
Abstract
Background
Glycosylated haemoglobin (HbA1c) is considered reliable for diagnosing and monitoring diabetes mellitus (DM). It also indicates cardiovascular complications related to DM. However, only a few studies have been conducted on this topic.
Methods
We conducted a cross-sectional study to investigate the association between newly diagnosed hypertension and HbA1c among non-diabetic Sudanese adults. The sociodemographic characteristics of the participants in the sample were gathered using a questionnaire, and HbA1c was measured using an Ichroma machine.
Results
Three hundred and eighty-four healthy participants were enrolled in this study. The median (interquartile range [IQR]) age was 56.0 (14.0) years, and 72.1% of the participants were female. The median (IQR) body mass index (BMI) was 31.2 (8.7) kg/m2. One hundred and fifteen (29.9%) participants presented newly diagnosed hypertension. The results of the multivariate analysis showed that age (adjusted odd ratio [AOR] = 1.03; 95% confidence interval [CI] = 1.01‒1.05); BMI (AOR = 1.09; 95% CI = 1.05‒1.14); HbA1c levels (AOR = 2.18; 95% CI = 1.29‒3.67) was positively associated with newly diagnosed hypertension. For an HbA1c level of 5.0% or more, the sensitivity and specificity of newly diagnosed hypertension were 91.3% and 28.2%, respectively (area under the curve = 0.61; 95% CI = 0.55–0.67; P ˂ 0.001). Participants who presented HbA1c levels of 5.0% or more were found to be at higher risk for newly diagnosed hypertension (AOR = 2.53; 95% CI = 1.14‒5.61).
Conclusion
The results of this study indicated a high prevalence of newly diagnosed hypertension, and HbA1c levels were positively associated with newly diagnosed hypertension.
Similar content being viewed by others


Introduction
The incidence of non-communicable diseases has increased globally, especially in African countries [1]. Non-communicable diseases are associated with significant morbidity, mortality and financial burdens [1]. Hypertension is a serious medical condition that is significantly associated with risks of heart, brain, kidney and other diseases [1]. Over one billion adults aged 30–79 years worldwide are expected to have hypertension, and low- and middle-income countries constitute a majority of this population [1]. The prevalence of hypertension was found to be 46% in adult Africans aged 25 and above, as compared to 35% in Europe and North America [1]. Several factors have been reported to be associated with hypertension, such as age [2], gender [3], obesity [4], smoking and alcohol consumption [5].
In 2019, the global prevalence of diabetes mellitus (DM) was estimated to be 9.3% (463 million people) and was expected to rise to 10.2% (578 million) and 10.9% (700 million) by 2030 and 2045, respectively [6]. Glycosylated haemoglobin (HbA1c) represents one of the most important diagnostic tools for the diagnosis of DM, and it is an indicator used to determine glycaemic control in most DM patients [7]. High baseline HbA1c levels have been predominantly associated with an increased incidence of hypertension independently of obesity and DM [8].
The current evidence of an association between HbA1c levels and hypertension is not conclusive. Although some previous studies have shown that HbA1c levels are associated with hypertension [3, 8,9,10,11,12], others have failed to identify a relationship between the two [13,14,15,16]. Moreover, HbA1c has prognostic importance because it is used to predict cardiovascular complications related to metabolic syndrome [8]. However, most previous studies on this topic have been conducted in high-income countries, and no data have been published on the association between HbA1c and hypertension in African populations. Therefore, it is vital to conduct such studies in Africa to yield the data necessary for carrying out evidence-based interventions. Among African countries, Sudan has been shown to have an estimated 30% prevalence of hypertension [17]. In 2019, the Diabetes Atlas, compiled by the International Diabetes Federation, included Sudan among countries that had a DM prevalence of more than 12% [6, 18]. We performed this study to assess the associations between HbA1c and newly diagnosed hypertension in eastern Sudan.
Methods
Study design and ethical approval
Study area
Gadarif, which is one of the 18 states of Sudan, has an area of 75,263 km2. Based on the 2008 census, the total population of this state is 1,336,662, and the annual population growth rate is 4.7% [19]. Collecting and trading forest products and charcoal burning are the traditional economic activities of the region, in addition to agriculture, grazing and forest utilisation. The livestock production carried out in the state serves to enhance the traditional pastoral and agropastoral systems [20].
