
Abstract
Background
Lifestyle adjustment has been reported as one of the interventions for dyslipidemia. This study aimed to explore the effect of overall lifestyle on the risk of all-cause mortality and cardiovascular disease (CVD) death in dyslipidemia patients with or without lipid-lowering therapy.
Methods
This was a retrospective cohort study, and data were extracted from the National Health and Nutrition Examination Survey (NHANES). Overall lifestyle was assessed based on Mediterranean diet score, physical activity, smoking status, sleep duration, and body mass index (BMI). Multivariate Cox regression model was used to explore the effect of overall lifestyle score on the risk of all-cause mortality and CVD death. Results were shown as hazard ratio (HR), with 95% confidence interval (CI).
Results
A total of 11,549 dyslipidemia patients were finally included in this study. The results showed that optimal overall lifestyle was associated with the decreased risk of all-cause mortality (HR = 0.47, 95%CI: 0.34–0.64) and CVD death (HR = 0.45, 95%CI: 0.22–0.94) in patients without lipid-lowering therapy. The similar results were found in patients with lipid-lowering therapy (all-cause mortality: HR = 0.45, 95%CI: 0.33–0.62; CVD death: HR = 0.38, 95%CI: 0.23–0.63).
Conclusions
A favorable overall lifestyle may have great benefits to improve the prognosis of dyslipidemia, highlighting the importance of overall lifestyle adjustment for dyslipidemia patients.
Similar content being viewed by others


Background
Dyslipidemia is defined as an increase in the plasma concentrations of total cholesterol (TC), low density lipoprotein-cholesterol (LDL-C) or triglycerides (TG), or a low plasma concentration of high-density lipoprotein cholesterol (HDL-C), or a combination of these features [1]. The prevalence of dyslipidemia is approximately 18% in the United States, and has been a main risk factor for cardiovascular disease (CVD) [1]. Dyslipidemia accounts for about 4.40 million global death and 98.62 million disabilities in 2019, which causes a big burden to medical system [1].
Lipid-lowering medications have been used for the treatment of dyslipidemia; however, side effect of lipid-lowering drugs is a problem that cannot be ignored [2]. The American Heart Association (AHA) recommends a healthy lifestyle across life course and judicious use of lipid-lowering drugs depending on the patients’ risk status [3]. Previous studies have reported that the single lifestyle factor (diet or fitness) combined with statin drugs were associated with the reduced level of cholesterol and decreased risk of mortality [4, 5]. It was known that human lifestyle was overall rather than single [6]. A study by Booth et al. have found that a higher number of healthy lifestyle factors was associated with the lower incidence of atherosclerotic cardiovascular diseases and lower risk of all-cause mortality in dyslipidemia patients with statin therapy [7]. However, this finding needed to be further verified.
In addition, evidence showed that the prescription rate for statins is low in dyslipidemia patients, and 52.3% of dyslipidemia patients do not receive statin therapy [8]. Therefore, adjusting lifestyle is recommended as the primary method for dyslipidemia patients without lipid-lowering therapy [3]. Trautwein et al. have found that a plant-based diet was conducive to lowering LDL-C level and decreasing the risk of CVD in dyslipidemia patients [9]. However, the effect of overall lifestyle on the prognosis of dyslipidemia patients without lipid-lowering therapy has not been reported.
In this study, we aimed to further explore the association between overall lifestyle and the risk of CVD death and all-cause mortality in dyslipidemia patients with lipid-lowering therapy. Also, we explored the effect of overall lifestyle on the risk of CVD death and all-cause mortality in dyslipidemia patients without lipid-lowering therapy.
