
Abstract
Background
Increased waist circumference (WC) is one of the cardiovascular disease (CVD) risk factors used to predict cardiovascular events. Waist circumference cut-off values for predicting metabolic syndrome and other cardiovascular risks have been previously studied. Carotid intima-media thickness (CIMT) is one of the cardiovascular risk factor recently described and reported to be suitable as it is a direct measurement of vascular quality. Hence the aim of the present study was to determine the optimal WC cut-off point for the prediction of subclinical CVD.
Methods
The study was a cross-sectional study using quantitative methods, conducted among 1318 adults aged between 40 and 60 years old, residing in a rural Black population in Limpopo province. Carotid Intima-Media Thickness measurements were performed using a LOGIQ ultrasound system (GE Healthcare, CT, USA). Waist Circumference (WC) (cm) was measured to the nearest 0.1 cm. Bivariate correlation, logistic regression and receiver operating characteristic were analysed using the statistical package for social sciences version 26.0 software.
Results
Among the total population, 69% were women and 31% men with a mean age of 53 ± 7 years. Among women, WC at a cut-off value of 95 cm gave the highest sensitivity of 57%, the specificity of 55% and an area under the curve (AUC) of 0.588. In men, an optimum WC cut-off point of 82 cm yielded the highest sensitivity and specificity at 72% and 70% respectively, with an AUC of 0.767 p < 0.001.
Conclusion
The traditional waist circumference cut-off points (94 cm for women and 80 cm for men) that are currently used for the diagnosis of metabolic syndrome might not be suitable in the prediction of an increased CIMT.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Introduction
The prevalence of cardiovascular diseases (CVDs) and their associated risk factors are reported to be increasing worldwide [1]. In 2015, CVDs were responsible for about 17.9 million deaths worldwide [1, 2]. Previously, a high prevalence of CVD risks was seen in developed countries, but recent data confirms that half of the global burden of CVDs were reported among low and middle-income countries [3]. This might be due to epidemiological transition, urbanisation, economic development, adoption of a western lifestyle and the improvement of living conditions [4,5,6]. Or it could be due to the increase in the prevalence of obesity, the major risk factor for CVD [4]. In Africa, 38% of all non-communicable disease-related deaths were attributed to CVD [7] and 1 million deaths in sub-Saharan Africa were linked to CVD, contributing 5.5% of the global CVD related deaths [7].
The risk for the development of CVD can be assessed at the subclinical stage [8] by direct assessment of vascular changes, and/or indirectly by assessing the presence of the vascular risk factors [9]. The direct assessment methods include computerised tomography (CT), Magnetic resonance angiography (MRA) and ultrasound scanning [10]. Ultrasound is usually used for the measurements of the carotid intima-media thickness (CIMT) and the presence of plaque for the assessment of atherosclerosis [11]. Ultrasound is the preferred method for epidemiological studies as it is less complicated, inexpensive and non-invasive as it does not expose one to radiation [12].
Obesity, particularly abdominal obesity, is associated with several cardiometabolic risk factors and is also independently associated with atherosclerotic CVDs [13, 14]. Several reports have documented a positive association between abdominal obesity and CIMT [15,16,17]. Abdominal obesity can be assessed using different techniques, among all the techniques waist circumference (WC) is the most commonly used technique as it is non-invasive, cheap and easy to perform compared to Magnetic Resonance Imaging (MRI), computed tomography (CT) and ultrasound [18, 19].
There are several WC cut-off points used to define the risk for CVD. The International Diabetes Federation (IDF) recommended the cut-off point for abdominal obesity using a WC of 94 cm in men and 80 cm in women for European and African descended population [20], while the National Cholesterol Educational Programme Adult Treatment Panel III (NCEP-ATP III) recommends the use of 102 cm for men and 88 cm for women as the cut-off points for defining abdominal obesity without regard to race [21]. However, these standardised cut-offs were concluded based on the European population and they are being used by researchers among sub-Saharan Africans [20]. This might lead to the misdiagnosis of abdominal obesity among Africans since there are discrepancies in fat distribution across different populations [22].
Several studies have tried to come up with waist circumference cut off values among Africans [23,24,25,26], these studies used metabolic syndrome as an outcome event. Recently, CIMT has been recognised as one of the better measure of a subclinical atherosclerosis a CVD risk factor [11]. Therefore, it is of a vital importance to go beyond the use of only traditional CVD risk factors, as the absence and/or presence of the risk factors does not excludes the presence and/or absence of a vascular disease [27]. Hence, the risk for CVD can be better predicted by directly assessing the vascular changes through CIMT. The use of CIMT has been supported by The Screening for Heart Attack Prevention and Education (SHAPE) Task Force [28] and Society of Atherosclerosis Imaging and Prevention [29].