A cross-sectional community-based study was conducted from January to May 2019, for which a multistage sampling approach was employed. We adopted simple random sampling to select four of the 11 localities (the smallest administrative units in Sudan) in Gadarif. In total, the sample comprised 384 participants, who were recruited from the four localities according to their size.
Inclusion criteria
Sudanese residents who were over 18 years of age and living in a household were chosen using the lottery method. The participants were apparently healthy subjects who were not known to have or be treated for DM or hypertension. If a selected house was not inhabited, if there was no suitable participant in the household or if the inhabitants refused to participate, we moved on to the next house.
Exclusion criteria
The exclusion criteria were as follows: individuals below the age of 18, pregnant women, those with DM, hypertension, hemoglobinopathy, acute illnesses or psychosis, debilitated patients, those who refused to participate in the study, temporary residents and those suffering from any chronic disease that could affect HbA1c levels measurement (e.g., thyroid problems, asthma, epilepsy, severe anaemia or end-stage renal disease). Individuals who were on medications that affect blood sugar or blood pressure were also excluded (Fig. 1).

Shows the inclusion and exclusion criteria of the participants in eastern Sudan
All eligible participants were invited to participate in the study, and two well-trained medical officers were assigned to interview those who agreed to do so. The study was explained to the participants, all of whom signed an informed consent form. The World Health Organisation’s three-level stepwise-approach questionnaire was adopted for data collection [21]. The questionnaire was employed to collect the following data: demographic and behavioural information and physical measurements, including anthropometric measurements, blood pressure and biochemical test results for non-communicable disease surveillance.
The questionnaire was used to collect the following sociodemographic characteristics: age, sex, marital status (married, divorced or unmarried), employment status (employed or unemployed), education level (less than secondary level or equal to or higher than secondary level), smoking habits (those who had smoked more than 100 cigarettes in their lives and reported having smoked in the past year were considered smokers) and alcohol consumption (one or more drinks in the previous month).
The weight and height of the participants were measured using standard procedures. Next, their body mass index (BMI) was obtained using the following equation: weight (kg)/height (m2). Their blood pressure was measured using a standard mercury sphygmomanometer after the patients had rested for at least 10 min in a seated position. The procedure was fully explained to each participant before their arm was maintained at the level of the heart using an appropriately sized cuff. The mean of two (at an interval of 1–2 min) blood pressure readings was recorded. If there was a difference of more than 5 mmHg between the two readings, the measurements were taken again until a stable reading was achieved.
Blood glucose measurement
A total of 3 ml of venous blood was drawn from each participant after providing a thorough explanation of the associated procedure and technique. The blood samples were collected under aseptic conditions in a vacuum blood collection tube containing ethylene diamine tetraacetic acid (EDTA). Random blood glucose levels were immediately tested for the samples using a glucometer (Accu-Check Active, Roche Diagnostics, Germany). The samples were transported to a modern diagnostic laboratory where HbA1c levels were measured using an Ichroma machine (Republic of Korea).
Diagnosis of DM
DM was defined as recommended by the American Diabetes Association and the International Diabetes Federation for non-pregnant adults (HbA1c levels of 6.5% or higher) [18, 22]. We selected the HbA1c test for this study because it is convenient to administer and evaluate. Moreover, it reflects the average blood glucose levels during the previous two to three months and directly correlates to blood glucose levels. The HbA1c test is practical, and, as it is not affected by recent food intake, a fasting period is not required. Further, it can be administered at any time of the day.
Diagnosis of hypertension
The participants were considered hypertensive if their systolic blood pressure was 140 mmHg or more, their diastolic blood pressure was 90 mmHg or more or both these criteria were met in both repeated measurements [23].
Sample size calculation
A single population proportion Kish Leslie formula (n = z2 p (1—p)/d2) was used to calculate the sample size. We assumed that the maximum proportion (50%) of newly discovered hypertension had the maximum sample size estimation. Thus, our sample of 384 participants presented a 95% confidence level, and we expected that 10% of them might not respond or might have incomplete data.
Statistical analysis
The data were analysed using SPSS for Windows (version 22.0). Continuous data (including HbA1c) were checked for normality using the Shapiro–Wilk test, and it was found that all data were not distributed normally. The data were expressed as a numerical proportion or as a median (interquartile range [IQR]) where applicable. A univariate analysis was performed, in which newly diagnosed hypertension was the dependent variable. The independent variables were age, gender, employment, education, BMI and HbA1c. Multicollinearity (variance inflation factor pf less than four) was checked but not detected. A logistic regression analysis was applied to the variables if their univariate p was less than 0.20, and a backward-stepwise likelihood ratio regression was used for adjustment. Next, the odds ratios (OR) and 95% confidence intervals (CI) were calculated. A p value of less than 0.05 was considered significant. Reliability tests (sensitivity and specificity) and cut-off values for HbA1c were conducted using the receiver operating characteristic (ROC) curve and the area under the curve (AUC).
