
Abstract
Background
Endothelial dysfunction is common in diabetes. Apolipoprotein (apo) A-IV functions to antagonize inflammation and oxidative stress. The present study aimed to investigate the relationship between flow-mediated dilation (FMD) and serum apoA-IV level in type 2 diabetes mellitus (T2DM) patients.
Methods
A total of 84 T2DM patients with chest discomfort were enrolled in this study. Their baseline characteristics and clinical parameters were documented. Endothelial function of the participants was evaluated by examining FMD of brachial artery. The severity of coronary atherosclerosis was determined by quantitative coronary angiography. Serum apoA-IV levels were measured by ELISA.
Results
These diabetic patients were dichotomized into low FMD (n = 42) and high FMD (n = 42) groups. Serum apoA-IV levels were significantly higher in high FMD group than in low FMD group (29.96 ± 13.17 vs 17.69 ± 9.16 mg/dL, P < 0.001). Moreover, the patients were also categorized into three apoA-IV tertile groups. FMD was significantly different across three apoA-IV tertiles (P < 0.001). Serum apoA-IV levels were positively correlated to FMD (r = 0.469, P < 0.001). Logistic regression analysis was performed to determine risk factors for low FMD. apoA-IV levels together with the risk factor hsCRP remained significantly to be independent determinants of low FMD (P < 0.01). Linear regression analysis was performed, and apoA-IV levels together with total-to-HDL cholesterol ratio were independently correlated with FMD (P < 0.01).
Conclusions
Serum apoA-IV levels are associated with FMD, suggesting that apoA-IV protects endothelial function in patients with T2DM.
Similar content being viewed by others

Introduction
Diabetes is a crucial risk factor for atherosclerosis. Diabetes induces formation of advanced glycated end-product formation, oxidative stress and chronic inflammation, leading to arterial endothelial dysfunction and development of atherosclerotic cardiovascular diseases [1, 2]. Impairment of endothelial function precedes structural changes of atherosclerosis and plays a central role throughout the whole process of atherosclerosis [3, 4]. Test of endothelial function allows ascertainment of arterial physiology and pathology status. Flow-mediated dilation (FMD) is a non-invasive tool for examining peripheral artery endothelium-dependent dilation with high-resolution ultrasonography. The dilation is largely nitric oxide (NO)-mediated process in response to sudden increase in blood flow or shear stress [5,6,7]. FMD relates to endothelial function and independently predicts cardiovascular events [8].
ApoA-IV is a glycoprotein synthesized mainly by the small intestine [9]. The majority of circulating apoA-IV is lipid-free or associated with chylomicrons, with a minor portion related to HDL [10]. ApoA-IV has been proved to be atheroprotective due to positive role in reverse cholesterol transport [11, 12], intestinal lipid absorption [13], glucose homeostasis, insulin secretion [14] and the properties of anti-oxidation and anti-inflammation [15, 16]. However, the relation of apoA-IV and endothelial function remains unclear, especially in diabetic milieu of which vascular endothelium is probably impaired.
Thus, the present study investigated the relationship between vascular endothelial function and serum apoA-IV levels in patients with T2DM. The endothelial function of diabetic patients was evaluated by examining FMD. Serum apoA-IV levels were determined by ELISA.
Methods
The study followed the principles of outlined in the Declaration of Helsinki, and written informed consent was obtained from all participants.
Study population and samples
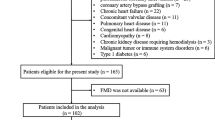
A total of 161 T2DM patients with paroxysmal chest discomfort undergoing coronary angiography from July 2019 to May 2020 for the diagnosis of coronary artery disease were enrolled in the present study. For the purpose of research, we excluded patients with following diseases including acute coronary syndrome (n = 19), history of coronary revascularization (n = 16), chronic heart failure (n = 10), concomitant valvular disease (n = 5), pulmonary heart disease (n = 8), congenital heart disease or cardiomyopathy (n = 9), renal failure requiring hemodialysis (n = 3) and malignant tumor or immune system disorders (n = 7). In the end, 84 patients were enrolled (Fig. 1).

Flowchart of patient enrollment
Serum samples were obtained from patients after 12 h fasting. These samples were stored at − 80 °C until analysis.
