
Abstract
Background
GRACE risk score models are capable of predicting all-cause mortality of non-ST elevation myocardial infarction (NSTEMI) patients. However, its utility for evaluating major adverse cardiovascular events (MACE) in NSTEMI patients with multivessel disease (MVD) remains unclear.
Methods and results
This study was designed as a retrospective cohort study that recruited patients with NSTEMI and multivessel disease between September 2013 and December 2018 in Daping Hospital, Chongqing, China. The primary outcome was a composite outcome that included all-cause mortality, recurrent angina, non-fatal myocardial infarction, coronary re-vascularization, and non-fatal strokes. Of the 827 patients with NSTEMI, 32 did not complete follow-up and 430 were excluded because of single-vessel disease. The remaining 365 NSTEMI patients with MVD had a median follow-up of 3.0 (IQR 2.6–3.3) years, 78 patients experienced outcomes. The GRACE risk score predicted the MACE (hazard ratio 1.014, 95% CI 1.006–1.021, P < 0.001). The GRACE risk score performed well in predicting all-cause mortality (c-statistic 0.72, 95% CI 0.59–0.85, P = 0.001) in MVD but was less powerful in predicting MACE (c-statistic 0.69, 95% CI 0.62–0.75, P < 0.001). When combining the GRACE risk score with the SYNTAX score, and blood urea nitrogen for predicting all-cause mortality and MACE events, the c-statistic value increased to 0.82 and 0.81 (P < 0.001).
Conclusion
In NSTEMI patients with MVD, the GRACE score showed an acceptable predictive value for all-cause mortality, but it was less powerful in predicting MACE. Blood urea nitrogen may be valuable in assessing long-term cardiovascular events in patients with MVD.
Similar content being viewed by others


Introduction
Multivessel disease (MVD) was encountered in approximately 50% of patients with non-ST-segment elevation myocardial infarction (NSTEMI) [1,2,3]. Compared with single vessel disease, NSTEMI patients with multivessel disease have reported with a higher incidences of cardiovascular events [4]. In combination with advancing age and comorbidities, their risks for major adverse cardiovascular events (MACE) were substantially increased [4, 5]. Compared with STEMI and stable coronary artery disease, there was currently less evidence describing the optimal treatment strategy for NSTEMI [4]. Therefore, it was prudent important to carry out risk assessment for the long-term prognosis of NSTEMI patients with MVD.
The GRACE risk score provided an excellent discriminative performance among risk assessment models with all-cause mortality as the clinical endpoint [6,7,8]. It was also recommended by 2020 European Society of Cardiology guidelines of non-ST-segment elevation acute coronary syndrome management to assess short- or long-term mortality risk in patients with NSTEMI [9]. The GRACE risk score was originally developed to estimate the risk of death in hospitals, and the clinical endpoint only takes into account all-cause mortality [9], excluding other cardiovascular events such as recurrent angina, non-fatal myocardial infarction, coronary revascularization. But these diseases also provided great burdens to the public health and economics. And until now, the ideal tool predicting the incidence of the MACE of NSTEMI patients was still lacking, and whether the GRACE score was suitable for assessing MACE of NSETMI patients remained unclear, especially in patients with MVD.
To solve the current dilemma, we used the clinical data of NSTEMI patients with MVD, which were regularly followed up for 3 years, to analyze the factors influencing the long-term prognosis of patients and the predictive discriminatory capacity of GRACE score.