It will be interesting to determine which waist circumference cut-off values could be used to predict a better outcome event (CIMT), as opposed to metabolic syndrome. According to our knowledge, there has not been any study that determined the waist circumference cut off values to predict subclinical CVD among Africans. The aim of the present study was therefore to determine an optimal WC cut-off for the prediction of subclinical CVD as measured by Carotid Intima-Media Thickness among African adults.
Methods
Study design and population
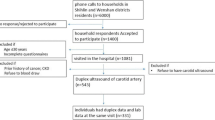
The study was a cross-sectional study using quantitative methods. The study was conducted among 1318 adults, aged between 40 and 60 years old, residing in a rural population of Limpopo, DIMAMO formerly called Dikgale Health and Demographic surveillance system (HDSS) centre. Dikgale is a rural area occupied by Black South Africans predominantly Northern Sotho (Sepedi) speaking. This rural area is composed of 15 rural villages with a total population of 35,000. DIMAMO is situated in South Africa, Limpopo Province, Capricorn district, approximately 30 km away from the University of Limpopo and about 40–50 km northeast of Polokwane, the capital city of Limpopo Province.
Sample collection
For analysis of possible CVD risk factors, overnight fasting blood was collected by a professional nurse from each participant into EDTA-coated tubes (purple top tubes) for blood lipids, and sodium fluoride/potassium oxalate coated tubes (grey top tubes) for glucose analysis. The tubes were centrifuged at 3000 rpm for 10 min and the resulted plasma was separated from red cells within 6 h of collection and transferred into 2 ml cryotubes for storage. The samples were transported to the University of Limpopo laboratory (chemical pathology laboratory) for storage and analysis. Plasma was stored at − 80 °C until use. Glucose tests were performed immediately after separation.
Data collection
Participants with a history of CVD or its treatment, pregnant women and those with incomplete data were excluded from study participation. Anthropometric measurements performed were weight, height and WC. Weight (kg) was measured to the nearest 0.1 kg with the respondent wearing light clothes and without shoes using the Omron-B100 scale. Height (m) was measured to the nearest 0.1 m using a stadiometer. Participants were requested to stand vertically on the stadiometer without shoes. Body mass index (BMI) was calculated dividing weight in kilograms by height measured in meters squared. Waist circumference (WC) (cm) was measured to the nearest 0.1 cm at the level of the iliac crest while the participant was at minimal respiration.
Carotid Intima-Media Thickness measurements were done using a LOGIQe ultrasound system (GE Healthcare, CT, USA), according to detailed procedures and methods that were previously published by Ali et al., 2018. For CVD risk factors, Blood pressure was measured using a digital sphygmomanometer (Omron M6, Omron, Kyoto, Japan), detailed procedure [30]; fasting blood glucose and lipids were determined using the AU480 auto analyzer from Beckman Coulter.
Outcome
In both genders, a CIMT of ≥ 0.80 mm was classified as an increased CIMT [31].
Predictors
In this study, CVD risk factors assessed were obesity, abdominal obesity measured by WC, increased CIMT, hypertension, diabetes and dyslipidaemia. Obesity was defined by a BMI ≥ 30 kg/m2 [32]. Abdominal obesity was defined by a WC of ≥ 94 cm in men and 80 cm in women [20].
Covariates
Hypertension was defined as a resting SBP ≥ 140 mmHg and/or DBP ≥ 90 mmHg [33]. Diabetes was defined as a fasting blood glucose of ≥ 7.0 mmol/L [34]. Dyslipidaemia was defined as one or more of the following: Triglyceride ≥ 1.7 mmol/L, Total Cholesterol ≥ 5.2 mmol/L, High-Density Lipoprotein-Cholesterol (< 1.03 mmol/L in men, < 1.29 mmol/L in women) and Low-Density Lipoprotein-Cholesterol ≥ 3.4 mmol/L [21].
