
Abstract
Background
QT interval as an indicator of ventricular repolarization is a clinically important parameter on an electrocardiogram (ECG). QT prolongation predisposes individuals to different ventricular arrhythmias and sudden cardiac death. The current study aimed to identify the best heart rate corrected QT interval for a non-hospitalized Iranian population based on cardiovascular mortality.
Methods
Using Fasa PERSIAN cohort study data, this study enrolled 7071 subjects aged 35–70 years. Corrected QT intervals (QTc) were calculated by the QT interval measured by Cardiax® software from ECGs and 6 different correction formulas (Bazett, Fridericia, Dmitrienko, Framingham, Hodges, and Rautaharju). Mortality status was checked using an annual telephone-based follow-up and a minimum 3-year follow-up for each participant. Bland–Altman, QTc/RR regression, sensitivity analysis, and Cox regression were performed in IBM SPSS Statistics v23 to find the best QT. Also, for calculating the upper and lower limits of normal of different QT correction formulas, 3952 healthy subjects were selected.
Results
In this study, 56.4% of participants were female, and the mean age was 48.60 ± 9.35 years. Age, heart rate in females, and QT interval in males were significantly higher. The smallest slopes of QTc/RR analysis were related to Fridericia in males and Rautaharju followed by Fridericia in females. Thus, Fridericia’s formula was identified as the best mathematical formula and Bazett’s as the worst in males. In the sensitivity analysis, however, Bazett’s formula had the highest sensitivity (23.07%) among all others in cardiac mortality. Also, in the Cox regression analysis, Bazett’s formula was better than Fridericia’s and was identified as the best significant cardiac mortality predictor (Hazard ratio: 4.31, 95% CI 1.73–10.74, p value = 0.002).
Conclusion
Fridericia was the best correction formula based on mathematical methods. Bazett’s formula despite its poorest performance in mathematical methods, was the best one for cardiac mortality prediction. Practically, it is suggested that physicians use QTcB for a better evaluation of cardiac mortality risk. However, in population-based studies, QTcFri might be the one to be used by researchers.
Similar content being viewed by others

Background
The QT interval on an electrocardiogram (ECG) indicates ventricular repolarization which is measured from the beginning of the QRS wave to the end of the T wave [1]. It is an important parameter on ECG due to its prolongation.
Prolongation of QT has two main categories of etiology. The first is a congenital or familial form of QT prolongation, known as long QT syndrome (LQTS). There are at least 14 genes responsible for LQTS [2], and the prevalence of LQTS is reported as approximately one in 2500 people [3] which makes this etiology an important one. The second is an acquired form of QT prolongation. The role of several factors such as smoking [4], elevated lipid profiles [5], a history of prior cardiovascular diseases [6], chronic diseases such as diabetes, renal failure, and thyroid disturbances [7], metabolic syndrome [8], body fat mass [9], liver failure [10], electrolyte imbalances like potassium [11] and calcium [7], as well as that of some medications, including antimicrobial, psychoactive, and cardiovascular drugs, have been shown and suggested in QT prolongation [12]. Besides, the effects of age [13] and the female gender [14] on the QT interval should not be ignored.
QT prolongation can cause clinical symptoms such as vertigo and syncope [15] and may lead to cardiovascular events such as stroke and ventricular arrhythmias, including ventricular fibrillation (VF), Torsade de Pointes (TdP) [16, 17], and ultimately, sudden cardiac death (SCD) [18]. Recently, Simpson et al. showed the association between drug-induced QT prolongation and SCD [19], showing an increased risk of non-arrhythmic causes of death. Prolongation of the QT interval has been studied extensively in patients with cardiac diseases, and its association with increased risk of all-cause mortality has been reported [20].
The relation between QT and RR intervals has been reported to be highly individual [21, 22]. Also, it has shown that heterogeneity of myocardial repolarization will not change with increasing age [23]. It is not clear why the QT/RR relationship should reflect interindividual variability physiologically, but it is contingent on the complex interplay of the individual ionic channels which hold the potential for ventricular myocyte action [24, 25]. Moreover, the genes responsible for these channels may vary among individuals [26, 27]. In this case, the ionic complexity of the repolarization process could perhaps lead to major differences, even between healthy normal hearts [21, 28]. There are various formulas for the calculation of the corrected QT interval to adjust the heart rate effect and cause the relationship between RR and QT interval to subside [29]. Formulas known for QT interval correction are presented in Table 1. The most popular correction formula was proposed by Bazett (QTcB) [30]. According to the study by Shen Luo et al. [31], Bazett’s formula has only become popular because physicians recommend it to their students who lack knowledge of the benefits of other formulas and use it merely as instructed. They have also suggested that Hodges’ formula is the best correction formula in the field. Lately, Dash et al. [32] reported that Fridericia’s formula may be a better choice than Bazett’s for the calculation of QTc in subjects with AF.
The current study aimed to identify the best heart rate corrected QT interval for a non-hospitalized Iranian population to determine which QT correction formula would be the best based on cardiovascular-cause mortality among Fasa PERSIAN cohort study subjects.
Method
Population
Data from the Fasa Cohort Study as a branch of the PERSIAN cohort which was started on 2015–2016 was used [33]. All participants came from a rural region in Fasa and within the age range of 35–70 years old. Before entering the Fasa Cohort Study, each participant signed an informed consent letter. A telephone-based follow-up was performed each year for all of the participants without any missing data. In the case of an event, their relatives were interviewed about it. Patients' medical data were checked and analyzed in cases of hospitalization or death. Each participant with a recorded electrocardiogram (ECG) entered the study (n = 7239). Subjects with incomplete ECG data and those with a non-sinus rhythm ECG or QRS duration of more than 120 ms were excluded (n = 168). Ultimately, 7071 subjects remained in the study.
Demographics and medical history
Demographic data regarding age and gender were recorded in a questionnaire. Patients’ histories of cardiovascular diseases (CVD) such as stroke, coronary heart disease (CHD), or myocardial infarction (MI) as well as medical conditions such as diabetes, hypertension, renal failure, chronic lung disease, hepatitis, and thyroid dysfunction were questioned and evaluated by the protocol mentioned in reference 32 [33]. Patients were asked to bring any medication taken within 2 weeks of the study for registration at the interview time for maximum precision and to be recorded in electrical form. Mortality status was checked using a telephone-based follow-up each year, and the date of a subject’s mortality was recorded electronically. National and regional death registry systems were searched for confirmation and the reason for death.