Methods
Study design and data source
This was a retrospective cohort study based on the National Health and Nutrition Examination Survey (NHANES) (https://www.cdc.gov/nchs/nhanes/index.htm). NHANES was a program of the National Center for Health Statistics (NCHS) of the Centers for Disease Control and Prevention (CDC), and examined a nationally representative sample of about 5,000 people each year [10]. NHANES combined interviews and physical examinations. Interviews consisted of demographic, socioeconomic, dietary, and health-related questions. Examination section included medical, dental, physiological measurements, and laboratory tests. Seven cycles of NHANES from 2005 to 2018 (2005–2006, 2007–2008, 2009–2010, 2011–2012, 2013–2014, 2015–2016, and 2017–2018) were downloaded. The protocols from NHANES have all been approved by the National Center for Health Statistics Research Ethics Review Board (ERB) [11]. The requirement of ethical approval for this was waived by the Institutional Review Board of Jinan Hospital, because the data was accessed from NHANES (a publicly available database). Written informed consent was not required as this study was based on publicly available data. All methods were performed in accordance with the relevant guidelines and regulations.
Study population
Participants meeting the following criteria were included: (1) age ≥ 18 years old; (2) with dyslipidemia: TC ≥ 200 mg/dL (5.2 mmol/L), TG ≥ 150 mg/dL (1.7 mmol/L), LDL-C ≥ 130 mg/dL (3.4 mmol/L), HDL-C ≤ 40 mg/dL (1.0 mmol/L) [12], self-reported hypercholesterolemia, or undergoing lipid-lowering therapy; and (3) with data on lifestyle factors. Participants meeting the following criteria were excluded: (1) missing data on survival.
Lipid-lowering therapy
Participants with self-reported use of lipid-lowering drugs and cholesterol-lowering treatments were determined to receive lipid-lowering therapy. When be asked “In the past 30 days, have you used or taken medication for which a prescription is needed? Do not include prescription vitamins or minerals you may have already told me about”, participants answering “Yes” were then asked for drug name. Participants reporting 3-Hydroxy-3-methyl glutaryl coenzyme A (HMG-COA) reductase inhibitors (statins), miscellaneous antihyperlipidemic agents, fibric acid derivatives, bile acid sequestrants, cholesterol absorption inhibitors, antihyperlipidemic combinations, and PCSK9 inhibitors were regarded as taking lipid-lowering drugs.
Overall lifestyle assessment
Overall lifestyle was assessed based on the following five lifestyle factors: Mediterranean diet score, physical activity level, smoking status, sleep duration, and BMI [6, 7]. Each category was divided into poor, intermediate, and optimal, which scored 0, 1, and 2, respectively. Overall lifestyle score was the sum of the individual score of all 5 lifestyle factors, and divided into poor (0–3 points), intermediate (4–6 points), and optimal (7–10 points).
Mediterranean diet score included 9 components, and sex-specific medians were used as the cutoff to dichotomize the food groups [13, 14]. One point was assigned to the consumption above the median of presumed beneficial foods (legumes, cereals, fruits and nuts, high vegetables, fish, monounsaturated fatty acids-to-saturated fatty acids ratio) and the consumption below the median of presumed detrimental foods (meat and meat products, and dairy products). For alcohol, one point was assigned to men who consumed 10–25 g/day and to women who consumed 5–15 g/day. The total score of Mediterranean diet was 18, and divided into poor (0–6 points), intermediate (7–11 points), and optimal (12–18 points).
Physical activity was divided into high level (scored 2 points) and low level (scored 1 points). For work or sports/fitness/recreational activities, participant did one of these activities at vigorous-intensity, which caused a large increase in breathing or heart rate for at least 10 min continuously, was considered as high level of physical activity. For work, usual way to and from places, and sports/fitness/recreational activities, participants did two of these activities at moderate-intensity, which caused a small increase in breathing or heart rate for at least 10 min continuously, was considered as high level of physical activity. Otherwise, participants were considered at low level of physical activity.
For smoking status, when be asked “Do you smoked at least 100 cigarettes in life” and “Do you now smoke cigarettes”, someone who answered “No” for the first question was classified as “never smoker”; someone who answered “Yes” for the first question and “No” for the second question was classified as “former smoker”; someone who answered “Yes” for both the first and the second question was classified as “current smoker” [15]. Smoking status was divided into poor (current smoking), intermediate (former smoking), and optimal (never smoking).