Results
Initially, 715 participants were screened, of which 331 were excluded for certain reasons such as DM, pregnancy and medical diseases (Fig. 1). Thus, 384 healthy non-diabetic participants were enrolled in the study. The median (IQR) age was 56.0 (14.0) years, and 329 (72.1%) participants were female. Of these, 237 (61.7%) were married, 239 (62.2%) had above secondary level education and 124 (32.3%) were employed. Only 7 (1.8%) participants were smokers, and none of them were alcoholics. The median (IQR) BMI was 31.2 (8.7) kg/m2 (Table 1). Finally, 115 (29.9%) participants were found to have newly diagnosed hypertension. The HbA1c levels were significantly higher among patients with newly diagnosed hypertension compared to those who were non-hypertensive (Fig. 2).

Box plot of HbA1c levels among hypertensive and non-hypertensive non-diabetic subjects
The univariate analysis included patients with newly diagnosed hypertension who were significantly older, had high levels of HbA1c, were married, had above secondary education and were obese (Table 2).
The results of the multivariate regression analysis were as follows: age (AOR = 1.03; 95% CI = 1.01‒1.05), BMI (AOR = 1.09; 95% CI = 1.05‒1.14) and HbA1c levels (AOR = 2.18; 95% CI = 1.29‒3.67) were found to be positively associated with newly diagnosed hypertension. There was no significant association between marital status, level of education and newly diagnosed hypertension (Table 3).
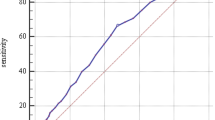
For HbA1c levels of 5.0% and above, the sensitivity and specificity of the diagnosis of newly diagnosed hypertension were 91.3% and 28.2%, respectively (AUC = 0.61; 95% CI = 0.55–0.67; P ˂ 0.001) (Fig. 3). Thus, participants with HbA1c levels of 5.0% or more were at higher risk for newly diagnosed hypertension (AOR = 2.53; 95% CI = 1.14‒5.61; P = 0.022).

ROC curve analysis of HbA1c and hypertension risk in non-diabetic subjects
Discussion
The main finding of our study was the association between HbA1c levels and newly diagnosed hypertension. In this study, each percentage increase in HbA1c was observed to increase the risk for newly diagnosed hypertension by 2.18 times (AOR = 2.18). Using a cut-off point for HbA1c levels of 5.0% or more, the sensitivity and specificity of the diagnosis of hypertension were calculated as 91.3% and 28.2%, respectively. These results are in line with those of a prospective cohort study that includes 9,603 middle-aged American participants, where elevated HbA1c levels (even without a prior diagnosis of DM) were associated with hypertension among diabetic as well as non-diabetic individuals [8]. In a previous study with 19,858 non-diabetic American women, the highest HbA1c quintile was associated with hypertension among the participants [10]. Further, the results of the Framingham Heart Study also revealed that high HbA1c levels were associated with hypertension [9]. A recent study on 376,644 cases in the United Kingdom found that HbA1c was a significant predictor of hypertension risk [11]. Two studies conducted in China showed that higher HbA1c levels significantly increased the risk of hypertension and isolated systolic hypertension among non-diabetic patients without significantly affecting diastolic blood pressure [3, 12]. Additionally, a significant association was observed between HbA1c and hypertension among patients with T2DM in Brazil [24, 25], Korea [26] and Belgium [27].
In contrast to our findings, a recently published study demonstrated that HbA1c in diabetic patients was not correlated with arterial stiffness; however, the concomitant hypertension was a significant potential risk for arterial stiffness [13]. Furthermore, certain studies demonstrated a non-significant association between HbA1c and the risk of developing hypertension in non-diabetic populations in Israel [14], Japan [15] and Germany [16]. Another study reported a non-significant association between HbA1c and the increased risk of developing hypertension among women without diabetes after adjusting for BMI [10]. Interestingly, a non-significant correlation was found between the HbA1c levels of patients with T2DM and the risk of them developing either systolic or diastolic blood pressure in Iran [28, 29] and Brazil [30]. Surprisingly, two previous studies reported an inverse relationship between HbA1c levels and high blood pressure in patients with T2DM [31, 32].