Methods
Study population
This study was designed as a retrospective registry of patients admitted with the diagnosis of acute NSTEMI in Daping Hospital (tertiary medical center with emergency departments in Chongqing, China) of the Army Military Medical University from September 2013 to December 2018 (According to the criteria recommended by 2011/2015 European Society of Cardiology Guidelines [10, 11]). Based on the results of coronary angiography, NSTEMI patients with MVD were enrolled. Multivessel coronary artery disease was defined as a lesion ≥ 70% in at least 2 native coronary artery distributions. The patients were followed up for 3 years from the date of diagnosed as MVD. Patients’ status was checked from medical records in hospitals or by telephone for any patients who had moved during the follow-up. The outcomes were the major adverse cardiovascular events (MACE) of all-cause mortality included in-hospital mortality, recurrent angina, nonfatal MI, coronary revascularization, and nonfatal stroke. The study was reviewed and approved by the Ethics Committee of Daping Hospital. All patients provided written informed consent, and this study was conducted in accordance with the Declaration of Helsinki.
General clinical information
The following data were collected from the electronic medical records: age, gender, weight, height, previous medical history, medications on admission, heart rate and blood pressure on admission, cardiac arrest at admission, Killip classification, 12 Lead electrocardiogram, cardiac ultrasound report, time of onset of symptoms, time of first medical contact, time of coronary angiography, length of hospital stay, and routinely available laboratory data including potassium, serum creatinine (Scr), blood urea nitrogen (BUN), fasting glucose, creatine kinase-MB, Troponin I, total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides, and full blood count. If a patient had been checked multiple times, only the first measurement result was taken.
The coronary angiography report was confirmed by the experienced interventional cardiologist in a blinded manner. The analyzed coronary angiography data included severity of coronary artery stenosis (left main artery, left anterior descending artery, circumflex artery, right coronary artery), culprit vessel if applicable, stent type, and Thrombolysis in Myocardial Infarction (TIMI) classification. We used the widely accepted methods to calculate the following three scoring systems: TIMI, Global Registry of Acute Coronary Events (GRACE) [9], and Synergy between PCI with Taxus and cardiac surgery (SYNTAX) score [12]. All the scoring systems were assessed at the time of the patients admitted to the emergency department.
Statistical analysis
The data were presented as median and interquartile ranges or percentages, unless otherwise indicated. Baseline characteristics were compared according to the quartiles of the GRACE risk score [Quartile 1 (≤ 122); Quartile 2 (123–143); Quartile 3 (144–165); Quartile 4 (≥ 166)]. Comparisons among multiple groups were performed using the Kruskal–Wallis H test or χ2 test according to their variable types. We used Cox proportional hazards regression models to investigate the association between the MACE and GRACE risk score values, and the results were expressed as hazard ratios (HR) and 95% confidence intervals (CI). A multivariate adjustment method was used to control for confounding factors: based on the significance of univariate regression analysis (P < 0.05) or their biological plausibility (i.e., heart rate, hypertension, chronic kidney disease, and Previous MI), these covariates were selected as potential confounding factors and forced into the multivariate Cox model analyses. Every 10-point increment in the GRACE score was calculated by GRACE score divided by 10. We used Kaplan-Meier plots to display the cumulative risk of MACE, and a log-rank test was used to compare groups. To assess the discriminatory capacity of cardiovascular events, receiver operating characteristic curve analysis was performed, and results were expressed as c-statistic. The data were analyzed by SPSS 25.0 software (New York, USA). The value of two-sided P < 0.05 was considered statistically significant.
Results
Characteristics of patients
Of the 3370 patients who had acute coronary syndrome in the study period September 2013 to December 2018, 397 (11.8%) patients had a diagnosis of NSTEMI with MVD. 32(0.08%) patients were excluded because of missing follow-up data. Finally,365 NSTEMI patients (278 men and 87 women; age, 65.5 ± 11.0 years) were included in the analyze. During median 3.0(IQR 2.6–3.3) years follow-up 78(21.4%) patients experienced outcomes. These included 18(4.9%) all-cause mortality, 18(4.9%) recurrent angina, 15(4.1%) nonfatal MI, 34(9.3%) coronary revascularization, and 10(2.7%) nonfatal stroke cases (Fig. 1). The patients were divided into four groups according to the quartiles of the GRACE risk score [Quartile 1 (≤ 122): n = 93; Quartile 2 (123–143): n = 92; Quartile 3 (144–165): n = 90; Quartile 4 (≥ 166): n = 90] and the baseline characteristics of the patients were analyzed (Table 1). Patients with a higher GRACE risk scores were more likely to be male, smoke cigarettes, drink alcohol and aging. The mean heart rate, mean blood pressure, the prevalence of MACE, Scr and BUN levels, and use of aspirin increased significantly with a higher GRACE risk score. The cardiac enzymes, total cholesterol and fasting glucose values, the prevalence of diabetes, hypertension, sepsis and chronic kidney disease, history of MI or PCI, use of antihypertensive drug and lipid-lowering drug, and other clinical examination reports did not differ among the GRACE risk score quartile groups.

