
Abstract
Purpose
We evaluated quality of life (QoL) in pregnant women who underwent transthoracic echocardiography-guided percutaneous closure of atrial septal defect (ASD).
Methods
A total of 45 pregnant women underwent transthoracic echocardiography-guided percutaneous closure of ASD. We assessed QoL using the 36-Item Short Form Survey (SF-36) and compared results between pre- and post-procedure patients, as well as between those with ASD and healthy women in their second and third trimesters of pregnancy.
Results
All patients showed improved right ventricular function and were classified as Class I, post-procedure. Mean SF-36 scores of the post-procedure group were better on all sub-scales than those of the pre-procedure group (p < 0.05), with the exception of role-emotional and mental health. Mean SF-36 scores for the pre-procedure group were also lower on all sub-scales than those of healthy pregnant controls (p < 0.05), with the exception of role physical, role emotional, and mental health. There was no difference between the post-procedure group and healthy pregnant controls. In a subgroup analysis, scores were better in some dimensions (social functioning and role emotional) for post-procedure patients in the 31–40 years of age group and the group on their second or third pregnancies than those of the 20–30 years of age group and the group on their first pregnancies (p < 0.05).
Conclusion
After closure of ASD, QoL in pregnant women was improved. In a subgroup analysis, the younger women and those on their first pregnancy performed more poorly in some dimensions (social functioning and role emotional); this suggested that these groups should receive more proactive intervention.
Plain English summary
Limited data was available on the general quality of life (QoL) in pregnant women with atrial septal defect (ASD), even though the condition could produce anxiety over health of the pregnancy and fetus. The percutaneous closure procedure was available for ASD during pregnancy; however, pregnant women were often concerned that the required X-rays would harm the fetus. A safe and effective procedure, percutaneous closure of ASD guided by transthoracic echocardiography, was widely used for this condition. This study used the 36-Item Short Form Survey (SF-36) to assess QoL in pregnant women with ASD pre- and post-procedure and compared the results to those of healthy pregnant women at a similar stage of pregnancy. Post-procedure QoL in pregnant women with ASD was improved; however, the younger women and those on their first pregnancy performed more poorly in some dimensions (social functioning and role emotional). Our results suggested that these groups should receive more proactive intervention.
Similar content being viewed by others


Introduction
Atrial septal defect (ASD) is a common congenital heart disease with a morbidity rate of 1/1000 [1]. Patients with ASD could go misdiagnosed if they did not present with clinical symptoms. However, when women entered pregnancy, circulating blood volume might increase by 40%–45%. At 32–34 weeks gestation, blood volume and cardiac load might reach a peak [2, 3]. In pregnant women with ASD, the left-to-right shunt was increased and the right atrium and right ventricle enlarged, which might lead to pulmonary hypertension and heart failure. Thus, for mis- or undiagnosed female patients of childbearing age, an ASD diagnosis often took place during pregnancy due to decreased cardiac function.
With the development of interventional technology, percutaneous closure of ASD guided by transthoracic echocardiography was now widely used in clinical practice. At present, many studies had evaluated the safety and efficiency of the technique [4,5,6] but scarce data had been reported about the quality of life (QoL) in pregnant women with ASD before and after this procedure. Depression and fear of disease might have a negative impact on the pregnant women’s QoL, and the curing of the disease might increase confidence and QoL.
In this study, we used the 36-Item Short Form Survey (SF-36) to assess QoL in pregnant women with ASD before and after procedure and compared the results with those of healthy women at a similar stage of pregnancy.
Methods
Patients
From January 2017 to January 2022, 45 pregnant women with ASD underwent percutaneous closure of ASD guided by transthoracic echocardiography. Right ventricular function was evaluated by echocardiography before and after the procedure, and 45 healthy pregnant women at similar stages of pregnancy were used as controls. Baseline characteristics were shown in Table 1. All pregnant women were diagnosed with ASD during the second trimester (20–24 weeks); the procedures were also performed during this period. The procedure indications for pregnant women with ASD were: (1) dyspnea symptoms; (2) cardiac function was grade II-III; 3) echocardiography indicated that the right ventricular function was impaired.
SF-36 Health Survey
The SF-36, used to assess the health-related QoL, consists of eight domains: physical functioning, role physical, bodily pain, general health, vitality, social functioning (SF), role emotional (RE), mental health [7].
The survey was conducted in the outpatient department of cardiovascular surgery for the patient group and in the outpatient department of obstetrics for the control group. All participants completed a short face-to-face interview and study questionnaire, which was completed in two periods. For the patient group, there was a pre-procedure period (in the second trimester) and post-procedure period (in the third trimester). For the control group, there was a second trimester and a third trimester.
We divided 45 patients into subgroups by age and number of pregnancy (i.e., ‘first’ alludes to a patient’s first pregnancy). We compared QoL between pre-procedure and post-procedure patients, between each post-operative subgroup, and between patients and healthy controls in the second and third trimesters of pregnancy.