Electrocardiogram
Each participant had a 12-lead ECG with a 2000 Hz sampling rate and 0.04 µV/bit (24-bit resolution). ECGs were recorded using a device (Cardiax® [34]) on shaved precordium and with patients in the supine and postprandial state for the best possible results. Patients were in the supine position 15 min before recording and were told to relax, breathe normally, refrain from moving and talking, but remain awake during the procedure. Heart rates, QRS duration, and QT intervals of all ECGs were analyzed and reported automatically by the Cardiax software (version 3.50.2, International Medical Equipment Developing Co. Ltd., Budapest, Hungary) and exported to the central data software. The mean of QT intervals on lead II on every beat during 10 s was reported as the QT interval of each subject. For the correction of QT intervals, the 6 most popular correction formulas were used (Table 1).
Normal healthy subjects for optimum QT correction formula
To find the best QT correction formula, first, the healthy subjects in the study were selected for the best results. Individuals with the following criteria were selected: (1) having no CVD history; (2) having no significant medical condition, such as diabetes, hypertension, renal failure, chronic lung disease, hepatitis, or thyroid dysfunction; (3) no medication consumption that would influence the cardiovascular system and the QT interval; (4) having an RR interval of 0.5–1.5 s.
The American organization CredibleMeds provides lists of drugs that are associated with QTc-prolongation which are continuously updated with new information and revised by their review team. This study used a list of drugs with known and possible risks for TdP, which accounted for 187 cardiac and non-cardiac drugs in total [35].
Finally, 3952 subjects were identified as meeting the above criteria, and their data were used in analyses to find the optimum QT correction formula. Their data was also used in calculating the upper and lower limits of normal (ULN and LLN) for each QT correction formula based on the 95% and 5% percentile of these subjects, respectively.
Statistical analysis
Data were presented as mean ± standard deviation (SD) and count (percentage) and were compared between males and females by independent sample t and chi-square tests. The paired t test was used to compare mean differences of QTc intervals, and their intercorrelation was evaluated by the Pearson correlation coefficient. To indicate the differences between QTc intervals, a Bland–Altman plot was used [36]. Four different methods were used to find the optimum QT correction formula. The QTc1 was a linear regression model between QT and RR adjusted by gender based on the Framingham formula (QT = α + β * RR – β2 * male) [37]. The QTc2 was another linear regression model between QT and heart rate based on the Hodges formula (QT = α + β * HR) [38]. The QTc3 was a logarithmic transformation of both QT and RR based on Spence et al. [39] after gender distinction. The slope (β) of the linear regression between QT interval and RR after logarithmic transformation was obtained (LogQT = α + β * LogRR), and then the optimized formula was defined as (QTc3 = QT/RRβ). The fourth method was based on Wernicke et al. [40]. The value of “d” was found to range from 0.301 to 0.499 by 0.001 in QTc4 = QT/RRd as the lowest correlation between QTc4 and RR. A simple linear regression separated by gender between the RR and QTc intervals was performed to find the best correction formula for the study population. The calculations for ULN and LLN and their 95% confidence interval have been described above. To validate the ULN cut points which were extracted from normal healthy population QTc intervals, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated for the prediction of all-cause and cardiac mortality rates. Cox regression analysis was performed to calculate the hazard ratio (HR) and 95% confidence interval of mortality. In this analysis, survival days to death as time, death as an event, and QTc interval > ULN as an independent factor were defined. Cox regression analysis was performed in both unadjusted and multivariable-adjusted models.
Results
Demographics
From 7071 subjects, 56.4% were female, and the mean age was 48.60 ± 9.35 years. Age and heart rate in females and QRS duration and QT interval in males were significantly higher (p < 0.001). After the correction of the QT interval, all QTc interval means were higher in females (p < 0.001). Cardiac deaths and all-cause mortality were more frequent in male subjects. The baseline characteristics of subjects are reported in Table 2 according to gender. Other descriptive data on ECG parameters are reported in Additional file 1: Table S1.
Mean difference and correlation of different QTc intervals
The highest correlation was detected between Framingham and Fridericia QTc intervals (r = 0.995, p value < 0.001), and the smallest correlation was related to Bazett-Fridericia and Hodges-Rautahatju QTc intervals (r = 0.935, p value < 0.001) in male subjects. In females, interestingly the highest correlation was r = 0.992 in Rautahatju and Dmitrienko QTc intervals with p value < 0.001, and the smallest correlation, which was the same as in male subjects, was found in the Bazett and Fridericia QTc intervals (r = 0.918, p value < 0.001). All mean differences and correlations between different QTc formulas in both genders have been reported in Additional file 1: Table S2. For a better comparison of different QTc intervals, the Bland–Altman analysis was performed (Additional file 1: Table S3). The Bland–Altman graphs in males and the Bland–Altman graphs for females is provided in Additional file 1: Figure S1.
The optimum QT correction formula
To determine the best QT correction formula for our study population, four statistical methods from previously published papers were evaluated. The similar statistical method from 4 common QT correction formulas performed and their results are reported in Table 3. First, a method similar to the Framingham formula was used, a linear regression model between QT interval and RR. The results showed QT = 0.267 + 0.155 * RR − 0.009 * male, which was very similar to the Framingham correction formula (QT = 0.234 + 0.154 * RR − 0.012 * male) [37]. For the second method, heart rate was used in a linear regression model with a QT interval similar to that of the Hodges formula. The data showed the slope of this regression to be 0.176 (QT = 0.176 * HR), which was very near the Hodges correction formula (QTcH = QT + 0.00175 (HR-60)) [38]. The third method used was one previously described in Spence et al. [39]. β for females and males in this method was 0.365 (standard error = 0.011) and 0.333 (standard error = 0.011), respectively. The male slope had the same coefficient in the Fridericia formula, and the female slope was only slightly higher. The final method used was introduced by Wernicke et al. [40]. The value of “d” was considered to be the result of the zero correlation between the QT and RR intervals (d = 0.316). Again, the correction formula was similar to the Fridericia formula. The R2 of these correction formulas is reported in Table 3.