Study profile
Association between GRACE risk score and MACE
At 2.5 years, the cumulative incidence rates of the MACE were shown according to the GRACE risk score levels in Fig. 2, and the rates were significantly higher in the fourth quartile group than in the first quartile group (P < 0.001). To further explore the correlation between the GRACE score and the prevalence of MACE, Cox proportional hazards model analysis was performed. In univariable analyses, older age, higher heart rate on admission, higher BUN and Scr, higher GRACE risk score and SYNTAX score, history of diabetes and PCI, but not other medical history and other clinical examination reports, were associated with MACE (Additional file 1: Table S1). The age- and sex-adjusted HR increased linearly with elevating GRACE score levels, and this relationship remained significant after adjusting for age, sex, BMI, heart rate, systolic blood pressure, smoking status, alcohol use, diabetes, hypertension, chronic kidney disease, previous MI, previous PCI, BUN, Scr, and use of aspirin patients (Table 2). In the multivariable analyses model, the fourth quartile of GRACE score (≥ 166) was associated with increased risk of the MACE compared with the first quartile of GRACE score (≤ 122), after adjusting for the above confounding factors [HR 3.64, 95% confidence interval (CI) 1.32–10.01, P = 0.012]. Every 10-point increment in the GRACE score was similarly associated with an increased risk of the MACE, after adjusting for the confounding factors (HR 1.19, 95% CI 1.06–1.32, P = 0.002).

Kaplan-Meier plot of cumulative probability of cardiovascular events by quartiles of the GRACE risk scores. MACE, major adverse cardiovascular events
To avoid overfitting of the multivariable analyses model, the stepwise forward Cox regression model was performed to identify predictors based on the likelihood ratio test. The results showed that GRACE score (HR 1.014, 95% CI 1.006–1.021, P < 0.001), SYNTAX score (HR 1.101, 95%CI 1.070–1.133, P < 0.001), and BUN (HR 1.082, 95%CI 1.020–1.148, P = 0.009) were independently associated with MACE (Table 3).
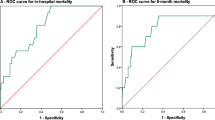
Estimation of the risk prediction ability for all-cause mortality and MACE
To investigate the predictive value of the GRACE score for all-cause mortality and MACE, receiver operating characteristic curve analysis were performed (Table 4). The results demonstrated that GRACE score (c = 0.72, 95% CI 0.59–0.85, P = 0.001), SYNTAX score (c = 0.75, 95% CI 0.66–0.84, P < 0.001), and BUN on admission (c = 0.78, 95% CI 0.66–0.89, P < 0.001) showed a good predictive value of all-cause mortality. For the prediction of comprehensive MACE, the discriminative value of GRACE score, and BUN decreased to varying degrees. However, the SYNTAX score maintained its predictive power in predicting MACE. Combining the three predictors significantly improved the performance of predicting cardiovascular events (all-cause mortality: c = 0.82, 95% CI 0.74–0.92, P < 0.001; MACE: c = 0.81, 95% CI 0.75–0.86, P < 0.001).
