
Abstract
Background
Despite use of drug-eluting stents (DES), in-stent restenosis (ISR) continues adversely affecting clinical outcomes of patients undergoing percutaneous coronary intervention (PCI). Apolipoprotein A-I (apoA-I) has athero-protective effects. However, there is a paucity of clinical data regarding the association between apoA-I and ISR. We sought to investigate whether serum apoA-I is related to ISR after DES-based PCI.
Methods
In this retrospective case control study, 604 consecutive patients who underwent DES implantation before were enrolled. Patients who underwent repeat angiography within 12 months were included in the early ISR study (n = 205), while those beyond 12 months were included in the late ISR study (n = 399). ISR was defined as the presence of > 50% diameter stenosis at the stent site or at its edges. Clinical characteristics were compared between ISR and non-ISR patients in the early and late ISR study, respectively, after adjusting for confounding factors by multivariate logistic regression, stratified analysis, and propensity score matching. The predictive value was assessed by univariate and multivariate logistic regression analysis, receiver operating characteristic (ROC) curve analysis, and quartile analysis.
Results
In the early ISR study, 8.8% (18 of 205) patients developed ISR. Serum apoA-I in the ISR group was lower than that in the non-ISR group (1.1 ± 0.26 vs. 1.24 ± 0.23, P < 0.05). On multivariate logistic regression analysis, apoA-I was an independent risk factor for early ISR. Incidence of early ISR showed negative correlation with apoA-I and could be predicted by the combined use of apoA-I and glycosylated hemoglobin (HbA1c) level. In the late ISR study, 21.8% (87 of 399) patients developed ISR. On subgroup analysis, late ISR showed negative correlation with apoA-I irrespective of intensive lipid lowering; on multivariate logistic regression analysis, apoA-I was also an independent risk factor for late ISR. In patients with intensive lipid lowering, combined use of apoA-I, stenting time, and diabetes predicted the incidence of late ISR.
Conclusions
ApoA-I was an independent risk factor for ISR, and showed a negative correlation with ISR after DES-based PCI. Combined use of apoA-I and clinical indicators may better predict the incidence of ISR under certain circumstances.
Similar content being viewed by others


Background
Despite extensive use of drug-eluting stents (DES), in-stent restenosis (ISR) continues to be a significant problem affecting 5–10% of patients undergoing percutaneous coronary intervention (PCI). ISR has been shown to be an independent risk factor for major adverse cardiac events (MACE) and poor long-term clinical outcomes after DES-based PCI [1,2,3]. The recent advances in intracoronary imaging, including intravascular ultrasound (IVUS) and optical coherence tomography (OCT), have helped unravel the pathophysiological mechanisms of ISR. Early ISR (i.e., ISR occurring within 12 months after implantation) is mainly caused by vascular endothelial deprivation and neointimal hyperplasia, while late ISR (i.e., ISR occurring beyond 12 months after deployment) is predominantly related to neo-atherosclerosis [4,5,6,7]. Previous studies have shown that 3–20% of patients will develop early or late ISR after implantation of new-generation DES together with intensive lipid-lowering therapy [8,9,10,11,12]. This highlights the clinical relevance of preventing ISR.
Apolipoprotein A-I (apoA-I), the major protein component of high-density lipoprotein cholesterol (HDL-C), is mainly involved in cholesterol reverse transport, and plays a pivotal role in the regulation of lipid metabolism. In recent animal studies, apoA-I was shown to decrease the occurrence and progression of neo-atherosclerosis and ISR by inhibiting inflammation, smooth muscle cell (SMC) proliferation, angiogenesis, and platelet activation [13,14,15,16,17,18,19]. However, there is a paucity of clinical data regarding the association of apoA-I with ISR in patients with coronary heart disease undergoing PCI with DES implantation. In this study, we sought to investigate whether serum apoA-I is related to early and late ISR after DES-based PCI.
Methods
Study population
A total of 743 consecutive patients who received repeat coronary angiography within or beyond 12 months of initial DES-based PCI for de novo coronary lesions, were screened from the database of Shanghai East Hospital from January 2019 to December 2019. Of these, 139 patients were excluded because of the following exclusion criteria: PCI within the last 6 month (n = 23); chronic total occlusion (CTO) (n = 16); bifurcation lesion with dual stent strategy (n = 16); long lesion with stents in a series (n = 15); implantation of biodegradable vascular scaffold (BVS) (n = 9); intervention for saphenous vein graft (SVG) stenosis (n = 4); renal failure requiring hemodialysis (n = 9); malignant tumor or immune system disorders (n = 12); and non-availability of lipid profile data (n = 35). Thus, the remaining 604 patients were included in the final analysis. Among these, 205 patients underwent repeat angiography within 12 months of initial DES-based PCI (early ISR study) and 399 underwent repeat angiography beyond 12 months after initial procedure (late ISR study) (Fig. 1).