Data analysis
Data were analysed using the Statistical Package for Social Sciences (SPSS) version 26.0 software. The distributions of variables were determined using skewness and kurtosis test, variables that were normally distributed were expressed as mean \(\pm\) standard deviation. In the present study, the following tests were used: An Independent Student t-test was to compare the means of CIMT, biochemical and anthropometric measurements between men and women. Chi-square was used to compare the prevalence of cardiometabolic risk factors. Bivariate correlation was used to determine the association between WC and CIMT. Partial correlation was used to determine the association between WC and CIMT after controlling for age and gender. Linear regression was used to determine whether WC was a predictor of an increased CIMT. The receiver operating characteristics (ROC) curve was used to determine an optimal WC cut-off in predicting an increased CIMT. The optimal cut-off values of waist circumference were calculated by plotting the true-positive rate (sensitivity) against the false-positive rate (1-specificity). For all analysis, statistical significance was set at a probability (p) level of 0.05.
Results
Baseline characteristics of the study population are summarised in Table 1. The study was conducted among 1318 participants from a rural population of which 69% were women and 31% were men. The mean age was 52 ± 8 years and there was no significant difference between men and women. The overall mean BMI, WC and CIMT were 27.7 ± 8.0 kg/m2, 89.6 ± 16.0 cm and 0.65 ± 0.12 mm, respectively. Women had a higher mean BMI, WC, DBP, LDL-c and glucose compared to men (p < 0.001), while CIMT and other biochemical measurements were not significantly different across gender. The overall prevalence of obesity (BMI ≥ 30 km/m2), abdominal obesity (WC ≥ 94 cm in men and ≥ 80 cm in women) and an increased CIMT were 35%, 58% and 9.5% respectively. The prevalence of obesity and abdominal obesity was higher among women than men (p < 0.001). There was no significant difference in the prevalence of an increased CIMT between genders (p = 0.301).
Bivariate correlation shows a positive relationship between WC with both sides of CIMT measurements and their average (p = ≤ 0.001). Waist circumference and CIMT remained significantly associated even after controlling for gender and age (p = ≤ 0.001). Among other measurements of obesity, WC was found to be the only predictor of an increased CIMT (p = 0.007). Individuals with high WC were found to be 1.78 times more likely to be risk for an increased CIMT. See Table 2. Hypertension and glucose were positively associated with an increased CIMT (p = ≤ 0.001), while BMI, insulin, cholesterol, triglyceride, LDL-C and dyslipidaemia were not associated with CIMT. Linear regression analysis was again performed across gender. Among women, age, WC, hypertension and glucose were positively associated with an increased CIMT (p = 0.001, 0.006, 0.001 and 0.003). While insulin was negatively associated with an increased CIMT (p = 0.025). Dyslipidaemia, cholesterol, triglyceride, LDL-C and BMI were not associated with an increased CIMT (Table 3). Among men, age, WC, hypertension and glucose were positively associated with an increased CIMT (p = 0.001). While insulin, dyslipidaemia cholesterol, triglyceride, LDL-C and BMI were not associated with an increased CIMT (Table 4).
The receiver operating characteristics (ROC) curve and its coordinates are summarised in Figs. 1 and 2 as well as Table 5, respectively. Among women, WC at a cut-off value of 95 cm gave the highest sensitivity of 57%, the specificity of 55% and an area under the curve (AUC) of 0.588. The Youden index (YI), 95% confidence interval (CI), positive likelihood ratio (PLR), positive predictive value (PPV) and the p value were 0.120, 0.526–0.650, 1.3, 56% and p = 0.007, respectively. When using sensitivity, a cut-off point of 90 cm yielded the highest sensitivity of 70%. Specificity, PLR, PPV and YI of 43%, 1.2, 55% and 1.2 respectively. For men, WC at a cut-off point of 82 cm yielded the highest sensitivity of 72%, a specificity of 70% with its corresponding AUC of 0.767, 95% CI (0.685–0.848), PLR (2.4) and a p value of p ≤ 0.001.

Receiver Operating Characteristics (ROC) curve for waist circumference to predict the risk of an increased CIMT (> 0.80 mm) in women

ROC curve for waist circumference as a predictor of an increased CIMT (> 0.80 mm) in men
Table 6 summarises WC cut-off points previously reported among African countries as well as from the present study. Several studies investigated optimal WC cut-off points for the prediction of CVD risk among African populations. These studies used different CVD risk factors as an outcome factor and also reported different optimal WC cut-off points for each risk factor. Using CIMT as an outcome, the present study reported a WC cut-off point of ≥ 82 cm for men and ≥ 95 cm for women. This was different to the cut-off points reported by several South African studies using Metabolic Syndrome [23,24,25, 35] and to those recommended by WHO and IDF.
