
Abstract
Background
The Centers for Disease Control and Prevention’s (CDC) March 2016 opioid prescribing guideline did not include prescribing recommendations for surgical pain. Although opioid over-prescription for surgical patients has been well-documented, the potential effects of the CDC guideline on providers’ opioid prescribing practices for surgical patients in the United States remains unclear.
Methods
We conducted an interrupted time series analysis (ITSA) of 37,009 opioid-naïve adult patients undergoing inpatient surgery from 2013–2019 at an academic medical center. We assessed quarterly changes in the discharge opioid prescription days’ supply, daily and total doses in oral morphine milligram equivalents (OME), and the proportion of patients requiring opioid refills within 30 days of discharge.
Results
The discharge opioid prescription declined by -0.021 (95% CI, -0.045 to 0.003) days per quarter pre-guideline versus -0.201 (95% CI, -0.223 to -0.179) days per quarter post-guideline (p < 0.0001). Likewise, the mean daily and total doses of the discharge opioid prescription declined by -0.387 (95% CI, -0.661 to -0.112) and -7.124 (95% CI, -9.287 to -4.962) OME per quarter pre-guideline versus -2.307 (95% CI, -2.560 to -2.055) and -20.68 (95% CI, -22.66 to -18.69) OME per quarter post-guideline, respectively (p < 0.0001). Opioid refill prescription rates remained unchanged from baseline.
Conclusions
The release of the CDC opioid guideline was associated with a significant reduction in discharge opioid prescriptions without a concomitant increase in the proportion of surgical patients requiring refills within 30 days. The mean prescription for opioid-naïve surgical patients decreased to less than 3 days’ supply and less than 50 OME per day by 2019.
Similar content being viewed by others


Introduction
Post-surgical prescriptions are a major source of hospital opioid prescriptions at discharge [1]. In the United States, opioids are often over-prescribed to patients after surgical procedures [2,3,4,5,6,7,8]. As a result, excess opioids can be a potential source for overdose, misuse, diversion, and new persistent opioid use among surgical patients [8,9,10,11,12,13,14]. There is a general consensus among medical providers that postoperative opioid prescriptions should be optimized to balance the provision of effective postoperative pain control and the risk of opioid-related adverse effects [9,10,11].
In response to the opioid prescription epidemic, the Centers for Disease Control and Prevention (CDC) of the United States published the Guideline for Prescribing Opioids for Chronic Painin March 2016 to improve the safety and effectiveness of pain treatment and to reduce the risks of opioid use disorder, overdose, and death [12]. The guideline recommended prescribing up to three days’ supply for patients with non-surgical acute pain, and suggested a careful assessment of risks and benefits when the prescribed dose exceeds 50 oral morphine milligram equivalents (OME) per day [12]. Significant improvements in opioid prescribing practices in non-surgical patients have been observed after the release of 2016 CDC guideline [13].
It is important to note that the CDC guideline was not intended to address postoperative opioid prescribing [12], and the CDC has not yet developed a formal guideline to address opioid prescribing in postoperative patients. Sutherland et al. recently analyzed a private insurance database for patients undergoing 8 common surgical procedures and found an association of decreased opioid dispensing after the CDC guideline in opioid naïve surgical patients, which highlights the potential influence of these guidelines in the surgical setting [14]. However, this study focused on opioids that were filled by patients but did not include data on the opioid prescriptions that were written by providers [14]. Prior studies have found that up to 21% of opioids remain unfilled after surgery [4]. Therefore, it remains unclear if the trends they observed were the result of patients’ decision to fill less postsurgical opioid prescriptions, or the result of providers changing their opioid prescribing practices change after the CDC guideline.
To investigate the potential effect of 2016 CDC guideline on provider level opioid prescribing practice, we assessed the opioid prescribing practices for surgical patients upon discharge at a large academic medical center in California between 2013 and 2019 with interrupted time series analysis. We examined trends in the days’ supply, total and daily dose of the discharge opioid prescription, and 30-day opioid refill prescriptions written for opioid-naïve patients undergoing all inpatient surgical procedures.
Materials and methods
Study design and data source
We conducted an interrupted time series analysis (ITSA) of adult opioid-naïve patients undergoing inpatient surgery from January 2013 through December 2019 at University of California San Francisco Medical Center. Study data were derived from the electronic medical record (EMR) system (Epic Systems, Verona, WI). This study was approved by the IRB at our institution, which waived patient consent for acquisition of data (IRB# 18–26,728).
