
Abstract
Background
In Burkina Faso, demographics are changing and we are seeing a growing prevalence of older patients in intensive care units. Elderly people have increased health care needs but there is a lack of geriatric specialists. This study aimed to analyze in-hospital outcome of patients aged over 65 years, admitted to the Intensive Care Unit (ICU) at Yalgado Hospital.
Methods
We carried out a 5-year retrospective study in the ICU of Yalgado Ouédraogo Hospital. Elderly patients with completed records were included. Baseline characteristics, clinical and outcome were analyzed.
Results
Two thousand one hundred sixteen patients were admitted to ICU, 237 (11.2%) of whom were included. There were 70 females and 167 males. The median age was 71.7 ± 6.1 years. The overall mortality rate in ICU was 73%, of whom 90% died within 7 days after admission. In multivariate analysis, shock (Odds Ratio: OR = 2.2, p = 0.002), severe brain trauma (OR; 9.6, p = 0.002), coma (OR 5.8 p < 0.003), surgical condition (OR = 4.2, p = 0.003), ASAPS Score ≥ 8 (OR = 4.3, p = 0.001), complication occurring (OR = 5.2, p = 0.001) and stroke (OR = 3.7, p = 0.001) were independent factors.
Conclusion
Elderly patients were frequent in ICU and their mortality rate was high. Stroke, severe brain trauma, surgery, complications occurring during hospitalization were independent risk factors of death.
Similar content being viewed by others


Background
Elderly is defined as a chronological age equal to or above 65 years worldwide or above 60 years in Africa [1]. Worldwide, the elderly population continues to grow due to increased life expectancy [2]. In 2015, the world elderly population rose by 55 million and the proportion reached 8.5% [3]. In Africa, the proportion of elderly accounted for 6.6% in 2015 and will reach 9.6% in 2050. This increase is also seen in Burkina Faso. In 1985, the census in Burkina Faso reported 319,496 elderly people accounting for 4% of the general population. [4] This rose to 475,812 (2.4%) in 2016 [5]. Despite the increase of the number of elderly people in Burkina Faso, their proportion is reduced by the explosion of births and the youth of the population. One of the consequences of the growth in the number of elderly patients is the increased requirement for admission to ICU. They require appropriate healthcare facilities, and special skills and human resources. They have higher morbidity and mortality because of associated co-morbidities. In developing countries, intensive care is limited by poverty, lack of equipment, inadequate skills and insufficient human resources. This study aims to assess outcomes for elderly patients admitted to ICU in the first referral teaching hospital Yalgado Ouédraogo in Burkina Faso.
Methods
We carried out a retrospective study of elderly patients admitted to the ICU of the tertiary Hospital Yalgado Ouédraogo over a five-year period (1st January, 2011 to 31st December, 2015). Yalgado Hospital is a tertiary care, governmental hospital, with an overall capacity of 800 beds and an 8 bed ICU where patients are managed by anesthesiologists. The average number of admissions to ICU was about 200 patients per year with a mortality of 51.6% [6]. The ICU is poorly equipped (one transport ventilator, one defibrillator and monitors). Patients receive fluid and electrolyte management, transfusions, oxygen, vasoactive drugs, and nutrition (parenteral and oral nutrition). Non-invasive ventilation and CPAP were not used. Relevant data recorded includes socio-demographic characteristics, co-morbidities, diagnosis, indications for ICU admission, Glasgow Coma Score at admission, the Ambulatory Simplified Acute Physiologic Score (ASAPS) [7], Charlson co-morbidity score, need for mechanical ventilation, blood transfusion and or hemodialysis, sepsis, shock on admission, length of stay and outcome. The Ambulatory Simplified Acute Physiologic Score is a scale used for patients admitted to ICU to evaluate the severity of their condition.
Ethical and National Scientific Research and Technology Center (ENSRTC) approved the study. The Epidemiologic Information package version 7.1.5.0 was used for data analysis. Descriptive statistics included frequency for nominal variables and mean ± standard deviations or medians and interquartile ranges for continuous variables according to their distribution. Independent t-test (continuous variables) and Chi-square test (categorical variables) were used in univariate analysis when comparing age groups, survivors to non-survival patients. A p value ≤0.05 was considered as significant. The total sample was divided into three groups according to age (65–74 years or « young old », 75–84 years or old old, and > 85 years or oldest old).
Results
In total, 2116 patients were admitted to ICU of whom 237 (11.2%) were included in our study. The mean age was 71.7 ± 6.1 years, with male: female ratio of 2.3. The demographic characteristics are summarized in Table 1.
Comorbidity was identified in 191 cases (80.6%) of which 49.4% (n = 117) had more than 2 comorbidities and 19.4% (n = 46) had none. The Charlson median score was 4.8. A score ≥ 4 was recorded in 89.4% at admission in ICU. Past histories of hypertension (50.6%), diabetes (23.6%) and peptic ulcers (6.3%) were common. The clinical features are summarized in Table 2. 42.1% of patients were comatose, with Glasgow coma score < 8. 100 (49.02%) patients had ASAPS score ≥ 8.