Discussion
In the present study, a high prevalence of selected cardiovascular risk factors was observed. Among the study population, 35% were obese and 58% had a high waist circumference. This was higher compared to 23.6% and 34% reported in the same province by Sengwayo et al. [36] and Maimela et al. [37], respectively. The difference between these two findings might be due to the different WC cut-off points used. In the present study IDF cut-off points of ≥ 94 cm for men and ≥ 80 cm for women were used, while Maimela’s study used the NCEP cut off points of ≥ 102 cm for men and ≥ 88 cm for women. Women had a higher BMI and waist circumference than men. This was also observed in studies conducted in the same population [36,37,38,39]. This might be due to a lack of physical activity among women as compared to men [37].
The prevalence of an increased CIMT was 9.7%. This is low compared to the prevalence observed in a study conducted among Black South Africans by Holland et al. [31]. This may be because the present study is a population-based study that used apparently healthy participants whilst Holland et al. [31] study used participants with established coronary artery disease. In the present study, CIMT did not show any significant difference between men and women. This was supported by a population-based study conducted in Nigeria [40].
Hypertension, one of the risk factors for CVD, was observed among 33% of the study population. This finding was comparable to several studies conducted in the Black rural population [38, 41, 42]. In the present study, women were seen to be more hypertensive as compared to men. The same pattern was reported in previous studies conducted in the same area by Peltzer & Phaswana-mafuya [43] and Alberts et al. [38]. The prevalence of Diabetes (using American Diabetes Association criteria for fasting glucose of ≥ 7.0 mmol/L) was found to be 11%. This is in line with the prevalence reported in KwaZulu-Natal [44] and the same areas as in the present study [38].
In the present study, the prevalence of most cardiovascular risk factors was higher compared to previous studies conducted among the African population. This confirms a continuous increase in the prevalence of CVD risk factors reported by Teo and Dokainish [3].
Previously, CVD risk was only assessed by the presence of CVD risk factors such as old age, hypertension, obesity, high cholesterol and low HDL [45]. There is some experimental evidence against the use of only CVD risk factors in identifying individuals at high risk from the normal ones [46, 47]. It was reported that traditional CVD risk factors alone explain only 60–65% of the CVD risk, and the presence of one or more risk factors is common even among individuals who may not develop a clinical disease [48]. Some acute clinical events may occur among patients without any CVD risk factors [48]. As a result, the better approach currently proposed is to use both CVD risk factors and the information obtained from the assessment of vascular changes of the carotid arteries using an ultrasound [12]. It is reported that the measurement of CIMT provides more accurate information as compared to conventional risk factors, hence it is regarded as a valuable method of assessing CVD risk factors [40].
Previous studies have reported a positive association between cardiovascular outcomes with an increased CIMT [49,50,51]. An increased CIMT was also positively associated with presence of conventional CVD risk factors [16, 52, 53]. Abdominal obesity measured through WC was reported to be one of the traditional risk factors for CVDs [17]. In the present study, WC was found to be positively associated with CIMT and also a predictor of an increased CIMT. These findings have also been reported in previous studies [15, 54].
According to the authors’ knowledge, the present study is the first to determine the optimal WC cut-off points for predicting an increased CIMT as the authors did not find any study that has assessed the optimal WC cut-off points where an increased CIMT was the outcome event. It is also the first study of this kind conducted among Africans. As a result, the findings of the present study are mostly compared with studies investigating WC cut-off points where the outcome event is either metabolic syndrome or other cardiometabolic risk factors.
There are several studies investigated the optimum WC cut-off points in both rural and urban parts of SA and Africa (Table 6), but the outcome variable were other cardiovascular risk factors [23,24,25,26, 35], not an increased CIMT. There are inconsistencies regarding the optimal WC cut-off points for predicting different cardiovascular risk factors across the globe, among African countries and within South Africa (Table 6). Since CIMT is gaining recognition as an indicator of an early progression of atherosclerosis and a risk factor for CVD, it is important to establish the optimal cut-off points for waist circumference using CIMT as an output variable.