After extraction from an electronic data warehouse, the data were validated for accuracy with iterative chart auditing. To ensure accurate and complete data extraction, data reports were evaluated to identify inconsistencies, missingness, extreme values, and invalid codes. Discrepancy management included reviewing discrepancies, investigating the reason, and resolving them. The data extracted had no missingness. After a proper quality check and assurance, the final dataset was locked so that the dataset could not be modified and only the final clean dataset was used for analysis.
Study cohort
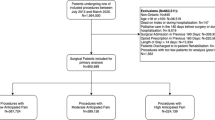
Our study included all opioid-naïve patients aged 18 years and older who underwent any surgery requiring a post-operative inpatient stay of at least 24 h after leaving the post-anesthesia care unit (PACU), and who were discharged to either home, a skilled nursing facility or rehabilitation facility. If a patient had multiple surgical procedures during the same surgical admission, we used the first surgical procedure as the index procedure for that admission. If a patient had additional procedures during the study period during subsequent hospitalizations, we categorized those subsequent hospitalizations as new patient encounters. We excluded patients discharged to other acute level care sites and hospice. We defined opioid-naïve as any patients without opioids listed on their medication list at the time of admission and without an active opioid prescription documented in their EMR starting six months prior to the date of surgery. Patients were stratified based on whether they underwent surgery before or after the release of the March 2016 CDC opioid guideline. Hence, patients who underwent surgery between the 1st quarter of 2013 to the 1st quarter of 2016 were included in the pre-guideline group and patients who underwent surgery between the 2nd quarter of 2016 to the 4th quarter of 2019 were included in the post-guideline group.
Opioid dose calculation
The opioid dosage on the discharge opioid prescription was converted into OMEs using standard opioid conversion ratios [15]. The daily dose on the discharge opioid prescription was defined as the maximum allowable dose in a 24-h period according to the written prescription. Whenever more than one prescription was prescribed to the patient at hospital discharge, the daily OME and total OME on the opioid discharge prescription were calculated as the sum of all written opioid prescriptions. Opioid dose reflects the dose that was prescribed by providers at discharge and not what was filled by patients. Opioid refill prescriptions were defined as opioid prescriptions written after the discharge opioid prescription between 1 and 30 days after hospital discharge.
Statistical analysis
We used descriptive statistics to compare baseline differences in patient characteristics in the.
pre- and post- guideline groups. The mean days’ supply, mean daily OME, and mean total OME at discharge, and the percentage of patients who required opioid refill prescriptions within 30 days of hospital discharge were assessed quarterly. Data were analyzed by segmental linear regression with least squares regression (Prism 9.0) as an interrupted time series analysis (ITSA). We reported the slopes and their 95% confident intervals (CI) before and after the CDC opioid guideline was released, as well as the p-values to determine the model as segmental linear regression or as simple linear regression of a straight line. Additional detail about the ITSA can be found in the Supplemental Material 1.
The differences between the 1st quarter of 2016 and the last quarter of 2019 in day’s supply, daily and total doses were analyzed with unpaired two-tailed t test. The differences between the 1st quarter of 2016 and the last quarter of 2019 in percentage of patients receiving more than 3 days’ supply or more than 50 OME per day, and the percentage of patients requiring opioid refill prescriptions within 30 days of discharge were analyzed with two-tailed Chi-square test. Both analyses were conducted with Prism 9.0.
Results
A total of 37,009 opioid naïve patients undergoing any inpatient surgical procedures met inclusion criteria. There were 15,288 patients in the pre-guideline group, and 21,721 patients in the post-guideline group. Patient characteristics were similar between two groups on age, gender, race, length of stay, and mental health disorders (Table 1). There was no significant change in postsurgical hospital stay before or after the guideline. The proportion of surgical volume by service was similar between pre- and post-guideline, with the exception of obstetrics and gynecology due to the expansion of our women and children’s hospital in 2015 (Table 1).