Ultimately, attempts to find the best QT correction formula for the current study population led to three previously published formulas, the Framingham, Hodges, and Fridericia formulas. As reported in Additional file 1: Tables S2 and Table 3, these three formulas are closely correlated; thus, a QTc and RR regression analysis was performed to achieve a better comparison.
QTc and RR regression analysis
The best QTc formula is the one that minimizes the influence of RR in the QTc interval. Therefore, when a scatter-dot plot between QTc and RR is drawn, the formula with the lowest slope and R2 closest to zero is the best correction formula.
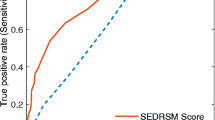
The data from the QTc/RR analysis of each QT correction formula is shown in Table 4. In males, the smallest slope and R2 were related to QTcFri. In females, QTcR had the smallest slope and R2 followed by QTcFri and QTcH. For a better visual comparison, Fig. 1 has been provided. In this figure, a straighter line means the minimum influence of RR in QTc.

Comparison of linear regression slopes of different QTc formulas in both genders. A QTc/RR analysis in male, B QTc/RR analysis in females. QTc corrected QT interval, RR RR interval, Bazett’s correction formula (QTcB), Fridericia’s correction formula (QTcFri), Dmitrienko’s correction formula (QTcD), Framingham’s correction formula (QTcFra), Hodges’s correction formula (QTcH), Rautaharju’s correction formula (QTcR)
The normal limits
The healthy subjects in the current study were n = 3952. The highest ULN (458.92 and 476.84 ms in males and females, respectively) among the QTc was related to Bazett in both genders. As expected, there were differences between males and females in ULN and LLN. Overall, LLNs and ULNs were higher in women. All LLNs and ULNs of each QTc interval are reported in Table 5.
Validation of QTc intervals by mortality
Among the total study population, 79 (1.1%) subjects died within 3 years from registration day, of whom 58% were male and 56% of deaths were due to cardiac causes. Table 6 shows the sensitivity, specificity, PPV, and NPV for all-cause and cardiac mortality predictions for subjects with a QTc higher than ULN in males. In the case of all-cause mortality, the sensitivity levels of QTcB, QTcFra, QTcR, and QTcD were higher than the others (17.39%) with almost equal specificity (~ 93%). In the case of cardiac mortality, QTcB with a sensitivity of 23.07% was the most sensitive, followed by QTcFri, QTcFra, QTcR, and QTcD with a sensitivity level of 15.38% and almost equal specificity (~ 93%). Information about sensitivity, specificity, PPV, and NPV for all-cause and cardiac mortality predictions in females is reported in Additional file 1: Table S4 due to low index values.
Cox regression analysis
A summary of the Cox regression analysis is reported in Table 7. In the unadjusted regression, the HRs of QTcB, QTcFri, QTcFra, QTcR, and QTcD were statistically significant. The highest HR for all-cause mortality was related to QTcFra (HR = 3.20, p value = 0.003). In cardiac mortality, the highest and only significant HR was related to QTcB (HR = 4.31, p value = 0.002). After performing adjusted model analysis with age and heart rate, the highest HR values decreased, yet they both remained statistically significant (p value < 0.05). The results of the Cox regression analysis in female subjects and both genders are reported in Additional file 1: Table S5 and S6. Also, the detailed result of the Cox regression analysis of the un- and multivariate-adjusted model of All-cause and cardiac mortality prediction by QTc > ULN in different QTc intervals in males are reported in Additional file 1: Table S7. One single Cox regression model was performed to allow all QTcs to compete with each other (Additional file 1: Table S8). In this regression analysis, age and heart rate (as continues variables) were forced to stay in the model in all steps. Six correction formulas were competing with each other as a backward stepwise selection variable method. There are two separate regression models for all-cause and CVD mortality. QTcFra in the all-cause mortality model and QTcB in the cardiac-cause mortality model was only remaining in the final step (p value < 0.05).
Discussion
Main findings
The findings of the current study suggest that (1) the best mathematical rate correction QT interval formula is the QTcFri, and (2) QTcB may be the best QT correction formula based on cardiac mortality. (3) Also, our study suggested QTcFra as the best QT correction formula based on all-cause mortality. Attempts to find the best QT correction for the non-hospitalized population in this study led us to the QTcFra, QTcH, and QTcFri formulas. For a better comparison of these three formulas, different statistical analyses were performed, and QTcFri was identified as the best formula for the current study population. To validate it in clinical aspects, QTcFri was surprisingly under the QTcB prediction in both all-cause and cardiac mortality.
To the best of our knowledge, this is the first study to determine the best QT correction formula in an Iranian population. There are several reports in the literature regarding this comparison among formulas; however, they are generally based on hospitalized patients with no consideration given to a normal healthy population. Moreover, there is virtually no mortality rate for assessing and validating their interpretations. Furthermore, QTc intervals are clinically significant, especially with drug administration in apparently normal patients in society and for monitoring the side effects of many drugs, including psychiatry and cardiac medications. A great number of these people are not hospitalized, yet their QT intervals need to be considered before and during the administration of such drugs.
Descriptive data of ECG parameters
CVD is the leading cause of premature death worldwide with 17.9 million deaths in 2012, which is expected to rise to 23 million deaths in 2030. Moreover, the low- and medium-income countries, especially the Eastern Mediterranean countries, account for 50 percent of deaths and 80% of the global burden from this disease [41]. The prevalence and prediction rate of CVD in Iran imply the importance of CVD [42]. ECG as a test with a high prediction value, can be used to predict the chance of CVD development [43]. Descriptive data showed that P duration, PR interval, QRS duration, P and QRS axis were higher in women. Heart rate and all QTc interval had a higher mean and SD in males than females. Pinto Filho et al. [44] in a large Brazilian population showed that mean of P duration, PR interval, QRS duration were higher in their male subjects which were in contrast to our results but in case the mean of P axis was in a line with our study. Moreover, the median of P duration, PR interval, P axis in the aforementioned study was higher than ours. The increasing trends of P duration, PR interval, QRS duration, P axis, and QTc intervals with increasing age were almost similar to other populations such as Brazilian [44], Netherlands [45], Indians [46], and Chinese [47].