Flowchart of patient enrollment
Data collection
Demographic and clinical characteristics including age, sex, risk factors for coronary artery disease (smoking, hypertension, diabetes, hyperlipidemia), and medication history were collected. Serum lipid profile and levels of creatinine, high-sensitivity C-reactive protein, and glycosylated hemoglobin (HbA1c) were determined using standard laboratory techniques. Glomerular filtration rate (GFR) was estimated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation [20]. Left ventricular ejection fraction (LVEF) was assessed by two-dimensional echocardiography according to the modified Simpson’s rule.
Coronary angiography and intervention
The initial coronary angiography and PCI with stent implantation as well as the repeat coronary angiography were performed using the standard technique described previously [21]. Selective coronary angiography was performed in different views (at least two orthogonal views for each segment of the coronary). The choice of DES was at the discretion of the operator. Pre-dilation and post-dilation were routinely performed during stent implantation with standard manipulation. However, nitroglycerin was routinely used to exclude coronary spasm. Initial PCI-related information was summarized, such as stenting time (time from initial PCI), lesion distribution, number of stents used, stent diameter, and stent length. The results of repeat coronary angiography were reviewed by two experienced interventional cardiologists, who were blinded to the patients' clinical data, using quantitative coronary angiography (QCA). ISR was defined as the presence of > 50% diameter stenosis on angiography at the stent site or at its edges (adjacent 5 mm segments).
Statistical analysis
Normally distributed continuous variables are presented as mean ± standard deviation and between-group differences assessed using two independent samples t test. Non-normally distributed continuous variables are presented as median (interquartile range) and between-group differences assessed using the Mann Whitney U-test. Categorical variables are presented as frequency (percentage) and between-group differences assessed using the Chi squared test. Pearson’s correlation was used to assess the correlation between normally distributed continuous variables. Spearman’s correlation was used to assess correlation of stenting time with age, lipid profile, or HbA1c level; Kendall's Tau-b method was employed to assess the correlation between sex, hypertension, diabetes, smoking status, and other categorical variables or between categorical variables and other continuous variables.
Univariate logistic regression was used to identify the risk factors for ISR. Multivariate logistic regression was performed to identify the independent risk factors and odds ratio with 95% confidence interval (CI) were calculated after adjusting for age, sex, hypertension, diabetes, smoking status, and significant variables in the univariate analysis. Receiver operating characteristic (ROC) curve analysis was performed to assess the ability of apoA-I alone or in combination with other significant variables to distinguish between ISR group and non-ISR group; the optimal cut-off values as well as the corresponding area under the curve (AUC) were calculated. Net reclassification index (NRI) and integrated discrimination improvement (IDI) were used to determine the optimal prediction model. P for trend was calculated using quartile analysis to assess any linear correlation between apoA-I and ISR.
Propensity score matching (PSM) was performed in a 1:1 ratio, using different clinical characteristics (such as sex, age, stenting time, hypertension, diabetes, and smoking) and laboratory parameters as matching variables, and using 0.1 or 0.05 as the calipers, according to the sample size. Thus, a new 1:1 case–control study was performed for further analysis.
All statistical analyses were performed using SPSS 22.0 and R Project 2.15.3. Two-tailed P values < 0.05 were considered indicative of statistical significance.
Results
Association of apoA-I with early ISR
Among the 205 patients who underwent repeat angiography within 12 months after initial PCI, 18 patients developed ISR (ISR group) while 187 patients did not develop ISR (non-ISR group). There were no significant differences between ISR and non-ISR groups with respect to age and sex distribution, proportion of patients with hypertension, smoking, and history of old myocardial infarction; however, ISR group had a higher proportion of patients with diabetes mellitus (78% vs. 32%, P < 0.05). There were no significant between-group differences with respect to lipid profile (including LDL-C), serum hs-CRP, creatine, eGFR, LVEF, and medication history. Lesion distribution, number, diameter, and length of stents were also comparable in the two groups. In the ISR group, serum level of apoA-I was significantly lower (1.1 ± 0.26 vs. 1.24 ± 0.23, P < 0.05) while HbA1c level was significantly higher (7.65 ± 1.21 vs. 6.81 ± 1.51, P < 0.05) than that in the non-ISR group (Table 1).