Insulin resistance is the main pathophysiological factor behind the increased risk of developing both T2DM and hypertension [33]. In addition, the coincidence of glycaemic control and hypertension can be explained by dysfunctional pancreatic β cells and adiposity along with insulin resistance [8, 34]. HbA1c is one of the best indices for assessing insulin resistance in not only diabetic patients but also obese non-diabetic individuals [35]. Insulin resistance was shown to be dramatically upregulated across the quartile levels of HbA1c in those without diabetes [36]. High levels of HbA1c have been linked to proinflammatory cell signalling and oxidative stress, which may induce arterial stiffness [37]. Similarly, higher HbA1c values were shown to predict the development of hypertension as a result of high glucose flux across endothelial cell membranes [38]. Furthermore, the formation and accumulation of advanced glycation end products was observed to stem from excess circulating glucose that binds proteins, lipids and nucleic acids [39]. The accumulation of advanced glycation end products in the vessel wall was indicated to be the main contributor for the inflammation process, oxidative stress and endothelial dysfunction, subsequently altering blood pressure [39], increasing systemic vascular resistance and causing arterial stiffness [30]. In addition, the glycosylation of haemoglobin was demonstrated to impair oxygen carrying capacity, hence promoting hypoxia and the associated systemic vascular vasodilatory adaptations and inflammatory responses [40]. Similarly, increased levels of HbA1c were observed to facilitate endothelial damage, which led to the further release of endothelin from the endothelial cells and hindered the production of prostacyclin and nitric oxide, resulting in vasomotor dysfunction and further elevation in blood pressure [41]. In the current study, greater age was statistically significantly associated with the risk of developing hypertension. This result is consistent with that of a previous study conducted in Sudan, which revealed a significant association between increasing age and the prevalence of hypertension [2]. Similarly, a recent meta-analysis that included 43,025 older African adults (above the age of 53) demonstrated that older age was independently associated with hypertension [42]. Our results indicated that the BMI is a significant predictor of the development of hypertension. Several previous studies have illustrated significant associations between obesity and hypertension in Africa [5, 42,43,44,45]. The results of the current study and a recently published paper in Sudan showed no significant association between an individual’s gender and the presence of hypertension [2]. However, some previous studies reported that gender was a significant predictor of hypertension [3, 46]. Interestingly, in the present study, only 1.8% of the participants were smokers, and no participants reported alcohol consumption. It is possible that the rates of smoking and alcohol consumption were underestimated, as many individuals may not have been willing to admit these social habits given that they are stigmatised, particularly among females.
Conclusion
HbA1C is a significant predictor of newly diagnosed hypertension among healthy adult non-diabetic Sudanese. Hence, it can be used to modify or prevent hypertension among those who have considerably high HbA1c levels.
Limitations of the study
Our study has the following limitations. The causes and the effects of the results could not be inferred, as this was a cross-sectional study. Only a single measurement of HbA1c at baseline was available, which may have resulted in misclassification. Other causes of secondary hypertension cannot be excluded. Moreover, other factors, such as dyslipidemia, were not assessed. Also the high number of females participant which may be due to the availability of females at home during the data collection.
Availability of data and materials
The datasets used and/or analysed during the current study are available in the [OSF] repository, [https://osf.io/jcx6b/?view_only=3ffb18e18d804929ab2008377924d572].
References
Poulter NR, Prabhakaran D, Caulfield M. Hypertension. In: The Lancet. Lancet Publishing Group, 2015, pp. 801–812.
Omar SM, Musa IR, Osman OE, et al. Prevalence and associated factors of hypertension among adults in Gadarif in eastern Sudan: a community-based study. BMC Public Health. 2020;20(1):291.
Song J, Wei N, Zhao Y, et al. Elevated glycosylated hemoglobin levels and their interactive effects on hypertension risk in nondiabetic Chinese population: a cross-sectional survey. BMC Cardiovasc Disord. 2020;20(1):218.
Omar SM, Taha Z, Hassan AA, et al. Prevalence and factors associated with overweight and central obesity among adults in the Eastern Sudan. PLOS ONE. 2020;15(4):e0232624.
Abebe SM, Berhane Y, Worku A, et al. Prevalence and associated factors of hypertension: a crossectional community based study in Northwest Ethiopia. PLoS ONE. 2015;10:e0125210.
Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9 th edition. Diabetes Res Clin Pract. 2019;157:107843.
Yazdanpanah S, Rabiee M, Tahriri M, et al. Evaluation of glycated albumin (GA) and GA/HbA1c ratio for diagnosis of diabetes and glycemic control: a comprehensive review. Crit Rev Clin Lab Sci. 2017;54:219–32.
Bower JK, Appel LJ, Matsushita K, et al. Glycated hemoglobin and risk of hypertension in the atherosclerosis risk in communities study. Diabetes Care. 2012;35:1031–7.
Singer DE, Nathan DM, Anderson KM, et al. Association of HbA1c with prevalent cardiovascular disease in the original cohort of the Framingham heart study. Diabetes. 1992;41:202–8.
Britton KA, Pradhan AD, Gaziano JM, et al. Hemoglobin A1c, body mass index, and the risk of hypertension in women. Am J Hypertens. 2011;24:328–34.
Au Yeung SL, Luo S, Schooling CM. The impact of glycated hemoglobin on risk of hypertension: a Mendelian randomization study using UK Biobank. J Hypertens. 2020;38:38–44.
Hidru TH, Yang X, Xia Y, et al. The relationship between plasma markers and essential hypertension in middle-aged and elderly Chinese population: a community based cross-sectional Study. Sci Rep. 2019;9(1):6813.
Nuamchit T, Siriwittayawan D, Thitiwuthikiat P. The relationship between glycemic control and concomitant hypertension on arterial stiffness in Type II Diabetes. Vasc Health Risk Manag. 2020;16:343.
Geva M, Shlomai G, Berkovich A, et al. The association between fasting plasma glucose and glycated hemoglobin in the prediabetes range and future development of hypertension. Cardiovasc Diabetol. 2019;18:1–9.
Heianza Y, Arase Y, Kodama S, et al. Fasting glucose and HbA1c levels as risk factors for the development of hypertension in Japanese individuals: Toranomon hospital health management center study 16 (TOPICS 16). J Hum Hypertens. 2015;29:254–9.
Kroke A, Liese AD, Keil U, et al. Arterial hypertension and glycemia in non-diabetic subjects: Is there an association independent of obesity. Diabetes Metab Res Rev. 1999;15:99–105.
Ataklte F, Erqou S, Kaptoge S, et al. Burden of undiagnosed hypertension in sub-saharan africa: A systematic review and meta-analysis. Hypertension. 2015;65:291–8.
IDF Diabetes Atlas 9th edition 2019, https://www.diabetesatlas.org/en/ (Accessed 19 May 2021).
Sudan—5th Sudan Population and Housing Census 2008—IPUMS Subset.
Bushara MOA, Ibrahim HH. Food security status for the household: a case study of Al-Qadarif State, SUDAN (2016). J Soc. 2017;6:2167. https://doi.org/10.4172/2167-0358.1000217.
Riley L, Guthold R, Cowan M, et al. The world health organization STEPwise approach to noncommunicable disease risk-factor surveillance: Methods, challenges, and opportunities. Am J Public Health. 2016;106:74–8.
American Diabetes Association Glycemic targets: standards of medical care in Diabetesd 2018. Diabetes Care 2018; 41: S55–S64.
Weber MA, Schiffrin EL, White WB, et al. Clinical practice guidelines for the management of hypertension in the community: a statement by the American Society of Hypertension and the International Society of Hypertension. J Clin Hypertens (Greenwich). 2014;16:14–26.
de Farias CB, Coelli S, Satler F, et al. Glycated hemoglobin and blood pressure levels in adults with Type 2 diabetes: How many patients are on target? Can J Diabetes. 2021;45:334–40.
Malerbi DA, Franco LJ. Multicenter study of the prevalence of diabetes mellitus and impaired glucose tolerance in the urban Brazilian population aged 30–69 yr. Diabetes Care. 1992;15:1509–16.
Jung JY, Oh CM, Ryoo JH, et al. The influence of prehypertension, hypertension, and glycated hemoglobin on the development of type 2 diabetes mellitus in prediabetes: the Korean Genome and Epidemiology Study (KoGES). Endocrine. 2018;59:593–601.
Camara S, Bouenizabila E, Hermans MP, et al. Novel determinants preventing achievement of major cardiovascular targets in type 2 diabetes. Diabetes Metab Syndr Clin Res Rev. 2014;8:145–51.