QT prolongation
Previous studies have reported that abnormal QT prolongation predisposes individuals to ventricular arrhythmias (such as VF, TdP, and SCD) [16, 18, 48]. It has also been suggested that QT interval prolongation may be a marker of subclinical atherosclerosis [49]. A qualitative review in 2004 [50] reported that there is no evidence of an increased risk of all-cause and cardiac mortality due to QTc prolongation. Although it has been reported that this risk may increase in patients with a history of CVD, a further meta-analysis study by Zhang et al. [51] suggested that there is a relative risk of more than 1.50 in the highest QT interval group compared to the lowest. Due to the importance of QT prolongation and a lack of studies on QT intervals, different QTc formulas, and their comparison in an Iranian population, the current study aimed to find the best QT correction formula and the normal limits based on mathematics and mortality.
Comparing different QTc intervals
Several previous studies have compared different QTc formulas to determine which is the best. The most commonly used formula, Bazett’s, has been challenged in several studies [31, 52,53,54,55,56] due to reasons such as the over-correction of QTc intervals at higher heart rates and under-correction at lower heart rates. The current study also reports the same result. In Fig. 1, it is obvious that QTcB in short RR has much higher values of QTc interval and vice versa. Previous studies [31, 57] have suggested the use of QTcFri, QTcH, and QTcFra instead of QTcB. The current study also suggests these formulas as the best three based on mathematical methods. Luo et al. [31] reported that Bazett's formula is common simply because of its popularity among physicians and their students without considering previous studies. They have also demonstrated some QTc formulas are good for bradycardia while others are better for tachycardia. For example, the Framingham formula has less correction above 100 bpm, and the Hodges formula has less correction at heart rates below 60 bpm than others. Ultimately, they concluded that QTcH was the best formula for their population.
QTc and RR regression are accepted as an assessment for the accuracy of the correction formula [58]. In the ideal form, if the regression line has zero slopes, the value of QTc is statistically independent of RR. In a simpler explanation, the best correction formula is the one that minimizes the influence of RR. The positive and negative values of the slope are evidence for over- and under-correction of formulas. For example, in the positive slope of different QTcs between RR and QTc intervals, some over-correction is expected in RR intervals > 1.0 s, but some under-correction is expected in RR intervals < 1 s. The opposite is expected to happen in the favor of a negative correlation such as QTcB as discussed earlier (Table 4 and Fig. 1). With this evidence, it can be stated that QTcB was the poorest correction formula mathematically in the current study for both males and females. Moreover, the smallest slope and minimum influence of RR in QTc in males was related to QTcFri in this study.
There were also some differences in QTc intervals between males and females. Heart rates and all QTc intervals were statistically higher in females, which was expected and is in line with previous studies [52, 57]. Previous studies have also reported higher values of slope in women compared with men in QT interval and RR analyses [59]. The current study did not show the same in all of QTc intervals, but QTcFri and QTcFra slopes were higher in females. Moreover, the highest differences in slope between males and females belonged to QTcR. Interestingly, the only QTc interval which had a turning point (from a negative to a positive slope) between males and females was QTcFra (− 0.010 in males to 0.019 in females). For this gender difference, there are some possible mechanisms including differences in cardiac electrophysiology, sex hormones, and autonomic nervous system [60,61,62,63].
Normal limits
The results of the current study showed that QTcB had the highest ULN among QTc formulas in both genders and the highest LLN in females. The highest LLN in male subjects was related to QTcR. The ULN and LLN of the best correction formula for the current study population, QTcFri, was near sex-specific clinical standards cutoffs, especially in males (450 ms for males and 470 ms for females [64]). There are also normal limits of differences in gender. Overall, the normal limits were higher in women. QTcB had a ULN at least 11 ms more than the other formulas and was the highest value among others which can be supported by previous studies [31, 57]. It is noteworthy that the abovementioned ULNs were driven from the population and, to some extent, the use of the upper domain of these QTc might be risky in cases of certain drug administration or drug studies. These ULNs should be investigated to be validated for clinical use.
Mortality prediction
In the current study, QTcB, QTcFra, QTcR, and QTcD in all-cause mortality and QTcB in cardiac mortality had the highest sensitivity. Vandenberk et al. [57] recently reported that the highest sensitivity in 30-day mortality was related to QTcFri and QTcFra (27.9%) and in 1-year mortality was related to QTcFri (16.3%). It should be mentioned that the authors did not report the sensitivity of the QTc formulas in cardiac mortality or with a gender distinction. In the Cox regression, an increased risk of all-cause mortality was seen in prolonged QTcB, QTcFri, QTcFra, QTcR, and QTcD, and among them, the highest HR was related to QTcFra. In cardiac mortality, only prolonged QTcB showed an increased risk of mortality among others. It should be mentioned that these increased risks could not be observed in females. Previous studies of cases of mortality HR in prolonged QTc are limited and restricted to a few QTc formulas. The Framingham study [65] reported that in the age and sex-adjusted model, HR for CHD mortality was 1.14 (95% CI 1.10–1.18) in QTcB and 1.09 (95% CI 1.04–1.13) in QTcFra, which is in line with the current results regarding the superiority of QTcB in cardiac mortality compared to others. Schouten et al. [66] reported a 1.8 HR for CVD mortality in subjects with QTcB > 440 ms. Although these two studies had a much longer follow-up, they support the current results. Nielsen et al. [67] showed in a large population study that QTcFra ≥ 466 ms had an HR = 2.53 (95% CI, 2.15–2.98) in all-cause and an HR = 4.08 (95% CI, 2.93–5.69) in cardiac mortality in men. Unfortunately, these studies did not calculate HR in different QTc formulas for a better comparison. A recent study did compare HR in different QTc formulas [57] and reported that the highest HR in 1-year cardiac mortality was QTcR (5.64) followed by QTcB (4.48). Unfortunately, the researchers of that study focused on the all-cause mortality in the main text and concluded that QTcFri and QTcFra are the best correction formulas. In addition, their population was hospitalized and, consequently, had a higher mortality rate, which can be one reason for the differences between their findings and those of the current study.
