
Abstract
Background
Cardiac epicardium hemangiomas are exceedingly rare; however, they can cause significant hemodynamic impairment and large pericardial effusions. On rare occasion, cardiac tumors coexist with malformations of the heart.
Case presentation
We present the case of a 10-month-old female infant with a rare cardiac surface hemangioma coexisting with malformations of the heart. It revealed an atrial septal defect (ASD) coexisting with an abnormal occupying lesion with high echogenicity. It was 35*12*9 mm in size and was found in the anterior atrioventricular junction to the posterior atrioventricular junction at the bottom of the ventricular septum by transthoracic echocardiography. We performed surgical treatment of the atrial septal defect and performed biopsy with the occupying lesion. The histopathological examination reported a benign tumor as hemangioma. As far as we know, this is the first case in which cardiac surface hemangioma was found to coexist with an atrial septal defect.
Conclusions
Cardiac epicardium hemangiomas is a rare solid tumor of the heart. If the mass is impossible to resect and does not cause hemodynamic impairment, only mass biopsy is possible.
Similar content being viewed by others


Background
Primary cardiac tumors are exceedingly rare in the pediatric population, with an estimated prevalence ranging from 0.027 to 0.49%, and cardiac hemangiomas are even rarer. Although cardiac hemangiomas are histologically benign and may even regress spontaneously, they can cause significant complications including large pericardial effusions, congestive heart failure, inflow or outflow tract obstructions, and disturbances in heart rhythm in some cases. Rarely, cardiac hemangiomas may also coexist with congenital heart lesions, in particular cardiac epicardium hemangiomas. Herein, we report a very rare case of a cardiac epicardium hemangiomas with atrial septal defect in a 10-month-old female infant.
Case presentation
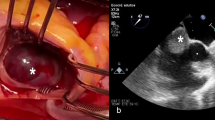
A 10-month-old female infant with history of pneumonia was diagnosed with a large atrial septal defect (ASD) 22*21 mm in size. The patient had a large atrial septal defect, a significant cardiac murmur, and recurrent pulmonary infections; additionally, the infant’s growth was significantly delayed and feeding was slightly difficult. Therefore, we decided to treat the child surgically because of the septal defect and the associated symptoms. When she underwent a routine pre-operation transthoracic echocardiography, it revealed an abnormal occupying lesion with high echogenicity 35*12*9 mm in size, stretching across from the anterior atrioventricular junction to the posterior atrioventricular junction at the bottom of the ventricular septal area. Transthoracic echocardiography revealed no hemodynamic changes due to the mass (Fig. 1A-C). A computerized tomography scan and positron emission tomography confirmed the presence of the mass in the same area (Fig. 2). The electrocardiogram showed sinus rhythm with incomplete right bundle branch block. Routine laboratory tests were ordered, and no abnormal results were found. No family history was obtained.

A Transthoracic echocardiogram obtained in the parasternal non-standard four-chamber view showing the mass with uneven echo. B Transthoracic echocardiogram obtained in the right ventricular inflow tract view showing the mass and the atrial septal defect (white arrow). C Transthoracic echocardiogram obtained in the Subxiphoid view showing the mass. D, E Transthoracic echocardiogram showing the mass that has developed two years after the surgery. MV, mitral valve; RV, right ventricle

Computerized tomography scan (A) and positron emission tomography (B, C) confirmed the presence of the mass in the same area (cross area)
We observed two keys of dealing with this patient. The first was that ASD should be surgically repaired because the size of the orifice was too large to close by a device alone. The second was the strategy to deal with the trickiest part-the occupying lesion. The mass was impossible to resect and only biopsy with the occupying lesion was possible because of the position and the type of mass. The histopathological examination reported a benign tumor as hemangioma, and the patient was discharged without any symptoms on the fourth day after surgery and the tumor was given observation therapy. In the two-year follow-up period, the patient remained asymptomatic, and the size of the tumor remained unchanged (Fig. 1D,E).
Discussion
Although ASD is the simplest congenital heart disease to repair, the optimal treatment timing for asymptomatic ASD is still unclear. However, most cardiologists agree that ASD with significant symptoms should be closed once the diagnosis is confirmed. In this case, transcatheter closure may not be feasible due to the large defect and early age.
The incidence of cardiac tumor is 0.02%, and 75% of them are benign. The most common heart tumor in infants is rhabdomyoma [1], which was the first thing we considered in this case. We changed our view when we opened the patient’s chest and saw the tumor (Fig. 3A). The tumor, which stretched across from the right atrial surface to the right ventricular surface, had an irregular shape and a rubbery consistency. This tumor could be touched from the anterior atrioventricular junction to the posterior atrioventricular junction along the bottom of the heart. We reconfirmed that this was an unresectable tumor and performed a biopsy.