Trend change in days’ supply of postoperative discharge opioid prescriptions after CDC guideline
The quarterly change in the mean days’ supply on the discharge opioid prescription was -0.021 days per quarter in the pre-guideline period (95% CI, -0.045 to 0.003) (Fig. 1a). In the post-guideline period, the trend changed significantly, with a quarterly change in mean days’ supply of -0.201 (95% CI, -0.223 to -0.179, p < 0.0001). Overall, the mean days’ supply decreased by 49.5%, from 5.64 ± 0.14 days in the 1st quarter of 2016 to 2.85 ± 0.09 days in the last quarter of 2019 (p < 0.0001).

Duration of postoperative discharge opioid prescription, 2013–2019. a Mean duration of the discharge opioid prescription for postoperative patients before and after the release of the CDC opioid guideline. Data are presented as the mean days’ supply on the discharge opioid prescription in quarterly intervals from the 1st quarter of 2013 through the 4th quarter of 2019. The vertical line represents the first quarter after the release of the CDC opioid guideline in March 2016. By the 3rd quarter of 2019, the mean duration of the postoperative discharge opioid prescription had decreased to less than 3 days. b Proportion of postoperative patients receiving a discharge opioid prescription with greater than 3 days’ supply before and after the release of the CDC opioid guideline. Data are presented as the percentage of postoperative patients receiving a discharge opioid prescription with greater than 3 days’ supply in quarterly intervals from the 1st quarter of 2013 through the 4th quarter of 2019. The vertical line represents the first quarter after the release of the CDC guideline in March 2016. By the 4th quarter of 2018, the proportion of postoperative patients receiving a discharge opioid prescription with greater than 3 days’ supply had decreased to less than 50%. Dc = discharge; Rx = prescription, 3d = 3 days, and CI = confidence interval
In the pre-guideline period, the proportion of patients who received a discharge opioid prescription of greater than 3 days’ supply increased by 0.260 percentage points per quarter (95% CI, 0.049% to 0.470%) (Fig. 1b). In the post-guideline period, the trend changed significantly, decreasing by 2.485 percentage points per quarter (95% CI, -2.678% to -2.292%, p < 0.0001). Overall, the proportion of patients who received a discharge opioid prescription of greater than 3 days’ supply decreased by 45.3%, from 72.8% in the 1st quarter of 2016 to less than 39.8% in the last quarter of 2019 (p < 0.0001).
Trend change in daily dose of postoperative discharge opioid prescriptions after CDC guideline
The mean daily dose prescribed pre-guideline decreased by 0.387 OME per quarter (95% CI, -0.661 to -0.112) (Fig. 2a). Post-guideline, there was a significant change in the trend of mean daily dose prescribed by 2.307 OME per quarter (95% CI, -2.560 to -2.055, p < 0.0001). Overall, the mean daily dose prescribed for patients decreased by 46.5%, from 77.18 ± 3.17 OME in the 1st quarter of 2016 to 41.28 ± 1.16 OME in the last quarter of 2019 (p < 0.0001).

Daily dose on the postoperative discharge opioid prescription, 2013–2019. a Mean daily dose prescribed on the postoperative discharge opioid prescription before and after the release of the CDC opioid guideline. Data are presented as the mean daily dose prescribed on the postoperative discharge opioid prescription in quarterly intervals from the 1st quarter of 2013 through the 4th quarter of 2019. The vertical line represents the first quarter after the release of the CDC guideline in March 2016. By the 1st quarter of 2019, the mean daily dose on the postoperative discharge prescription had decreased to less than 50 OME. b Proportion of postoperative patients receiving a discharge opioid prescription with greater than 50 OME per day before and after release of the CDC opioid guideline. Data are presented as the percentage of postoperative patients receiving a postoperative discharge opioid prescription with a daily dose greater than 50 OME in quarterly intervals from the 1st quarter of 2013 through the 4th quarter of 2019. The vertical line represents the first quarter after the release of the CDC guideline in March 2016. By the 2nd quarter of 2018, the proportion of postoperative patients receiving a discharge opioid prescription with greater than 50 daily OME had decreased to less than 50%. Dc = discharge; Rx = prescription, and CI = confidence interval
The proportion of patients with a daily dose of discharge opioid prescription greater than 50 OME decreased by 0.413 percentage points per quarter (95% CI, -0.768% to -0.057%) (Fig. 2b). Post-guideline, the trend changed significantly, decreasing by 1.814 percentage points per quarter (95% CI, -2.141 to -1.488%, p < 0.0001). Overall, the percentage of patients with a discharge opioid prescription greater than 50 OME per day decreased by 45.0%, from 57.0% in the 1st quarter of 2016 to 31.4% in the last quarter of 2019 (p < 0.0001).