Coronary angiography
Coronary angiography was performed through the femoral or radial approach, using the Cardiovascular Measurement System version 3.0 software (Terra, GE, USA). All angiograms were reviewed by two experienced interventional cardiologists, both of whom were blinded to the study protocol and clinical data. A judgment was made by a third cardiologist if these two doctors had disagreement on lesion severity. The analysis of coronary lesion was performed as described previously [17].
Flow-mediated dilation
FMD on brachial artery of right upper arm was evaluated by an experienced ultrasound doctor, who was blinded to study design and clinical data of the participants, by using a high-resolution ultrasound machine with a 10‐MHz linear array probe and the GE Vivid 7 Imaging System following the recommended protocol [18, 19]. Briefly, the process was to measure the brachial artery diameter by recording the distance between the proximal and distal end of the intimal at the end of diastole (gated by R wave on electrocardiogram). The blood pressure cuff was banded distal to the imaged artery and held inflated on patients’ right upper arm for 5 min at 200 mmHg with the help of an assistant. FMD measurements were taken continuously from deflation for no less than 3 min. Baselines were recorded before inflation at the same artery segment under quiet and temperature-controlled circumstances for at least 1 min. The final FMD data is calculated as ratio of maximum brachial artery dilation to the baseline value.
ApoA-IV measurement
Serum apoA-IV levels were measured with HUMAN APOLIPOPROTEIN IV (ApoA4) ELISA kit (SK00401-01) according to the instructions provided by the manufacturer (AVISCERA BIOSCIENCE, INC.). ApoA-IV levels were determined by comparing OD values on 450 nm with a standard curve of gradient dilution of human recombinant apoA-IV protein. ApoA-IV levels were presented as mg/dL.
Statistical analyses
Continuous variables are presented as mean ± standard deviation (SD), and categorical data are summarized as frequency (percentage). For continuous variables, normal distribution was evaluated with the Kolmogorov–Smirnov test. Differences among groups were analyzed by one-way analysis of variance (ANOVA) and significance of trend was analyzed by linear ANOVA. For categorical clinical variables, differences between groups were evaluated by the linear chi-square test or Fisher’s exact test. Correlation between factors was analyzed by Pearson correlation test. Multivariable logistic regression models were performed to assess the independent determinants of FMD without (Model 1) and with apoA-IV (Model 2). Multivariable linear regression was performed to assess independent factors correlated with FMD. Overall significance level (2-tailed) of 0.05 was set as criterion. All statistical analyses and figures were performed with IBM SPSS Version 26 for Mac (IBM SPSS Inc, Chicago, IL, USA), Prism 9 for macOS (1994—2021 GraphPad Software, LLC) and Adobe Illustrator 23.1.1.
Results
Serum apoA-IV levels are higher in diabetic patients with high FMD, and FMD is significant different across three apoA-IV tertiles
The diabetic patients (n = 84) were dichotomized into low FMD (n = 42, 1.26% ~ 5.88%) and high FMD (n = 42, 5.88% ~ 13.58%) groups. The baseline characteristics and clinical parameters of these two FMD groups were detailed in Table 1A. Elder age and high apoB level were observed in low FMD group as compared with high FMD group. Notably, serum apoA-IV levels were significantly higher in high FMD group than in low FMD group (29.96 ± 13.17 vs. 17.69 ± 9.16, P < 0.001).
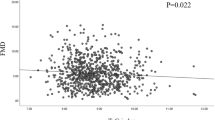
These diabetic patients (n = 84) were also categorized into three apoA-IV tertile groups (Table 1B), with the range of three ApoA-IV tertiles as follow, tertile 1, < 16.87 mg/dL; tertile 2, 16.87–29.60 mg/dL and tertile 3, > 29.60 mg/dL. Significant difference regarding age (P < 0.05) and fasting blood glucose (P < 0.01) was observed among the three tertile groups. Importantly, FMD (P < 0.001) was significantly different across the three apoA-IV tertiles (Fig. 2A). Moreover, Serum apoA-IV levels were positively correlated to FMD in all the diabetic patients (r = 0.469, P < 0.001) (Fig. 2B). As for the severity of CAD, Gensini score and SYNTAX score were both observed declining from apoA-IV tertile 1 to tertile 3, though the trends weren’t statistically significant.

