
Abstract
Background
Postoperative delirium (POD) is an acute form of brain dysfunction that can result in serious adverse consequences. There has been a link between cognitive dysfunction and poor sleep. The present study aimed to determine the association and prediction of subjective sleep quality and postoperative delirium during major non-cardiac surgery.
Methods
One hundred and thirty-four patients, aged 60 years or older, were scheduled for elective laparotomy or orthopaedic procedures. The Pittsburgh Sleep Quality Index (PSQI) and sleep log were used to assess perioperative subjective sleep quality in participants. Nursing Delirium Screening Checklist (NU-DESC) was used for screening, and the Confusion Assessment Method (CAM) was used to diagnose POD during the first seven days following surgery. The association between subjective sleep quality and POD was assessed using a multivariate logistic regression model. Thereafter, the prediction performance of subjective sleep quality was evaluated using a receiver operating characteristic (ROC) curve.
Results
All assessments were completed on 119 patients who had an average PSQI score of 7.0 ± 2.4 before surgery. 23 patients (19.3%) suffered from POD. The multivariate logistic regression analysis showed that the occurrence of POD was closely related to age, BMI, PSQI and operation time. After adjusting for related factors, there was a statistically significant association between PSQI and POD occurrence (OR = 1.422, 95%CI 1.079–1.873, per 1-point increase in PSQI). The ROC curve analysis showed that the optimal PSQI cutoff value was 8.0 for predicting POD, and the area under the ROC (AUROC) value of PSQI was 0.741 (95%CI 0.635 to 0.817). The AUROC of the model developed by the multivariate logistic regression analysis was 0.870 (95%CI 0.797 to 0.925).
Conclusions
The study found that preoperative subjective sleep quality was strongly associated with POD during major non-cardiac surgery. Additionally, PSQI combined with age, BMI, and operation time improved POD prediction.
Similar content being viewed by others
Introduction
Postoperative delirium (POD), occurring in the hours to days after surgical procedures, is an acute form of brain dysfunction and it is associated with numerous adverse outcomes, including decreased physical function, declined activities of daily living, prolonged hospitalization, and increased risks of rehospitalization and death [1,2,3,4]. Nevertheless, the pathogenesis of POD is unclear, and the efficacy and acceptability of pharmacological interventions for the treatment is uncertain, so identifying associated risk factors are particularly crucial to preventing its occurrence [5,6,7].
Sleep is a natural state of reduced arousal that promotes the organismal health and cognitive function. Self-reported sleep quality has been associated with cognitive performance [8]. Both short and long sleep may predict cognitive impairment, suggesting a U-shaped association [9]. Poor sleep health is common among perioperative patients [10, 11]. Due to the disease itself, accompanying symptoms, psychological factors and other reasons, patients often suffer from sleep problems [12]. Meanwhile, POD patients may show lethargy or sleep cycle inversion, which may affect the postoperative outcome [13, 14]. It has been verified that sleeping disorders are significantly associated with the increased risk of developing POD [15, 16].
However, whether subjective sleep quality can serve as a predictor for POD in patients undergoing major surgery remains unclear. Thus, the goal of this study was to determine the association and prediction of subjective sleep quality and POD during major non-cardiac surgery.
Materials and methods
The observational study was conducted in the department of anesthesiology of Ningbo No. 2 Hospital between January 2020 and December 2020. The protocol approved by the Ethics Committee of Ningbo No. 2 Hospital (approval No. PJ-NBEY-KY-2017-029-01), and registered with the Chinese Clinical Trial Registry (www.chictr.org.cn; identifier: ChiCTR-OOC-17,013,414). Before surgery, the patients or their family members provided written informed consent.
Patient selection
Patients scheduled for non-cardiac major surgery under general anesthesia were eligible for the study. Inclusion criteria: (1) aged 60 years and older; (2) undergoing laparotomy (gastrointestinal tumors surgery) or orthopaedic operation (unilateral hip or knee replacement); (3) American Society of Anesthesiologists (ASA) ≤ grade III. Exclusion criteria: (1) pre-existing neurological or psychiatric conditions (review of medical records); (2) having an alcohol or drug dependency (based on Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-V) criteria); (3) preoperative Mini-Mental State Examination (MMSE) score < 20; (4) Geriatric Depression Scale (GDS) score >5; (5) with impaired vision or hearing, unable to read or speak; (6) surgical duration of greater than 4 h; (7) data not completed or lost to follow-up.
