
Abstract
Background
Haemoglobin (Hb) variants such as sickle cell trait (SCT/HbAS) play a role in protecting against clinical malaria, but little is known about the development of immune responses against malaria parasite (Plasmodium falciparum surface protein 230 (Pfs230) and Plasmodium falciparum erythrocyte binding antigen 175 region-3 (PfEBA175-3R)) and vector (on the An. gambiae Salivary Gland Protein-6 peptide 1 (gSG6-P1)) antigens in individuals with variants Hb genotypes. This study assessed antibody (IgG) responses against malaria parasite, Pfs230 and PfEBA175-3R and vector, gSG6-P1 in febrile individuals with variant Hb genotypes.
Methods
The study was conducted on symptomatic malaria patients attending various healthcare facilities throughout Ghana. Microscopy and ELISA were used to determine the natural IgG antibody levels of gSG6-P1, PfEBA175-3R & Pfs230, and Capillarys 2 Flex Piercing was used for Hb variants determination.
Results
Of the 600 symptomatic malaria patients, 50.0% of the participants had malaria parasites by microscopy. The majority 79.0% (398/504) of the participants had Hb AA, followed by HbAS variant at 11.3% (57/504) and HbAC 6.7% (34/504). There were significantly (p < 0.0001) reduced levels of gSG6-P1 IgG in individuals with both HbAC and HbAS genotypes compared to the HbAA genotype. The levels of gSG6-P1 IgG were significantly (p < 0.0001) higher in HbAS compared to HbAC. Similarly, Pfs230 IgG and PfEBA-175-3R IgG distributions observed across the haemoglobin variants were significantly higher in HbAC relative to HbAS.
Conclusion
The study has shown that haemoglobin variants significantly influence the pattern of anti-gSG6-P1, Pfs230, and PfEBA-175 IgG levels in malaria-endemic population. The HbAS genotype is suggested to confer protection against malaria infection. Reduced exposure to infection ultimately reduces the induction of antibodies targeted against P. falciparum antigens.
Similar content being viewed by others


Background
Malaria continues to be a significant public health problem in Ghana, as it is in the rest of Sub-Saharan Africa. Ghana is one of ten African countries with the highest malaria burden with 5.9 million, 5.7 million, and 5.3 million malaria cases and 39,214, 12,557 and 11,557 malaria related death in 2020, 2021 and 2022 respectively [1,2,3]. Malaria is an endemic disease in Ghana, with seasonal changes in the north. The southern and middle belts have two different rainy seasons, but the northern region has a single rainy season that lasts from May to September. The transmission time in the northern section is six to seven months, and in the higher part, it is three to four months. Between July and November, the most malaria cases occur. Children under the age of five, as well as pregnant women, are more vulnerable due to weakened immunity. Malaria transmission in the southern belt lasts nine months or more.
Global efforts to control malaria shifted from reducing malaria morbidity and mortality to targeting the eradication of malaria [4, 5]. And in pursuit of this objective, several vaccine research efforts have focused on the pre-erythrocytic stage or transmission-blocking and blood-stage vaccine development but have encountered setbacks due to the redundancy in the invasion pathways and polymorphic nature of parasites’ antigens [6, 7]. Although haemoglobin variants such as sickle cell trait (SCT) are known to play a role by conferring protection against clinical malaria, little or no information about the effects of haemoglobin variants have on the production of malaria parasite antibodies [8, 9].
Malaria has had a considerable effect on human population genetics and continues to do so since traits conferring partial tolerance to infection or disease progression are selected in endemic areas [10]. This malaria hypothesis has been validated for several genetic polymorphisms such as HbS/C genotypes, and it is well established that hemoglobin variants, specifically HbAS, can confer relative malaria resistance [11,12,13,14].
HbAS has been associated with a high proportion of polyclonal P. falciprum infections, suggesting an increased breadth of antibody responses [9, 15]. It has been proposed that the protective effect of HbAS’s is related to multiple complex mechanisms linked with the immune response to malaria [9]. Populations living in malaria endemic have a variety of hemoglobin variants that may work synergistically to reduce Plasmodium virulence in humans and result from various geographical founding effects. Consequently, the diagnosis of parasites in febrile malaria patients provides knowledge that assists malaria-endemic countries in assessing their place on the spectrum of malaria elimination [3].