FMD and apoA-IV. (A) FMD distribution in apoA-IV tertiles in diabetic patients; (B) Correlation between FMD and apoA-IV in diabetic patients
Decreased ApoA-IV level is an independent determinant of low FMD in patients with T2DM
We performed logistic regression analyses to determine risk factors for low FMD. In model 1 (Table 2), major risk factors in Table 1 including male, age, BMI, hypertension, smoking, eGFR, hsCRP, HbA1c, HOMA-IR, DM duration, and total-to-HDL cholesterol ratio were included. The result showed that hsCRP (OR = 1.469, 95%CI 0.993–2.171, P < 0.05) was significantly associated with low FMD. In model 2, apoA-IV was included together with the other risk factors in model 1. Decreased ApoA-IV (OR = 0.906, 95%CI 0.856–0.959, P < 0.01) and hsCRP (OR = 1.621, 95%CI 1.018–2.580, P < 0.05) remained significantly to be independent determinants of low FMD, with calibrations of both models as follows, P = 0.872 for Model 1 and P = 0.930 for Model 2 in Hosmer–Lemeshow test. The addition of apoA-IV in Model 2 significantly improved predictive performance with an increase of Nagelkerke R2 by 17.8%. In multiple linear regression analysis, apoA-IV (β = 0.407, P < 0.001) and total-to-HDL cholesterol ratio (β = -0.258, P < 0.01) were independently correlated with FMD (Table 3).
In addition, the cut-off point of apoA-IV in predicting low FMD was 20.57 mg/dL, with sensitivity 78.57% and specificity 69.05% (Fig. 3A). ROC curves for both models (Fig. 3B) showed that the addition of apoA-IV in Model 2 effectively elevated AUC (AUC = 0.79, 95% CI 0.68–0.87 P < 0.001), comparing with Model 1 (AUC = 0.87, 95% CI 0.76–0.92 P < 0.001) (P = 0.049).

ROC curves. (A) ROC of apoA-IV for detecting low FMD in diabetic patients; (B) ROC of Model 1 and Model 2 for detecting low FMD in diabetic patients
Discussion
ApoA-IV is a cardiovascular protective factor and exerts anti-inflammatory and anti-oxidative stress effects [11,12,13,14,15,16]. The present study has demonstrated that serum apoA-IV levels are significantly associated with FMD in T2DM patients. Serum apoA-IV levels are higher in patients with high FMD. In logistic analysis, decreased serum apoA-IV level was an independent determinant of low FMD in T2DM patients. In linear regression analysis, apoA-IV was independently correlated with FMD. Our findings have suggested a notion that apoA-IV protects endothelial function as represented by FMD in diabetic patients, consistent with previous evidence [11,12,13,14,15,16].
It has been evidenced that the endothelial function is the main element of vascular homeostasis regarding vasoconstriction-vasodilation regulation, anti-inflammatory and anticoagulant properties. Among endothelium-derived mediators, nitric oxide suppresses cell inflammation and inflammatory cell adhesion, inhibits thrombosis, facilitates blood flow, and limits vessel wall remodeling [20]. Endothelial dysfunction is a diffuse vascular disorder characterized by reduced NO bioavailability. It occurs at early stage of atherosclerosis, and progresses throughout the whole atherosclerosis process, which significantly aggravates under diabetic condition [21]. FMD of peripheral conduit arteries is one of the common tests for endothelial function. Previous study shows that FMD is lower in T2DM group versus control group [22]. FMD surveillance may have prognostic significance. Since FMD responds rapidly to treatment, it is used to verify drug efficacy and to evaluate bioactive substances [23].
In the present study, serum apoA-IV levels were positively associated with FMD in T2DM patients and decreased apoA-IV level was an independent determinant of low FMD in diabetic patients in logistic regression analysis. Our results suggest that apoA-IV protects endothelial function and subsequently prevent atherogenesis, which is consistent with previous studies [11,12,13,14,15,16]. Previous researches have also demonstrated that in animal models, apoA-IV transgenic mice reveal remarkable attenuation in atherogenesis after western diet as compared with control mice [24]. ApoE-/- mice with overexpression or infusion of human apoA-IV manifest less atherosclerotic lesions with steady fiber cap and smaller lipid core [16, 25, 26]. In human, serum apoA-IV concentrations negatively correlate with CAD in Caucasian, Asian Indian and Chinese population [27, 28] and also with chronic kidney disease in a prospective cohort study [29]. Our findings add novel information regarding apoA-IV function, jointly supporting apoA-IV as a cardiovascular protective factor.