Sleep quality assessment
Following hospital admission, sleep quality of the patients over the previous month was assessed with the Pittsburgh Sleep Quality Index (PSQI) [17]. The PSQI consists of 19 items categorized into 7 subscales: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction. The subscales are scored from 0 to 3 (0, very good; 1, fairly good; 2, fairly bad; and 3, very bad), and the total score ranges from 0 to 21. Higher scores indicate poorer sleep quality. Postoperative sleep quality was assessed by a sleep log, which was revised in accordance with the PSQI.
Confirmation of POD
The Confusion Assessment Method (CAM) was used by a specially trained staff to diagnose POD [18], that was evaluated twice a day (8:00 am-10:00 am and 4:00 pm-6:00 pm) during the first 7 postoperative days [19]. Meanwhile, the Nursing Delirium Screening Checklist (NU-DESC) was used by trained nurses to screen for POD in patients [20, 21]. In case of a positive screening, the staff used the CAM to diagnose POD again.
Perioperative management
The patients enrolled in the study underwent general anesthesia with orotracheal intubation. Induced anesthesia was achieved using etomidate, propofol, rocuronium, and sufentanil, then maintain anesthesia was achieved through the use of sevoflurane inhalation, propofol, and remifentanil. Anesthetics were modified to achieve a bispectral index (BIS) between 40 and 60 as a guide to anesthesia depth. Hypotension was defined as a mean arterial pressure (MAP) below 60 mmHg, or 30% of the baseline MAP. Intraoperatively, hypotension was treated with vasoactive drugs immediately and then MAP was maintained at a stable level (20% above or below baseline). In most cases, dexmedetomidine was not restricted, and the anesthesiologist could use it according to the medication’s instructions. As a standard procedure, all patients received postoperative analgesia with a patient-controlled analgesia pump.
Clinical data collection
Perioperative clinical data were collected as follows: (1) data on age, gender, body mass index (BMI), ASA physical status, years of education and lifestyle habits; (2) preoperative MMSE [22], GDS [23] and PSQI; (3) laboratory tests including Hemoglobin, Albumin, white blood cell count (WBC), and C-reactive protein (CRP); (4) other clinical data including, type of operation, duration of surgery and anesthesia, the use of vasoactive drugs and dexmedetomidine (continuous intravenous infusion during surgery), and estimated blood loss, infusion volume (volume of crystalloids and colloids administered during surgery).
Statistical analysis
The sample size was estimated using PASS 15.0 software (NCSS, USA). According to the results of previous studies on sleep disorders and POD, the incidence of POD in patients with sleep disorders after non-cardiac surgery was 30-53% [24, 25]. The relative risk (RR) of POD in patients with sleep disorders was 3 times higher than that in patients without sleep disorders. Therefore, this study assumed that the incidence rate of POD in patients with preoperative sleep disorders after non-cardiac surgery was 40%, and the sample size was determined to be 112 cases according to the confidence level of 0.9 and the test level α value of 0.05. The expected postoperative loss of follow-up rate was 10%, and a total of 124 patients needed to be included.
Analysis of the data was performed using SPSS 26.0 statistical analysis software (IBM Corporation, Armonk, NY, USA), and the receiver operating characteristic (ROC) curve was plotted and the area under the ROC (AUROC) value calculated using GraphPad Prism (v8.0.1). Quantitative data were tested for normality firstly. Data with normal distribution were expressed as mean ± standard deviation, while data with non-normal distribution were expressed as median [interquartile range (IQR)], and statistical analysis was conducted by double-tail T-test or U test respectively. Classification data and grade data were expressed as cases or rates (%) and analyzed by Chi-square test or Fisher’s exact test. The relevant confounding factors with P value less than 0.1 were screened by univariate analysis, and corrected by multivariate logistic regression. The negative double logarithm likelihood ratio test was used to test the overall importance of the model, and the fit of the model was evaluated by the chi-square test of the Hosmer-Lemeshow fit. All the above results were statistically different when P < 0.05 was considered by bilateral test.