Moreover, antibodies against various P. falciprum antigens are crucial for controlling and managing parasite burden and disease progression. The prevalence of IgG of gSG6-P1, PfEBA175, and Pfs230 varies among individuals based on exposures and the level of malaria transmission among communities [16,17,18]. Haemoglobin (Hb) interacts with the innate immune system directly or through binding to pathogen-associated molecular patterns (PAMPs) [19]. In the search for immunological surrogates of immunity against malaria, a plethora of research has focused on antibody levels without determining the Hb genotype of the individuals, which is undoubtedly a critical parameter in developing immunity to malaria.
There is, thus, the need to know whether variant haemoglobin genotypes affect the development of antibody responses against malaria antigens. Although some antibodies have been identified as key to malaria protection and alleviating symptoms of the disease, there is a lack of rigorous information on the influence of haemoglobin variants on IgG levels in symptomatic patients across Ghana. The study determined the levels of antimalarial antibodies in symptomatic malaria patients with variant Hb genotypes (HbAS and HbAC).
Methods
Study design and study population
The study was carried out among symptomatic malaria patients seeking treatment at randomly selected healthcare facilities in the ten regions of Ghana. The enrolled suspected malaria patients (n = 600) were between the ages of 1 to 88 years. The samples were conveniently selected from 300 samples that tested positive and 300 samples that tested negative for P. falciparum by microscopy. Approximately, 1 ml of venous blood was collected from each participant into EDTA vacutainer tubes for malaria and mosquito antibody level estimation and haemoglobin phenotyping.
Microscopy
Thin and thick blood smears were prepared using 2 µL and 6 µL respectively of whole blood and processed as previously described [20]. Two independently WHO-certified microscopists examined the slides using an x100 oil immersion microscope.
Indirect enzyme-linked immunosorbent assay (ELISA)
An indirect ELISA was used to quantify the Immunoglobin G (IgG) antibodies levels against gSG6-P1, Pfs 230 and EBA-175 antigens among the participants using a previously published protocol [21, 22]. A 96-well NUNG Maxisorp ELISA plate was coated with either 1 µg/well of gSG6-P1 in phosphate buffer saline (PBS, pH 7.2), 20 µl/well EBA-175 in PBS, pH 7.2 or 1 µg/well of Pfs230 in carbonate buffer, pH 9.0 and incubated overnight at 4°C. The samples used include diluted plasma (1:200), a positive control sample obtained from a pool of seropositive individuals and negative control samples obtained from various pools of seronegative individuals in duplicate. The plates were washed three times and incubated for 1 hour with 100 µl/well of 1:3000 dilution of goat antihuman IgG-HRP. The plates were incubated with peroxidase substrate 3,3’,5,5’-teramethylbenzidine (TMB) for 10 min. 100 µl of 0.2 mM sulfuric acid was added to halt the enzymatic reactions and the optical densities (OD) of the contents in the wells were read at 450 nm using a Multiskan FC plate reader (Thermo Scientific, USA).
Haemoglobin genotyping
Two methods were used for haemoglobin genotyping. Part of the samples were analyzed using the automated multi-assay analyzer, the Capillarys 2 Flex Piercing ® [23, 24]. The analyzer was calibrated using a Hb A1c package (Sebia, Lisses, France. The samples were vortexed and mixed for 5 s and applied in a conical tube and barcoded for easy identification before sliding the sample rack for analysis. All sample preparations and analyses were performed in compliance with the manufacturer’s instructions. The second method used for Hb genotyping was based on the most commonly used method, the cellulose acetate electrophoresis at alkaline pH using standard procedure. Known samples of HbA, HbS, HbC and HbF were used as controls for each gel that was ran.
Data analysis
The information was entered into Excel and analyzed with GraphPad Prism (v.9.5.0). The data were grouped according to regions, diagnostic tests, haemoglobin genotypes, gender and age categories. The infection frequency was represented by simple counts and proportions. The IgG antibodies were categorized into 0-999, 1000–1999, 2000–2999 and > 3000 ng/mL for gSG6-P1 and Pfs230 IgG antibodies and 0-1999, 2000–4999, 5000–9999 and > 10,000 ng/mL for PfEBA175 3R IgG antibodies and analyzed using median and ranges [24]. The pattern of antibody distribution between P. falciprum positive and negative infections by microscopy were assessed using the odds ratio (OR). The statistical significance in the antibody distribution across haemoglobin (Hb) phenotypes was analyzed using the Chi-square test. Wilcoxon signed-rank test was used to assess the statistical significance in the distribution of antibodies across Hb genotypes. Statistical significance was set at P < 0.05.
