
Abstract
Background
Patients with Heart failure (HF) commonly have a water-electrolyte imbalance due to various reasons and mechanisms, and hyponatremia is one of the most common types. However, currently, there are very few local studies on hyponatremia risk assessment in patients with acute decompensated heart failure (ADHF), and there is a lack of specific screening tools. The aim of this study is to identify a prediction model of hyponatremia in patients with acute decompensated heart failure (ADHF) and verify the prediction effect of the model.
Methods
A total of 532 patients with ADHF were enrolled from March 2014 to December 2019. Univariate and multivariate logistic regression analyses were performed to investigate the independently associated risk factors of hyponatremia in patients with ADHF. The prediction model of hyponatremia in patients with ADHF was constructed by R software, and validation of the model was performed using the area under the receiver operating characteristic curve (AUC) and calibration curves.
Results
A total of 65 patients (12.2%) had hyponatremia in patients with ADHF. Multivariate logistic regression analysis demonstrated that NYHA cardiac function classification (NYHA III vs II, OR = 12.31, NYHA IV vs II, OR = 11.55), systolic blood pressure (OR = 0.978), serum urea nitrogen (OR = 1.046) and creatinine (OR = 1.006) were five independent prognostic factors for hyponatremia in patients with ADHF. The AUC was 0.757; The calibration curve was near the ideal curve, which showed that the model can accurately predict the occurrence of hyponatremia in patients with ADHF.
Conclusions
The prediction model constructed in our study has good discrimination and accuracy and can be used to predict the occurrence of hyponatremia in patients with ADHF.
Similar content being viewed by others
Introduction
Heart failure (HF) is a clinical syndrome characterised by cardiomyocyte injury and structural and functional changes due to various reasons, which ultimately leads to ventricular blood pumping and (or) filling decline, thus failing to meet the body’s needs. Acute decompensated heart failure (ADHF) has emerged as a global public health problem owing to its high incidence rate, rehospitalisation rate and mortality [1,2,3]. Patients with HF commonly have a water-electrolyte imbalance due to various reasons and mechanisms, and hyponatremia is one of the most common types [4,5,6]. According to earlier reports [7,8,9,10,11], the hyponatremia incidence ranged between 7.2%–27% in inpatients with HF. Meanwhile, hyponatremia is independently associated with poor HF patient prognosis [12]. The incidence of adverse events also increases along with the increase in the degree of hyponatremia [13,14,15]. Therefore, it is of great significance to maintain blood sodium balance in patients with HF. There are presently a few local studies on hyponatremia risk assessment in ADHF patients. There is a lack of specific screening tools.
A nomogram is a widely used prognostic model that can intuitively reflect the predictive ability of prognostic factors based on the length of line segments. A nomogram can guide clinicians to make rapid and comprehensive judgments and help them make individualized clinical decisions [16]. We have performed a retrospective analysis of the patients with ADHF in a third-grade hospital. The large sample size of the hospital facilitated reliable research conclusions.
The present study was carried out to construct a risk prediction model by analysing the influential factors of hyponatremia in patients with ADHF. Our study is expected to provide nursing staff with specific screening tools for hyponatremia risk in patients with ADHF.
Materials and methods
Study population
The study participants were 590 patients who were admitted to a third-grade hospital for ADHF from March 2014 to December 2019. This study was approved by the ethics committee.
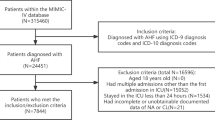
Inclusion criteria: patients with ADHF according to the definition in the Guidelines for diagnosis and treatment of HF [17]. Exclusion criteria: patients with malignancies, patients with cognitive impairment and dementia, patients with severe mental illness, patients with primary hepatic and renal failure and patients with other severe uncontrollable systemic diseases. Finally, we included 532 patients (Fig. 1).

Study flow chart
Definition of hyponatremia
The enrolled patients were divided into the normal blood sodium group (serum sodium ≥ 135 mmol/L) and the hyponatremia group (serum sodium < 135 mmol/L) [11] according to the results of the serum sodium test on the day of admission.
Covariates
The baseline data and serum samples were collected from the enrolled patients within 24 h after admission, associated with echocardiography completion and other instrumental examinations within 48 h. The following data were collected, including: (1) demographic data: name, age, gender, height and weight; (2) disease information: primary aetiology and comorbidities of HF (diabetes, hypertension, coronary heart disease, etc.); (3) laboratory examinations: albumin, creatinine, serum urea nitrogen, C-reactive protein, N-terminal pro-brain natriuretic peptide (NT-proBNP), etc.; and (4) instrumental examination: echocardiography.
