
Abstract
Background
Ventricular conduction blocks (VCBs) are associated with poor outcomes in patients with known cardiac diseases. However, the prognostic implications of VCB patterns in dilated cardiomyopathy (DCM) patients need to be evaluated. The purpose of this study was to determine all-cause mortality in patients with DCM and VCB.
Methods
This cohort study included 1119 DCM patients with a median follow-up of 34.3 (19.5–60.8) months, patients were then divided into left bundle branch block (LBBB), right bundle branch block (RBBB), intraventricular conduction delays (IVCD) and narrow QRS groups. The all-cause mortality was assessed using Kaplan-Meier survival curves and Cox regression.
Results
Of those 1119 patients, the all-cause mortality rates were highest in patients with IVCD (47.8, n = 32), intermediate in those with RBBB (32.9, n = 27) and LBBB (27.1 %, n = 60), and lowest in those with narrow QRS (19.9 %, n = 149). The all-cause mortality risk was significantly different between the VCB and narrow QRS group (log-rank χ2 = 51.564, P < 0.001). The presence of RBBB, IVCD, PASP ≥ 40 mmHg, left atrium diameter and NYHA functional class were independent predictors of all-cause mortality in DCM patients.
Conclusions
Our findings indicate that RBBB and IVCD at admission,but not LBBB, were independent predictors of all-cause mortality in patients with DCM.
Similar content being viewed by others

Background
Dilated cardiomyopathy (DCM), a leading cause of heart failure and arrhythmia, is a disease of the heart muscle characterized by ventricular dilation and impaired systolic function. The prognosis in patients with DCM is poor. However, the clinical spectrum is wide, and it is difficult for physicians to predict which clinical course an individual patient may follow.
Patients with DCM present with an increase in the QRS duration in the presence of a ventricular conduction block (VCB) [1–3]. There is controversy regarding the type of bundle branch block (BBB) that is associated with poorer outcomes in patients with heart failure (HF) [4–8]. Most studies indicate that left BBB (LBBB) is an independent prognostic marker, whereas right BBB (RBBB) is a weaker marker or not associated with a worse prognosis. Conversely, two studies recently showed that RBBB but not LBBB is associated with an increased 1-year and 4-year mortality risk in hospitalized patients with HF [9, 10]. Patients with intraventricular conduction delays (IVCDs) can also present with DCM, often without specifying the particular type of BBB. These patients also have worse clinical outcomes [1–3].
The prognostic implications of VCB in the long-term mortality of patients with DCM merit examination due to the lack of data on this issue. Therefore, in the present study, we evaluated the association of VCB patterns and all-cause mortality and compared the prognostic values of RBBB, LBBB, and IVCD in hospitalized patients with DCM.
Subjects and methods
Patients and follow-up
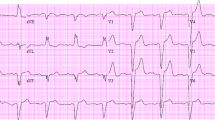
This study was a retrospective, observational cohort study of patients with DCM observed from November 2003 to September 2011. VCB (LBBB, RBBB, IVCD) were identified from records of individual 12-lead ECGs in 1317 patients (Fig. 1). The patients were admitted due to their decompensation symptoms and the physical signs of heart failure, and DCM was defined as systolic dysfunction with LV dilation in the absence of an apparent secondary cause of cardiomyopathy [11]. We measured the following DCM exclusion criteria [12, 13]: systemic hypertension (>160/100 mmHg), coronary artery disease (>50 % in one or more major branches), chronic excess alcohol consumption (>40 g/day for females, > 80 g/day for males for more than five years after 6 months of abstinence), systemic diseases known to cause IDC, pericardial diseases, congenital heart disease, cor pulmonale, and rapid, sustained supraventricular tachycardia. Of the 1317 enrolled patients, 23 patients with missing electrocardiograph test results and 175 patients with various secondary cardiomyopathies were excluded from the study. The secondary cardiomyopathies included the following: 80 patients with ischemic heart disease by coronary angiography; 26 patients with overt hyper- and hypothyroidism thyroid disease; 24 patients with alcohol-induced cardiomyopathy; 16 patients with congenital heart disease; 16 patients with left ventricle noncompaction; 7 patients with chronic anemia (hemoglobin <60 g/L); 2 patients with peripartum cardiomyopathy; and 4 patients with rheumatic heart disease or systemic immune disease (Fig. 2). Thus, the final analysis included 1119 patients. The primary end point of the study was all-cause mortality, which was assessed for all patients through their medical records (patient’s hospital records, periodically examining the patient in the outpatient clinic) and medical follow-up calls with trained personnel. Data from patients who underwent cardiac transplantation were censored at the time of transplantation. The median follow-up period was 34.3 (19.5–60.8) months, and the study protocol was approved by the Ethics Commission of Fuwai Hospital.