As indicated earlier this is the first study to determine the WC cut off values for predicting CIMT and thus there are no available studies to compare to. Hence, findings from the present study were compared to studies used Metabolic syndrome as an outcome event. In the present study, a cut-off point of 95 cm for women yielded the highest AUC, sensitivity and specificity at 0.588, 57% and 55%, respectively. Regardless of the statistical significance of the cut-off (p = 0.007), the sensitivity, specificity and AUC are slightly low to justify the use of this cut-off. This was low due to, both sensitivity and specificity were used to identify an optimum cut-off. When sensitivity is used, a cut-off point of 90 cm yielded the highest sensitivity of 70% and a specificity of 43%. This was also low when compared to AUC, sensitivity and specificity (0.713, 88% and 46% respectively) yielded by a cut-off point of 89.46 cm reported by Owolabi et al. [35] and also when compared to AUC, sensitivity and specificity observed among men. Since specificity and sensitivity of a diagnostic test can differ with the disease prevalence [55], low AUC, specificity and sensitivity among women might be due to differences in sample spectrum between women and men. Another study conducted in SA, reported a cut-off of 92 cm among women (sensitivity 45.9% and specificity 81.9%) [25]. In this study, specificity was prioritised over sensitivity.
For men, a cut-off point of 82 cm yielded the highest AUC, sensitivity and specificity of 0.767, 72% and 70% respectively (p = 0.001). This was low compared to the WC cut-off point reported by several studies here in SA (Table 4) [23,24,25,26, 35] and 94 cm recommended by IDF. Unlike for women, the sensitivity, AUC and specificity produced by a cut-off for were justifiable high to consider the use of this cut-off. At the traditional WC cut-off value of 94 cm, the sensitivity and specificity dropped to 59.3% and 52.3% respectively. Inconsistency regarding the WC cut-off has been observed between the present study and other studies conducted among African population (Table 6). This was also observed even among the studies that used the same outcome (metabolic syndrome).
To the author’s acknowledge, the present study is the first of its kind and as a result data supporting the present study’s findings is limited. The second limitation is that the present study is conducted among one race residing in a rural area and probably one ethnic group and thus findings of the present study may not apply among other population groups.
Conclusion
From the results of the present study, it is concluded that the prevalence of CVD and its associated risk factors are continuing to increase among Black rural populations. Both traditional risk factors and the measurement of CIMT should be used to assess CVD risk. The conventional waist circumference cut-off points (94 cm for men and 80 cm for women) that are being used for predicting metabolic syndrome or other conventional risk factors may not be appropriate for predicting an increased CIMT. Supported by findings from the present and previous studies, a WC cut-off specifically to each risk factor should be generated and used other than using the same cut-off for all risk factors. The present study thus suggests that the waist circumference of 90 cm for women and 82 cm for men is suitable for predicting increased CIMT among this population.
Limitations
To the author’s acknowledge, the present study is the first of its kind and as a result data supporting the present study’s findings is limited. The second limitation is that the present study is conducted among one race residing in a rural area and probably one ethnic group and thus findings of the present study may not apply among other population groups.
Recommendations
Similar studies should be conducted among different ethnic groups and races to validate the results from the present study.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding authors on reasonable request.
Abbreviations
- CIMT:
-
Carotid intima-media thickness
- CI:
-
Confidence interval
- WC:
-
Waist circumference
- DBP:
-
Diastolic blood pressure
- SBP:
-
Systolic blood pressure
- BMI:
-
Body mass index
- CVD:
-
Cardiovascular disease
- ROC:
-
Receiver operating characteristics
- YI:
-
Youden index
- AUC:
-
Area under the curve
- PLR:
-
Positive likelihood ratio
- WHO:
-
World Health Organisation
- IDF:
-
International Diabetes Federation
- NCEP-ATP III:
-
National cholesterol education-adult treatment panel III
- HDL-c:
-
High-density lipoprotein-cholesterol
- LDL-c:
-
Low-density lipoprotein-cholesterol
- CT:
-
Computerised tomography
References
Ruan Y, Guo Y, Zheng Y, Huang Z, Sun S, Kowal P, et al. Cardiovascular disease (CVD) and associated risk factors among older adults in six low-and middle-income countries: results from SAGE Wave 1. BMC Public Health. 2018;18(1):1–13.
Roth GA, Johnson C, Abajobir A, Abd-Allah F, Abera SF, Abyu G, et al. Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J Am Coll Cardiol. 2017;70(1):1–25.
Teo KK, Dokainish H. The emerging epidemic of cardiovascular risk factors and atherosclerotic disease in developing countries. Can J Cardiol. 2017;33(3):358–65.
Keates AK, Mocumbi AO, Ntsekhe M, Sliwa K, Stewart S. Cardiovascular disease in Africa: epidemiological profile and challenges. Nat Rev Cardiol. 2017;14(5):273–93.