Statistical analysis
SPSS 22.0 and R 3.6.0 were used for statistical analysis. Qualitative data were expressed in (%), and the chi-square test was used for inter-group comparison. Meanwhile, quantitative data were presented in the form of mean ± standard deviation (x ± s) or median (interquartile range), which were compared using an independent sample t-test or rank sum test between groups. Univariate logistic regression analysis was performed to analyse the potentially related hyponatremia factors. Multivariate logistic stepwise regression analysis was conducted to screen the independent related hyponatremia factor, during which indicators with P < 0.05 in univariate analysis were included in the model, and indicators with P > 0.05 in multivariate analysis were excluded from the model. Nomogram model drawing and internal validation adopted the R 3.6.0 software package. The receiver operating characteristic (ROC) curve was additionally drawn, and the area under the ROC curve (AUC) was calculated to identify the accuracy of the model. The calibration curve was applied to evaluate the consistency between the predicted value and the actual value of the prediction model. P < 0.05 meant that the difference was statistically significant.
Results
Baseline characteristics
Of the 532 patients enrolled in this study, there were 353 males (66.4%), and the average age was (61.0 ± 16.0) years old. Patients with New York Heart Association (NYHA) cardiac function grades II, III and IV accounted for 16.9%, 53.4% and 29.7% of the total cases, respectively. The average EF value was 42.3% ± 14.6%. Meanwhile, 65 patients (12.22%) were identified to have hyponatremia (serum sodium < 135 mmol/L). Table 1 shows the baseline data of patients grouped based on hyponatremia existence. It was found that there were statistically significant differences between groups in NYHA cardiac function grades, blood pressure, serum potassium, albumin, creatinine, uric acid, urea nitrogen, glutamic oxaloacetic transaminase, NT-proBNP and body mass index (all P < 0.05).
Analysis of related factors of hyponatremia
The indicators with statistically significant differences in univariate analysis were included in multivariate stepwise logistic regression analysis. As shown in Table 2, NYHA cardiac function classification (NYHA III vs II, OR = 12.31, NYHA IV vs II, OR = 11.55), systolic blood pressure (OR = 0.978), serum urea nitrogen (OR = 1.046) and creatinine (OR = 1.006) were the independent prognostic factors for hyponatremia in patients with ADHF (all P < 0.05).
Construction of Nomogram prediction model of hyponatremia in patients with ADHF
The construction of the Nomogram model included the NYHA cardiac function classification, systolic blood pressure, urea nitrogen and creatinine to predict hyponatremia risk in ADHF patients, as presented in Fig. 2.

Predictive model for the development of hyponatremia in ADHF patients
Internal validation of Nomogram for predicting hyponatremia in patients with ADHF
The AUC of the ROC was used to assess the accuracy of the constructed Nomogram model. The AUC was 0.757 (95% CI [0.718, 0.793], P < 0.001), suggesting that this model could predict hyponatremia occurrence. Meanwhile, the calibration curve revealed that the Nomogram model had good consistency in predicting hyponatremia occurrence in ADHF patients. The results are shown in Figs. 3 and 4.

ROC curves of the prediction model

Calibration diagram
Discussion
Multiple neurohormonal changes generally cause hyponatremia in patients with ADHF, particularly renin-angiotensin aldosterone system (RAAS) activation to stimulate the release of arginine vasopressin. RAAS has an indirect impact on circulating the water-electrolyte balance through the autonomic nervous system and vasoactive peptides [18]. Creatinine and urea nitrogen concentrations are considered to be the renal function indicators [19], and their increase may indicate an abnormal renal function in the detected patients, leading to water-electrolyte imbalance under the disordered RAAS context. In our study, serum urea nitrogen level was detected to have a stronger association with hyponatremia in patients with ADHF. Similarly, existing research documented that a high serum urea nitrogen level was a risk factor for adverse ADHF events [20]. Serum urea nitrogen at a high level can increase hypoxia tolerance and lead to an increase in blood flow velocity per unit time concerning the mechanism of action; it can simultaneously aggravate the degree of atherosclerosis and eventually result in ADHF [21, 22]. Furthermore, cardiac dysfunction may increase brain natriuretic peptide secretion, which can act on the kidney, inhibit the renin and aldosterone release, increase urinary sodium excretion, and possibly lead to hyponatremia [23]. Meanwhile, diet is also an influential factor in the serum urea nitrogen level, especially in protein intake and endogenous protein catabolism [18, 24]. Patients with ADHF have increased consumption of energy and enhanced protein catabolism, further accelerating the discharge of urea nitrogen [25]. Therefore, it is important for medical workers to pay close attention to the patient’s renal function, especially the urea nitrogen level. There is a need to formulate detailed and personalised dietary plans to ensure the supplementation of high-quality protein and sodium [26].