Results
Patient characteristics
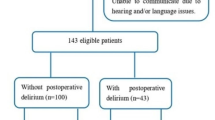
Initially, 161 patients aged 60 or older were screened for elective major non-cardiac surgery (Fig. 1). Of these, 21 patients were ineligible, and 6 patients declined to participate. In addition, 15 patients with compound exclusion criteria, and a total of 119 patients were finally followed up. POD occurred in 23 patients, accounting for 19.3%.
The mean age of participants was 71.2 ± 5.5 years, and 56 were males (47.1%). The demographic and baseline characteristics of all the patients are presented in Table 1.

Flow diagram of the study. Abbreviations MMSE Mini-Mental State Examination, GDS Geriatric Depression Scale, POD Postoperative delirium
Correlation analysis between subjective sleep quality and POD
Univariate and multivariate binary logistic regression analysis results for POD were shown in Table 2. Parameters with statistical difference P < 0.1 in univariate analysis of POD-related risk factors were selected as variables, that is, age, BMI, constipation, PSQI and operation time were included in multivariate logistic regression analysis. The results showed that the occurrence of POD was closely related to age, BMI, PSQI and operation time (P < 0.05). After adjusting for related factors, there was a statistically significant association between PSQI and POD occurrence (OR = 1.422, 95%CI 1.079–1.873, per 1-point increase in PSQI).
Prediction of subjective sleep quality on POD
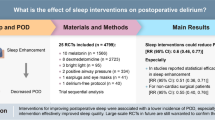
Multivariate logistic regression analysis results were used to develop a prediction model. The ROC curve analysis of PSQI and the model were shown in Fig. 2. It showed that the optimal PSQI cutoff value was 8 based on the Youden index for predicting POD. When using PSQI > 8, the AUROC of PSQI was 0.741 (95%CI 0.635 to 0.817) with a sensitivity and specificity of 56.5% and 86.5%, respectively. The AUROC of the model was 0.870 (95%CI 0.797 to 0.925), corresponding sensitivity and specificity were 97.7% and 65.6%. The results of the Hosmer-Lemeshow goodness-of-fit test (11.785, P = 0.161) indicated that the model had a prediction effect.

ROC curves of PSQI and the model. Abbreviations AUC area under the ROC curve. Model adjusted for age, BMI, constipation, PSQI and operative time
Discussion
POD is a great threat and challenge for those patients who undergo major surgery. As seen from previous studies [26,27,28], it occurs in 5-54% of patients after gastrointestinal surgery and total joint arthroplasty. It is possible that the wide variation in results can be explained by different study populations, as well as partly explained by delirium’s diagnostic approach [29]. The present study used CAM for diagnosis, which is the method used in most studies [30, 31], as well as Nu-DESC was used for screening to improve POD detection rates [32]. As a result of this study, 19.3% (23/119) of participants showed symptoms of POD.
In this study, subjective sleep quality was measured using the PSQI scale, which has become a widely used clinical sleep assessment scale worldwide due to its high reliability and validity [17]. It is indicative of worse sleep quality to have higher PSQI scores. One research indicates that sleep quality is poor if the score is greater than 5 [25]. The study showed that the optimal PSQI cutoff value was 8 based on the Youden index for predicting POD. It is therefore possible to provide better clinical guidance.
In the present study, preoperative subjective sleep quality was significantly associated with an increased risk of developing POD in patients undergoing major non-cardiac surgery. The results of relevant studies support this conclusion [33, 34]. Sleep disturbance was common during perioperative periods, and it adversely affected cognitive function after surgery [14]. We also found that patients had poorer sleep quality after surgery, but this did not seem to predict POD onset. This may be because there were many factors affecting sleep quality after surgery, and we didn’t interfere with them. Furthermore, sleeping disorders may be secondary symptoms of POD, but we did not exclude patients with sleeping disorders diagnosed during or after POD.