On univariate logistic regression analysis, apoA-I, diabetes, and HbA1c level were risk factors for early ISR (Table 2). However, apoA-I level showed no significant correlation with diabetes or HbA1c level by Kendall’s tau-b correlation.
On multivariate logistic regression analysis, apoA-I (OR 0.013, 95% CI 0.000–0.574) and HbA1c (OR 1.429, 95% CI 1.022–1.999) were independent risk factors for early ISR.
On ROC curve analysis, the optimal cut-off value of apoA-I (1.275 g/L) had a 39% sensitivity and 92.3% specificity for diagnosis of early ISR (AUC 0.632); however, the AUC for HbA1c alone or combined model (apoA-I, HbA1c) was comparatively higher (Fig. 2). The combined model was associated with a significant absolute NRI of 11.31% (P < 0.001) and an IDI of 6.86% (z = 1.75, P = 0.04) compared with HbA1c alone, suggesting that combined use of apoA-I and HbA1c can better predict the incidence of early ISR.

Receiver operating characteristic (ROC) analysis using A apoA-I, B HbA1c, C apoA-I and HbA1c combined, to estimate the strength of the model predicting the incidence of early in-stent restenosis
With increasing quartile of apoA-I, the incidence of early ISR decreased by 35.3%, 34.9%, and 81.5%, respectively, compared with the lowest quartile. The downward trend was more obvious after adjusting for various confounding factors in the three clinical models (48.9%, 72.7%, 96.4%). These results indicated a negative correlation between the incidence of early ISR and apoA-I (Table 3, Fig. 3).

Association of each apoA-I quartile with early ISR incidence, adjusted by three models
Association of apoA-I with late ISR
Among the 399 patients who underwent repeat angiography beyond 12 months after initial PCI, 87 patients developed ISR (median stenting time, 44 months) and 312 did not develop ISR (median stenting time, 32 months). There were no significant differences between ISR and non-ISR groups with respect to age, sex, risk factors for coronary artery disease, hs-CRP, creatine, eGFR, coronary lesion distribution, and number/diameter/length of stent (P > 0.05 for all). However, the ISR group had a significantly higher prevalence of old myocardial infarction (OMI) (27% vs. 20%), lower LVEF (56.98 ± 8.67 vs. 59.11 ± 7.42), and lower compliance with statin therapy (71.3% vs. 82.4%). Patients with ISR had higher HbA1c level than those with non-ISR (6.94 ± 1.65% vs. 6.55 ± 1.28%, P = 0.021). There were significant differences in lipid profile between the two groups; ISR patients had significantly higher levels of total cholesterol (TC) (3.82 ± 1.39 vs. 3.38 ± 0.91), triglycerides (TG) (1.83 ± 1.1 vs. 1.51 ± 1.14), LDL-C (2.45 ± 1.35 vs. 2.01 ± 0.81), apoB (0.88 ± 0.39 vs. 0.72 ± 0.24), apoE (40.31 ± 16.77 vs. 35.33 ± 14.84), but lower levels of HDL-C (1.02 ± 0.24 vs. 1.16 ± 0.32) and apoA-I (1.16 ± 0.19 vs. 1.26 ± 0.23). LDL-C showed a correlation with TC, TG, apoB, and apoE levels, but not with HDL-C or apoA-I levels. Therefore, patients were stratified by LDL-C level for further analysis whereby patients with LDL-C ≤ 1.8 mmol/L were assigned to the intensive lipid-lowering subgroup, while the others (LDL-C > 1.8 mmol/L) were assigned to the non-intensive lipid-lowering subgroup.
Intensive lipid-lowering subgroup
In the intensive lipid-lowering subgroup, there were no significantly different features between the ISR and non-ISR patients except for median stenting time (35 vs. 26 months), HDL-C (1.04 ± 0.26 vs. 1.16 ± 0.29), and apoA-I (1.11 ± 0.18 vs. 1.24 ± 0.22) (Table 1).
On univariate logistic regression analysis, apoA-I and stenting time were risk factors of late ISR in the intensive lipid-lowering subgroup (Table 2). There was no significant correlation between apoA-I and stenting time.
On multivariate logistic regression analysis, apoA-I (OR 0.037, 95% CI 0.002–0.695), stenting time (OR 1.017, 95% CI 1.003–1.031), and diabetes (OR 2.853, 95% CI 1.027–7.930) were independent risk factors for late ISR after adjusting for sex, age, hypertension, smoking status, TG, LDL-C, hs-CRP, eGFR, LVEF, and other confounding factors.