Discussion
This study explored the relationship between the GRACE risk score and the occurrence of MACE in NSTEMI patients with MVD. In our study, we noticed a significant correlation between the occurrence of MACE and the GRACE risk score. Even after adjusting for confounders, the GRACE risk score was still independently associated with MACE. The GRACE risk score was previously reported for predicting the risk of all-cause mortality or (and) MI in patients with NSTEMI [6,7,8,9]. However, the value of the GRACE risk score for MACE in MVD remained undetermined. Our study found that the GRACE risk score performed well in predicting all-cause mortality in MVD, but was less powerful in predicting MACE. Furthermore, we also found that combining the GRACE risk score with the SYNTAX score, and BUN significantly improved the ability to predict MACE.
In our study, MVD accounted for 48% of NSTEMI patients. This finding was consistent with previous reports that a substantial proportion (up to 50%) of patients with NSTEMI undergoing invasive management had MVD on the angiography [1,2,3, 13]. Compared with single-vessel disease, MVD had a worse quality of life and higher cardiovascular risk [4, 14]. Patients with MVD were usually accompanied with comorbid risk factors such as elderly age, hypertension, diabetes impaired renal function, as well as lung disease, a higher likelihood of a previous MI and dyslipidemia [4, 15]. Therefore, it was very important to provide long-term MACE risk assessment in NSTEMI patients with MVD for secondary prevention.
The multiple risk factors make it challenging to evaluate the long-term prognosis and risk stratification of MVD to allow early intervention. Among many prognostic models aimed to estimate the risk of all-cause mortality, the GRACE risk score provided the best discriminative power. [7, 8] Although many validation studies confirmed the validity of GRACE in multiple clinical settings, to our knowledge, we were the first to evaluate its performance in predicting long-term outcomes in patients with MVD. The GRACE score, which was recommended for predicting all-cause mortality in NSTEMI patients, did not show a particular advantage in predicting MACE performance compared with other risk factors in our study. This result may be due to differences in the predictive value of the GRACE score between different clinical endpoints [7, 16, 17]. The GRACE score prospectively verified that the c-statistic value of ACS patients predicting death 6 months after admission was 0.81, while the c-statistic value predicting death or MI was 0.73 [18]. This may be an important reason why the difference in the GRACE score predicts all-cause mortality (c = 0.72) and MACE (c = 0.69) of NSTEMI patients with MVD.
All versions of the GRACE risk score model used the same eight variables (age, systolic blood pressure, heart rate, Scr, cardiac arrest at admission, elevated cardiac biomarkers, ST-segment deviation, and Killip class) for risk prediction [9]. The eight variables were transient indicators at admission, without considering the patient’s comorbidity or long-term indicators (such as the degree of coronary atherosclerosis) [7]. The early death of NSTEMI patients was more attributable to ischemia/thrombosis-related events, and the later death was more related to the progression of atherosclerosis and non-cardiovascular causes such as diabetes [4, 9]. This also explained the good performance of diabetes and SYNTAX score in predicting all-cause mortality in patients with MVD. Similarly, the inadequate predicting value of the GRACE score for long-term prognosis of patients with MVD may be due to comorbidity and coronary atherosclerosis which are not taken into consideration. Recently, a study found that in predicting the severity and extent of coronary artery stenosis, GRACE score can detect normal coronary individuals or mild CAD patients very well. But in high-risk patients it had a high negative predictive value [19]. In patients with MVD, the severity and extent of coronary artery stenosis is an important factor to the MACE. Thus, this may also a reason for the inadequate predicting value of the GRACE score for long-term prognosis of patients with MVD.