Sleep duration was obtained from the question “How much sleep do you usually get at night on weekdays or workdays”, and divided into poor (< 5 h/day or > 10 h/day), intermediate (5-5.9 h/day or 8.1–10 h/day), and optimal (6–8 h/day) [16].
BMI was calculated as body weight (kg)/height (m2), and divided into underweight (BMI < 18.5 kg/m2), normal weight (18.5 kg/m2 ≤ BMI < 25 kg/m2), overweight (25 kg/m2 ≤ BMI < 30 kg/m2), and obesity (BMI ≥ 30 kg/m2) [17]. This category was divided into optimal (normal weight), intermediate (underweight or overweight), and poor (obesity).
Outcomes
Outcomes were all-cause mortality and CVD death. All-cause mortality was defined as death from any cause, and CVD death was defined as death from heart diseases and cerebrovascular diseases [18]. The follow-up was terminated when the included patients died.
Covariates of interest
Data of included patients were obtained, including age, gender, race, education level, poverty income ratio (PIR), triglyceride, LDL-C, TC, HDL-C, history of CVD, family history of CVD, hypertension, and diabetes.
Statistical analysis
Measurement data in normal distribution were expressed as mean ± standard deviation (mean ± SD), and differences were compared using t-test (between two groups) or variance analysis (more than two groups). Measurement data in non-normal distribution were expressed as median [M (Q1, Q3)], and differences between groups were compared using rank sum test. Counting data were expressed as number (n) and percentage (%), and differences in groups were compared using chi-square test. Missing data were processed using multiple imputation method, and sensitivity analysis was performed before and after the interpolation.
Univariate Cox regression model was used to select the potential confounders, and the selected confounders were then adjusted in the multivariate Cox regression model to explore the effect of overall lifestyle score on the all-cause mortality and CVD death. Given that BMI could be an intermediate factor between behavioral factors and health outcomes [19], sensitivity analysis which excluded BMI from the overall lifestyle score and included it as a covariate was performed to explore the effect of overall lifestyle score on the all-cause mortality and CVD death. Subgroup analysis was performed based on age. Statistical analysis was performed using SAS 9.4 (SAS Institute Inc., Cary, NC, USA) and R (version 4.2.1, R Foundation for Statistical Computing, Vienna, Austria). P < 0.05 was considered as statistical difference.
Results
Selection and baseline information of patients
A total of 29,426 dyslipidemia patients with age ≥ 18 years were extracted from 2005 to 2018 NHANES database. Of these, we excluded 2,708 patients missing data on lifestyle factors [physical activity level (n = 11); Mediterranean diet score (n = 1644); sleep duration (n = 88), BMI (n = 471), and smoking status (n = 494)] and 15,153 patients missing data on blood lipid test [TC (n = 2302) and LDL-C (n = 12,851)]. In the remaining 11,565 patients, 16 patients were excluded due to missing data on survival. Finally, 11,549 patients were included in this study for analysis (Fig. 1).

The flowchart of patient section
In the included patients, there were 1,109 patients in the poor overall lifestyle group, 7,292 patients in the intermediate overall lifestyle group, and 3,148 patients in the optimal overall lifestyle group. Sensitivity analysis showed that estimates were not significantly different before versus after imputation for missing data (all P > 0.05) (Additional file table S1). The mean age of included patients was 53.54 ± 17.08 years, and there were 50.51% of male (n = 5833). In addition, there were 32.15% of patients with lipid-lowering therapy (n = 3713) and 67.85% of patients without lipid-lowering therapy (n = 7836) (Table 1). The characteristics of patients without lipid-lowering therapy were shown in Additional file table S2, and the characteristics of patients with lipid-lowering therapy were shown in Additional file table S3.
Effect of overall lifestyle on the risk of all-cause mortality and CVD death in dyslipidemia patients with or without lipid-lowering therapy
Table 2 shows that age, race, education level, PIR, HDL-C, family history of CVD, history of CVD, hypertension, and diabetes were covariates for all-cause mortality in patients without lipid-lowering therapy. Age, race, education level, PIR, HDL-C, history of CVD, hypertension, and diabetes were covariates for CVD death in patients without lipid-lowering therapy. Age, race, education level, PIR, LDL-C, TC, history of CVD, hypertension, and diabetes were covariates for all-cause mortality in patients with lipid-lowering therapy. Age, education level, PIR, LDL-C, TC, history of CVD, hypertension, and diabetes were covariates for CVD death in patients with lipid-lowering therapy.