Limitations
Measuring QT interval, even by an automated method, may produce false-positive QT prolongation due to uncertain determination of QT intervals. Defining the T-wave termination may be challenging in some ECGs for both a physician's eye and computer algorithms [68]. Also, as a 10-s ECG was recorded there may be a problem with QT/RR hysteresis lag and although we tried to record ECG in the optimum state, the stability of heart rate may not be guaranteed [69].
The population approach for finding the best QTc formula may not be the right method, as we do not share the same QT/RR relationship. The individualized QTc formula should be the best method due to individual differences in people. This opinion has been also suggested by others [70, 71]. Unfortunately, a series of ECG for each participant was not available in this study, which makes this limitation an undeniable one.
The better performance of QTcB in mortality prediction may be due simply to over- and under-correction and its artificial prolongation of QTc intervals. This issue cannot be ignored, especially in the current population-based study.
The association of metabolic syndrome, hypertension, obesity, diabetes, impaired glucose tolerance, and elevated insulin levels [72,73,74,75,76,77] with prolonged QTc and the effect other factors discussed earlier [4,5,6,7, 10,11,12,13,14] on QT intervals and cardiovascular events should not be ignored. Moreover, there is an issue about the relation and interrelation of some of these factors on both QT intervals and cardiovascular events at the same time. Thus, the results of further studies should be adjusted with these factors to minimize their influence.
As another limitation, the observed results in males could not be exploited in females. Although the mortality rates of both genders were similar, no relationship could be shown between prolonged QTc and mortality in women. A longer follow-up study with a higher mortality rate and multi-variable adjustment by different analysis method such as machine learning or deep learning [78] should be conducted in the future.
Finally, an urban Iranian population may present different findings while our data were from rural regions. So the validation of the study's findings should be done externally with a different population to enable us to generalize the results of the current study.
Conclusion
QT interval should be corrected by the heart rate of the individuals and there are several heart rate correction formulas. As the QTcFri had the smallest influence of RR in QTc in our study, it is suggested that QTcFri may be the best heart rate correction formula by focusing on mathematical methods. However, if we focus on cardiovascular deaths, despite its poorest performance in mathematical methods, QTcB may be the best one. Practically, it is suggested that physicians use QTcB for a better evaluation of the risks of cardiac mortality. However, in population-based studies, QTcFri might be the one to be used by researchers.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request to the corresponding author.
Abbreviations
- ECG:
-
Electrocardiogram
- LQTS:
-
Long QT syndrome
- VF:
-
Ventricular fibrillation
- TdP:
-
Torsade de Pointes
- SCD:
-
Sudden cardiac death
- QTc:
-
Corrected QT interval
- QTcB:
-
Corrected QT interval by Bazett’s formula
- QTcFri:
-
Corrected QT interval by Fridericia’s formula
- QTcD:
-
Corrected QT interval by Dmitrienko’s formula
- QTcFra:
-
Corrected QT interval by Framingham’s formula
- QTcH:
-
Corrected QT interval by Hodges’s formula
- QTcR:
-
Corrected QT interval by Rautaharju’s formula
- CVD:
-
Cardiovascular diseases
- CHD:
-
Coronary heart disease
- MI:
-
Myocardial infarction
- ULN:
-
Upper limits of normal
- LLN:
-
Lower limits of normal
- PPV:
-
Positive predictive value
- NPV:
-
Negative predictive value
- HR:
-
Hazard ratio
References
Kim SM, George B, Alcivar-Franco D, Campbell CL, Charnigo R, Delisle B, Hundley J, Darrat Y, Morales G, Elayi S-C. QT prolongation is associated with increased mortality in end stage liver disease. World J Cardiol. 2017;9(4):347.
Waddell-Smith KE, Skinner JR. Update on the diagnosis and management of familial long QT syndrome. Heart Lung Circ. 2016;25(8):769–76.
Schwartz PJ, Stramba-Badiale M, Crotti L, Pedrazzini M, Besana A, Bosi G, Gabbarini F, Goulene K, Insolia R, Mannarino S. Prevalence of the congenital long QT syndrome. Circulation. 2009;120(18):1761.
Sohaib SMA, Papacosta O, Morris RW, Macfarlane PW, Whincup PH. Length of the QT interval: determinants and prognostic implications in a population-based prospective study of older men. J Electrocardiol. 2008;41(6):704–10.
Castro VM, Clements CC, Murphy SN, Gainer VS, Fava M, Weilburg JB, Erb JL, Churchill SE, Kohane IS, Iosifescu DV. QT interval and antidepressant use: a cross sectional study of electronic health records. BMJ. 2013;346:f288.
Tisdale JE, Jaynes HA, Kingery JR, Mourad NA, Trujillo TN, Overholser BR, Kovacs RJ. Development and validation of a risk score to predict QT interval prolongation in hospitalized patients. Circ Cardiovasc Quality Outcomes. 2013;6(4):479–87.
Pickham D, Helfenbein E, Shinn JA, Chan G, Funk M, Weinacker A, Liu J-N, Drew BJ. High prevalence of corrected QT interval prolongation in acutely ill patients is associated with mortality: results of the QT in Practice (QTIP) Study. Crit Care Med. 2012;40(2):394–9.
Yazdanpanah MH, Sayyadipoor S, Hojati SR, Nikmanesh A, Farjam M, Homayounfar R. The association of metabolic syndrome and its components with electrocardiogram parameters and abnormalities among an Iranian rural population: the Fasa PERSIAN cohort study. Diabetes Metab Syndrome Obes Targets Ther. 2020;13:2975.
Yazdanpanah MH, Bahramali E, Naghizadeh MM, Farjam M, Mobasheri M, Dadvand S. Different body parts’ fat mass and corrected QT interval on the electrocardiogram: the Fasa PERSIAN cohort study. BMC Cardiovasc Disord. 2021;21(1):1–11.
Pasquier M, Pantet O, Hugli O, Pruvot E, Buclin T, Waeber G, Aujesky D. Prevalence and determinants of QT interval prolongation in medical inpatients. Intern Med J. 2012;42(8):933–40.