ROC curve analysis revealed five clinical models to predict the incidence of late ISR, among which the dual model (apoA-I, stenting time) and triple model (apoA-I, stenting time, diabetes) had comparable higher AUC (0.744 and 0.754) (Fig. 4). Compared with the dual model, the triple model had an additive NRI of − 3.26% (P = 0.752), an absolute NRI of 11.04% (P = 0.367), but a significant IDI of 4% (z = 2.27, P = 0.011). This suggested that use of apoA-I together with stenting time and diabetes can better predict the incidence of late ISR.

Receiver operating characteristic (ROC) curve analysis using A apoA-I, B stenting time, C apoA-I and diabetes combined, D apoA-I and stenting time combined, E apoA-I and stenting time and diabetes combined, to estimate the strength of the model predicting the incidence of late in-stent restenosis
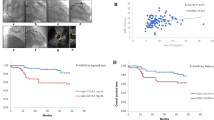
Quartile analysis showed that with increasing quartile of apoA-I, the incidence of late ISR decreased by 8.8%, 68.7%, and 80.3%, respectively, compared with the lowest quartile. When further adjusted for different confounding factors by three clinical models, the downward trend was more obvious (48.2%, 82.1%, 89.9%). These results showed that the incidence of late ISR in intensive lipid-lowering patients was negatively related with apoA-I (Table 4, Fig. 5).

Association of each apoA-I quartile with late ISR incidence in patients with intensive lipid-lowering, adjusted by three models
Non-intensive lipid-lowering subgroup
In patients without intensive lipid-lowering, differences in lipid profile (including TC, LDL-C, HDL-C, apoA-I, apoB), HbA1c, and stenting time remained statistically significant (Table 1). Therefore, propensity score matching (PSM) was performed in a 1:1 ratio, using sex, age, stenting time, TC, LDL-C, HDL-C, HbA1c, hypertension, diabetes, and smoking as matching variables, and 0.1 as the calipers. As a result, a new case group (ISR-PSM, n = 47) and a control group (NISR-PSM, n = 41) were obtained to evaluate the association of apoA-I with late ISR.
After PSM, ISR patients had significantly lower apoA-I (1.19 ± 0.20 vs. 1.42 ± 0.30) and HDL-C (1.03 ± 0.25 vs. 1.31 ± 0.45) level, while there were no significant differences with respect to the other clinical or laboratory features (Table 5).
On multivariate logistic regression analysis of PSM cohort, apoA-I (OR 0.011, 95% CI 0.000–0.946) was an independent risk factor for late ISR, rather than HDL-C.
On ROC curve analysis, the optimal cut-off apoA-I level of 1.235 g/L as the diagnostic criteria was associated with 85.4% sensitivity and 59.6% specificity (AUC 0.756) (Fig. 6).

Receiver operating characteristic (ROC) analysis using apoA-I, to estimate the strength of the model predicting the incidence of late in-stent restenosis after PS matching
Quartile analysis illustrated a significant negative linear correlation between the incidence of late ISR and apoA-I. With increasing quartile of apoA-I, the incidence of late ISR decreased by 14.3%, 65.9% and 89% respectively, compared with the lowest quartile. Moreover, the linear correlation persisted even after adjusting for different confounding factors in the three clinical models (Table 6, Fig. 7).

Association of each apoA-I quartile with late ISR incidence after PS matching, adjusted by three models
Association of apoA-I with all-patients ISR
Finally, all 604 patients enrolled in the study were divided into ISR group (n = 105) and non ISR group (n = 499). There were significant differences between the two groups with respect to baseline clinical characteristics and laboratory parameters. Therefore, propensity score matching (PSM) was again performed in a 1:1 ratio, using sex, age, stenting time, LDL-C, hypertension, diabetes, and smoking as matching variables, and 0.05 as the calipers. As a result, a propensity score-matched case group (ISR-PSM, n = 100) and control group (NISR-PSM, n = 100) were obtained to further evaluate the association of apoA-I with all-patients ISR.
After PSM, ISR patients had significantly longer stenting time (33.5 vs. 12, P = 0.008), while there were no significant differences with respect to the other clinical or laboratory features (Table 7).
On multivariate logistic regression analysis of all-patients PSM cohort, apoA-I (OR 0.024, 95% CI 0.000–0.564), male sex (OR 2.674, 95% CI 1.041–6.870), and stenting time (OR 1.011, 95% CI 1.003–1.019) were independent risk factors for all-patients ISR (Table 8).