An example figure of narrow QRS, LBBB, RBBB, and IVCD

Derivation of the study cohort
Echocardiography
The patients were imaged in the left lateral decubitus position using a commercially available system equipped with a 3.5 MHz transducer. Two-dimensional gray-scale, pulsed, continuous, color Doppler data were acquired from the parasternal and apical views. The left ventricular ejection fraction (LVEF) was calculated using the biplane Simpson’s technique.
Because pulmonary artery systolic pressure (PASP) is equal to the right ventricular systolic pressure in the absence of pulmonary stenosis, PASP was estimated using Doppler echocardiography by calculating the right ventricular to right atrial pressure gradient during systole (approximated by the modified Bernoulli equation as 4v2, where v is the velocity of the tricuspid regurgitation jet in m/s). Right atrial pressure, estimated based on the echocardiographic characteristics of the inferior vena cava and assigned a standardized value, was then added to the calculated gradient to give PASP. According to the new guideline, presence of PASP ≥ 40 mmHg was likely to be pulmonary hypertension (PH) [14].
Statistical analyses
Continuous variables are expressed as the means ± SDs or medians and interquartile ranges. The categorical variables among groups were compared using chi-square (χ 2) tests. Analysis of variance was used to compare continuous variables among multiple groups. Hazard ratios with 95 % confidence intervals were used to estimate the adjusted relative risk of the VCB groups. The Kaplan-Meier survival curves were compared using the log-rank test. Multivariate Cox proportional hazards regression models were used to adjust for any confounding variables among groups. First, the potential variables were evaluated by univariate analysis and were then selected based on their clinical and statistical significance. Second, a multivariate analysis was performed using Cox proportional hazards regression modelling adjusted for baseline variables. SPSS version 16.0 software (SPSS, Chicago, Illinois) was used for all statistical analyses. All of the tests were two-sided, and a p value < 0.05 was used to determine statistical significance.
Results
Characteristics of the study population
The cohort consisted of 1119 patients with DCM: 298 (26.6) women and 821 (73.4) men; 1076 (96.2) were from the Han population and 43 (3.8 %) were from other races: the mean age was 51.1 ± 14.7 years. Of those, 19.8 (n = 221) had LBBB, 7.3 (n = 82) had RBBB, 6.0 (n = 67) had IVCD, and 66.9 % (n = 749) had narrow QRS. Table 1 summarizes the baseline clinical characteristics of the cohort. Among the patients with VCBs (LBBB, RBBB and IVCD) and narrow QRS, the number of women with RBBB was lower, and there was a lower frequency of a history of hypertension but a greater frequency of PASP ≥ 40 mmHg in patients with RBBB. Patients with LBBB were older, were predominantly male, had more frequent essential hypertension and had longer QRS durations, QT intervals and larger LV diameters. The patients with IVCD had higher levels of circulating bilirubin, larger left atriums (LAs), larger right ventricle (RV) diameters, longer PR intervals, and less use of beta blockers, aspirin and spironolactone during admission.
Relation between VCB patterns and all-cause mortality
Among the 1119 patients studied, 268 died and 3 underwent heart transplantation during a median follow-up of 34.3 (19.5–60.8) months. The all-cause mortality rates were highest in patients with IVCD (47.8 %, n = 32); intermediate in patients with RBBB (32.9, n = 27) and LBBB (27.1 %, n = 60); and lowest in patients with narrow QRS (19.9 %, n = 149). Over the median of 34.3 month follow-up, there was a significant difference in all-cause mortality risk between the VCB and narrow QRS groups (log-rank χ 2 = 51.564, P < 0.001) (Fig. 3).