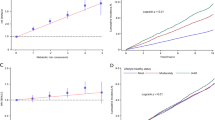
After adjusting these covariates, we found that better overall lifestyle was associated with the lower risk of all-cause mortality (intermediate: HR = 0.68, 95%CI: 0.52–0.90; optimal: HR = 0.47, 95%CI: 0.34–0.64) and CVD death (optimal: HR = 0.45, 95%CI: 0.22–0.94) than the poor overall lifestyle in patients without lipid-lowering therapy. We also found the significant association between better overall lifestyle and lower risk of all-cause mortality (intermediate: HR = 0.55, 95%CI: 0.42–0.73; optimal: HR = 0.45, 95%CI: 0.33–0.62) and CVD death (intermediate: HR = 0.46, 95%CI: 0.32–0.68; optimal: HR = 0.38, 95%CI: 0.23–0.63) in patients with lipid-lowering therapy (Table 3). Additional file table S4 shows the similar association between lifestyle and the risk of all-cause mortality and CVD death after removing BMI from the overall lifestyle score.
Effect of overall lifestyle on the risk of all-cause mortality and CVD death in dyslipidemia patients with or without lipid-lowering therapy based on age
After adjusting race, education level, PIR, HDL-C, family history of CVD, history of CVD, hypertension, and diabetes, optimal overall lifestyle was found to be associated with the lower risk of all-cause mortality in patients without lipid-lowering therapy and with age < 65 years (HR = 0.53, 95%CI: 0.32–0.88) and age ≥ 65 years (HR = 0.57, 95%CI: 0.33–0.99). After adjusting race, education level, PIR, HDL-C, history of CVD, hypertension, and diabetes, intermediate overall lifestyle was associated with the lower risk of CVD death in patients without lipid-lowering therapy and with age < 65 years (HR = 0.34, 95%CI: 0.14–0.83). In patients with lipid-lowering therapy, better overall lifestyle was found to be associated with lower risk of all-cause mortality (intermediate: HR = 0.65, 95%CI: 0.46–0.91; optimal: HR = 0.56, 95%CI: 0.39–0.82) in age ≥ 65 years group after adjusting race, education level, PIR, LDL-C, TC, history of CVD, hypertension, and diabetes. After adjusting education level, PIR, LDL-C, TC, history of CVD, hypertension, and diabetes, the association between better overall lifestyle and lower risk of CVD death was found in patients with lipid-lowering therapy and with age ≥ 65 years (intermediate: HR = 0.52, 95%CI: 0.33–0.81; optimal: HR = 0.50, 95%CI: 0.30–0.82) (Table 4).
Discussion
In this cohort study, 11,549 dyslipidemia patients from NHANES database were included. We found that better overall lifestyle was associated with the decreased risk of all-cause mortality and CVD death in dyslipidemia patients with or without lipid-lowering therapy. In subgroup of age ≥ 65 years, better overall lifestyle reduced the risk of all-cause mortality in patients without lipid-lowering therapy, and reduced the risk of all-cause mortality and CVD death in patients with lipid-lowering therapy. In subgroup of age < 65 years, better overall lifestyle reduced the risk of all-cause mortality and CVD death in patients without lipid-lowering therapy.