Medical conditions (60%), particularly of the Central Nervous System (CNS) (37.97%), were the most common. Among all diseases, stroke was most frequent (27.4%) followed by peritonitis. Care was based on fluid and electrolyte management, pain relief, and supply of oxygen. Only 2 patients were mechanically ventilated. During hospitalization, complications occurred in 89 patients (37.55%) of which acute respiratory distress syndrome (ARDS) was the main one (10.55%). In total 173 (73%) patients died in ICU. Table 3 summarizes the diagnoses and in-hospital outcome of patients.
The mean length of ICU stay was 5.3 ± 7.4 days [IC 95%; 1–58]. Ninety percent of those that died, did so within a week while 10% died after a week. Survivors and non-survivors were comparable based on demographic data (Table 4). When comparing survivors to non-survivors, there was a significant difference related to the emergency context (p = 0.001), surgical condition (p = 0.003), coma condition (p = 0.001), shock (p = 0.002), Charlson score ≥ 8 (p = 0.03), ASAPS score 8 ≥ at admission (p = 0.0001), stroke (p < 0.0001), diabetic complication (p = 0.01), and complication in ICU (p = 0.001) in univariate analysis.
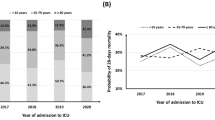
Most patients were between 64 to 74 years old. There was a significant difference between the age groups for Charlson score (p = 0.001) and complications in ICU (p = 0.01) (Table 5).
In multivariate analysis, surgery, coma at admission, shock, stroke, and severe brain trauma were independent risks factors of ICU death (Table 6).
Discussion
This retrospective study found that elderly patients represented 11.2% of admissions to ICU. This rate is comparable to the (10%) of Owojuyigbe et al. [8] and the (16.6%) of Belayachi et al. [9]. In developed countries elderly admissions rate to ICU was high. The rate of admission in our study may be due to life expectancy shortness that reflects Burkinabè demographic profile.
Patients mean age was 71.7 ± 6.1 years in our study. Other study found a mean age of 72 years in Morocco [9], 75.4 ± 6.8 years in Brasilia [10] and 73 years in Nigeria [8]. In our study, patients were mainly males. There was no correlation between gender and admission in the literature [8, 9]. Some studies reported similar results to ours [11, 12], but Fowler et al. [13] reported higher mortality in the female group.
Patient outcome was poor in our study with a mortality rate of 73%. Belayachi et al. [9] in Morocco, Wade et al. [14] in Senegal reported 44.7 and 42.8% respectively. The high mortality reported in Africa compared to developed countries may be due to inadequate equipment, resources and care limitations [9].
Advanced age alone does not preclude successful outcome [15]. In multivariate analysis independent risk factors were surgical conditions, coma, shock during admission, ASAPS ≥8, stroke, severe brain trauma. This result is comparable to literature reports [16, 17]. In our findings, stroke was the main cause of hospitalization, followed by peritonitis. There is no difference between age groups in term of mortality. The mean length of stay in ICU was 5.3 ± 6.8 days. While 46.6% of patients died within the first 3 days of admission, 90% of patient died within a week. For patients over 84 years, LOS was shorter and in-hospital mortality was less than patients aged less than 84 years. This can be explained by the family taking their relative home once they understand that the outlook for recovery is bleak. This explains the relatively low mortality rate and short stay. The overall poor outcomes may be due to late consultation and poor quality of care due to the inadequate facilities, equipment and lack of medications. Delay in consultation may be related to limited education, use of traditional medicine, poverty with concern about hospital costs and poor transportation.
This study has limitations due to being retrospective. We did not assess the impact of pre-hospitalization condition. Blood test abnormalities, and the impact of APACHE and SOFA scores on outcome were not evaluated and long-term mortality after hospital discharge was not studied.
Conclusion
These results show that elderly patients in ICU have a high risk of ICU death. Risk factors include coma at admission, shock state, high ASAPS, severe brain trauma, stroke and surgical condition. We need to better equip our ICU to assess and manage carefully elderly patients in order to reduce ICU mortality. Training geriatric specialists could improve chronic disease care of older patients and reduce their admission to ICU. A prospective study could give more information on risk and long term outcome of these frail patients.
Abbreviations
- ACS:
-
Alteration of consciousness
- AMCD:
-
Acute metabolic complication of diabetes
- APACHE:
-
Acute physiology and chronic health evaluation
- ARDS:
-
Acute respiratory distress syndrome
- ASAPS:
-
Ambulatory simplified acute physiologic score
- ICU:
-
Intensive care unit
- NCSRT:
-
National Center of Scientific Research and Technology
- OR:
-
Odd ratio
- SBT:
-
Severe brain trauma
- SOFA:
-
Sequential organ failure assessment
References
Mkum. WHO _ Definition of an Older or Elderly Person. 2013 https://www.scribd.com/document/190077600/WHO-Definition-of-an-Older-or-Elderly-Person
Wan H, Goodkind D, Kowal P. An aging world: 2015; 2016. p. P95/16–1.