Kaplan-Meier survival curves for patients with DCM: patients with LBBB, RBBB, IVCD and narrow QRS (log-rank χ 2 = 51.564, P < 0.001). Abbreviations: DCM, dilated cardiomyopathy; VCB, Ventricular conduction block; LBBB, left bundle branch block; RBBB, right bundle branch block; IVCD, intraventricular conduction delay
Cox proportional hazard models
Table 2 summarizes the results of the Cox models in which each of the parameters were entered separately as the mortality explanatory variable. The univariate analysis indicated that age, history of essential hypertension and atrial fibrillation (AF), NYHA functional classes, disease duration, systolic blood pressure, diastolic blood pressure, LV, LA diameters, LVEF, PASP ≥ 40 mmHg, and the presence of LBBB, RBBB and IVCD were predictors of all-cause mortality in DCM patients. After adjustments for age, gender, history of essential hypertension and AF, smoking and drinking status, disease duration, blood pressure, heart rate, LV diameter and LVEF value, using either forward or backward selection, and the presence of RBBB, IVCD, PASP ≥ 40 mmHg, the NYHA functional class and LA diameter were the only variables that remained in the model and emerged as important predictors. However, unlike RBBB and IVCD, LBBB was not a predictor of death using the multivariate analysis.
Discussion
In this study, we investigated the associations among different patterns of VCB and all-cause mortality in patients with DCM. Our major new finding suggests that RBBB and IVCD upon admission, but not LBBB, were strong predictors of all-cause mortality in patients with DCM.
Several studies investigating the predictive value of QRS morphology in patients with HF yielded conflicting results regarding mortality risk associated with the BBB pattern [4–7]. Baldasseroni et al. [5, 6] reported that complete LBBB, but not RBBB, was associated with a higher adjusted 1-year mortality rate in 5,517 outpatients with HF. McCullough et al. [4] found higher 2-year mortality rates for RBBB and LBBB compared with patients with normal QRS, but a multivariate analysis demonstrated that RBBB was not as powerful a predictor of mortality as LBBB. Most recently, Mueller et al. [7] analyzed the impact of the BBB pattern on long-term mortality and found that the mortality was significantly higher in HF patients with RBBB. Two studies recently showed that RBBB, but not LBBB, is associated with increased mortality risk in HF patients [9, 10]. None of these studies, however, reported the relationship between RBBB and mortality risk in the patients with DCM. In the present study, we found that RBBB and IVCD patients with DCM had a higher all-cause mortality than patients with LBBB, and patients with any pattern of VCB had higher all-cause mortality rates than patients with a narrow QRS. A multivariate analysis demonstrated that RBBB and IVCD, but not LBBB, were the predictors of all-cause mortality in patients with DCM.
Approximately 30% of patients with heart failure or cardiomyopathy have VCBs, such as left or right bundle-branch blocks [5, 9]. Some studies have shown that in patients with HF, the prevalence of LBBB is higher than in patients with RBBB [4, 5, 7]. LBBB is associated with more severe HF characterized by an advanced NYHA functional class and decreased LVEF, whereas RBBB is more prevalent in men and is not associated with advanced HF symptoms or ventricular dysfunction [5, 6]. In our study, the prevalence of VCB was 33.1 %; more patients had LBBB than RBBB or IVCD. Patients with LBBB had longer QRS durations, larger LV diameters and lower LVEF values than those with RBBB. However, patients with RBBB had more frequent of PASP ≥ 40 mmHg, along with larger RV diameters, than those with LBBB.
One of the reasons for a worse prognosis in patients with RBBB may be that they have an elevated pulmonary pressure compared with those with LBBB or a narrow QRS. Acquired RBBB is often associated with PH and right-sided cardiac failure, and PH complicated by heart failure is generally considered to be an indicator of a poor prognosis [11, 15]. In addition, right ventricular dysfunction has an additive predictive value in patients with left ventricular systolic dysfunction [16]. Furthermore, RBBB may be a marker not only of right ventricular dysfunction but also of severe intraventricular desynchronization of both ventricles. Recently, Fantoni et al. [17] reported that patients with RBBB had larger right ventricle electrical conduction delays compared with patients with LBBB using electromagnetic, catheter-based, 3-dimensional mapping. In the present study, compared with LBBB, patients with RBBB had more frequent of PASP ≥ 40 mmHg, larger RV diameters and higher all-cause mortality rates during follow-up.