Meanwhile, the results showed that age, BMI and operation duration were independent risk factors for POD in our results of univariate analysis. After adjusting for the above factors by multivariate logistic regression, subjective sleep quality was still strongly associated with POD. Then, we developed a predictive model based on the independent risk factors above. The AUC for subjective sleep quality and the model were 0.741 and 0.870, respectively. Clearly, the model is more accurate when predicting POD. However, in clinical applications, sleep quality may be better for intervention due to age and BMI immutability, as well as the uncertainty of the operation time. Therefore, clinicians should pay more attention to evaluating patients’ sleep quality, and seek solutions to improve sleep quality for patients. Those may be beneficial in preventing postoperative delirium after major noncardiac surgery.
It is possible to improve poor sleep quality with non-pharmacological and pharmacological interventions. Sleep disruptions in intensive care units can be reduced through non-pharmacological sleep aids, such as soothing music, earplugs, and eye masks [35]. One meta-analysis revealed that melatonin, which is a hormone produced by the pineal gland, protects against delirium by improving sleep quality and treating inflammation in surgical and intensive care patients [36]. Su et al. demonstrated that the administration of a prophylactic low-dose infusion of dexmedetomidine, an α2 adrenergic receptor agonist, resulted in significantly reduced incidence of POD in post-surgical non-cardiac patients [37].
There were several limitations to this study. First, the study did not employ objective sleep quality tests. The gold standard for measuring sleep is polysomnography (PSG), but it is not applicable due to the particularity of perioperative patients [25]. Moreover, we were seeking a simple way to predict POD. Second, during the hospital stay before surgery, sleep status was not specifically measured. Due to the hospital environment and frequent interruptions, sleep quality in the hospital is usually poor. Third, due to sample size limitations, there is still a residual risk of confusion due to the lack of match with important baseline features in this study. In addition, only patients undergoing specific forms of surgery were included in this study, which was conducted at a single institution in a limited geographical region. Hence, further research on this topic is warranted in order to extend the generalizability of the findings.
Conclusions
In conclusion, our results revealed that preoperative subjective sleep quality was strongly associated with POD during major non-cardiac surgery. Additionally, PSQI combined with age, BMI and operation time improved POD prediction.
Data Availability
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ASA:
-
American society of anesthesiologists
- AUROC:
-
Area under the ROC
- BIS:
-
Bispectral index
- BMI:
-
Body mass index
- CAM:
-
Confusion assessment method
- CRP:
-
C-reactive protein
- GDS:
-
Geriatric depression scale
- IQR:
-
Interquartile Range
- MMSE:
-
Mini-mental state examination
- NU-DESC:
-
Nursing delirium screening checklist
- POD:
-
Postoperative delirium
- PSQI:
-
Pittsburgh sleep quality index
- ROC:
-
Receiver operating characteristic
- WBC:
-
White blood cell count
References
Jin Z, Hu J, Ma D. Postoperative delirium: perioperative assessment, risk reduction, and management[J]. Br J Anaesth. 2020;125(4):492–504.
Kirfel A, Guttenthaler V, Mayr A, et al. Postoperative delirium is an independent factor influencing the length of stay of elderly patients in the intensive care unit and in hospital[J]. J Anesth. 2022;36(3):341–8.
Lee SJ, Jung SH, Lee S, et al. Postoperative delirium after hip surgery is a potential risk factor for incident dementia: a systematic review and meta-analysis of prospective studies[J]. Arch Gerontol Geriatr. 2020;87:103977.
Shi Z, Mei X, Li C, et al. Postoperative delirium is Associated with Long-term decline in activities of daily Living[J]. Anesthesiology. 2019;131(3):492–500.
Flükiger J, Hollinger A, Speich B, et al. Dexmedetomidine in prevention and treatment of postoperative and intensive care unit delirium: a systematic review and meta-analysis[J]. Ann Intensiv Care, 2018;8(1).