Grandinetti A, Seifried S, Mor J, Chang HK, Theriault AG. Prevalence and risk factors for prolonged QTc in a multiethnic cohort in rural Hawaii. Clin Biochem. 2005;38(2):116–22.
Roden DM. Drug-induced prolongation of the QT interval. N Engl J Med. 2004;350(10):1013–22.
Benoit SR, Mendelsohn AB, Nourjah P, Staffa JA, Graham DJ. Risk factors for prolonged QTc among US adults: third National Health and Nutrition Examination Survey. Eur J Cardiovasc Prev Rehabil. 2005;12(4):363–8.
Akylbekova EL, Crow RS, Johnson WD, Buxbaum SG, Njemanze S, Fox E, Sarpong DF, Taylor HA, Newton-Cheh C. Clinical correlates and heritability of QT interval duration in blacks: the Jackson Heart Study. Circ Arrhythmia Electrophysiol. 2009;2(4):427–32.
Moss AJ. Prolonged QT-interval syndromes. JAMA. 1986;256(21):2985–7.
Yap YG, Camm AJ. Drug induced QT prolongation and torsades de pointes. Heart. 2003;89(11):1363–72.
Woosley RL, Schwartz PJ. Drug-induced long QT syndrome and torsades de pointes. In: Cardiac repolarization. Springer; 2020: 185–200.
Straus SM, Kors JA, De Bruin ML, van der Hooft CS, Hofman A, Heeringa J, Deckers JW, Kingma JH, Sturkenboom MC, Stricker BH, et al. Prolonged QTc interval and risk of sudden cardiac death in a population of older adults. J Am Coll Cardiol. 2006;47(2):362–7.
Simpson TF, Salazar JW, Vittinghoff E, Probert J, Iwahashi A, Olgin JE, Ursell P, Hart A, Moffatt E, Tseng ZH. Association of QT-prolonging medications with risk of autopsy-defined causes of sudden death. JAMA Intern Med. 2020;180(5):698–706.
Anderson HN, Bos JM, Haugaa KH, Morlan BW, Tarrell RF, Caraballo PJ, Ackerman MJ. Prevalence and outcome of high-risk QT prolongation recorded in the Emergency Department from an Institution-Wide QT Alert System. J Emerg Med. 2018;54(1):8–15.
Malik M, Färbom P, Batchvarov V, Hnatkova K, Camm A. Relation between QT and RR intervals is highly individual among healthy subjects: implications for heart rate correction of the QT interval. Heart. 2002;87(3):220–8.
Andršová I, Hnatkova K, Helánová K, Šišáková M, Novotný T, Kala P, Malik M. Individually rate corrected QTc intervals in children and adolescents. Front Physiol. 2019;10:994.
Reardon M, Malik M. QT interval change with age in an overtly healthy older population. Clin Cardiol. 1996;19(12):949–52.
Liu D-W, Antzelevitch C. Characteristics of the delayed rectifier current (IKr and IKs) in canine ventricular epicardial, midmyocardial, and endocardial myocytes: a weaker IKs contributes to the longer action potential of the M cell. Circ Res. 1995;76(3):351–65.
Gintant GA. Two components of delayed rectifier current in canine atrium and ventricle: does IKs play a role in the reverse rate dependence of class III agents? Circ Res. 1996;78(1):26–37.
Roden DM. Taking the “idio” out of “idiosyncratic”: predicting torsades de pointes. Pacing Clin Electrophysiol. 1998;21(5):1029–34.
Priori SG, Napolitano C, Schwartz PJ. Low penetrance in the long-QT syndrome: clinical impact. Circulation. 1999;99(4):529–33.
Vink AS, Clur S-AB, Postema PG, Blom NA, Wilde AA. Age, sex and racial differences in cardiac repolarization and arrhythmogenesis. In: Cardiac Repolarization. Springer; 2020: 119–129.
Rabkin S, Cheng X. Nomenclature, categorization and usage of formulae to adjust QT interval for heart rate. World J Cardiol. 2015;7:315–25.
Bazett H. An analysis of the time-relations of electrocardiograms. Ann Noninvasive Electrocardiol. 1997;2(2):177–94.
Luo S, Michler K, Johnston P, Macfarlane PW. A comparison of commonly used QT correction formulae: the effect of heart rate on the QTc of normal ECGs. J Electrocardiol. 2004;37:81–90.
Dash A, Torado C, Paw N, Fan D, Pezeshkian N, Srivatsa U. QT correction in atrial fibrillation–measurement revisited. J Electrocardiol. 2019;56:70–6.
Farjam M, Bahrami H, Bahramali E, Jamshidi J, Askari A, Zakeri H, Homayounfar R, Poustchi H, Malekzadeh R. A cohort study protocol to analyze the predisposing factors to common chronic non-communicable diseases in rural areas: Fasa cohort study. BMC Public Health. 2016;16(1):1090.
CARDIAX computerized ECG system. http://www.imed.hu/en.html.
Altman DG, Bland JM. Measurement in medicine: the analysis of method comparison studies. J R Stat Soc Ser D (Stat). 1983;32(3):307–17.
Sagie A, Larson MG, Goldberg RJ, Bengtson JR, Levy D. An improved method for adjusting the QT interval for heart rate (the Framingham Heart Study). Am J Cardiol. 1992;70(7):797–801.
Hodges M. Bazett’s QT correction reviewed: evidence that a linear QT correction for heart rate is better. J Am Coll Cardiol. 1983;1:694.
Spence S, Soper K, Hoe C-M, Coleman J. The heart rate-corrected QT interval of conscious beagle dogs: a formula based on analysis of covariance. Toxicol Sci. 1998;45(2):247–58.
Wernicke JF, Faries D, Breitung R, Girod D. QT correction methods in children and adolescents. J Cardiovasc Electrophysiol. 2005;16(1):76–80.
Sarrafzadegan N, Mohammmadifard N. Cardiovascular disease in Iran in the last 40 years: prevalence, mortality, morbidity, challenges and strategies for cardiovascular prevention. Arch Iran Med. 2019;22(4):204–10.