Kelly BB, Fuster V. Promoting cardiovascular health in the developing world: a critical challenge to achieve global health. 2010.
Micklesfield LK, Lambert EV, Hume DJ, Chantler S, Pienaar PR, Dickie K, et al. Socio-cultural, environmental and behavioural determinants of obesity in Black South African women. Cardiovasc J Afr. 2013;24(9):369.
Mensah GA, Sampson UKA, Roth GA, Forouzanfar MH, Naghavi M, Murray CJL, et al. Mortality from cardiovascular diseases in sub-Saharan Africa, 1990–2013: a systematic analysis of data from the Global Burden of Disease Study 2013. Cardiovasc J Afr. 2015;26(2 H3Africa Suppl):S6.
Singh SS, Pilkerton CS, Shrader CD, Frisbee SJ. Subclinical atherosclerosis, cardiovascular health, and disease risk: is there a case for the Cardiovascular Health Index in the primary prevention population? BMC Public Health. 2018;18(1):1–11.
Niiranen TJ, Vasan RS. Epidemiology of cardiovascular disease: recent novel outlooks on risk factors and clinical approaches. Expert Rev Cardiovasc Ther. 2016;14(7):855–69.
Cooney M, Cooney M-T, Maher V, Khan B, Leong T, Graham I. Improvement in the estimation of cardiovascular risk by carotid intima-medial thickness: a report from the Dublin Cardiohealth station study. Prev Med Rep. 2015;2:725–9.
Kasliwal RR, Bansal M, Desai D, Sharma M. Carotid intima–media thickness: current evidence, practices, and Indian experience. Indian J Endocrinol Metab. 2014;18(1):13.
Ravani A, Pablo Werba J, Frigerio B, Sansaro D, Amato M, Tremoli E, et al. Assessment and relevance of carotid intima-media thickness (C-IMT) in primary and secondary cardiovascular prevention. Curr Pharm Des. 2015;21(9):1164–71.
Lukács A, Horváth E, Máté Z, Szabó A, Virág K, Papp M, et al. Abdominal obesity increases metabolic risk factors in non-obese adults: a Hungarian cross-sectional study. BMC Public Health. 2019;19(1):1–8.
Fan H, Li X, Zheng L, Chen X, Wu H, Ding X, et al. Abdominal obesity is strongly associated with cardiovascular disease and its risk factors in elderly and very elderly community-dwelling Chinese. Sci Rep. 2016;6(1):1–9.
Eickemberg M, Amorim LDAF, Almeida M da CC de, Aquino EML de, Fonseca M de JM da, Santos I de S, et al. Indicators of abdominal adiposity and carotid intima-media thickness: results from the longitudinal study of adult health (ELSA-Brazil). Arq Bras Cardiol. 2019;(AHEAD).
Ren L, Cai J, Liang J, Li W, Sun Z. Impact of cardiovascular risk factors on carotid intima-media thickness and degree of severity: a cross-sectional study. PLoS ONE. 2015;10(12):e0144182.
Gast KB, Smit JWA, den Heijer M, Middeldorp S, Rippe RCA, le Cessie S, et al. Abdominal adiposity largely explains associations between insulin resistance, hyperglycemia and subclinical atherosclerosis: the NEO study. Atherosclerosis. 2013;229(2):423–9.
De Lucia-Rolfe E, Norris SA, Sleigh A, Brage S, Dunger DB, Stolk RP, et al. Validation of ultrasound estimates of visceral fat in Black South African adolescents. Obesity. 2011;19(9):1892–7.
Shuster A, Patlas M, Pinthus JH, Mourtzakis M. The clinical importance of visceral adiposity: a critical review of methods for visceral adipose tissue analysis. Br J Radiol. 2012;85(1009):1–10.
Alberti KGMM, Zimmet P, Shaw J. The metabolic syndrome—a new worldwide definition. Lancet. 2005;366(9491):1059–62.
Cleeman JI, Grundy SM, Becker D, Clark L. Expert panel on detection, evaluation and treatment of high blood cholesterol in adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP III). JAMA. 2001;285(19):2486–97.
Ujcic-Voortman JK, Bos G, Baan CA, Verhoeff AP, Seidell JC. Obesity and body fat distribution: ethnic differences and the role of socio-economic status. Obes Facts. 2011;4(1):53–60.
