfunction in the elderly. A randomized controlled trial. Acta Anaesth Belg. 2016;67:129–37.
Aldecoa C, et al. European society of anaesthesiology evidence-based and consensus-based guideline on postoperative delirium. Eur J Anaesthesiol. 2017;34(4):192–214.
Wang L, et al. Comparison of intranasal dexmedetomidine and oral midazolam for premedication in pediatric dental patients under general anesthesia: a randomised clinical trial. Biomed Res Int. 2020;2020:5142913.
Zhao J et al. Prevention of dexmedetomidine on postoperative delirium and early postoperative cognitive dysfunction in elderly patients undergoing thoracoscopic lobectomy. Evidence-based complementary and alternative medicine, 2022. 2022.
Funai Y, et al. Systemic dexmedetomidine augments inhibitory synaptic transmission in the superficial dorsal horn through activation of descending noradrenergic control: an in vivo patch-clamp analysis of analgesic mechanisms. Pain. 2014;155(3):617–28.
Joseph A, Giovannitti J, DMD,* Sean M, Thoms DMD, MS,†, Crawford JJ. Alpha-2 adrenergic receptor agonists: a review of current clinical applications. Anesth Prog. 2015;62(1):31–9.
Skvarc DR, et al. Post-operative cognitive dysfunction: an exploration of the inflammatory hypothesis and novel therapies. Neurosci Biobehav Rev. 2018;84:116–33.
Zhang G, et al. A systematic review and meta-analysis of the correlation between operation time and postoperative delirium in total hip arthroplasty. Ann Palliat Med. 2021;10(10):10459–66.
Song KJ, et al. Etiology and related factors of postoperative delirium in orthopedic surgery. Clin Orthop Surg. 2019;11(3):297–301.
Andrasi TB et al. Risk factors for postoperative delirium after cardiac surgical procedures with cardioplegic arrest. Eur J Cardiothorac Surg. 2022;62(1).
Seo JS, et al. Risk factors for delirium after spine surgery in elderly patients. J Korean Neurosurg Soc. 2014;56(1):28–33.
Oh Y-S. Hyoung-Joon Chun, and Hyeong-Joong Yi. Incidence and risk factors of acute postoperative delirium in geriatric neurosurgical patients. J Korean Neurosurg Soc. 2008;43:143–8.
Shirvani F, Sedighi M, Shahzamani M. Metabolic disturbance affects postoperative cognitive function in patients undergoing cardiopulmonary bypass. Neurol Sci. 2022;43(1):667–72.
Hu XY, et al. Automated machine learning-based model predicts postoperative delirium using readily extractable perioperative collected electronic data. CNS Neurosci Ther. 2022;28(4):608–18.
Poyrazoglu HH, et al. Investigating the impacts of preoperative steroid treatment on tumor necrosis factor-alpha and duration of extubation time underwent ventricular septal defect surgery. Balkan Med J. 2016;33(2):158–63.
Zhang J, et al. Effects of three anesthesia methods on inflammation, oxidative stress, analgesia and cognition in elderly patients receiving hip replacement. Cell Mol Biol (Noisy-le-grand). 2022;68(2):103–8.
Johannes G, Schuderer LR, Wunschel M, Spanier G, Spoerl S, Gottsauner MJ, Maurer M, Meier JK, Peter Kummer, T Orsten E. Reichert and T obias Ettl. Elective T racheotomy in patients receiving mandibular reconstructions: reduced postoperative V entilation time and lower incidence of hospital-acquired pneumonia. Clin Med. 2023;12(883):2–14.
Shokri H, Ali I. A randomized control trial comparing prophylactic dexmedetomidine versus clonidine on rates and duration of delirium in older adult patients undergoing coronary artery bypass grafting. J Clin Anesth. 2020;61:109622.
Park JB, et al. Efficacy and safety of dexmedetomidine for postoperative delirium in adult cardiac surgery on cardiopulmonary bypass. Korean J Thorac Cardiovasc Surg. 2014;47(3):249–54.
Chew WZ, et al. Bispectral index (BIS) monitoring and postoperative delirium in elderly patients undergoing surgery: a systematic review and meta-analysis with trial sequential analysis. J Cardiothorac Vasc Anesth. 2022;36(12):4449–59.