Ikeda N et al. found in their research that there was a positive correlation between systolic blood pressure and blood sodium at admission, which was consistent with this study’s results [27]. The blood sodium level and extracellular volume in the general population both have an independent impact on the blood pressure level [28]; therefore, low blood sodium can induce hypotension. On the contrary, in the presence of hypotension, there is an activated RAAS system in vivo and long-term over-activation of the system, which may cause neuroendocrine mechanism disturbance and eventually lead to hyponatremia [29,30,31]. In this regard, ADHF patients’ sodium salt consumption should be controlled by the nursing staff, especially for patients with low systolic blood pressure [32]. Moreover, patients with cardiac function grades III and IV have more severe HF, accompanied by an increased degree of oedema, which may further aggravate hyponatremia occurrence. Hence, timely cardiac function correction and maintenance of systolic blood pressure stability are the keys to controlling subsequent disease deterioration.
In this study, the Nomogram prediction model was verified with an AUC of 0.757, and the calibration curve was near the ideal curve, indicating that the model has good discrimination. The prediction model for hyponatremia in patients with ADHF established in this study can intuitively and visually predict hyponatremia occurrence in ADHF patients.
However, our study has some limitations. Firstly, we only conducted a retrospective study in one hospital, so the sample population was limited, further limiting the use of nomograms. Secondly, some indicators were not included in the model because of the high rate of missing data, which decreased the comprehensiveness of the model. The accuracy of the model can be further improved if these missing variables, such as alanine aminotransferase, serum calcium ions and oedema, are added in future studies [33]. Thirdly, we only used the data for the internal verification of our model, and other external data still need to be used to further verify its performance and clinical applicability.
Conclusion
The findings in our study suggest that there is a high hyponatremia risk in ADHF patients with a high creatinine level, a high serum urea nitrogen level, low systolic blood pressure, and cardiac function grades III and IV. This study establishes a risk prediction model for hyponatremia in patients with ADHF, which has good prediction ability. Hyponatremia risk screening in patients at the initial stage of admission can significantly benefit nursing staff to carry out scientific prevention and control, as well as precise implementation according to the specific risk factors.
Availability of data and materials
The data analyzed in this study are not publicly available due to the privacy policy of the hospital but are available from the corresponding author on reasonable request.
References
Hao G, Wang X, Chen Z, Zhang L, Zhang Y, Wei B, et al. Prevalence of heart failure and left ventricular dysfunction in China: the China Hypertension Survey, 2012–2015. Eur J Heart Fail. 2019;21(11):1329–37. https://doi.org/10.1002/ejhf.1629.
Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Drazner MH, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;62(16):e147-239. https://doi.org/10.1016/j.jacc.2013.05.019.
Hunt SA, Abraham WT, Chin MH, Feldman AM, Francis GS, Ganiats TG, et al. 2009 Focused update incorporated into the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines Developed in Collaboration With the International Society for Heart and Lung Transplantation. J Am Coll Cardiol. 2009;53(15):e1–90. https://doi.org/10.1016/j.jacc.2008.11.013.
Bozkurt B, Coats AJS, Tsutsui H, Abdelhamid CM, Adamopoulos S, Albert N, et al. Universal definition and classification of heart failure: a report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure: Endorsed by the Canadian Heart Failure Society, Heart Failure Association of India, Cardiac Society of Australia and New Zealand, and Chinese Heart Failure Association. Eur J Heart Fail. 2021;23(3):352–80. https://doi.org/10.1002/ejhf.2115.
Kurmani S, Squire I. Acute Heart Failure: Definition, Classification and Epidemiology. Curr Heart Fail Rep. 2017;14(5):385–92. https://doi.org/10.1007/s11897-017-0351-y.
McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599–726. https://doi.org/10.1093/eurheartj/ehab368.