Trend change in total dose of postoperative discharge opioid prescriptions after CDC guideline
The mean total dose prescribed pre-guideline decreased by 7.124 OME per quarter (95% CI, -9.287 to -4.962) (Fig. 3). There was a significant trend change in the post-guideline period, with a decrease of 20.68 OME per quarter (95% CI, -22.66 to -18.69, p < 0.0001). Overall, the total dose prescribed for patients decreased 63.7%, from 474.61 ± 18.96 OME in the 1st quarter of 2016 to 175.27 ± 7.54 OME in the last quarter of 2019 (p < 0.0001).

Total dose prescribed on the postoperative discharge opioid prescription, 2013–2019. Mean total dose prescribed on the postoperative discharge opioid prescription before and after the release of the CDC opioid guideline. Data are presented as the mean total dose prescribed on the postoperative discharge opioid prescriptions in quarterly intervals from the 1st quarter of 2013 through the 4th quarter of 2019. The vertical line represents the first quarter after the release of the CDC guideline in March 2016. Dc = discharge; Rx = prescription, and CI = confidence interval
Trend change in 30-day postoperative opioid refills after CDC guideline
Opioid refill prescriptions within 30 days of discharge remained stable throughout the study, with no statistically significant change in quarterly refill trends (-0.040 percentage points per quarter, 95% CI, -0.179 to 0.098 pre-guideline versus 0.064 percentage points per quarter, 95% CI, -0.063 to 0.191 post-guideline, p = 0.372) or in the proportion of patients receiving a refill prescription (16.41% in the 1st quarter of 2016 versus 16.65% in the last quarter of 2019, p = 0.865) (Fig. 4).

Proportion of postoperative patients receiving an opioid refill prescription within 30 days of discharge, 2013–2019. Proportion of postoperative patients receiving an opioid refill prescription within 30 days of discharge before and after the release of the 2016 CDC opioid guideline. Data are presented as the percentage of postoperative patients receiving an opioid refill prescription within 30 days of discharge in quarterly intervals from the 1st quarter of 2013 through the 4th quarter of 2019. The vertical line represents the first quarter after the release of the CDC guideline in March 2016. Rx = prescription, and CI = confidence interval
Sensitivity analysis
Due to the change in volume of obstetrics and gynecology procedures at our institution during the study period, we performed the same ITSA analyses on our obstetrics and gynecology cases, the results of which did not differ from overall trends (not shown).
Discussion
In this interrupted time series analysis, we found that the publication of the 2016 CDC opioid guideline was associated with significant trend changes in opioid prescribing practices for postsurgical patients. By assessing the association of provider prescribing practices with CDC guideline release, our study adds additional perspective to prior work that focused primarily on opioids filled by surgical patients after CDC guideline release [14, 16]. Specifically, we identified significant decreases in the day’s supply, daily dose, and total dose of opioid prescriptions written at discharge. Compared to the 1st quarter of 2016 when the CDC guideline was released, the mean days’ supply, mean daily dose and mean total dose on the discharge opioid prescription decreased by 49.5%, 46.5%, and 63.7%, respectively, by the 4th quarter of 2019.
The CDC guideline recommends prescribing up to three days’ supply for acute non-surgical pain indications and a starting daily dose of less than 50 OME to reduce the risk of fatal overdose or other opioid-related adverse effects, including the risk of transitioning to chronic opioid use [12]. Although the CDC guideline does not apply to surgical patients [12], we found that the mean days’ supply had decreased to less than 3 days by the 3rd quarter of 2019, and the mean daily dose had decreased to less than 50 OME by the 1st quarter of 2019 at our institution, a tertiary care hospital performing complex surgical procedures in patients with a range of comorbid conditions.
Importantly, despite the significant decreases in the OME and days’ supply of the discharge opioid prescriptions for surgical patients after the release of the 2016 CDC guideline, the percentage of patients requiring opioid refill prescriptions within 30 days of discharge did not change when compared with the pre-guideline period. This suggests that the significant reduction in the discharge opioid prescription did not result in insufficient opioid coverage for surgical patients. Our findings are consistent with previous reports that the probability of having an opioid refill within 30 days after surgery was not correlated with the dosage of the discharge opioid prescription [17], and that reducing the amount of opioid on the discharge prescription did not compromise post-operative pain control or patients’ satisfaction [16, 18,19,20].