Habibi Khorasani S, Masoumi M, Nakhaei M, et al. Relationship Between the hypertension stage and hemoglobin A1c in patients with type 2 diabetes. Iran Hear J. 2019;20:75–83.
Janghorbani M, Amini M. Hypertension in type 2 diabetes mellitus in Isfahan, Iran: Incidence and risk factors. Diabetes Res Clin Pract. 2005;70:71–80.
Moreno B, De Faria AP, Ritter AMV, et al. Glycated hemoglobin correlates with arterial stiffness and endothelial dysfunction in patients with resistant hypertension and uncontrolled diabetes mellitus. J Clin Hypertens. 2018;20:910–7.
Cabrales P, Salazar Vázquez MA, Salazar Vázquez BY, et al. Blood pressure reduction due to hemoglobin glycosylation in type 2 diabetic patients. Vasc Health Risk Manag. 2008;4:917–22.
Bilgin R, Donma O, Sagliker Y. Glucose, glycated hemoglolin and fructosamine levels in essential hypertension. Biochem Mol Biol Int. 1993;31:1129–33.
Wang F, Han L, Hu D. Fasting insulin, insulin resistance and risk of hypertension in the general population: a meta-analysis. Clin Chim Acta. 2017;464:57–63.
Chehregosha H, Khamseh ME, Malek M, et al. A View Beyond HbA1c: Role of continuous glucose monitoring. Diabetes Therapy. 2019;10:853–63.
Boursier G, Sultan A, Molinari N, et al. Triglycerides and glycated hemoglobin for screening insulin resistance in obese patients. Clin Biochem. 2018;53:8–12.
Jung CH, Rhee EJ, Kim KJ, et al. Relationship of glycated hemoglobin A1c, coronary artery calcification and insulin resistance in males without diabetes. Arch Med Res. 2015;46:71–7.
Saisho Y. Glycemic variability and oxidative stress: a link between diabetes and cardiovascular disease? Int J Mol Sci. 2014;15:18381–406.
Cosentino F, Lüscher TF. Effects of blood pressure and glucose on endothelial function. Curr Hypertens Reports. 2001;3:79–88.
Goh SY, Cooper ME. The role of advanced glycation end products in progression and complications of diabetes. J Clin Endocrinol Metab. 2008;93:1143–52.
Paffett ML, Walker BR. Vascular adaptations to hypoxia: Molecular and cellular mechanisms regulating vascular tone. Essays Biochem. 2007;43:105–19.
Prasad K. Does HbA1cc play a role in the development of cardiovascular diseases? Curr Pharm Des. 2018;24:2876–82.
Bosu WK, Reilly ST, Aheto JMK, et al. Hypertension in older adults in Africa: a systematic review and meta-analysis. PLoS ONE. 2019;14:e0214934.
Chin JH, Twinobuhungiro A, Sandhu A, et al. Determinants of raised blood pressure in Urban Uganda: a community-based case-control study. Ethn Dis. 2017;27:15–20.
Kassa A, Woldesemayat EM. Hypertension and diabetes mellitus among patients at Hawassa University Comprehensive Specialized Hospital, Hawassa, Southern Ethiopia. Int J Chronic Dis. 2019;2019:1–8.
Manus MB, Bloomfield GS, Leonard AS, et al. High prevalence of hypertension in an agricultural village in Madagascar. PLOS One. 2018;13(8):e0201616.
Bushara S, Noor S, Ibraheem AA, et al. Prevalence of and risk factors for hypertension among urban communities of North Sudan: detecting a silent killer. J Fam Med Prim Care. 2017;5:605.
Acknowledgements
The authors would like to thank the participants for their contribution
Funding
No funding was received.
Author information
Authors and Affiliations
Contributions
SMO, IRM and IA conceived and designed the study. SMO and OA recruited the participants. ME, OA and IA analysed the data and wrote the manuscript. All contributing authors of this original manuscript authorised the final version of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the ethical committee of the Faculty of Medicine, Gadarif University, Sudan (2019, # 07). Written informed consent was obtained from all participants prior to their participation in the study. All methods were applied in accordance with the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Omar, S.M., Musa, I.R., Abdelbagi, O. et al. The association between glycosylated haemoglobin and newly diagnosed hypertension in a non-diabetic Sudanese population: a cross-sectional study. BMC Cardiovasc Disord 22, 208 (2022). https://doi.org/10.1186/s12872-022-02649-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-022-02649-y