SYNTAX score and BUN were also closely associated with the occurrence of MACE in our forward stepwise Cox regression analysis. SYNTAX score was a risk scoring method for quantitatively evaluating the complexity of lesions based on 11 anatomical features of coronary angiographic lesions [12, 20]. Compared with GRACE scores, SYNTAX score provided an effective, objective, evidence-based tool to evaluate the severity and extent of coronary artery stenosis [21]. For patients with MVD who were candidates for both PCI and coronary artery bypass grafting (CABG), the SYNTAX score can be used to help make treatment decisions [12]. In patients with three-vessel disease undergoing PCI and stenting, a higher SYNTAX scores significantly predicted a higher risk of MACE [22]. Consistent with previous studies [12, 21, 23], we also found that the SYNTAX score had good performance in predicting all-cause mortality and MACE in our study. Besides, the BUN levels were strongly associated with cardiovascular events in patients with MVD in our study. This finding was consisted with the previous study, in patients with PCI when GFR < 30 mL/min people were more susceptible to occurrence of MACE [24]. BUN is a predictor of the prognosis of patients with heart failure, and the correlated better with mortality than did Scr and glomerular filtration rate [25,26,27]. This may explain why BUN was related to MACE in the Cox analysis, but Scr showed a non-significant P-value in the multivariate analysis. Finally, we found that the GRACE risk score combined with the SYNTAX score, and BUN improved the ability to predict all-cause mortality (c = 0.82) and MACE (c = 0.81) to a satisfactory level. This suggested that BUN was an important predictor of long-term prognosis in patients with MVD, which may provide an effective tool for establishing an ideal model for predicting cardiovascular events.
This study had several limitations. Firstly, it was a single center study with relatively small sample size. Secondly, we were unable to assess differences in GRACE scores due to improved medical conditions. Finally, we were not able to estimate thresholds for each event because of the small number of secondary outcome events. Therefore, further studies with multicenter and larger samples are necessary.
Despite these limitations, the conclusions of our study are still reliable. Based on the assumptions of a two-sided alpha of 5%, 80% power, and a 20% dropout rate, the estimated sample size according to the Freedman’s method was 329, while the sample size for this study was 365 [28]. In addition, we adjusted for a variety of clinical risk factors and potential confounders that could confound interpretation of the data.
In conclusion, the GRACE score showed an acceptable predictive value for all-cause mortality in patients with MVD, whereas it was insufficiently effective in predicting MACE. BUN on admission was independent predictor of the MACE in patients with MVD. Our finding supported that BUN may be potentially useful in predicting the long-term prognosis of NSTEMI patients with MVD.
Availability of data and materials
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
References
Omer MA, Brilakis ES, Kennedy KF, Alkhouli M, Elgendy IY, Chan PS, Spertus JA. Multivessel versus culprit-vessel percutaneous coronary intervention in patients with non-ST-segment elevation myocardial infarction and cardiogenic shock. JACC Cardiovasc Interv. 2021;14(10):1067–78.
Mehta SR, Bossard M. Acute coronary syndromes and multivessel disease: completing the evidence. JACC Cardiovasc Interv. 2020;13(13):1568–70.
Ge J, Li J, Yu H, Hou B. Hypertension is an independent predictor of multivessel coronary artery disease in young adults with acute coronary syndrome. Int J Hypertens. 2018;2018:7623639.
Baumann AAW, Mishra A, Worthley MI, Nelson AJ, Psaltis PJ. Management of multivessel coronary artery disease in patients with non-ST-elevation myocardial infarction: a complex path to precision medicine. Ther Adv Chronic Dis. 2020;11:2040622320938527.
Henriques JP, Claessen BE. A SMILE and a frown: one-stage or multistage PCI in NSTEMI patients with multivessel disease. J Am Coll Cardiol. 2016;67(3):273–4.
Fox KA, Fitzgerald G, Puymirat E, Huang W, Carruthers K, Simon T, Coste P, Monsegu J, Gabriel Steg P, Danchin N, et al. Should patients with acute coronary disease be stratified for management according to their risk? Derivation, external validation and outcomes using the updated GRACE risk score. BMJ Open. 2014;4(2): e004425.
D’Ascenzo F, Biondi-Zoccai G, Moretti C, Bollati M, Omede P, Sciuto F, Presutti DG, Modena MG, Gasparini M, Reed MJ, et al. TIMI, GRACE and alternative risk scores in acute coronary syndromes: a meta-analysis of 40 derivation studies on 216,552 patients and of 42 validation studies on 31,625 patients. Contemp Clin Trials. 2012;33(3):507–14.