Girard TD, Exline MC, Carson SS, et al. Haloperidol and Ziprasidone for treatment of Delirium in critical Illness[J]. N Engl J Med. 2018;379(26):2506–16.
Kim MS, Rhim HC, Park A, et al. Comparative efficacy and acceptability of pharmacological interventions for the treatment and prevention of delirium: a systematic review and network meta-analysis[J]. J Psychiatr Res. 2020;125:164–76.
Siddarth P, Thana-udom K, Ojha R, et al. Sleep quality, neurocognitive performance, and memory self-appraisal in middle-aged and older adults with memory complaints[J]. Int Psychogeriatr, 2020:1–11.
Lo JC, Groeger JA, Cheng GH, et al. Self-reported sleep duration and cognitive performance in older adults: a systematic review and meta-analysis[J]. Sleep Med. 2016;17:87–98.
Luo Z, Li L, Wang D, et al. Preoperative sleep quality affects postoperative pain and function after total joint arthroplasty: a prospective cohort study[J]. J Orthop Surg Res, 2019;14(1).
Su X, Wang D. Improve postoperative sleep[J]. Curr Opin Anaesthesiol. 2018;31(1):83–8.
Dolan R, Huh J, Tiwari N, et al. A prospective analysis of sleep deprivation and disturbance in surgical patients[J]. Annals of Medicine and Surgery. 2015;6:1–5.
Watson PL, Ceriana P, Fanfulla F. Delirium: Is sleep important?[J]. Best Pract Res Clin Anaesthesiol. 2012;26(3):355–66.
Wang X, Hua D, Tang X, et al. The role of Perioperative Sleep Disturbance in Postoperative Neurocognitive Disorders[J]. Nat Sci Sleep. 2021;13:1395–410.
Li Y, Huang H, Le Y. Risk factors and predictive value of perioperative neurocognitive disorders in elderly patients with gastrointestinal tumors[J]. BMC Anesthesiol, 2021;21(1).
Wagner S, Ahrens E, Wachtendorf LJ, et al. Association of Obstructive Sleep Apnea with postoperative delirium in procedures of moderate-to-high complexity: a Hospital-Registry Study[J]. Anesthesia & Analgesia, 2023, Publish Ahead of Print.
Buysse DJ, Reynolds CR, Monk TH, et al. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research[J]. Psychiatry Res. 1989;28(2):193–213.
Inouye SK, van Dyck CH, Alessi CA, et al. Clarifying confusion: the confusion assessment method. A new method for detection of delirium[J]. Ann Intern Med. 1990;113(12):941.
Evered L, Silbert B, Knopman DS, et al. Recommendations for the nomenclature of Cognitive Change Associated with Anaesthesia and Surgery-2018[J]. Anesthesiology. 2018;129(5):872–9.
Gaudreau J, Gagnon P, Harel F, et al. Fast, systematic, and continuous Delirium Assessment in Hospitalized Patients: the nursing delirium screening Scale[J]. J Pain Symptom Manag. 2005;29(4):368–75.
Winter A, Steurer M, Dullenkopf A. Postoperative delirium assessed by post anesthesia care unit staff utilizing the nursing delirium screening scale: a prospective observational study of 1000 patients in a single swiss institution[J]. BMC Anesthesiol, 2015;15(1).
Katzman R, Zhang MY, Ouang-Ya-Qu, et al. A chinese version of the Mini-Mental State examination; impact of illiteracy in a Shanghai dementia survey[J]. J Clin Epidemiol. 1988;41(10):971.
Zhang H, Wang S, Wang L, et al. Comparison of the geriatric depression Scale-15 and the Patient Health Questionnaire‐9 for screening depression in older adults[J]. Geriatrics & Gerontology International. 2020;20(2):138–43.
Cho M, Song S, Ryu C. Sleep disturbance strongly related to the development of postoperative delirium in proximal femoral fracture patients aged 60 or Older[J]. Hip & Pelvis. 2020;32(2):93.
Todd OM, Gelrich L, MacLullich AM, et al. Sleep disruption at Home as an independent risk factor for postoperative Delirium[J]. J Am Geriatr Soc. 2017;65(5):949–57.