A Thoracotomy revealed a mass stretching across from the right atrial surface to the right ventricular surface; the mass had an irregular shape and a rubbery consistency. B The histopathological examination indicated a benign tumor as hemangioma (hematoxylin-eosin staining)
The coexistence of cardiac tumors and malformations of the heart may confuse physicians regarding the origin of the symptoms [2]. Some reports suggest that a space-occupying lesion may be associated with, or possibly induce, a malformation within the developing heart in some circumstances [2]. In this case, it was important to determine the histological characteristics of the tumor which may involve changes in hemodynamics or electrocardiogram results in the future. If a simple cardiac tumor is present, the ancillary tests become even more important. In this case, transthoracic echocardiograms and cardiac computerized tomography angiography(CTA) were done first after the child was admitted to the hospital. Transthoracic echocardiograms were the first to detect the cardiac mass, while the cardiac CTA did not indicate the cardiac mass, suggesting that cardiac CTA is not sensitive to hemangiomas. An MRI was not performed in this case, and we believe that cardiac MRI may have greater advantages in evaluating cardiac function and myocardial lesions. The most important test in this case was PET-CT, which determines the nature of the mass, its benignity and malignancy, and the presence of metastases.
The histopathological examination indicated a benign tumor, specifically a hemangioma (Fig. 3B). Hemangiomas in the heart are heterogenous with only a few present at birth or in infancy [3]. Only very few primary tumors and cysts of the pericardium, which are rare, are cardiac hemangiomas [4]. In children, the most common site of hemangioma is the right atrium, which may cause hydrops and cardiac tamponade because of large pericardial effusions [1]. Other common symptoms of hemangioma are atrial obstruction and changes in the electrocardiogram. In this case, no pericardial effusions were detected in surgery and no obstruction by the tumor was observed in echocardiography and no particular changes were observed in the electrocardiogram or electrocardiogram examination.
All symptomatic and hemodynamically compromised patients require surgical treatment [5]. Complete resection or even partial resection of benign cardiac tumors can provide strong early and long-term results. Nevertheless, only cardiac transplant should be considered for unresectable cardiac masses like this case if they seriously impair cardiac function [5]. In this case, we believe there was no impairment of cardiac function and therefore no need for resection of this tumor.
Conclusion
Cardiac epicardium hemangiomas is a rare solid tumor of the heart. If the mass is impossible to resect and does not cause hemodynamic impairment, only mass biopsy is possible.
Availability of data and materials
The raw data supporting the conclusions of this article will be made available by the corresponding authors, without undue reservation.
Abbreviations
- ASD:
-
Atrial septal defect
- CTA:
-
Computerized tomography angiography
References
Burke A, Tavora F. The 2015 WHO classification of tumors of the heart and pericardium. J THORAC ONCOL. 2016;11(4):441–52.
Djordjevic SA, Glumac S, Kalanj J. Cardiac haemangioma associated with a duct-dependent congenital heart disease in a newborn infant. CARDIOL YOUNG. 2017;27(5):990–2.
Burke A, Johns JP, Virmani R. Hemangiomas of the heart. A clinicopathologic study of ten cases. Am J Cardiovasc Pathol. 1990;3(4):283–90.
Mackie AS, Kozakewich HP, Geva T, Perez-Atayde AR, Mulliken JB. Vascular tumors of the heart in infants and children: case series and review of the literature. Pediatr Cardiol. 2005;26(4):344–9.
Padalino MA, Vida VL, Boccuzzo G, Tonello M, Sarris GE, Berggren H, Comas JV, Di Carlo D, Di Donato RM, Ebels T, Hraska V, Jacobs JP, Gaynor JW, Metras D, Pretre R, Pozzi M, Rubay J, Sairanen H, Schreiber C, Maruszewski B, Basso C, Stellin G. Surgery for primary cardiac tumors in children: early and late results in a multicenter European Congenital Heart Surgeons Association study. Circulation. 2012;126(1):22–30.
Acknowledgements
We thank LetPub (www.letpub.com) for its linguistic assistance during the preparation of this manuscript.
Funding
This study was supported by the National Natural Science Foundation of China (2018SK2132).
Author information
Authors and Affiliations
Contributions
SJH, TLZ and QW were responsible for the diagnosis and treatment of the patient. JLC prepared the manuscript. XYG and LX collected the clinical data. All the authors have read and approved the final manuscript and have agreed to be accountable for the content of the work. All authors contributed to the article and approved the submitted version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical review and approval were not required for this study on human participants according to local legislation and institutional requirements. Written informed consent to participate in this study was provided by the participant’s legal guardians.
Consent for publication
The patient’s legal guardians gave written informed consent to publish this manuscript.
Competing interests
None declared.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chen, J., Gong, X., Xie, L. et al. Atrial septal defect with a rare occupying lesion in heart. BMC Cardiovasc Disord 22, 482 (2022). https://doi.org/10.1186/s12872-022-02919-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-022-02919-9