Yazdanpanah MH, Homayounfar R, Khademi A, Zarei F, Shahidi A, Farjam M. Short sleep is associated with higher prevalence and increased predicted risk of cardiovascular diseases in an Iranian population: Fasa PERSIAN cohort study. Sci Rep. 2020;10(1):1–13.
Queen SR, Smulevitz B, Rentfro AR, Vatcheva KP, Kim H, McPherson DD, Hanis CL, Fisher-Hoch SP, McCormick JB, Laing ST. Electrocardiographic abnormalities among Mexican Americans: correlations with diabetes, obesity, and the metabolic syndrome. World J Cardiovasc Dis. 2012;2(2):50.
Pinto Filho MM, Brant LC, Padilha-da-Silva JL, Foppa M, Lotufo PA, Mill JG, Vasconcelo-Silva PR, Almeida MdCC, Barreto SM, Ribeiro ALP. Electrocardiographic findings in Brazilian adults without heart disease: ELSA-Brasil. Arq Bras Cardiol. 2017;109(5):416–24.
Rijnbeek PR, Van Herpen G, Bots ML, Man S, Verweij N, Hofman A, Hillege H, Numans ME, Swenne CA, Witteman JC. Normal values of the electrocardiogram for ages 16–90 years. J Electrocardiol. 2014;47(6):914–21.
Macfarlane PW, Lloyd SM, Singh D, Hamde S, Clark E, Devine B, Francq BG, Kumar V. Normal limits of the electrocardiogram in Indians. J Electrocardiol. 2015;48(4):652–68.
Chen C-Y, Chiang BN, Macfarlane PW. Normal limits of the electrocardiogram in a Chinese population. J Electrocardiol. 1989;22(1):1–15.
Sauer AJ, Moss AJ, McNitt S, Peterson DR, Zareba W, Robinson JL, Qi M, Goldenberg I, Hobbs JB, Ackerman MJ. Long QT syndrome in adults. J Am Coll Cardiol. 2007;49(3):329–37.
Festa A, D’Agostino R Jr, Rautaharju P, O’Leary DH, Rewers M, Mykkänen L, Haffner SM. Is QT interval a marker of subclinical atherosclerosis in nondiabetic subjects? The Insulin Resistance Atherosclerosis Study (IRAS). Stroke. 1999;30(8):1566–71.
Montanez A, Ruskin JN, Hebert PR, Lamas GA, Hennekens CH. Prolonged QTc interval and risks of total and cardiovascular mortality and sudden death in the general population: a review and qualitative overview of the prospective cohort studies. Arch Intern Med. 2004;164(9):943–8.
Zhang Y, Post WS, Blasco-Colmenares E, Dalal D, Tomaselli GF, Guallar E. Electrocardiographic QT interval and mortality: a meta-analysis. Epidemiology. 2011;22(5):660.
Strohmer B, Schernthaner CC, Paulweber B, Pichler M. Gender-specific comparison of five QT correction formulae in middle-aged participants in an atherosclerosis prevention program. Med Sci Monitor. 2007;13(4):CR165–71.
Puddu PE, Jouve R, Mariotti S, Giampaoli S, Lanti M, Reale A, Menotti A. Evaluation of 10 QT prediction formulas in 881 middle-aged men from the seven countries study: emphasis on the cubic root Fridericia’s equation. J Electrocardiol. 1988;21(3):219–29.
Malik M. Problems of heart rate correction in assessment of drug-induced QT interval prolongation. J Cardiovasc Electrophysiol. 2001;12(4):411–20.
Chiladakis J, Kalogeropoulos A, Arvanitis P, Koutsogiannis N, Zagli F, Alexopoulos D. Heart rate-dependence of QTc intervals assessed by different correction methods in patients with normal or prolonged repolarization. Pacing Clin Electrophysiol. 2010;33(5):553–60.
Dogan A, Tunc E, Varol E, Ozaydin M, Ozturk M. Comparison of the four formulas of adjusting QT interval for the heart rate in the middle-aged healthy Turkish men. Ann Noninvasive Electrocardiol. 2005;10(2):134–41.
Vandenberk B, Vandael E, Robyns T, Vandenberghe J, Garweg C, Foulon V, Ector J, Willems R. Which QT correction formulae to use for QT monitoring? J Am Heart Assoc. 2016;5(6):e003264.
Ramet J, Benatar A, Decraene T, Vandenplas Y. QT interval in normal infants during sleep with concurrent evaluation of QTcorrection formulae. Med Sci Monitor. 2002;8(5):CR351–6.
Extramiana F, Maison-Blanche P, Badilini F, Pinoteau J, Deseo T, Coumel P. Circadian modulation of QT rate dependence in healthy volunteers: gender and age differences. J Electrocardiol. 1999;32(1):33–43.
Surawicz B, Parikh SR. Differences between ventricular repolarization in men and women: description, mechanism and implications. Ann Noninvasive Electrocardiol. 2003;8(4):333–40.
Magnano AR, Holleran S, Ramakrishnan R, Reiffel JA, Bloomfield DM. Autonomic nervous system influences on QT interval in normal subjects. J Am Coll Cardiol. 2002;39(11):1820–6.
Rautaharju P, Zhou S, Wong S, Calhoun H, Berenson G, Prineas R, Davignon A. Sex differences in the evolution of the electrocardiographic QT interval with age. Can J Cardiol. 1992;8(7):690–5.
Pham TV, Rosen MR. Sex, hormones, and repolarization. Cardiovasc Res. 2002;53(3):740–51.
Goldenberg I, Moss AJ, Zareba W. QT interval: how to measure it and what is “normal.” J Cardiovasc Electrophysiol. 2006;17(3):333–6.
Noseworthy PA, Peloso GM, Hwang SJ, Larson MG, Levy D, O’Donnell CJ, Newton-Cheh C. QT interval and long-term mortality risk in the Framingham Heart Study. Ann Noninvasive Electrocardiol. 2012;17(4):340–8.
Schouten EG, Dekker JM, Meppelink P, Kok FJ, Vandenbroucke JP, Pool J. QT interval prolongation predicts cardiovascular mortality in an apparently healthy population. Circulation. 1991;84(4):1516–23.