Healthy lifestyle behaviors are considered as important ways to decrease the burden of diseases [20, 21]. Keeping a healthy diet that eating more vegetables, fruit, legumes, grains, and fish, and decreasing the intake of salt, sugar, fats, and red meat prevents about 11 million deaths every year worldwide [22]. Non-smoking, alcohol restriction, and adequate physical activity respectively prevent about 7 million, 3 million, and 1 million deaths annually [22]. Combining the healthy lifestyle behaviors results in greater health benefits than the single behavior, preventing more than 60% of premature deaths [23] and extending the expected life of patients without CVD, cancer, and type 2 diabetes by 7–10 years [24]. Dyslipidemia is the main risk factor for the development of atherosclerosis, and lifestyle interventions and lipid-lowering therapy are widely used in the management of CVD [25]. Many lifestyle factors are reported to contribute to the development of dyslipidemia, including dietary habits, increased BMI, and smoking [26]. Low intensity of physical activity and short sleeping duration have also been associated with dyslipidemia [27, 28]. Some studies have reported the effect of lifestyle adjustment on the prognosis of dyslipidemia patients [4, 5]. Kokkinos et al. have reported that the increase of fitness decreased the risk of mortality in dyslipidemia patients with lipid-lowering therapy, and the risk reduced by 70% in highly fit individuals compared to least fit individuals, highlighting the importance of physical activity for dyslipidemia patients [5]. Jula et al. have reported that dietary adjustment decreased TC level by 7.6%, LDL-C level by 10.8%, HDL-C level by 4.9%, and apolipoprotein B level by 5.7% in patients with hypercholesterolemia [4]. In this study, we found that overall lifestyle assessed by Mediterranean diet score, physical activity, smoking status, sleep duration, and BMI was associated with prognosis of dyslipidemia patients. Better overall lifestyle decreased the risk of all-cause mortality and CVD death in patients with or without lipid-lowering therapy. Our findings highlighted the importance of overall lifestyle adjustment in the improvement of poor prognosis for dyslipidemia patients whether receiving lipid-lowering treatment or not.
Age has been reported to be associated with dyslipidemia [29]. Herein, we explored the effect of overall lifestyle on the all-cause mortality and CVD death based on ages. For dyslipidemia patients with age ≥ 65 years, whether taking lipid-lowering treatment or not, better overall lifestyle contributes to reduce the risk of all-cause mortality. Molanorouzi et al. have found that older individuals exhibited greater concerns about health outcomes, which motivated them to adjust lifestyle for better physical and psychological health [30]. Better overall lifestyle was associated with the reduced risk of CVD death in patients with lipid-lowering treatment, while no significance was found in patients without lipid-lowering treatment, indicating that better overall lifestyle may have potential benefits to reduce the risk of CVD death and was especially important for the elderly receiving lipid-lowering treatment. For dyslipidemia patients with age < 65 years, better overall lifestyle was associated with the reduced risk of all-cause mortality and CVD death in the individuals without lipid-lowering therapy. Our findings indicated that a good overall lifestyle may help improve the prognosis of younger dyslipidemia patients not receiving lipid-lowering treatments.
This is a cohort study including a larger sample size to explore the effect of overall lifestyle on the prognosis of dyslipidemia patients, which provides evidence for the importance of lifestyle adjustment in the management of dyslipidemia. However, there are some limitations in this study. First, this is a retrospective study that selective bias is inevitable. Second, there is no information on the dosage and frequency of lipid-lowering medications due to the limitation of database; therefore, we cannot assess the effect of overall lifestyle on the prognosis based on dosage and frequency of lipid-lowering medication, which needs to be further explored in future studies. Third, although the five lifestyle factors included in the overall lifestyle score are the main components reported in previous studies, they may not represent all aspects of the lifestyle. Future studies should include more lifestyle factors to verify our findings.
Conclusion
In this study, we found that better overall lifestyle was associated with the reduced risk of all-cause mortality and CVD death in dyslipidemia patients with or without lipid-lowering therapy, indicating that adherence to a favorable lifestyle may have great benefits for the management of dyslipidemia whether receiving lipid-lowering treatment or not.
Data Availability
The datasets generated and/or analyzed during the current study are available in the NHANES database, https://wwwn.cdc.gov/nchs/nhanes/.