Although our results suggest that the 2016 CDC’s opioid guideline of less than 3 days’ supply and less than 50 daily OME might be applied to opioid prescriptions for certain surgical patients, we caution against extrapolating the CDC guideline to all surgical settings. While the mean daily dose and the mean days’ supply did fall below the CDC recommendations by 2019, there was still a wide range of discharge daily doses and days’ supply represented in our study. For example, by the end of 2019, 39.8% of discharge opioid prescriptions still exceeded a 3-day supply, and 31.4% of prescriptions had a daily dose of greater than 50 OME. It has been previously reported that the dosage of the discharge opioid prescription closely correlates with surgical complexity, and the opioid requirement for patients after different types of surgical procedures can vary [21, 22]. In addition, setting a simple limit for opioid prescriptions to surgical patients without the ability to individualize the dosage has been shown to be problematic [23]. A better approach might be to evaluate pre-discharge inpatient opioid consumption to guide the opioid prescription at discharge [24, 25]. Additional studies will be needed to determine the appropriate indications for applying the current CDC opioid guideline to the discharge opioid prescription to surgical patients. Further studies will also be needed to follow the trend of opioid prescriptions for surgical patients after 2019 to determine the appropriate range of dose and duration without increasing opioid refill prescriptions.
Our study was conducted during a time of increasing evidence of harm associated with unsafe opioid prescribing practices, the introduction of DEA rescheduling of hydrocodone containing drugs, and the introduction of institutional opioid prescribing initiatives, which could have contributed to safer opioid prescribing practices. While California, where our study is located, did not pass state-specific legislation to limit opioid prescriptions during the study period, the state did update its prescription drug monitoring programs (PDMP) policy in July 2016 requiring mandatory registration of opioid prescribers, when previously this had been voluntary [26]. As an institution, surgery specific care protocols like enhanced recovery after surgery (ERAS) were adopted both before and after the 2016 CDC guideline was released, some of which included guidance on appropriate dosing of opioid prescriptions at discharge. Nevertheless, ERAS initiatives were introduced over multiple years, both before and after the March 2016 CDC guideline release rather than being implemented at a single point in time. These opioid-related initiatives could have directly or indirectly impacted our institution’s overall opioid prescribing trends. Regardless, we found a statistically significant accelerated rate of decline in several key opioid prescribing indicators after March 2016. Given the March 2016 inflection point, these findings suggest that the release of the CDC guideline may explain the changes in the opioid prescriptions written for surgical patients at our institution.
This study has some limitations. The study was conducted at a single academic medical center in opioid-naïve surgical patients requiring an inpatient post-operative stay. Therefore, our findings may not be representative of prescribing practices at non-academic hospitals, among patients undergoing outpatient surgeries, or among patients who used opioids prior to admission. In addition, since our study was an analysis assessing discharge opioid prescriptions across all inpatient procedures at our academic medical center, the results may not reflect the trends of individual surgical subspecialties or surgical procedures; analysis of these individual surgical subspecialty trends is currently underway. Furthermore, because we did not analyze post-discharge pain scores, despite the lack of change in the rate of postoperative opioid refills, we cannot definitively state that patients’ postoperative pain remained unchanged during the study period. However, while insurance databases provide data on prescriptions filled, they do not include opioid prescriptions written by the provider. Therefore, analyzing institutional EMR data provides a reliable way to obtain information about opioid prescribing practices on a provider-level and can be used to detect changes in physician practice patterns in response to new guidelines.
In conclusion, we found that the release of the 2016 CDC opioid guideline was associated with a significant reduction in discharge opioid prescriptions without a concomitant increase in opioid refills within 30 days of discharge for surgical patients. By 2019, the mean postsurgical opioid prescription decreased to less than 3 days’ supply and less than 50 OME per day in our medical center.
Availability of data and materials
Raw large scale electronic medical record data were generated at our institution. The raw electronic medical record data were generated at our institution at the point of care during the usual course of providing healthcare and the data was de-identified prior to making it available for research. The datasets generated and analyzed during the current study are not publicly available because some of the covariates that were made available to the research team are still classified as protected health information by our IRB. Datasets can be made available from the corresponding author on reasonable request.