Discussion
In this retrospective case–control study, apoA-I was found to be an independent risk factor for ISR in patients undergoing DES-based PCI. This finding is consistent with previous studies that demonstrated anti-restenosis effects of apoA-I. However, most previous studies on the anti-restenosis effects of apoA-I were conducted in cell and animal models. Aart et al. found that anti-apoA-I antibody coating metal stents inhibited ISR compared with bare metal stents in their in vitro experiments and in vivo iliac artery injury model of New Zealand rabbits [22]. In the study by Laura et al., apoA-I coated bare metal scaffolds were found to inhibit in-stent thrombosis, platelet activation, and SMC proliferation in vitro, and to improve the biocompatibility of the stents in a mice model [23]. Ben found that the increase of apoA-I and HDL-C, due to inhibition of cholesterol ester transfer protein (CETP), inhibited the proliferation of SMC and neointimal hyperplasia in New Zealand rabbit iliac artery injury model [15]. In the study by Liu et al., direct intragastric injection of apoA-I mimetic peptide inhibited the proliferation of SMC and neointimal hyperplasia in rat carotid artery injury model [24].
However, there is a paucity of clinical data regarding the association between apoA-I and ISR. Few clinical studies have suggested a significant difference of apoA-I between ISR and non-ISR patients, which is probably due to individual differences or discrepancy of treatment compliance. To the best of our knowledge, the present study is the first to indicate that apoA-I is an independent risk factor for ISR, as we eliminated the influence of most confounding factors by distinguishing early ISR from late ISR, by excluding complicated lesions (CTO, bifurcation lesion, long lesion, grafts lesion), by performing stratification according to lipid-lowering therapy, and by applying propensity score matching.
In this study, the overall incidence of ISR was 17.4% (early ISR 8.8% and late ISR 21.8%), which is consistent with previous reports (3–20%) [25, 26], suggesting that our study is clinically representative even in the era of new-generation DES.
In the early ISR study, we found no significant difference in LDL-C level between ISR and non-ISR patients, suggesting that lipid infiltration may not be the main pathophysiological mechanism of early ISR; this is in line with the current view that the main mechanisms of early ISR involve endothelial deprivation, neointimal hyperplasia, and SMC proliferation [4,5,6,7]. We observed a negative correlation of the incidence of early ISR with serum level of apoA-I, but not HDL-C, suggesting that apoA-I may inhibit neo-intimal hyperplasia or SMC proliferation, thereby inhibiting the occurrence and development of early ISR in an HDL-C independent manner.
In the late ISR study, although intensive lipid-lowering therapy (LDL-C ≤ 1.8 mmol/L) was associated with reduced incidence of ISR, 15.7% of the patients still progressed to late ISR, indicating that further reducing the incidence of late ISR is still clinically relevant. The current European Society of Cardiology (ESC) dyslipidemias management guidelines recommend reduction in LDL-C level to 1.4 mmol/L in high-risk patients with atherosclerotic cardiovascular disease (ASCVD) [27]. However, the mechanism of late ISR mainly involves neo-atherosclerosis, which is not exactly the same as that of natural atherosclerosis; therefore, large-scale clinical studies are required to determine whether further decrease in LDL-C reduces late ISR. In our study, apo A-I affected the incidence of late ISR similar to early ISR, suggesting potential anti-neo-atherosclerosis/anti-restenosis effects of apoA-I. Therefore, based on intensive LDL-C lowering, further increasing the apoA-I level may be a new therapeutic target to inhibit the occurrence and development of late ISR.
In the all-patients ISR study, apoA-I was found to be an independent risk factor for ISR and had a protective effect, which was consistent with the results of early ISR and late ISR study. However, we found that the median stenting time in the ISR group was 33.5 months in contrast to 12 months in the non-ISR group; this indicated that the ISR group contained most patients with late ISR, while most of the patients in the non-ISR group were those who were routinely followed-up. Therefore, although appropriate matching was carried out according to propensity score, different pathogenic mechanisms between early and late ISR may affect the results as a potential confounding factor.