Abbreviations
- TC:
-
Total cholesterol
- LDL-C:
-
Low density lipoprotein-cholesterol
- TG:
-
Triglycerides
- HDL-C:
-
High-density lipoprotein cholesterol
- CVD:
-
Cardiovascular disease
- AHA:
-
American Heart Association
- BMI:
-
Body mass index
- NHANES:
-
National Health and Nutrition Examination Survey
- NCHS:
-
National Center for Health Statistics
- CDC:
-
Centers for Disease Control and Prevention
- ERB:
-
Ethics Review Board
- PIR:
-
Poverty income ratio
- HR:
-
Hazard ratio
References
Pirillo A, Casula M, Olmastroni E, Norata GD, Catapano AL. Global epidemiology of dyslipidaemias. Nat reviews Cardiol. 2021;18:689–700.
Abdul-Rahman T, Bukhari SMA, Herrera EC, Awuah WA, Lawrence J, de Andrade H, et al. Lipid lowering therapy: an era beyond statins. Curr Probl Cardiol. 2022;47:101342.
Grundy SM, Stone NJ. 2018 American Heart Association/American College of Cardiology Multisociety Guideline on the Management of Blood Cholesterol: Primary Prevention. JAMA cardiology. 2019; 4: 488-9.
Jula A, Marniemi J, Huupponen R, Virtanen A, Rastas M, Rönnemaa T. Effects of diet and simvastatin on serum lipids, insulin, and antioxidants in hypercholesterolemic men: a randomized controlled trial. JAMA. 2002;287:598–605.
Kokkinos PF, Faselis C, Myers J, Panagiotakos D, Doumas M. Interactive effects of fitness and statin treatment on mortality risk in veterans with dyslipidaemia: a cohort study. Lancet (London England). 2013;381:394–9.
Lu Q, Zhang Y, Geng T, Yang K, Guo K, Min X, et al. Association of Lifestyle factors and antihypertensive medication Use with risk of all-cause and cause-specific mortality among adults with hypertension in China. JAMA Netw open. 2022;5:e2146118.
Booth JN 3rd, Colantonio LD, Howard G, Safford MM, Banach M, Reynolds K, et al. Healthy lifestyle factors and incident heart disease and mortality in candidates for primary prevention with statin therapy. Int J Cardiol. 2016;207:196–202.
Bucholz EM, Rodday AM, Kolor K, Khoury MJ, de Ferranti SD. Prevalence and predictors of cholesterol screening, awareness, and Statin Treatment among US adults with familial hypercholesterolemia or other forms of severe dyslipidemia (1999–2014). Circulation. 2018;137:2218–30.
Trautwein EA, McKay S. The Role of Specific Components of a Plant-Based Diet in Management of Dyslipidemia and the Impact on Cardiovascular Risk. Nutrients. 2020; 12.
Ervin RB. Prevalence of metabolic syndrome among adults 20 years of age and over, by sex, age, race and ethnicity, and body mass index: United States, 2003–2006. Natl health Stat Rep. 2009;13:1–7.
Hirode G, Wong RJ, Wong. Trends in the prevalence of metabolic syndrome in the United States, 2011–2016. JAMA. 2020;323:2526–28.
Jellinger PS, Smith DA, Mehta AE, Ganda O, Handelsman Y, Rodbard HW, et al. American Association of Clinical Endocrinologists’ Guidelines for Management of Dyslipidemia and Prevention of Atherosclerosis. Endocr Pract. 2012;1:1–78.
Kim H, Kwon O. Higher Diet Quality is Associated with Lower Odds of Low Hand Grip Strength in the Korean Elderly Population. Nutrients. 2019; 11.
Bonaccio M, Di Castelnuovo A, Costanzo S, Persichillo M, De Curtis A, Cerletti C, et al. Interaction between Mediterranean diet and statins on mortality risk in patients with cardiovascular disease: findings from the Moli-sani Study. Int J Cardiol. 2019;276:248–54.
Natto SSYAL, Midle ZS, Gyurko JB, O’Neill R, Steffensen R. Association between time since quitting smoking and periodontitis in former smokers in the National Health and Nutrition examination surveys (NHANES) 2009 to 2012. J Periodontol. 2019;90:16–25.