Very limited data exists on patients with IVCD. Patients with myocardial infarction with IVCD had significantly greater interventricular asynchronies and higher BNP levels than post-myocardial infarction patients without IVCD [18]. In the Multicenter Unsustained Tachycardia Trial (MUSTT), patients with LBBB or IVCD had lower ejection fractions and a higher prevalence of congestive heart failure than those without these abnormalities. The presence of IVCD was associated with a 1.5-fold increased risk of cardiac arrest and total mortality in the patients treated with cardiac resynchronization therapy (CRT) [8]. In another study on heart failure with CRT, the all-cause mortality was also higher in patients with IVCD than LBBB or RBBB; the worst prognosis was seen in patients with IVCD [19]. The reason for the higher mortality rates in patients with IVCD is unclear, and further research is needed to confirm the role of IVCD in DCM.
The present study has several limitations. Like all hospital-based cohorts, this is a selected population of patients who have been referred for treatment. As with many studies of chronic diseases, the time of disease onset is not precisely known, and there may be variations in the length of the preclinical phase that influences the relationship between IVCD, PH and death. Because the N-terminal pro-brain natriuretic peptide (NT-pro-BNP) test was not commonly used until the later years of this study and was missing in 341 patients, we excluded NT-pro-BNP from the multivariate Cox analysis to avoid potential confounding variables in the statistical analyses. Ideally, all patients with DCM should be confirmed to be free of coronary artery disease. In practice, however, coronary arteriography is not routinely performed in all patients with congestive heart failure. Because retrospective studies cannot control the conditions under which patients are recruited or investigated, aside the patients who were once undertaken coronary artery angiography, coronary CT scan or cardiac radionuclide imaging in the other hospitals, there were only 334 patients undertaken coronary artery angiography and 80 patients with positive results in the present study. In addition, to exclude the confusion with ventricular hypertrophy, we defined patients with VCB as QRS duration more than 120 ms. Finally, the patients who creceived ICDs (implantable cardiac defibrillators) or CRTs were not included, and the use of spironolactone and digoxin was higher in the present study.
Conclusions
The present study indicated that RBBB and IVCD at admission were independent predictors of all-cause mortality in patients with DCM.
References
Bristow MR, Feldman AM, Saxon LA. Heart failure management using implantable devices for ventricular resynchronization: Comparison of Medical Therapy, Pacing, and Defi brillation in Chronic Heart Failure (COMPANION) trial. COMPANION Steering Committee and COMPANION Clinical Investigators. J Card Fail. 2000;6:276–85.
Kass DA, Chen CH, Curry C, Talbot M, Berger R, Fetics B, et al. Improved left ventricular mechanics from acute VDD pacing in patients with dilated cardiomyopathy and ventricular conduction delay. Circulation. 1999;99:1567–73.
Shamim W, Francis DP, Yousufuddin M, Varney S, Pieopli MF, Anker SD, et al. Intraventricular conduction delay: a prognostic marker in chronic heart failure. Int J Cardiol. 1999;70:171–8.
McCullough PA, Hassan SA, Pallekonda V, Sandberg KR, Nori DB, Soman SS, et al. Bundle branch block patterns, age, renal dysfunction, and heart failure mortality. Int J Cardiol. 2005;102:303–8.
Baldasseroni S, Gentile A, Gorini M, Marchionni N, Marini M, Masotti G, et al. Intraventricular conduction defects in patients with congestive heart failure: left but not right bundle branch block is an independent predictor of prognosis. A report from the Italian Network on Congestive Heart Failure (IN-CHF database). Ital Heart J. 2003;4:607–13.