Results
Characteristics of the study participants
the mean age ± SEM for the 600 study participants was 21.84 ± 0.80 years. A total of 57.3% of the population were female. Plasmodium falciparum was identified in 300 participants (50.0%). The highest (229,452, SE = 72,305) and lowest (35,217, SE = 11,091) mean parasite densities were obtained in study participants from the Upper West region and Central region respectively. Hb genotyping data were available for 504 (84%) of the population. The majority 398/504 (79.0%) of the participants had normal haemoglobin genotype (HbAA), followed by HbAS variant at 57/504 (11.3%) and HbAC 34/504 (6.7% ) (Table 1). Due to the low prevalence of the variant haemoglobin genotypes HbAS and HbAC, the data was analyzed at the national level rather than regional.
Parasite density and haemoglobin genotypes
Malaria parasite density was significantly higher in samples with haemoglobin AA compared to haemoglobin AC, p = 0.001 and AS, p < 0.001. similarly, malaria parasite density in samples with haemoglobin AS was significantly (p = 0.001) lower than the densities in haemoglobin AC samples (Fig. 1).

Distribution of parasite density among haemoglobin variants
Anopheles and Plasmodium falciparum antibody levels across the study population
The seroprevalence of gSG6-P1 was 223/399 (55.9% ), 34/57 (59.6% ) and 17/35 (48.6%) among microscopy-positive individuals with HbAA, HbAS and HbAC respectively. Similar seroprevalence patterns were observed for Pfs230 IgG and PfEBA-175-3R IgG antibodies in individuals with HbAA, HbAS and HbAC. The odds of detecting gSG6-P1 IgG antibodies among individuals that tested positive and negative by microscopy was 0.944 (0.431–2.052) and 1.478 (0.783–1.278) in Hb AC and Hb AS respectively. Similar observations were made for Pfs230 IgG and PfEBA-175-3R IgG antibodies in individuals with variant haemoglobin genotypes (Table 2).
Age and sex stratified Anopheles and Plasmodium falciparum IgG concentrations
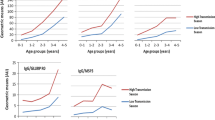
The median (95% CI) concentration of the gGS6-P1 IgG among the age 1–10, 11–20, 21–30, 31–40 and > 40 years were 1,245 (1,159-1,384), 1,306 (1,131-1,565), 1,314 (1,105-1,415),1,891 (1,720-2,411) and 1,490 (1,211-2,952) ng/mL respectively. There was a significant difference in the level of gSG6-P1 IgG antibodies between 1 and 10 years & 31–40 years, p < 0.001; 11–20 years & 31–40 years, p < 0.001; and 21–30 years & 31–40 years, p < 0.001 (Fig. 2a). There were no significant differences between age categories and the distribution of Pfs230 IgG except that responses in 1–10 years were less than in the > 40 years, p = 0.012 (Fig. 2b). Also, there were significant differences in the distribution of PfEBA-175 3R IgG between 1 and 10 years & 31–40 years, p = 0.011; 1–10 years & > 40 years, p = 0.001; 11–20 years & 21–30 years, p = 0.033; 11–20 years & 31–40 years, p = 0.014 and 11–20 years & > 40 years, p < 0.001 (Fig. 2c). There was a significant difference in levels of gSG6-P1 IgG antibodies between females and males, p = 0.012 (Fig. 3a). Pfs230 IgG (p = 0.846) levels showed no significant difference between female and male participants (Fig. 3b) and similarly, there was no significant difference in the PfEBA-175 3R IgG (p = 0.367) levels among female and male participants (Fig. 3c).