Wang C, Bangdiwala SI, Rangarajan S, Lear SA, AlHabib KF, Mohan V, et al. Association of estimated sleep duration and naps with mortality and cardiovascular events: a study of 116 632 people from 21 countries. Eur Heart J. 2019;40:1620–9.
Fahed G, Aoun L, Bou Zerdan M, Allam S, Bou Zerdan M, Bouferraa Y et al. Metabolic syndrome: updates on pathophysiology and management in 2021. Int J Mol Sci. 2022; 23(2).
Ma R, Gao J, Mao S, Wang Z. Association between heart rate and cardiovascular death in patients with coronary heart disease: a NHANES-based cohort study. Clin Cardiol. 2022;45:574–82.
Zhang YB, Chen C, Pan XF, Guo J, Li Y, Franco OH, et al. Associations of healthy lifestyle and socioeconomic status with mortality and incident cardiovascular disease: two prospective cohort studies. BMJ. 2021;373:n604.
Chiuve SE, Rexrode KM, Spiegelman D, Logroscino G, Manson JE, Rimm EB. Primary prevention of stroke by healthy lifestyle. Circulation. 2008;118:947–54.
Stampfer MJ, Hu FB, Manson JE, Rimm EB, Willett WC. Primary prevention of coronary heart disease in women through diet and lifestyle. N Engl J Med. 2000;343:16–22.
Loef M, Walach H. The combined effects of healthy lifestyle behaviors on all cause mortality: a systematic review and meta-analysis. Prev Med. 2012;55:163–70.
Global regional et al. and national comparative risk assessment of 84 behaviournvironmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet (London, England). 2018; 392: 1923-94.
Li Y, Schoufour J, Wang DD, Dhana K, Pan A, Liu X, et al. Healthy lifestyle and life expectancy free of cancer, cardiovascular disease, and type 2 diabetes: prospective cohort study. BMJ (Clinical research ed). 2020;368:l6669.
Anderson TJ, Mancini GB, Genest J Jr, Grégoire J, Lonn EM, Hegele RA. The new dyslipidemia guidelines: what is the debate? Can J Cardiol. 2015;31:605–12.
Opoku S, Gan Y, Fu W, Chen D, Addo-Yobo E, Trofimovitch D, et al. Prevalence and risk factors for dyslipidemia among adults in rural and urban China: findings from the China National Stroke Screening and prevention project (CNSSPP). BMC Public Health. 2019;19:1500.
Al-Hassan Y, Fabella E, Estrella E, Aatif M. Prevalence and determinants of Dyslipidemia: data from a Saudi University Clinic. Open Public Health Journal. 2018;11:416–24.
Enani S, Bahijri S, Malibary M, Jambi H, Eldakhakhny B, Al-Ahmadi J et al. The Association between Dyslipidemia, Dietary Habits and other Lifestyle indicators among non-diabetic attendees of primary Health Care Centers in Jeddah, Saudi Arabia. Nutrients. 2020; 12.
de Vries JK, Balder JW, Pena MJ, Denig P, Smit AJ. Non-LDL dyslipidemia is prevalent in the young and determined by lifestyle factors and age: the LifeLines cohort. Atherosclerosis. 2018;274:191–8.
Molanorouzi K, Khoo S, Morris T. Motives for adult participation in physical activity: type of activity, age, and gender. BMC Public Health. 2015;15:66.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
QW and HW designed the study. QW and DP wrote the manuscript. QW and DP collected, analyzed, and interpreted the data. HW critically reviewed, and edited the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The requirement of ethical approval for this was waived by the Institutional Review Board of Jinan Hospital, because the data was accessed from NHANES (a publicly available database). Written informed consent was not required as this study was based on publicly available data. All methods were performed in accordance with the relevant guidelines and regulations.
Consent for publication
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, Q., Pang, D. & Wang, H. Effect of overall lifestyle on the all-cause mortality and cardiovascular disease death in dyslipidemia patients with or without lipid-lowering therapy: a cohort study. BMC Cardiovasc Disord 23, 438 (2023). https://doi.org/10.1186/s12872-023-03450-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-023-03450-1