Motala AA, Esterhuizen T, Pirie FJ, Omar MAK. The prevalence of metabolic syndrome and determination of the optimal waist circumference cutoff points in a rural South African community. Diabetes Care. 2011;34(4):1032–7.
Crowther NJ, Norris SA. The current waist circumference cut point used for the diagnosis of metabolic syndrome in sub-Saharan African women is not appropriate. PLoS ONE. 2012;7(11):e48883.
Hoebel S, Malan L, Botha J, Swanepoel M. Optimizing waist circumference cut-points for the metabolic syndrome in a South African cohort at 3-year follow-up: the SABPA prospective cohort. Endocrine. 2014;47(3):959–61.
Murphy GAV, Asiki G, Nsubuga RN, Young EH, Maher D, Seeley J, et al. The use of anthropometric measures for cardiometabolic risk identification in a rural African population. Diabetes Care. 2014;37(4):e64–5.
Doneen AL, Bale BF. Carotid intima-media thickness testing as an asymptomatic cardiovascular disease identifier and method for making therapeutic decisions. Postgrad Med. 2013;125(2):108–23.
Naghavi M, Falk E, Hecht HS, Jamieson MJ, Kaul S, Berman D, et al. From vulnerable plaque to vulnerable patient—part III: executive summary of the Screening for Heart Attack Prevention and Education (SHAPE) Task Force report. Am J Cardiol. 2006;98(2):2–15.
in collaboration with the International D, Society A. Appropriate use criteria for carotid intima media thickness testing. Atherosclerosis. 2011;214(1):43–6.
Ali SA, Soo C, Agongo G, Alberts M, Amenga-Etego L, Boua RP, et al. Genomic and environmental risk factors for cardiometabolic diseases in Africa: methods used for Phase 1 of the AWI-Gen population cross-sectional study. Glob Health Action. 2018;11(sup2):1507133.
Holland Z, Ntyintyane LM, Raal FJ, Gill GV. Carotid intima–media thickness is a predictor of coronary artery disease in South African Black patients. Cardiovasc J Afr. 2009;20(4):237.
Purnell JQ. Definitions, classification, and epidemiology of obesity. Endotext. 2018.
Seedat YK, Rayner BL, Veriava Y. South African hypertension practice guideline 2014: erratum. Cardiovasc J Afr. 2015;26(2):90.
Mellitus D. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2005;28(S37):S5-10.
Owolabi EO, Ter Goon D, Adeniyi OV, Ajayi AI. Optimal waist circumference cut-off points for predicting metabolic syndrome among low-income black South African adults. BMC Res Notes. 2018;11(1):1–5.
Sengwayo DG, Moraba MM, Motaung S. Prevalence of obesity and dyslipidaemia in a rural Black community in Limpopo Province: peer reviewed original article. Med Technol SA. 2012;26(2):43–8.
Maimela E, Alberts M, Modjadji SEP, Choma SSR, Dikotope SA, Ntuli TS, et al. The prevalence and determinants of chronic non-communicable disease risk factors amongst adults in the Dikgale health demographic and surveillance system (HDSS) site, Limpopo Province of South Africa. PLoS ONE. 2016;11(2):e0147926.
Alberts M, Urdal P, Steyn K, Stensvold I, Tverdal A, Nel JH, et al. Prevalence of cardiovascular diseases and associated risk factors in a rural Black population of South Africa. Eur J Prev Cardiol. 2005;12(4):347–54.
Cois A, Day C. Obesity trends and risk factors in the South African adult population. BMC Obes. 2015;2(1):1–10.
Talle MA, Baba MM, Ibinaiye PO, Abdul H, Buba F. Carotid Intima-media Thickness and Risk of Cardiovascular Disease among Healthy Adult Volunteers in North Eastern Nigeria. Cardiol Angiol Int J. 2017;1–8.
Alberts M, Choma S, Dikotope S, Ntuli ST, Maimela E. Prevalence and associated risk factors of hypertension amongst adults in a rural community of Limpopo Province, South Africa. Afr J Prim Heal Care Fam Med. 2015;7(1):1–5.
Thorogood M, Connor M, Tollman S, Hundt GL, Fowkes G, Marsh J. A cross-sectional study of vascular risk factors in a rural South African population: data from the Southern African Stroke Prevention Initiative (SASPI). BMC Public Health. 2007;7(1):1–10.
Peltzer K, Phaswana-Mafuya N. Hypertension and associated factors in older adults in South Africa. Cardiovasc J Afr. 2013;24(3):66.