Abbreviations
- OME:
-
Oral morphine equivalents
- CDC:
-
Centers for Disease Control
- EMR:
-
Electronic medical record
- ITSA:
-
Interrupted time series analysis
References
Calcaterra SL, Yamashita TE, Min SJ, Keniston A, Frank JW, Binswanger IA. Opioid Prescribing at Hospital Discharge Contributes to Chronic Opioid Use. J Gen Intern Med. 2016;31:478–85.
Baker JA, Avorn J, Levin R, Bateman BT. Opioid Prescribing After Surgical Extraction of Teeth in Medicaid Patients, 2000–2010. JAMA. 2016;315:1653–4.
Wunsch H, Wijeysundera DN, Passarella MA, Neuman MD. Opioids Prescribed After Low-Risk Surgical Procedures in the United States, 2004–2012. JAMA. 2016;315:1654–7.
Bicket MC, Long JJ, Pronovost PJ, Alexander GC, Wu CL. Prescription Opioid Analgesics Commonly Unused After Surgery: A Systematic Review. JAMA Surg. 2017;152:1066–71.
Brummett CM, Steiger R, Englesbe M, Khalsa C, DeBlanc JJ, Denton LR, Waljee J. Effect of an Activated Charcoal Bag on Disposal of Unused Opioids After an Outpatient Surgical Procedure: A Randomized Clinical Trial. JAMA Surg. 2019;154:558–61.
Harris K, Curtis J, Larsen B, Calder S, Duffy K, Bowen G, Hadley M, Tristani-Firouzi P. Opioid pain medication use after dermatologic surgery: a prospective observational study of 212 dermatologic surgery patients. JAMA Dermatol. 2013;149:317–21.
Howard R, Fry B, Gunaseelan V, Lee J, Waljee J, Brummett C, Campbell D Jr, Seese E, Englesbe M, Vu J. Association of Opioid Prescribing With Opioid Consumption After Surgery in Michigan. JAMA Surg. 2019;154:e184234.
Ladha KS, Neuman MD, Broms G, Bethell J, Bateman BT, Wijeysundera DN, Bell M, Hallqvist L, Svensson T, Newcomb CW, Brensinger CM, Gaskins LJ, Wunsch H. Opioid Prescribing After Surgery in the United States, Canada, and Sweden. JAMA Netw Open. 2019;2:e1910734.
Waljee JF, Li L, Brummett CM, Englesbe MJ. Iatrogenic Opioid Dependence in the United States: Are Surgeons the Gatekeepers? Ann Surg. 2017;265:728–30.
Hollmann MW, Rathmell JP, Lirk P. Optimal postoperative pain management: redefining the role for opioids. Lancet. 2019;393:1483–5.
Neuman MD, Bateman BT, Wunsch H. Inappropriate opioid prescription after surgery. Lancet. 2019;393:1547–57.
Dowell D, Haegerich TM, Chou R. CDC Guideline for Prescribing Opioids for Chronic Pain - United States, 2016. MMWR Recomm Rep. 2016;65:1–49.
Bohnert ASB, Guy GP Jr, Losby JL. Opioid Prescribing in the United States Before and After the Centers for Disease Control and Prevention’s 2016 Opioid Guideline. Ann Intern Med. 2018;169:367–75.
Sutherland TN, Wunsch H, Pinto R, Newcomb C, Brensinger C, Gaskins L, Bateman BT, Neuman MD. Association of the 2016 US Centers for Disease Control and Prevention Opioid Prescribing Guideline With Changes in Opioid Dispensing After Surgery. JAMA Netw Open. 2021;4:e2111826.
Naidu RS, Schumacher M. UCSF OPIOID EQUIVALENCE TABLE. 2015. (https://cdn-links.lww.com/permalink/aln/b/aln_2018_05_23_behrends_aln-d-17-01295r2_sdc1.pdf).
Mark J, Argentieri DM, Gutierrez CA, Morrell K, Eng K, Hutson AD, Mayor P, Szender JB, Starbuck K, Lynam S, Blum B, Akers S, Lele S, Paragh G, Odunsi K, de Leon-Casasola O, Frederick PJ, Zsiros E. Ultrarestrictive Opioid Prescription Protocol for Pain Management After Gynecologic and Abdominal Surgery. JAMA Netw Open. 2018;1:e185452.