The mechanism of the effect of apoA-I on ISR is likely complex and multifactorial. As the main protein component of HDL-C, apoA-I is mainly involved in the process of reverse transport of cholesterol. It helps remove fat and cholesterol from macrophages in the arterial wall, thereby reducing the transformation of macrophages into foam cells and inhibiting the progression of atherosclerosis [28]. Moreover, apoA-I also ameliorates vascular endothelial function, inhibits smooth muscle proliferation and platelet function, and reduces inflammation and angiogenesis in plaque as well as prevents native and neo-atherosclerosis [13,14,15,16,17,18,19]. Laura et al. investigated the effect of apoA-I on ISR through in vivo experiments in mice [14]. They found that apoA-I improved the biocompatibility of implanted stents. Injection of apoA-I inhibited neointimal hyperplasia after stenting in mice, which was due to the phenotypic transformation of neointima and the promotion of endothelialization [14]. Zhang and Mao, respectively, showed that apoA-I, in conjunction with apoA-I binding protein (AIBP), can enhance cholesterol reverse transport, inhibit inflammation and angiogenesis, and decrease the development of neo-atherosclerosis [29,30,31,32,33].
However, some limitations of our study should be acknowledged: (1) This was a single center, cross-sectional, retrospective case–control study. Owing to the lack of follow-up data, we could not assess the impact of dynamic changes of apoA-I on ISR. (2) Most patients in the early ISR study had undergone regular angiographic follow-up, while most patients in the late ISR study were re-hospitalized due to angina pectoris. As a result, the incidence of late ISR in this study may be higher than that of natural restenosis; therefore, our results may have been affected by an element of selection bias. (3) Although our study excluded patients with early-onset ISR within 6 months mainly due to operative factors (such as stenting with geography-lack or mal-apposition, or excessive elastic rebound caused by over-pressure post-dilation), the confounding bias due to other operative factors cannot be ruled out. (4) With no prior IVUS or OCT processed, the diagnosis of ISR may have been confused with late in-stent thrombosis, leading to some information bias. (5) Not all potential confounding factors were accounted for in the analysis due to the lack of data.
Conclusions
In this study, serum level of apoA-I was an independent risk factor for ISR in patients undergoing DES-based PCI. Our results demonstrate that apoA-I may have an independent protective effect against early and late ISR regardless of HDL-C level. Further multi-center cohort studies and randomized controlled trials are required to provide more definitive evidence of apoA-I as a promising therapeutic target for further reducing the incidence of ISR after DES-based PCI.
Availability of data and materials
The datasets generated and analyzed during the present study are available from the corresponding author on reasonable request.
Abbreviations
- DES:
-
Drug-eluting stents
- ISR:
-
In-stent restenosis
- PCI:
-
Percutaneous coronary intervention
- MACE:
-
Major adverse cardiac events
- IVUS:
-
Intravascular ultrasound
- OCT:
-
Optical coherence tomography
- SMC:
-
Smooth muscle cell
- CTO:
-
Chronic total occlusion
- QCA:
-
Quantitative coronary angiography
- TC:
-
Total cholesterol
- TG:
-
Triglyceride
- LDL-C:
-
Low density lipoprotein cholesterol
- HDL-C:
-
High density lipoprotein cholesterol
- apoA-I:
-
Apolipoprotein A-I
- apoB:
-
Apolipoprotein B
- apoE:
-
Apolipoprotein E
- Lp(a):
-
Lipoprotein(a)
- HbA1c:
-
Glycosylated hemoglobin
- hs-CRP:
-
High-sensitivity C-reactive protein
- eGFR:
-
Estimated glomerular filtration rate
- LVEF:
-
Left ventricular ejection fraction
- ROC:
-
Receiver operating characteristic
- AUC:
-
Area under the curve
- NRI:
-
Net reclassification index
- IDI:
-
Integrated discrimination improvement
- PSM:
-
Propensity score matching
- CETP:
-
Cholesterol ester transfer protein
- ESC:
-
European Society of Cardiology
- ASCVD:
-
Atherosclerotic cardiovascular disease
- AIBP:
-
ApoA-I binding protein
- LAD:
-
Left anterior descending coronary artery
- LCX:
-
Left circumflex coronary artery
- RCA:
-
Right coronary artery
- BVS:
-
Biodegradable vascular scaffold
- SVG:
-
Saphenous vein graft
- ACEI:
-
Angiotensin converting enzyme inhibitor
- ARB:
-
Angiotensin receptor blocker
- MI:
-
Myocardial infarction
References
Taniwaki M, Stefanini GG, Silber S, Richardt G, Vranckx P, Serruys PW, et al. 4-year clinical outcomes and predictors of repeat revascularization in patients treated with new-generation drug-eluting stents: a report from the RESOLUTE All-Comers trial (A randomized comparison of a zotarolimus-eluting stent with an everolimus-eluting stent for percutaneous coronary intervention). J Am Coll Cardiol. 2014;63:1617–25.