Nielsen JB, Graff C, Rasmussen PV, Pietersen A, Lind B, Olesen MS, Struijk JJ, Haunsø S, Svendsen JH, Køber L. Risk prediction of cardiovascular death based on the QTc interval: evaluating age and gender differences in a large primary care population. Eur Heart J. 2014;35(20):1335–44.
Morganroth J, Silber SS. How to obtain and analyze electrocardiograms in clinical trials: focus on issues in measuring and interpreting changes in the QTc interval duration. Ann Noninvasive Electrocardiol. 1999;4(4):425–33.
Malik M, Johannesen L, Hnatkova K, Stockbridge N. Universal correction for QT/RR hysteresis. Drug Saf. 2016;39(6):577–88.
Malik M. Methods of subject-specific heart rate corrections. J Clin Pharmacol. 2018;58(8):1020–4.
Lester RM, Paglialunga S, Johnson IA. QT assessment in early drug development: the long and the short of it. Int J Mol Sci. 2019;20(6):1324.
Festa A, D’Agostino R Jr, Rautaharju P, Mykkänen L, Haffner SM. Relation of systemic blood pressure, left ventricular mass, insulin sensitivity, and coronary artery disease to QT interval duration in nondiabetic and type 2 diabetic subjects. Am J Cardiol. 2000;86(10):1117–22.
Schillaci G, Pirro M, Ronti T, Gemelli F, Pucci G, Innocente S, Porcellati C, Mannarino E. Prognostic impact of prolonged ventricular repolarization in hypertension. Arch Intern Med. 2006;166(8):909–13.
Fauchier L, Maison-Blanche P, Forhan A, D’Hour A, Lépinay P, Tichet J, Vol S, Coumel P, Fauchier JP, Balkau B. Association between heart rate–corrected QT interval and coronary risk factors in 2894 healthy subjects (the DESIR study). Am J Cardiol. 2000;86(5):557–9.
Strohmer B, Pichler M, Iglseder B, Paulweber B. Relationship of QT interval duration with carotid intima media thickness in a clinically healthy population undergoing cardiovascular risk screening. J Intern Med. 2005;257(3):238–46.
Dekker JM, Feskens EJ, Schouten EG, Klootwijk P, Pool J, Kromhout D. QTc duration is associated with levels of insulin and glucose tolerance: the Zutphen elderly study. Diabetes. 1996;45(3):376–80.
Keresztes K, Tamas G, Kadar E, Marton A, ter Kempler P. Autonomic neuropathy and Qt interval prolongation in insulin dependent diabetes mellitus (IDDM) and alcohol-related cirrhosis: possible predictors of survival? Med Sci Monitor. 1998;4(1):CR64–7.
Yazdanpanah MH, Mahmoodian M, Ghanaat F, Nemati MH. A deep neural network model for predicting in-hospital postoperative mortality and complications of open-heart surgeries: the shiraz open heart surgery study. Circulation. 2021;144(Suppl_1):A6996–A6996.
Fridericia LS. Die Systolendauer im Elektrokardiogramm bei normalen Menschen und bei Herzkranken. Acta Med Scand. 1920;53(1):469–86.
Dmitrienke AA, Sides GD, Winters KJ, Kovacs RJ, Rebhun DM, Bloom JC, Groh W, Eisenberg PR. Electrocardiogram reference ranges derived from a standardized clinical trial population. Drug Inf J. 2005;39(4):395–405.
Rautaharju PM, Zhang Z-M, Prineas R, Heiss G. Assessment of prolonged QT and JT intervals in ventricular conduction defects. Am J Cardiol. 2004;93(8):1017–21.
Acknowledgements
The authors appreciate all people that patiently contributed to this study including Kosar Hashemzadeh for her assisting in the manuscript preparation, especially on tables.
Funding
The authors did not receive any specific funding in this study.
Author information
Authors and Affiliations
Contributions
All authors read and approved the final manuscript. Conceptualization: MHY, MF. Methodology: MHY, MF, MMN. Software: MHY. Validation: SS. Formal analysis: MMN. Investigation: MHY, SS. Resources: SS, MF. Data curation: SS, MM. Writing (original draft preparation): MHY, MF. Writing (review and editing): MMN, MF. Visualization: MHY, MF. Supervision: MF. Project administration: MF. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The design of this study followed the guidelines and regulations of regional and national ethics committees. The protocol of this study, with reference number IR.FUMS.REC.1398.157, was approved by the regional and national research ethics committees (the equivalent of institutional review boards) of Fasa University of Medical Sciences.
Consent for publication
Not applicable.
Competing interests
The authors hereby affirm that the manuscript is original, that all statements asserted as facts are based on authors' careful investigation and accuracy, that the manuscript has not been published in total or in part previously and has not been submitted or considered for publication in total or in part elsewhere. Each author acknowledges he/she has participated in the work substantively and is prepared to take public responsibility for the work and authors have no competing interest in the results of the article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
Descriptive data of electrocardiogram parameters stratified by age and sex. Table S2. Mean difference and correlation between different QTc formulas. Table S3. Results of Bland-Altman analysis between different QTc formulas. Figure F1. Bland-Altman graphs of the difference between two QTc intervals versus average. Table S4. Sensitivity Analysis of All-cause and cardiac mortality prediction by QTc > ULN in different QTc intervals in female. Table S5. Cox regression analysis of unadjusted model of All-cause and cardiac mortality prediction by QTc > ULN in different QTc intervals in female. Table S6. Cox regression analysis of the un- and multivariate-adjusted model of All-cause and cardiac mortality prediction by QTc > ULN in different QTc intervals in both genders. Table S7. The detailed result of cox regression analysis of the uni- and multivariate-adjusted model of All-cause and cardiac mortality prediction by QTc > ULN in different QTc intervals in males. Table S8. The detailed result of cox regression analysis multivariate-adjusted model of All-cause and cardiac mortality prediction by QTc > ULN in different QTc intervals in males.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yazdanpanah, M.H., Naghizadeh, M.M., Sayyadipoor, S. et al. The best QT correction formula in a non-hospitalized population: the Fasa PERSIAN cohort study. BMC Cardiovasc Disord 22, 52 (2022). https://doi.org/10.1186/s12872-022-02502-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-022-02502-2