Scholz AF, Oldroyd C, McCarthy K, et al. Systematic review and meta-analysis of risk factors for postoperative delirium among older patients undergoing gastrointestinal surgery[J]. Br J Surg. 2016;103(2):e21–8.
Bin Abd Razak HR, Yung WYA. Postoperative delirium in patients undergoing total joint arthroplasty: a systematic Review[J]. J Arthroplast. 2015;30(8):1414–7.
Neuman MD, Feng R, Carson JL, et al. Spinal anesthesia or General Anesthesia for hip surgery in older Adults[J]. N Engl J Med. 2021;385(22):2025–35.
Rong X, Ding Z, Yu H, et al. Risk factors of postoperative delirium in the knee and hip replacement patients: a systematic review and meta-analysis[J]. J Orthop Surg Res, 2021;16(1).
Li T, Li J, Yuan L, et al. Effect of Regional vs General Anesthesia on incidence of postoperative delirium in older patients undergoing hip fracture surgery: the RAGA Randomized Trial[J]. JAMA. 2022;327(1):50–8.
Wildes TS, Mickle AM, Ben Abdallah A, et al. Effect of Electroencephalography-Guided Anesthetic Administration on Postoperative Delirium among older adults undergoing major Surgery[J]. JAMA. 2019;321(5):473.
Kim S, Choi E, Jung Y, et al. Postoperative delirium screening tools for post-anaesthetic adult patients in non‐intensive care units: a systematic review and meta‐analysis[J]. Journal of Clinical Nursing; 2021.
Fadayomi AB, Ibala R, Bilotta F, et al. A systematic review and Meta-analysis examining the impact of Sleep disturbance on postoperative Delirium[J]. Crit Care Med. 2018;46(12):e1204–12.
Wang H, Zhang L, Zhang Z, et al. Perioperative Sleep Disturbances and postoperative delirium in adult patients: a systematic review and Meta-analysis of clinical Trials[J]. Front Psychiatry, 2020;11.
Kamdar BB, King LM, Collop NA, et al. The Effect of a quality improvement intervention on Perceived Sleep Quality and Cognition in a medical ICU[J]. Crit Care Med. 2013;41(3):800–9.
Khaing K, Nair BR. Melatonin for delirium prevention in hospitalized patients: a systematic review and meta-analysis[J]. J Psychiatr Res. 2021;133:181–90.
Su X, Meng Z, Wu X, et al. Dexmedetomidine for prevention of delirium in elderly patients after non-cardiac surgery: a randomised, double-blind, placebo-controlled trial[J]. The Lancet. 2016;388(10054):1893–902.
Acknowledgements
The authors thank the nursing staff of the Ningbo No.2 Hospital, China.
Funding
This study was supported by grants of the Medical Scientific Research Foundation of Zhejiang Province, China (No. 2018KY693, 2020KY260, 2021KY286, 2022KY327, 2022KY1139), Ningbo Natural Science Foundation, China (No. 2019A610291) and Ningbo Leading Medical & Health Discipline (No.2022-B10).
Author information
Authors and Affiliations
Contributions
Jinwei Zheng: patient recruitment, study material preparation and writing up draft of the paper. Lulu Wang and Wei Wang: patient recruitment and data collection. Huafeng Zhang: data analysis and interpretation. Fangfang Yao: data collection. Junping Chen: designed the study and submitted the manuscript. Qingxiu Wang: designed the study and supervision. All authors have read and approved the manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study followed the Declaration of Helsinki. It was a prospective study, approved by the ethics committee of Ningbo No.2 Hospital (approval number: PJ-NBEY-KY-2017-029-01), and registered in the China Clinical Trial Center (www.chictr.org.cn; ID: ChiCTR-OOC-17013414). Before surgery, the patients or their family members provided written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zheng, J., Wang, L., Wang, W. et al. Association and prediction of subjective sleep quality and postoperative delirium during major non-cardiac surgery: a prospective observational study. BMC Anesthesiol 23, 306 (2023). https://doi.org/10.1186/s12871-023-02267-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12871-023-02267-x