Aragam KG, Tamhane UU, Kline-Rogers E, Li J, Fox KA, Goodman SG, Eagle KA, Gurm HS. Does simplicity compromise accuracy in ACS risk prediction? A retrospective analysis of the TIMI and GRACE risk scores. PLoS ONE. 2009;4(11): e7947.
Collet JP, Thiele H, Barbato E, Barthelemy O, Bauersachs J, Bhatt DL, Dendale P, Dorobantu M, Edvardsen T, Folliguet T, et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021;42(14):1289–367.
Hamm CW, Bassand JP, Agewall S, Bax J, Boersma E, Bueno H, Caso P, Dudek D, Gielen S, Huber K, et al. ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: the task force for the management of acute coronary syndromes (ACS) in patients presenting without persistent ST-segment elevation of the European society of cardiology (ESC). Eur Heart J. 2011;32(23):2999–3054.
Roffi M, Patrono C, Collet JP, Mueller C, Valgimigli M, Andreotti F, Bax JJ, Borger MA, Brotons C, Chew DP, et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: task force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European society of cardiology (ESC). Eur Heart J. 2016;37(3):267–315.
Thuijs DJFM, Kappetein AP, Serruys PW, Mohr F-W, Morice M-C, Mack MJ, Holmes DR, Curzen N, Davierwala P, Noack T, et al. Percutaneous coronary intervention versus coronary artery bypass grafting in patients with three-vessel or left main coronary artery disease: 10-year follow-up of the multicentre randomised controlled SYNTAX trial. The Lancet. 2019;394(10206):1325–34.
Keykhaei M, Ashraf H, Rashedi S, Farrokhpour H, Heidari B, Zokaei S, Bagheri S, Foroumadi R, Asgarian S, Amirian A, et al. Differences in the 2020 ESC versus 2015 ESC and 2014 ACC/AHA guidelines on the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Curr Atheroscler Rep. 2021;23(12):77.
Kolh P, Windecker S, Alfonso F, Collet JP, Cremer J, Falk V, Filippatos G, Hamm C, Head SJ, Jüni P, et al. 2014 ESC/EACTS guidelines on myocardial revascularization: the task force on myocardial revascularization of the European society of cardiology (ESC) and the European association for cardio-thoracic surgery (EACTS). Developed with the special contribution of the European association of percutaneous cardiovascular interventions (EAPCI). Eur J Cardiothorac Surg. 2014;46(4):517–92.
Virani SS, Alonso A, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Chang AR, Cheng S, Delling FN, et al. Heart disease and stroke statistics-2020 update: a report from the American heart association. Circulation. 2020;141(9):e139–596.
Eagle KA, Lim MJ, Dabbous OH, Pieper KS, Goldberg RJ, Van de Werf F, Goodman SG, Granger CB, Steg PG, Gore JM, et al. A validated prediction model for all forms of acute coronary syndrome: estimating the risk of 6-month postdischarge death in an international registry. JAMA. 2004;291(22):2727–33.
Granger CB, Goldberg RJ, Dabbous O, Pieper KS, Eagle KA, Cannon CP, Van De Werf F, Avezum A, Goodman SG, Flather MD, et al. Predictors of hospital mortality in the global registry of acute coronary events. Arch Intern Med. 2003;163(19):2345–53.
Fox KA, Dabbous OH, Goldberg RJ, Pieper KS, Eagle KA, Van de Werf F, Avezum A, Goodman SG, Flather MD, Anderson FA Jr, et al. Prediction of risk of death and myocardial infarction in the six months after presentation with acute coronary syndrome: prospective multinational observational study (GRACE). BMJ. 2006;333(7578):1091.