Deubner N, Berliner D, Frey A, Güder G, Brenner S, Fenske W, et al. Dysnatraemia in heart failure. Eur J Heart Fail. 2012;14(10):1147–54. https://doi.org/10.1093/eurjhf/hfs115.
Klein L, O’Connor CM, Leimberger JD, Gattis-Stough W, Piña IL, Felker GM, et al. Lower serum sodium is associated with increased short-term mortality in hospitalized patients with worsening heart failure: results from the Outcomes of a Prospective Trial of Intravenous Milrinone for Exacerbations of Chronic Heart Failure (OPTIME-CHF) study. Circulation. 2005;111(19):2454–60. https://doi.org/10.1161/01.Cir.0000165065.82609.3d.
Gheorghiade M, Rossi JS, Cotts W, Shin DD, Hellkamp AS, Piña IL, et al. Characterization and prognostic value of persistent hyponatremia in patients with severe heart failure in the ESCAPE Trial. Arch Intern Med. 2007;167(18):1998–2005. https://doi.org/10.1001/archinte.167.18.1998.
Gheorghiade M, Gattis WA, O’Connor CM, Adams KF Jr, Elkayam U, Barbagelata A, et al. Effects of tolvaptan, a vasopressin antagonist, in patients hospitalized with worsening heart failure: a randomized controlled trial. JAMA. 2004;291(16):1963–71. https://doi.org/10.1001/jama.291.16.1963.
Konstam MA, Gheorghiade M, Burnett JC Jr, Grinfeld L, Maggioni AP, Swedberg K, et al. Effects of oral tolvaptan in patients hospitalized for worsening heart failure: the EVEREST Outcome Trial. JAMA. 2007;297(12):1319–31. https://doi.org/10.1001/jama.297.12.1319.
Spasovski G, Vanholder R, Allolio B, Annane D, Ball S, Bichet D, et al. Clinical practice guideline on diagnosis and treatment of hyponatraemia. Eur J Endocrinol. 2014;170(3):G1-47. https://doi.org/10.1530/eje-13-1020.
Song EK, Moser DK, Kang SM, Lennie TA. Self-reported Adherence to a Low-Sodium Diet and Health Outcomes in Patients With Heart Failure. J Cardiovasc Nurs. 2016;31(6):529–34. https://doi.org/10.1097/jcn.0000000000000287.
Johansson P, van der Wal MH, Strömberg A, Waldréus N, Jaarsma T. Fluid restriction in patients with heart failure: how should we think? Eur J Cardiovasc Nurs. 2016;15(5):301–4. https://doi.org/10.1177/1474515116650346.
Castro-Gutiérrez V, Rada G. Is fluid restriction needed in heart failure? Medwave. 2017;17(Suppl1): e6817. https://doi.org/10.5867/medwave.2017.6817.
Iasonos A, Schrag D, Raj GV, Panageas KS. How to build and interpret a nomogram for cancer prognosis. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2008;26(8):1364–70. https://doi.org/10.1200/jco.2007.12.9791.
Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37(27):2129–200. https://doi.org/10.1093/eurheartj/ehw128.
Komaki T, Miura SI, Arimura T, Shiga Y, Morii J, Kuwano T, et al. The Change in Body Weight During Hospitalization Predicts Mortality in Patients With Acute Decompensated Heart Failure. J Clin Med Res. 2017;9(3):200–6. https://doi.org/10.14740/jocmr2890w.
Jobs A, Brünjes K, Katalinic A, Babaev V, Desch S, Reppel M, et al. Inferior vena cava diameter in acute decompensated heart failure as predictor of all-cause mortality. Heart Vessels. 2017;32(7):856–64. https://doi.org/10.1007/s00380-017-0944-0.
Christopoulou E, Liamis G, Naka K, Touloupis P, Gkartzonikas I, Florentin M. Hyponatremia in Patients with Heart Failure beyond the Neurohormonal Activation Associated with Reduced Cardiac Output: A Holistic Approach. Cardiology. 2022;147(5–6):507–20. https://doi.org/10.1159/000526912.
Romano S, Mansour IN, Kansal M, Gheith H, Dowdy Z, Dickens CA, et al. Left Ventricular global longitudinal strain predicts heart failure readmission in acute decompensated heart failure. Cardiovasc Ultrasound. 2017;15(1):6. https://doi.org/10.1186/s12947-017-0098-3.