Limitations of the study
First, the study is a cross-sectional study, aiming to investigate the relationship between FMD and apoA-IV, but not causative links. Second, apoA-IV has various modification forms in diabetic patients, which may influence the biological functions of apoA-IV [17]. In our future studies, prospective study regarding the relation of endothelial function and apoA-IV level or modifications of apoA-IV will be done.
Conclusion
Serum apoA-IV levels are associated with FMD in patients with T2DM, suggesting that apoA-IV protects endothelial function in patients with T2DM.
Availability of data and materials
The datasets generated and/or analysed during the current study are not publicly available due to patients’ privacy protection, but are available from the corresponding author on reasonable request.
References
Johnstone MT, Creager SJ, Scales KM, Cusco JA, Lee BK, Creager MA. Impaired endothelium-dependent vasodilation in patients with insulin-dependent diabetes mellitus. Circulation. 1993;88(6):2510–6.
Polovina MM, Potpara TS. Endothelial dysfunction in metabolic and vascular disorders. Postgrad Med. 2014;126(2):38–53.
Deanfield JE, Halcox JP, Rabelink TJ. Endothelial function and dysfunction: testing and clinical relevance. Circulation. 2007;115(10):1285–95.
Lahoz C, Mostaza JM. Atherosclerosis as a systemic disease. Rev Esp Cardiol. 2007;60(2):184–95.
Green DJ, Hopman MT, Padilla J, Laughlin MH, Thijssen DH. Vascular Adaptation to Exercise in Humans: Role of Hemodynamic Stimuli. Physiol Rev. 2017;97(2):495–528.
Celermajer DS, Sorensen KE, Gooch VM, Spiegelhalter DJ, Miller OI, Sullivan ID, et al. Non-invasive detection of endothelial dysfunction in children and adults at risk of atherosclerosis. Lancet. 1992;340(8828):1111–5.
Pyke KE, Tschakovsky ME. The relationship between shear stress and flow-mediated dilatation: implications for the assessment of endothelial function. J Physiol. 2005;568(Pt 2):357–69.
Ras RT, Streppel MT, Draijer R, Zock PL. Flow-mediated dilation and cardiovascular risk prediction: a systematic review with meta-analysis. Int J Cardiol. 2013;168(1):344–51.
Utermann G, Beisiegel U. Apolipoprotein A-IV: a protein occurring in human mesenteric lymph chylomicrons and free in plasma. Isolation and quantification Eur J Biochem. 1979;99(2):333–43.
Green PH, Glickman RM, Riley JW, Quinet E. Human apolipoprotein A-IV. Intestinal origin and distribution in plasma. J Clin Invest. 1980;65(4):911–9.
Guyard-Dangremont V, Lagrost L, Gambert P. Comparative effects of purified apolipoproteins A-I, A-II, and A-IV on cholesteryl ester transfer protein activity. J Lipid Res. 1994;35(6):982–92.
von Eckardstein A, Huang Y, Wu S, Sarmadi AS, Schwarz S, Steinmetz A, Assmann G. Lipoproteins containing apolipoprotein A-IV but not apolipoprotein A-I take up and esterify cell-derived cholesterol in plasma. Arterioscler Thromb Vasc Biol. 1995;15(10):1755–63.
Kohan AB, Wang F, Li X, et al. Apolipoprotein A-IV regulates chylomicron metabolism-mechanism and function. Am J Physiol Gastrointest Liver Physiol. 2012;302(6):G628–36.
Wang F, Li X, Bradshaw S, Yang Q, Caldwell JL, et al. Apolipoprotein A-IV improves glucose homeostasis by enhancing insulin secretion. Proc Natl Acad Sci U S A. 2012;109(24):9641–6.
Wang F, Kohan AB, Lo CM, Liu M, Howles P, Tso P. Apolipoprotein A-IV: a protein intimately involved in metabolism. J Lipid Res. 2015;56(8):1403–18.
Ostos MA, Conconi M, Vergnes L, Baroukh N, Ribalta J, Girona J, et al. Antioxidative and antiatherosclerotic effects of human apolipoprotein A-IV in apolipoprotein E-deficient mice. Arterioscler Thromb Vasc Biol. 2001;21(6):1023–8.