IgG antibody distribution across age categories. a gSG6-P1 IgG; b Pfs230 IgG; c PfEBA-175 IgG

IgG antibody distribution across gender. a gSG6-P1 IgG among males and females; b Pfs230 IgG among males and females; c PfEBA-175 IgG among males and females
gSG6-P1, Pfs230 and PfEBA-175-3R IgG concentrations and haemoglobin genotype
The results showed significantly reduced levels of gSG6-P1 IgG in HbAC, and HbAS, (p < 0.001) genotypes compared to the HbAA genotype. Also, the levels of gSG6-P1 IgG were significantly reduced in HbAC compared to HbAS, p < 0.001 (Fig. 4a). There were significantly reduced levels of Pfs230 IgG IgG in HbAC, and HbAS, (p < 0.001) genotypes compared to the HbAA genotype. Also, the levels of Pfs230 IgG IgG were significantly reduced in HbAC compared to HbAS, p < 0.001 (Fig. 4b). There were significantly reduced levels of PfEBA-175-3R IgG in HbAC, and HbAS, (p < 0.001) genotypes compared to the HbAA genotype. Also, the levels of PfEBA-175-3R IgG were significantly reduced in HbAC compared to HbAS, p < 0.001 (Fig. 4c).

Distribution of gSG6-P1 IgG antibody concentrations across haemoglobin variants. a The gSG6-P1 IgG distribution among Hb AA, Hb AC, Hb AS genotypes. b The Pfs230 IgG distribution among Hb AA, Hb AC, Hb AS genotypes. c The PfEBA-175-3R IgG distribution among Hb AA, Hb AC, Hb AS genotypes The data is presented as median and 95% CI; Statistical analysis was performed using the Wilcoxon rank test, ns, p >0.05; *, p < 0.05; **, p < 0.01; ***, p < 0.001; ****, p < 0.0001
Haemoglobin variants and the pattern of P. falciparum IgG antibodies in individuals that tested positive for P. falciparum by microscopy
The proportion of the haemoglobin genotypes between P. falciprum positive infection by microscopy and P. falciprum negative by microscopy showed the distribution of Hb genotype were the same. The difference in the proportion between microscopy positve (+) and microscopy negative (-) were 0.47% in HbAA, 2.08% in HbAC and 6.99% in HbAS. There were no significant differences in the prevalence Hb genotypes between microscopy positive and negative individuals (Table 3). Comparing the proportion of the P. falciprum infection in Hb AA and other Hb genotypes showed a highly significant difference in the proportions of P. falciprum infection in other Hb genotypes compared to Hb AA. The difference in the proportion of P. falciprum infections between HbAA and HbAC is 73.1% (×2 = 316.69, p < 0.001) and HbAA and HbAS is 67.24% (×2 = 264.07, p < 0.0001) (Table 4). The mean P. falciprum IgG antibodies were lower in HbAC (Pfs230 IgG = 2149 and PfEBA175-3R = 6551) compared to HbAA (Pfs230 = 3073 and PfEBA175-3R = 10,651). The HbAS on the other hand had a higher mean P. falciprum IgG antibodies (Pfs230 = 3530 and PfEBA175-3R = 11,470) compared to HbAA (Table 5).
Discussion
The study assessed the haemoglobin variants (sickle cell trait and haemoglobin C trait) on the An. gambiae Salivary Gland Protein-6 peptide 1 (gSG6-P1), Plasmodium falciparum surface protein 230 (Pfs230) and Plasmodium falciparum erythrocyte binding antigen 175 region-3 (PfEBA175-3R) immune responses among symptomatic malaria infection in Ghana.
The identification of biomarkers for assessing potential exposure to vector bites and the risk of vector-borne infections have recently gained substantial importance [25, 26]. Previous reports showed that Plasmodium falciparum-infected individuals presented with higher levels of IgG response against gSG6-P1 antigen than the uninfected individuals [25, 27,28,29]. Generally, the average time for outdoor activities has decreased over the years across ages due to work, rest, and leisure pursuits impacted by technological advancement [30]. The outdoor time among age groups under 30 years has decreased by 20% compared to age group 31 to 50 years decreased by only 9% [31, 32]. Thus, the age group 31–40 years age group likely spent more time in outdoor activities that exposed them to mosquito bites and increased the level of IgG concentration of gSG6-P1 among them compared to those under 30 years. The study observed high seroprevalence of IgG response against gSG6-P1 antigen in HbAA and HbAS participants among P. falciprum positive infections by microscopy compared to participants with submicroscopic positive P. falciprum infections. Contrarily, the participants with HbAC had a high seroprevalence of IgG response against gSG6-P1 antigen in the samples with P. falciparum negative infection by microscopy compared to Plasmodium falciparum positive infection samples diagnosed with microscopy.