Tibrewala A, Wehbe RM, Wu T, Harap R, Ghafourian K, Wilcox JE, et al. Hyponatremia Is a Powerful Predictor of Poor Prognosis in Left Ventricular Assist Device Patients. ASAIO J (American Society for Artificial Internal Organs: 1992). 2022;68(12):1475–82. https://doi.org/10.1097/mat.0000000000001691.
Rodriguez M, Hernandez M, Cheungpasitporn W, Kashani KB, Riaz I, Rangaswami J, et al. Hyponatremia in Heart Failure: Pathogenesis and Management. Curr Cardiol Rev. 2019;15(4):252–61. https://doi.org/10.2174/1573403x15666190306111812.
Natella PA, Le Corvoisier P, Paillaud E, Renaud B, Mahé I, Bergmann JF, et al. Long-term mortality in older patients discharged after acute decompensated heart failure: a prospective cohort study. BMC Geriatr. 2017;17(1):34. https://doi.org/10.1186/s12877-017-0419-2.
Lin Z, Zhao Y, Xiao L, Qi C, Chen Q, Li Y. Blood urea nitrogen to serum albumin ratio as a new prognostic indicator in critical patients with chronic heart failure. ESC heart failure. 2022;9(2):1360–9. https://doi.org/10.1002/ehf2.13825.
Omar HR, Guglin M. Rise of first follow-up sodium in patients hospitalized with acute heart failure is associated with better outcomes. Int J Cardiol. 2018;269:201–6. https://doi.org/10.1016/j.ijcard.2018.06.071.
Ikeda N, Yamashita H, Hattori J, Kato H, Yoshita K, Nishi N. Reduction of Cardiovascular Events and Related Healthcare Expenditures through Achieving Population-Level Targets of Dietary Salt Intake in Japan: A Simulation Model Based on the National Health and Nutrition Survey. Nutrients. 2022;14(17). https://doi.org/10.3390/nu14173606.
Baek EJ, Kim S. Current Understanding of Pressure Natriuresis. Electrolyte Blood Press. 2021;19(2):38–45. https://doi.org/10.5049/ebp.2021.19.2.38.
de Oliveira MG, Nadruz W Jr, Mónica FZ. Endothelial and vascular smooth muscle dysfunction in hypertension. Biochem Pharmacol. 2022;205:115263. https://doi.org/10.1016/j.bcp.2022.115263.
Te Riet L, van Esch JH, Roks AJ, van den Meiracker AH, Danser AH. Hypertension: renin-angiotensin-aldosterone system alterations. Circ Res. 2015;116(6):960–75. https://doi.org/10.1161/circresaha.116.303587.
Yang W, Li H, Cheng Z, Lu Y, Li W, Feng J, et al. Dex modulates the balance of water-electrolyte metabolism by depressing the expression of AVP in PVN. Front Pharmacol. 2022;13:919032. https://doi.org/10.3389/fphar.2022.919032.
Żarnowski A, Jankowski M, Gujski M. Public Awareness of Diet-Related Diseases and Dietary Risk Factors: A 2022 Nationwide Cross-Sectional Survey among Adults in Poland. Nutrients. 2022;14(16). https://doi.org/10.3390/nu14163285.
Li C, Xu F, Han D, Zheng S, Ma W, Yang R, et al. Developing and verifying a multivariate model to predict the survival probability after coronary artery bypass grafting in patients with coronary atherosclerosis based on the MIMIC-III database. Heart Lung. 2022;52:61–70. https://doi.org/10.1016/j.hrtlng.2021.11.009.
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
Concept and design: Qin Wang, Huanhuan Gong, Ying Zhou. Acquisition of data: All authors. Statistical analysis: Huanhuan Gong, Shengen Liao,Yating Huang. Drafting of the manuscript: Qin Wang, Huanhuan Gong, Ying Zhou,Shengen Liao. Critical revision of the manuscript for important intellectual content: All authors.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Ethics approval was obtained from the (the independent ethical review board of the First Afliated Hospital of Nanjing Medical University & Ethical approval number: 2011-SR-012). The study was in Accordance with Declaration of Helsinki. All participants gave written informed consent to participate in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Gong, H., Zhou, Y., Huang, Y. et al. Construction of risk prediction model for hyponatremia in patients with acute decompensated heart failure. BMC Cardiovasc Disord 23, 520 (2023). https://doi.org/10.1186/s12872-023-03557-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-023-03557-5