Statistical analysis
Data are presented as numbers or percentages for categorical variables, while median and interquartile range or mean ± standard deviations were provided for continuous variables. The Mann–Whitney U test or Kruskal–Wallis test was used for continuous variables (pre-procedure data, post-procedure data, subgroup data, and healthy control data). Analysis was performed with SPSS version 22.0 (IBM Corp., Armonk, NY, USA). A p < 0.05 was set as statistically significant.
Results
Among the 45 participants, 26 were aged 20–30 years and 23 were on their first pregnancy. There was no difference between patients and healthy controls, with the exception of cardiac function classification by the New York Heart Association (NYHA) Functional Classification (Table 1). All post-procedure patients had improved functional status to a NYHA classification of Class I. The end-systolic length and width of the right atrium, the right ventricular systolic pressure, and the right ventricular Tei index were also decreased following the procedure. Additionally, the right ventricular ejection fraction was improved following the procedure. (p < 0.05) (Table 2).
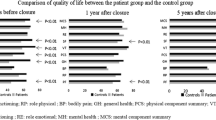
Pregnant women with ASD performed better in several measures post-procedure. Table 3 showed the significant differences between scores for pre-procedure and post-procedure data on all scales with the exception of role emotional and mental health (p < 0.05). In some domains (physical functioning, bodily pain, general health, vitality, and social functioning), there was a significant difference between the pre-procedure group and the healthy control group in the second trimester of pregnancy (p < 0.05) (Table 4). There was no difference between the post-procedure group and healthy pregnant controls in the third trimester (Table 5). In the subgroup analysis, the post-procedure participants in the 31–40 years of age group and the second or third pregnancy group scored better than the patients in the 20–30 years of age group and the first pregnancy group for the social functioning and role emotional dimensions (p < 0.05; Tables 6 and 7). In the 20–30 years of age subgroup and the first pregnancy subgroup, the healthy pregnant control group scored better than the post-procedure group for the role emotional dimension. (p < 0.05; Tables 8 and 10). In the 31–40 years of age subgroup and the second or third pregnancy subgroup, there was no difference between the healthy pregnant control group and the post-procedure group (Tables 9 and 11).
Discussion
This study found that QoL in pregnant women with ASD was improved overall following percutaneous closure of ASD with guidance by transthoracic echocardiography.
ASD was a common congenital heart disease for which percutaneous closure was the first-line procedure. However, patients with ASD who were pregnant comprise a special group. In pregnancy, circulating blood volume could increase, which, when combined with a left-to-right shunt can increase the load of the right ventricle and, in cases of large ASD, could lead to pulmonary hypertension and right ventricular dysfunction. Current guidelines recommended cardiological surveillance for all pregnant women with ASD as they were at risk (albeit a small risk) of paradoxical embolism, arrhythmia, and heart failure [8]. Further, percutaneous closure of ASD was an effective and safe procedure for this issue; however, although the time of X-ray fluoroscopy was very short, lasting only a few minutes, and the abdomen was covered with lead clothing, pregnant women were quite often concerned that X-rays will harm the fetus. Thus, guidance by transthoracic echocardiography had been developed for the safe and effective percutaneous closure of ASD [9, 10] as this procedure did not require X-ray fluoroscopy, eliminating radiation concerns.
In this study, we found that QoL in pregnant women with ASD before procedure was lower than that of healthy pregnant controls (in their second trimester). Additionally, QoL was greatly improved following the procedure and was no different from that of healthy pregnant women (in their third trimester). Pregnant women might experience nervousness and depression due to decreased cardiac function or fear of harm to the fetus, thus having a reduced QoL. In our study, participants with ASD underwent successful procedure without complications (arrhythmias, embolisms, or residual shunts). Post-procedure echocardiographic data also showed improvement of right ventricular function. In a previous study, Eroglu et al. [11] reported that the right ventricle was reconstructed 24 h after the closure of ASD, and that the clinical and hemodynamics of patients were improved and maintained during the long-term follow-up period [12, 13]. Additionally, Lazic et al. [14] had reported that the right side of the heart is associated with aerobic capacity. Therefore, owing to the improvement of heart function and the elimination of worry, the overall QoL of pregnant women was expected to improve following surgical closure of the ASD.
In this study, we found that post-procedure pregnant women in the 31–40 years of age and the second or third pregnancy groups had higher scores those in the 20–30 years of age and the first pregnancy groups in the social function and role emotional dimensions. These findings were consistent with previous reports in the literature. For example, García-Blanco et al. [15] reported that social functioning (family functioning, maternal attitudes, and social support) improved with age. McHorney et al. [16] reported that advanced maternal age women was associated with a six or more point increase in the social functioning or role emotional QoL domains. Further, Berryman et al. [17] showed that older pregnant women possessed a greater sense of preparedness and more flexible problem-solving capacities. Thus, it standed to reason that second or third pregnant women would perform better in these aspects due to their experience in pregnancy, suggesting that younger women and those on their first pregnancy should be provided more psychological intervention and social support.
Limitations
This study was not without limitations. First, the present study was a descriptive study with a limited sample size, which only reflected the status of pregnant women with ASD in one geographical area. Second, this was cross-sectional research and a longitudinal study should be designed in the future to assess QoL of pregnant individuals with ASD throughout pregnancy.