Heybati K, et al. Outcomes of dexmedetomidine versus propofol sedation in critically ill adults requiring mechanical ventilation: a systematic review and meta-analysis of randomized controlled trials. Br J Anaesth. 2022;129(4):515–26.
Liu X, et al. Dexmedetomidine vs propofol sedation reduces delirium in patients after cardiac surgery: a meta-analysis with trial sequential analysis of randomized controlled trials. J Crit Care. 2017;38:190–6.
Wu M, et al. Perioperative dexmedetomidine reduces delirium after cardiac surgery: a meta-analysis of randomized controlled trials. J Clin Anesth. 2018;50:33–42.
Patel M, Onwochei DN, Desai N. Influence of perioperative dexmedetomidine on the incidence of postoperative delirium in adult patients undergoing cardiac surgery. Br J Anaesth. 2022;129(1):67–83.
Turan A, et al. Dexmedetomidine for reduction of atrial fibrillation and delirium after cardiac surgery (DECADE): a randomized placebo-controlled trial. Lancet (London England). 2020;396(10245):177–85.
Lewis K, et al. Dexmedetomidine vs other sedatives in critically ill mechanically ventilated adults: a systematic review and meta-analysis of randomized trials. Intensive Care Med. 2022;48(7):811–40.
Shi M, et al. Dexmedetomidine for the prevention of emergence delirium and postoperative behavioral changes in pediatric patients with sevoflurane anesthesia: a double-blind, randomized trial. Drug Des Dev Therapy. 2019;13:897–905.
Tasbihgou SR, Barends CRM, Absalom AR. The role of dexmedetomidine in neurosurgery. Best Pract Research: Clin Anaesthesiol. 2021;35(2):221–9.
Xie K, et al. Postoperative infusion of dexmedetomidine via intravenous patient-controlled analgesia for prevention of postoperative delirium in elderly patients undergoing surgery. Aging Clin Exp Res. 2023;35(10):2137–44.
Funding
The research of our article was funded by the National Nature funding (No:82171265).
Author information
Authors and Affiliations
Contributions
Jin-Xiang Huang: This author helped design the study, retrieve the data, analyze the data, and draft the manuscript; Shan-shan Zhang: This author helped design the study, retrieve the data, analyze the data, and prepare the manuscript; Shu-xian Wang, Da-shuang, Fang-Ru Luo: This author helped design the study and retrieve the data; Cheng-jiang Liu: This author helped design the study and prepare the manuscript; Hong Li: This author helped conduct the study and draft the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This is a systematic review and meta-analysis, ethics approval and consent to participate are not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1:
PRISMA 2020 Checklist

Supplementary Material 2: PS Fig 1
the league chart provided for further information about in reducing postoperative delirium and Postoperative cognitive dysfunction in 5 drugs

Supplementary Material 3: PS Fig 2
the forest plot comparing multiple drugs

Supplementary Material 4: PS Fig 3
operation more than 3h. Comparison of the incidence of postoperative delirium among five drugs when the operation time is more than 3 hours

Supplementary Material 5: PS Fig 4
the ring inconsistency verifies that there is no obvious inconsistency between direct comparison and indirect comparison

Supplementary Material 6: PS Fig 5
the node splitting map indicate that there is no apparent local inconsistency for both direct and indirect comparisons
Supplementary Material 7: PS Table 1
the Study characteristics included in our meta-analysis were published between 2014 and 2022
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cite this article
Huang, JX., Zhang, SS., Wang, SX. et al. The role of perioperative sedative anesthetics in preventing postoperative delirium: a systematic review and network-meta analysis including 6679 patients. BMC Cardiovasc Disord 24, 147 (2024). https://doi.org/10.1186/s12872-024-03783-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-024-03783-5