Aegon. 2013. The changing face of retirement: the Aegon retirement readiness survey 2013—country reports. Aegon and the Transamerica Center for Retirement Studies. Dowloaded in URL: https://www.aegon.com/en/Home/Research/Aegon-Retirement-Readiness-Survey-2013.
Institut national de la statistique et de la demographie; La population du Burkina Faso de 1997 à 2006. 2009.
The world factbook. Africa, Burkina Faso, June 2017. URL: https://www.cia.gov/library/publications/the-world-factbook/geos/uv.html. Accessed 21 June 2017.
Bonkoungou P, Traoré I, Bako YP, Sanou J, Ouédraogo N. La mortalité en réanimation polyvalente du centre hospitalier universitaire Yalgado Ouédraogo de Ouagadougou au Burkina–Faso. Ann Fr Anesth Reanim. 2014;33(2):A310. https://doi.org/10.1016/j.annfar.2014.07.523. https://www.sciencedirect.com/science/article/pii/S0750765814007722
Dia NM, et al. Interest of ambulatory simplified acute physiology score (ASAPS) applied to patients admitted in an intensive care unit of an infectious diseases unit in Dakar. PS SowBull Soc Pathol Exot. 2015;108:175–80.
Owojuyigbe AM, Adenekan AT, Babalola RN, Adetoye AO, Olateju SOA, Akonoghrere UO. Pattern and outcome of elderly admissions into the Intensive Care Unit (ICU) of a low resource tertiary hospital. East Cent Afr J Surg. 2016;21(2):40. ISSN 2073–9990
Jihane B, El khayari M, Dendane T, Madani N, Abidi K, Abouqal R, Zeggwagh AA. Factors predicting mortality in elderly patients admitted to a Moroccan medical intensive care unit. S Afr J Crit Care. 2012;28(1):22–7. https://doi.org/10.7196/SAJCC.122.
de Cristo Stein F, Barros RK, Feitosa FS, Toledo DO, da Silva JM Jr, Ísola AM, Rezende E. Prognostic factors in elderly patients admitted in the intensive care unit. Rev Bras Ter Intensiva. 2009;21(3):255–61.
Williams TA, Dobb GJ, Finn JC, Webb SA. Long-term survival from intensive care: a review. Intensive Care Med. 2005;31(10):1306–15.
Friedrich JO, Wilson G, Chant C. Long-term outcomes and clinical predictors of hospital mortality in very long stay intensive care unit patients: a cohort study. Crit Care. 2006;10(2):R59.
Fowler RA, Sabur N, Li P, Juurlink DN, Pinto R, Hladunewich MA, et al. Sex-and age-based differences in the delivery and outcomes of critical care. Can Med Assoc J. 2007;177(12):1513–9.
Wade K, Diaby A, Niang E, Diallo A, Diatta B. Outcome of elderly patients in an intensive care unit in Dakar, Senegal. Méd Santé Trop. 2011;22(2):223–4.
De Rooij SE, Govers A, Korevaar JC, Abu-Hanna A, Levi M, de Jonge E. Short-term and long-term mortality in very elderly patients admitted to an intensive care unit. Intensive Care Med. 2006;32:1039–44.
Lerolle N, Trinquart L, Bornstain C, Tadié J-M, Imbert A, Diehl J-L, et al. Increased intensity of treatment and decreased mortality in elderly patients in an intensive care unit over a decade*. Crit Care Med. 2010;38(1):59–64.
Tabah A, Philippart F, Timsit JF, Willems V, Français A, Leplège A, et al. Quality of life in patients aged 80 or over after ICU discharge. Crit Care. 2010;14(1):R2.
Acknowledgements
I would like to acknowledge, Professor Mion and Dr. Owue for English language improvement of this paper.
Availability of data and materials
The data of this study are available from the corresponding author (LANKOANDE Martin m.hamtaani@gmail.com, 15 BP 106 Ouagadougou 15).
Author information
Authors and Affiliations
Contributions
GS, ML collected and reviewed data; ML, SG, AS contributed to conception and design, analyzed and interpreted the data. ML, PB wrote the manuscript. RAFK revised of the manuscript in terms of important or intellectual content. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Authors’ information
-
GS is a general practitioner,
-
ML is a Anesthetist working at in Anesthesia and Intensive Care Unit at Regional Hospital of Koudougou,
-
PB is an Assistant in Anesthesiology at the University PhD Joseph Ki-Zerbo.
-
AS is an Assistant in Anesthesiology at the University PhD Joseph Ki-Zerbo
-
RAFK, PhD, is a professor in Anesthesiology at the University PhD Joseph Ki-Zerbo.
Ethics approval and consent to participate
The Ethical and National Scientific Research and Technology Center (ENSRTC) (number 032/16) approved this study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Lankoandé, M., Bonkoungou, P., Simporé, A. et al. Inhospital outcome of elderly patients in an intensive care unit in a Sub-Saharan hospital. BMC Anesthesiol 18, 118 (2018). https://doi.org/10.1186/s12871-018-0581-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12871-018-0581-x