Conclusion
The post-procedure QoL of pregnant women with ASD was improved overall following percutaneous closure of ASD with guidance by transthoracic echocardiography, which might contribute to pregnancy care and postpartum recovery. In a subgroup analysis, younger pregnant women and women on their first pregnancy performed more poorly in the social functioning and role emotional dimensions, suggesting that these groups require more active psychological and physical support.
Availability of data and materials
All data generated or analysed during this study are included in this published article.
References
Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol. 2002;39:1890–900.
Toiano NH. Physiologic and hemodynamic changes during pregnacy. AACN Adv Crit Care. 2018;29(3):273–83.
Ouzounian JG, Elkayam U. Physiologic changes during normal pregnancy and delivery. Cardiol Clin. 2012;30(3):317–29.
Yang M-C, Jiunn-Ren Wu. Recent review of transcatheter closure of atrial septal defect. Kaohsiun J Med Sci. 2018;34(7):363–9.
Akseer S, Holick E, Vishwannath V, et al. Prevalence and outcomes of pulmonary hypertension after percutaneous closure of atrial septal defect: a systematic review and meta-analysis. Eur Respir Rev. 2020;29(158):2000099.
Lairakdomrong K, Srimahachota S, Lertsapcharoen P, et al. Clinical results of large secundum atrial septal defect closure in adult using percutaneous transcatheter cocoon atrial septal occluder. J Med Assoc Thai. 2013;96(9):1127–34.
Ware J, Snow K, Kosinski M, et al. SF-36 health survey: manual and interpretation guide. Boston, MA: The Health instituet, New England Medical Center; 1993.
Webb G, Gatzoulis MA. Atrial septal defects in the adult: recent progress and overview. Circulation. 2006;114(15):1645–53.
Ye Z, Li Z, Yi H, et al. Optimization of echo views for percutaneous device closure of pediatric atrial septal defect through the femoral vein guided by transthoracic echocardiography without radiation. J Interv Caardiol. 2020; 8242790.
Dou H, Kan T, Guo X, et al. Long-term follow-up of transthoracic echocardiography-guided transcathete closure of large atrial septal defects(≧30 mm) using the SHSMA occluder. Pediatr Cardiol. 2020;41(4):716–23.
Eroglu E, Cakal SD, Cakal B, et al. Time course of right ventricular remodeling after percutaneous atrial septal defect closure: assessment of regional deformation properties with two-dimensional strain and strain rate imaging. Echocardiography. 2013;30(3):324–30.
Takaya Y, Taniguchi M, Akagi T, et al. Long-term effects of transcatheter closure of atrial septal defect on cardiac remodeling and exercise capatity in patients older than 40 years with a reduction in cardiopulmonary function. J Interv Cardiol. 2013;26:195–9.
Jalal Z, Hascoët S, Gronier C, et al. Long-term outcomes after percutaneous closure of ostium secundum atrial septal defect in the young: a nationwide cohort study. JACC Cardiovasc Interv. 2018;11(8):795–804.
Lazic JS, Tadic M, Antic M, Radovanovic D. The relationship between right heart and aerobic capacity in large cohort of young elite athletes. Int J Cardiovasc Imaging. 2019;35(6):1027–36.
García-Blanco A, Monferrer A, Grimaldos J, et al. A preliminary study to assess the impact of maternal age on stress-related variables in healthy nulliparous women. Psychoneuroendocrinology. 2017;78:97–104.
McHorney CA, Ware JE Jr, Lu JF, Sherbourne CD. The MOS 36-item short-form health survey (SF-36): III Tests of data quality, scaling assumptions, and reliability across diverse patient groups. Med Care. 1994;32(1):40–66.
Berryman JC, Thorpe K, Windridge KC. Older mothers: Conception, pregnancy and birth after 35. Pandora Press; 1995.
Acknowledgements
None.
Funding
This work was funded by the National Natural Science Foundation of China (U2005202), the Natural Science Foundation of Fujian Province (2020J02056).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Zhen-Fnag Zong, Qing-Song Wu, Jun Xiao, Tian-Ci Cai, Xiao-Dong Chen, Yue Shen. The first draft of the manuscript was written by Zhi-Huang Qiu and Liang-Wan Chen, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
All participants were informed of the purpose and content of the study before participating. Written informed consent was obtained from all the participants. They were also informed that their participation was voluntary and that they had the right and freedom to withdraw from the study at any time without the need provide a reason. The process was completely anonymous. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the ethics Committee of the hospital.
Consent for publication
Not Applicable.
Competing interests
There was no financial or non-financial interests that are directly or indirectly related to the work submitted for publication. The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Qiu, ZH., Zong, ZF., Wu, QS. et al. Quality of life in pregnancy after percutaneous closure of atrial septal defect guided by transthoracic echocardiography. BMC Cardiovasc Disord 22, 550 (2022). https://doi.org/10.1186/s12872-022-02995-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-022-02995-x