Dai Y, Shen Y, Li QR, Ding FH, Wang XQ, Liu HJ, et al. Glycated Apolipoprotein A-IV Induces Atherogenesis in Patients With CAD in Type 2 Diabetes. J Am Coll Cardiol. 2017;70(16):2006–19.
Thijssen DH, Black MA, Pyke KE, Padilla J, Atkinson G, Harris RA, et al. Assessment of flow-mediated dilation in humans: a methodological and physiological guideline. Am J Physiol Heart Circ Physiol. 2011;300(1):H2-12.
Corretti MC, Anderson TJ, Benjamin EJ, Celermajer D, Charbonneau F, Creager MA, et al. International Brachial Artery Reactivity Task Force Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: a report of the International Brachial Artery Reactivity Task Force. J Am Coll Cardiol. 2002;39(2):257–65.
Ghimire K, Altmann HM, Straub AC, Isenberg JS. Nitric oxide: what’s new to NO? Am J Physiol Cell Physiol. 2017;312(3):C254–62.
Villano A, Mencarelli E, Melita V, Rizzi A, Lamendola P, De Vita A, et al. Endothelial dysfunction and cardiovascular outcome in asymptomatic patients with type 2 diabetes: A pilot study. Diabetes Metab Res Rev. 2020;36(1):e3215.
Tai H, Jiang XL, Yao SC, Liu Y, Wei H, Li LB, et al. Vascular Endothelial Function as a Valid Predictor of Variations in Pulmonary Function in T2DM Patients Without Related Complications. Front Endocrinol (Lausanne). 2021;12:622768.
Lüscher TF, Taddei S, Kaski JC, Jukema JW, Kallend D, Münzel T, et al. Vascular effects and safety of dalcetrapib in patients with or at risk of coronary heart disease: the dal-VESSEL randomized clinical trial. Eur Heart J. 2012;33(7):857–65.
Cohen RD, Castellani LW, Qiao JH, Van Lenten BJ, Lusis AJ, Reue K. Reduced aortic lesions and elevated high density lipoprotein levels in transgenic mice overexpressing mouse apolipoprotein A-IV. J Clin Invest. 1997;99(8):1906–16.
Duverger N, Tremp G, Caillaud JM, Emmanuel F, Castro G, Fruchart JC, et al. Protection against atherogenesis in mice mediated by human apolipoprotein A-IV. Science. 1996;273(5277):966–8.
Geronimo FRB, Barter PJ, Rye KA, Heather AK, Shearston KD, Rodgers KJ. Plaque stabilizing effects of apolipoprotein A-IV. Atherosclerosis. 2016;251:39–46.
Kronenberg F, Stühlinger M, Trenkwalder E, Geethanjali FS, Pachinger O, von Eckardstein A, et al. Low apolipoprotein A-IV plasma concentrations in men with coronary artery disease. J Am Coll Cardiol. 2000;36(3):751–7.
Manpuya MW, Guo J, Zhao Y. The relationship between plasma apolipoprotein A-IV levels and coronary heart disease. Chin Med J (Engl). 2001;114(3):275–9.
Schwaiger JP, Kollerits B, Steinbrenner I, Weissensteiner H, Schönherr S, Forer L, et al. Apolipoprotein A-IV concentrations and clinical outcomes in a large chronic kidney disease cohort: Results from the GCKD study. J Intern Med. 2022;291(5):622–36.
Acknowledgements
None.
Funding
No funding.
Author information
Authors and Affiliations
Contributions
YD, LL: Conceptualization; LYL: Data Analysis, Writing- Original Draft Preparation; CS: Data Analysis; LYL, SC, YXW, RJ, XQW, FHD, QJC: Data Collection; LL and YD: Supervision, Writing-Review & Editing. The author(s) read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study followed the principles of outlined in the Declaration of Helsinki. The study protocol was approved by the Ruijin Hospital and Shanghai Jiao Tong University School of Medicine Ethics Committee. Trial number: NCT02089360. Written informed consent was obtained from all participants.
Consent for publication
Not applicable.
Competing interests
None by any of the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, LY., Chen, S., Wang, YX. et al. Serum apolipoprotein A-IV levels are associated with flow-mediated dilation in patients with type 2 diabetes mellitus. BMC Cardiovasc Disord 22, 446 (2022). https://doi.org/10.1186/s12872-022-02898-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-022-02898-x