Sekhri S, Arora NS, Cottrell H, Baerg T, Duncan A, Hu HM, Englesbe MJ, Brummett C, Waljee JF. Probability of Opioid Prescription Refilling After Surgery: Does Initial Prescription Dose Matter? Ann Surg. 2018;268:271–6.
Louie CE, Kelly JL, Barth RJ Jr. Association of Decreased Postsurgical Opioid Prescribing With Patients’ Satisfaction With Surgeons. JAMA Surg. 2019;154:1049–54.
Woodward MA, Zhang Y, Tannen B, Behunin N, Niziol LM, Waljee J. Association of Limiting Opioid Prescriptions With Use of Opioids After Corneal Surgery. JAMA Ophthalmol. 2020;138(1):76–80.
Howard R, Vu J, Lee J, Brummett C, Englesbe M, Waljee J. A Pathway for Developing Postoperative Opioid Prescribing Best Practices. Ann Surg. 2020;271:86–93.
Cho HE, Hu HM, Gunaseelan V, Chen JS, Englesbe MJ, Chung KC, Waljee JF: Does Surgical Intensity Correlate With Opioid Prescribing?: Classifying Common Surgical Procedures. Ann Surg 2020
Hill MV, McMahon ML, Stucke RS, Barth RJ Jr. Wide Variation and Excessive Dosage of Opioid Prescriptions for Common General Surgical Procedures. Ann Surg. 2017;265:709–14.
Chua KP, Brummett CM, Waljee JF. Opioid Prescribing Limits for Acute Pain: Potential Problems With Design and Implementation. JAMA. 2019;321:643–4.
Day RW, Newhook TE, Dewhurst WL, Arvide EM, Bruno ML, Vauthey JN, Tzeng CD. Assessing the 5x-Multiplier Calculation to Reduce Discharge Opioid Prescription Volumes After Inpatient Surgery. JAMA Surg. 2020;155(12):1166–7.
Porter ED, Bessen SY, Molloy IB, Kelly JL, Ramkumar N, Phillips JD, Loehrer AP, Wilson MZ, Hasson RM, Ivatury SJ, Henkin JR, Barth RJ Jr. Guidelines for Patient-CenteredOpioid Prescribing and Optimal FDA-Compliant Disposal of Excess Pills after Inpatient Operation: Prospective Clinical Trial. J Am Coll Surg. 2021;232:823-835 e2.
Castillo-Carniglia A, González-Santa Cruz A, Cerdá M, et al. Changes in opioid prescribing after implementation of mandatory registration and proactive reports within California’s prescription drug monitoring program. Drug Alcohol Depend. 2021;218:108405. https://doi.org/10.1016/j.drugalcdep.2020.108405 (published correction appears in Drug Alcohol Depend. 2021 Apr 1;221:108606).
Bernal JL, Cummins S, Gasparrini A. Interrupted time series regression for the evaluation of public health interventions: a tutorial. Int J Epidemiol. 2017;46:348–55.
Acknowledgements
We thank the editor and reviewers for their insightful suggestions.
Conflicts of interest
None to disclose.
Funding
None to disclose.
Author information
Authors and Affiliations
Contributions
E.L. designed the study, acquired, analyzed, and interpreted the data, wrote, and revised the manuscript. A.B. analyzed and interpreted the data and revised the manuscript. R.C. analyzed and interpreted the data. R.R. analyzed and interpreted the data and revised the manuscript. E.C.W. revised the manuscript. C.C. designed the study, analyzed, and interpreted the data, wrote, and revised the manuscript. Z.G. designed the study, analyzed, and interpreted the data, wrote and revised the manuscript. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the UCSF IRB, which waived patient consent for acquisition of data (IRB# 18–26728). Methods for data collection, management, and storage were carried out in accordance with IRB regulation.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: FigureS1.
Interrupted time series analysis with modeltesting beta 2 intercept. SupplementalMaterial 1. Interrupted Time Series Analysis [27].
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Langnas, E., Bishara, A., Croci, R. et al. Opioid prescribing practices at hospital discharge for surgical patients before and after the Centers for Disease Control and Prevention’s 2016 opioid prescribing guideline. BMC Anesthesiol 22, 141 (2022). https://doi.org/10.1186/s12871-022-01678-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12871-022-01678-6