Sahadew N, Singaram VS, Brown S. Distribution, incidence, prevalence and default of patients with diabetes mellitus accessing public healthcare in the 11 districts of KwaZulu-Natal, South Africa. South Afr Med J. 2016;106(4):389–93.
Hajar R. Risk factors for coronary artery disease: historical perspectives. Hear Views Off J Gulf Hear Assoc. 2017;18(3):109.
Armentano RL, Cymberknop LJ. Quantitative vascular evaluation: from laboratory experiments to point-of-care patient (experimental approach). Curr Hypertens Rev. 2018;14(2):76–85.
Greenland P, Knoll MD, Stamler J, Neaton JD, Dyer AR, Garside DB, et al. Major risk factors as antecedents of fatal and nonfatal coronary heart disease events. JAMA. 2003;290(7):891–7.
Pasternak RC, Abrams J, Greenland P, Smaha LA, Wilson PWF, Houston-Miller N. Task force# 1—identification of coronary heart disease risk: is there a detection gap? J Am Coll Cardiol. 2003;41(11):1863–74.
Chambless LE, Heiss G, Folsom AR, Rosamond W, Szklo M, Sharrett AR, et al. Association of coronary heart disease incidence with carotid arterial wall thickness and major risk factors: the atherosclerosis risk in communities (ARIC) study, 1987–1993. Am J Epidemiol. 1997;146(6):483–94.
Rosvall M, Janzon L, Berglund G, Engström G, Hedblad B. Incident coronary events and case fatality in relation to common carotid intima-media thickness. J Intern Med. 2005;257(5):430–7.
Lorenz MW, Schaefer C, Steinmetz H, Sitzer M. Is carotid intima media thickness useful for individual prediction of cardiovascular risk? Ten-year results from the Carotid Atherosclerosis Progression Study (CAPS). Eur Heart J. 2010;31(16):2041–8.
Touboul P-J, Hennerici MG, Meairs S, Adams H, Amarenco P, Bornstein N, et al. Mannheim carotid intima-media thickness consensus (2004–2006). Cerebrovasc Dis. 2007;23(1):75–80.
Femia R, Kozakova M, Nannipieri M, Gonzales-Villalpando C, Stern MP, Haffner SM, et al. Carotid intima-media thickness in confirmed prehypertensive subjects: predictors and progression. Arterioscler Thromb Vasc Biol. 2007;27(10):2244–9.
Zhang L, Yun S, Jian Z, Pan JM, Yu HY, Chen HB, et al. Relationship between waist circumference and elevation of carotid intima-media thickness in newly-diagnosed diabetic patients. Biomed Environ Sci. 2014;27(5):335–42.
Leeflang MMG, Rutjes AWS, Reitsma JB, Hooft L, Bossuyt PMM. Variation of a test’s sensitivity and specificity with disease prevalence. CMAJ. 2013;185(11):E537–44.
Acknowledgements
The authors acknowledge the community in the DIMAMO HDSS (the then Dikgale HDSS) for their participation in the study and the tribal authorities for granting permission to conduct the study. The authors further acknowledge the field workers for helping with data collection and recruitment of the participants.
Funding
The present study is a sub-project of the AWI-Gen Genomic and environmental risk factors for cardiometabolic diseases among Africans. National Institutes of Health (NIH) (U54HG006938) was the primary funders for the AWI-Gen project. Some of the laboratory consumables were funded by the Flemish Interuniversity Council (VLIR).
Author information
Authors and Affiliations
Contributions
MCR (corresponding author) designed the study, wrote the manuscript, contributed to data collection and statistical analysis. SC was involved in designing the study, contributed to data analysis and literature searches and was involved from the first draft through to the final draft of the manuscript. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All methods used in the present study were carried out in accordance with relevant guidelines and regulations aligned with the Declaration of Helsinki and approved by the Turfloop Research Ethics Committee, TREC/124/2015: PG. Permission to conduct the study at Dikgale was obtained from Dikgale tribal authorities. Participants who volunteered to participate were given consent forms translated to their home language and they gave their informed consent by signing. The participants were ensured of anonymity and confidentiality and that they could withdraw from the study at any time without any repercussions.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no conflict of interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ringane, M.C., Choma, S.S.R. The optimal WC cut-off points for the prediction of subclinical CVD as measured by carotid intima-media thickness among African adults: a cross-sectional study. BMC Cardiovasc Disord 21, 575 (2021). https://doi.org/10.1186/s12872-021-02389-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-021-02389-5