Rahmani R, Majidi B, Ariannejad H, Shafiee A. The value of the GRACE score for predicting the SYNTAX score in patients with unstable angina/Non-ST elevation myocardial Infarction. Cardiovasc Revasc Med. 2020;21(4):514–7.
Head SJ, Milojevic M, Daemen J, Ahn J-M, Boersma E, Christiansen EH, Domanski MJ, Farkouh ME, Flather M, Fuster V, et al. Mortality after coronary artery bypass grafting versus percutaneous coronary intervention with stenting for coronary artery disease: a pooled analysis of individual patient data. The Lancet. 2018;391(10124):939–48.
Takahashi K, Serruys PW, Gao C, Ono M, Wang R, Thuijs D, Mack MJ, Curzen N, Mohr FW, Davierwala P, et al. Ten-year all-cause death according to completeness of revascularization in patients with three-vessel disease or left main coronary artery disease: insights from the SYNTAX extended survival study. Circulation. 2021;144(2):96–109.
Safarian H, Alidoosti M, Shafiee A, Salarifar M, Poorhosseini H, Nematipour E. The SYNTAX score can predict major adverse cardiac events following percutaneous coronary intervention. Heart Views. 2014;15(4):99–105.
Chen SL, Han YL, Zhang YJ, Ye F, Liu HW, Zhang JJ, Xu B, Jiang TM, Zhou YJ, Lv SZ. The anatomic- and clinical-based NERS (new risk stratification) score II to predict clinical outcomes after stenting unprotected left main coronary artery disease: results from a multicenter, prospective, registry study. JACC Cardiovasc Interv. 2013;6(12):1233–41.
Younes Nozari AS, Kassaian SE, Jalali A, Roozbeh M, Safarian H. Effect of various degrees of chronic kidney disease on long-term outcome of patients with percutaneous coronary intervention. Arch Iran Med. 2019;22(5):247–51.
Khoury J, Bahouth F, Stabholz Y, Elias A, Mashiach T, Aronson D, Azzam ZS. Blood urea nitrogen variation upon admission and at discharge in patients with heart failure. ESC Heart Fail. 2019;6(4):809–16.
Ren X, Qu W, Zhang L, Liu M, Gao X, Gao Y, Cheng X, Xu W, Liu Y. Role of blood urea nitrogen in predicting the post-discharge prognosis in elderly patients with acute decompensated heart failure. Sci Rep. 2018;8(1):13507.
Jujo K, Minami Y, Haruki S, Matsue Y, Shimazaki K, Kadowaki H, Ishida I, Kambayashi K, Arashi H, Sekiguchi H, et al. Persistent high blood urea nitrogen level is associated with increased risk of cardiovascular events in patients with acute heart failure. ESC Heart Fail. 2017;4(4):545–53.
Freedman LS. Tables of the number of patients required in clinical trials using the logrank test. Stat Med. 1982;1:121–9.
Acknowledgements
Not applicable.
Funding
This study was supported by grants from the National Key Research & Development Program of China (2018YFA0107403) and Chongqing Natural Science Foundation (cstc2020jcyj-jqX0016).
Author information
Authors and Affiliations
Contributions
XC and HW conceived and designed the study, analyzed the data, and wrote the draft of the manuscript. XC XZ, and CZ collected clinical data and reviewed and edited the manuscript. LL and WW contributed to discussion and reviewed and edited the manuscript.All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was reviewed and approved by the Ethics Committee of Daping Hospital. All patients provided written informed consent, and this study was conducted in accordance with the Declaration of Helsinki. The identifying study participant information/images is not applicable.
Consent for publication
Not Applicable.
Competing interests
There are no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
. Supplemental information.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chen, X., Wu, H., Li, L. et al. The prognostic utility of GRACE risk score in predictive adverse cardiovascular outcomes in patients with NSTEMI and multivessel disease. BMC Cardiovasc Disord 22, 568 (2022). https://doi.org/10.1186/s12872-022-03025-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-022-03025-6