Baldasseroni S, Opasich C, Gorini M, Lucci D, Marchionni N, Marini M, et al. Left bundle-branch block is associated with increased 1-year sudden and total mortality rate in 5517 outpatients with congestive heart failure: a report from the Italian network on congestive heart failure. Am Heart J. 2002;143:398–405.
Mueller C, Laule-Kilian K, Klima T, Breidthardt T, Hochholzer W, Perruchoud AP, et al. Right bundle branch block and long-term mortality in patients with acute congestive heart failure. J Intern Med. 2006;260:421–8.
Zimetbaum PJ, Buxton AE, Batsford W, Fisher JD, Hafley GE, Lee KL, et al. Electrocardiographic predictors of arrhythmic death and total mortality in the multicenter unsustained tachycardia trial. Circulation. 2004;110:766–9.
Barsheshet A, Leor J, Goldbourt U, Garty M, Schwartz R, Behar S, et al. Effect of bundle branch block patterns on mortality in hospitalized patients with heart failure. Am J Cardiol. 2008;101:1303–8.
Barsheshet A, Goldenberg I, Garty M, Gottlieb S, Sandach A, Laish-Farkash A, et al. Relation of bundle branch block to long-term (four-year) mortality in hospitalized patients with systolic heart failure. Am J Cardiol. 2011;107:540–4.
Maron BJ, Towbin JA, Thiene G, Antzelevitch C, Corrado D, Arnett D, et al. Contemporary definitions and classification of the cardiomyopathies: an American Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention. Circulation. 2006;113(14):1807–16.
Elliott P. Cardiomyopathy. Diagnosis and management of dilated cardiomyopathy. Heart. 2000;84(1):106–12.
Mohan SB, Parker M, Wehbi M, Douglass P. Idiopathic dilated cardiomyopathy: a common but mystifying cause of heart failure. Cleve Clin J Med. 2002;69(6):481–7.
Galiè N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS)Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Heart J. 2016;37(1):67–119.
Abd El Rahman MY, Abdul-Khaliq H, Vogel M, Alexi-Meskishvili V, Gutberlet M, Lange PE. Relation between right ventricular enlargement, QRS duration, and right ventricular function in patients with tetralogy of Fallot and pulmonary regurgitation after surgical repair. Heart. 2000;84:416–20.
de Groote P, Millaire A, Foucher-Hossein C, Nugue O, Marchandise X, Ducloux G, et al. Right ventricular ejection fraction is an independent predictor of survival in patients with moderate heart failure. J Am Coll Cardiol. 1998;32:948–54.
Fantoni C, Kawabata M, Massaro R, Regoli F, Raffa S, Arora V, et al. Right and left ventricular activation sequence in patients with heart failure and right bundle branch block: a detailed analysis using three-dimensional non-fluoroscopic electroanatomic mapping system. J Cardiovasc Electrophysiol. 2005;16:112–9.
Ciuraszkiewicz K, Janion M, Dudek D, Gawor Z. Plasma B-type natriuretic peptide as a marker of myocardial asynchrony. Cardiology. 2009;113:193–7.
Rickard J, Kumbhani DJ, Gorodeski EZ, Baranowski B, Wazni O, Martin DO, et al. Cardiac resynchronization therapy in non-left bundle branch block morphologies. Pacing Clin Electrophysiol. 2010;33:590–5.
Acknowledgments
This study was supported by grants from the National Natural Science Foundation of China (no. 81000104, 81160141, 81470521).
Availability of data and materials
The datasets supporting all the conclusions of this article are included within the article.
Authors’ contributions
XL, RL, GN and WFconducted the patients’ enrollment, data collection and follow-up work. XL, XY and XX participated in the data collection and performed the statistical analysis. WH, XW, XX and MF conceived of the study and participated in its design and coordination, and they helped to draft the manuscript. All of the authors read and approved of the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
This study was submitted to and approved by the Ethics Commission of Fuwai Hospital. This is a retrospective study, so the content to participate is not applicable.
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Li, X., Luo, R., Fang, W. et al. Effects of ventricular conduction block patterns on mortality in hospitalized patients with dilated cardiomyopathy: a single-center cohort study. BMC Cardiovasc Disord 16, 136 (2016). https://doi.org/10.1186/s12872-016-0313-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12872-016-0313-4