Mehran R, Dangas G, Abizaid AS, Mintz GS, Lansky AJ, Satler LF, et al. Angiographic patterns of in-stent restenosis: classification and implications for long-term outcome. Circulation. 1999;100:1872–8.
Cassese S, Byrne RA, Schulz S, Hoppman P, Kreutzer J, Feuchtenberger A, et al. Prognostic role of restenosis in 10 004 patients undergoing routine control angiography after coronary stenting. Eur Heart J. 2015;36:94–9.
Kim MS, Dean LS. In-stent restenosis. Cardiovasc Ther. 2011;29:190–8.
Jinnouchi H, Kuramitsu S, Shinozaki T, Tomoi Y, Hiromasa T, Kobayashi Y, et al. Difference of tissue characteristics between early and late restenosis after second-generation drug-eluting stents implantation—an optical coherence tomography study. Circ J. 2017;81:450–7.
Feng C, Zhang P, Han B, Li X, Liu Y, Niu D, et al. Optical coherence tomographic analysis of drug-eluting in-stent restenosis at different times: a STROBE compliant study. Medicine (Baltimore). 2018;97:e12117.
Goto K, Zhao Z, Matsumura M, Dohi T, Kobayashi N, Kirtane AJ, et al. Mechanisms and patterns of intravascular ultrasound in-stent restenosis among bare metal stents and first- and second-generation drug-eluting stents. Am J Cardiol. 2015;116:1351–7.
Pérez de Prado A, Pérez-Martínez C, Cuellas Ramón C, Regueiro Purriños M, Diego Nieto A, Gonzalo-Orden JM, et al. Safety and efficacy of different paclitaxel-eluting balloons in a porcine model. Rev Esp Cardiol (Engl Ed). 2014;67:456–62.
Pedersen SH, Pfisterer M, Kaiser C, Jensen JS, Alber H, Rickenbacher P, et al. Drug-eluting stents and bare metal stents in patients with NSTE-ACS: 2-year outcome from the randomised BASKET-PROVE trial. EuroIntervention. 2014;10:58–64.
Cassese S, Byrne RA, Tada T, Pinieck S, Joner M, Ibrahim T, et al. Incidence and predictors of restenosis after coronary stenting in 10 004 patients with surveillance angiography. Heart. 2014;100:153–9.
Byrne RA, Cassese S, Windisch T, King LA, Joner M, Tada T, et al. Differential relative efficacy between drug-eluting stents in patients with bare metal and drug-eluting stent restenosis; evidence in support of drug resistance: insights from the ISAR-DESIRE and ISAR-DESIRE 2 trials. EuroIntervention. 2013;9:797–802.
Buccheri D, Piraino D, Andolina G, Cortese B. Understanding and managing in-stent restenosis: a review of clinical data, from pathogenesis to treatment. J Thorac Dis. 2016;8:E1150–62.
van der Vorst EP, Vanags LZ, Dunn LL, Prosser HC, Rye KA, Bursill CA. High-density lipoproteins suppress chemokine expression and proliferation in human vascular smooth muscle cells. FASEB J. 2013;27:1413–25.
Vanags LZ, Tan JTM, Galougahi KK, Schaefer A, Wise SG, Murphy A, et al. Apolipoprotein A-I reduces in-stent restenosis and platelet activation and alters neointimal cellular phenotype. JACC Basic Transl Sci. 2018;3:200–9.
Wu BJ, Li Y, Ong KL, Sun Y, Shrestha S, Hou L, et al. Reduction of in-stent restenosis by cholesteryl ester transfer protein inhibition. Arterioscler Thromb Vasc Biol. 2017;37:2333–41.
Lerch PG, Spycher MO, Doran JE. Reconstituted high density lipoprotein (rHDL) modulates platelet activity in vitro and ex vivo. Thromb Haemost. 1998;80:316–20.
Florentin M, Liberopoulos EN, Wierzbicki AS, Mikhailidis DP. Multiple actions of high-density lipoprotein. Curr Opin Cardiol. 2008;23:370–8.
Tso C, Martinic G, Fan WH, Rogers C, Rye KA, Barter PJ. High-density lipoproteins enhance progenitor-mediated endothelium repair in mice. Arterioscler Thromb Vasc Biol. 2006;26:1144–9.
Barter PJ, Nicholls S, Rye KA, Anantharamaiah GM, Navab M, Fogelman AM. Antiinflammatory properties of HDL. Circ Res. 2004;95:764–72.
Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150:604–12.
Mansoor A, Parth M, Anil KRR, Sudhir M. Percutaneous coronary intervention. 16 Jan 2021.
Strang AC, Knetsch ML, Koole LH, de Winter RJ, van der Wal AC, de Vries CJ, et al. Effect of anti-ApoA-I antibody-coating of stents on neointima formation in a rabbit balloon-injury model. PLoS ONE. 2015;10:e0122836.
Vanags LZ, Tan JTM, Santos M, Michael PS, Ali Z, Bilek MMM, et al. Plasma activated coating immobilizes apolipoprotein A-I to stainless steel surfaces in its bioactive form and enhances biocompatibility. Nanomedicine. 2017;13:2141–50.
Liu D, Wu M, Du Q, Ding Z, Qian M, Tong Z, et al. The apolipoprotein A-I mimetic peptide, D-4F, restrains neointimal formation through heme oxygenase-1 up-regulation. J Cell Mol Med. 2017;21:3810–20.
Kimura T, Morimoto T, Nakagawa Y, Kawai K, Miyazaki S, Muramatsu T, et al. Very late stent thrombosis and late target lesion revascularization after sirolimus-eluting stent implantation: 5-year outcome of the j-Cypher Registry. Circulation. 2012;125:584–91.
Räber L, Wohlwend L, Wigger M, Togni M, Wandel S, Wenaweser P, et al. Five-year clinical and angiographic outcomes of a randomized comparison of sirolimus-eluting and paclitaxel-eluting stents: results of the sirolimus-eluting versus paclitaxel-eluting stents for coronary revascularization LATE trial. Circulation. 2011;123:2819–28, 6 p following 28.
Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, Badimon L, Chapman MJ, De Backer GG, Delgado V, Ference BA, Graham IM. 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Atherosclerosis. 2019;290:140–205.
Yu XH, Fu YC, Zhang DW, Yin K, Tang CK. Foam cells in atherosclerosis. Clin Chim Acta. 2013;424:245–52.
Zhu L, Fang L. AIBP: a novel molecule at the interface of cholesterol transport, angiogenesis, and atherosclerosis. Methodist Debakey Cardiovasc J. 2015;11:160–5.
Zhang M, Li L, Xie W, Wu JF, Yao F, Tan YL, et al. Apolipoprotein A-1 binding protein promotes macrophage cholesterol efflux by facilitating apolipoprotein A-1 binding to ABCA1 and preventing ABCA1 degradation. Atherosclerosis. 2016;248:149–59.
Mao R, Meng S, Gu Q, Araujo-Gutierrez R, Kumar S, Yan Q, et al. AIBP limits angiogenesis through γ-secretase-mediated upregulation of notch signaling. Circ Res. 2017;120:1727–39.
Zhang M, Zhao GJ, Yao F, Xia XD, Gong D, Zhao ZW, et al. AIBP reduces atherosclerosis by promoting reverse cholesterol transport and ameliorating inflammation in apoE(−/−) mice. Atherosclerosis. 2018;273:122–30.
Zhang M, Zhao GJ, Yin K, Xia XD, Gong D, Zhao ZW, et al. Apolipoprotein a-1 binding protein inhibits inflammatory signaling pathways by binding to apolipoprotein a-1 in thp-1 macrophages. Circ J. 2018;82:1396–404.
Acknowledgements
Not applicable.
Funding
This study was funded by Key Disciplines Group Construction Project of Pudong Health Bureau of Shanghai (Grant No. PWZxq2017-05), and the Top-level Clinical Discipline project of Shanghai Pudong (Grant No. PWYgf2018-02). The authors declare that they have no financial relationship with the organization that sponsored the research, and the funding body was not involved in study design, data collection, analysis and writing of the study.
Author information
Authors and Affiliations
Contributions
(I) Conceptualization and design: XW, MZ. (II) Data curation: XW, MZ. (III) Data analysis and software: XW, JC. (IV) Writing—original draft: XW, MZ. (V) Writing—review and editing: all authors. (VI) Final approval of manuscript: all authors. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the ethics committee of Shanghai East Hospital Tongji University {No. 2018-083}. All procedures performed in studies involving human participants were in accordance with the 1964 Helsinki Declaration and its later amendments. All patients signed the written informed consent form.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, X., Zhang, M., Cheng, J. et al. Association of serum apoA-I with in-stent restenosis in coronary heart disease. BMC Cardiovasc Disord 22, 355 (2022). https://doi.org/10.1186/s12872-022-02762-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-022-02762-y