The study showed that the HbAC and HbAS have a reduced distribution of gSG6-p1 IgG antibodies compared to HbAA. The observation could partly explain the lower IgG gSG6-P1 antibodies having a significant association with P. falciprum infection by microscopic diagnosis. High IgG antibody levels are associated with malaria infection, whereas Hb traits such as HbAS and Hb AC protect against P. falciprum infection [33]. Thus, the low IgG levels in the Hb traits explain the counter effect haemoglobin variants have on antibody development. The gSG6-p1 IgG-specific antibodies were detected, and no screening was performed to test for cross-reactivity with other antigens from other pathogens. Currently, no study has reported on the cross-reactivity of gSG6-p1 IgG-specific antibodies to non-mosquito antigens [34, 35].
A significantly lower median of anti-Pfs230-specific IgG were observed in HbAC and Hb AS compared to HbAA. HbAS showed a significantly high IgG response to Pfs230 antigens when compared with HbAC. Both haemoglobin variants C and S are shown to protect against severe malaria [36]. Hb AC is associated with frequent patent carriage of parasites and gametocytes [36, 37]. Two independent studies from Ghana and Burkina Faso reported higher gametocyte carriage in HbAC when compared with HbAA individuals [38, 39]. The Pfs230 antigen is expressed on the surface of gametocytes and only becomes exposed to the host immune system upon destruction and rapture from erythrocytes. The low anti-Pfs230 IgG indicates reduced destruction of gametocytes in HbAC variants. Thus, higher gametocyte carriage in HbAC may be due to reduced gametocyte destruction and relatively produced patent gametocytes [38, 40]. The haemoglobin C is associated with a longer P. falciprum infection due to a higher parasitaemia threshold for pyrexia or a change in parasite dynamics that delays the parasites from reaching the pyrogenic threshold [39, 40].
The HbAS and HbAC target the pathogenic process of severe clinical malaria and influence non-severe clinical malaria risk [37]. The study observed a significantly lower IgG anti-PfEBA exposure in HbAS and HbAC compared with HbAA. Although, we do not fully understand different mechanisms in natural infections and how within-host parasite dynamics in the HbAA individuals and in AS or AC heterozygotes, the observation support previous finding that HbAC individuals frequently carry patent parasites, whereas HbAS individuals have reduced malaria positivity [36, 37]. Thus, lower exposure of P. falciprum parasite infections to the host immune system in HbAS results in low IgG antibody levels of EBA-175 compared to HbAC which sustains prolonged malaria infection with higher asexual parasite levels. Contrary to the finding of this study, some studies have reported enhanced IgG immune response specifically against P. falciprum erythrocyte membrane protein (PfEMP1) [41, 42]. A study conducted by Lell et al., demonstrated that the combination of naturally acquired immunity and sickle cell traits exhibited a remarkable synergistic effect, resulting in a substantial reduction in malaria symptoms [43].
Conclusion
Symptomatic malaria patients with variant haemoglobin had significantly reduced IgG titres of gSG6-P1, Pfs230, and PfEBA-175 antibodies. The HbAS genotype is suggested to confer protection against malaria infection. Reduced exposure to infection ultimately reduces the induction of antibodies targeted against P. falciparum antigens.
Availability of data and materials
All the data are available in the manuscript.
References
Ehiem RC, Lawson BW, Larbi JA. Malaria knowledge-base and prevalence of Parasitaemia in asymptomatic adults in the Forest Zone of Ghana. Acta Parasitol. 2022;67(4):1719–31.
Willyard C. The bumpy road to malaria vaccination. Nature. 2022;612(7941):48–9.
Acheampong PR, Mohammed A, Twumasi-Ankrah S, Sylverken AA, Owusu M, Acquah-Gyan E, Adjei TK, Otupiri E, Owusu-Dabo E. This disease is not meant for the hospital, it is Asram’: implications of a traditionally-defined illness on healthcare seeking for children under-5 in rural Ashanti, Ghana. PLOS Global Public Health. 2022;2(9):e0000978.
Kaslow DC, Biernaux S. RTS, S: toward a first landmark on the Malaria Vaccine Technology Roadmap. Vaccine. 2015;33(52):7425–32.
Shretta R, Liu J, Cotter C, Cohen J, Dolenz C, Makomva K, Newby G, Ménard D, Phillips A, Tatarsky A, Gosling R. Malaria elimination and eradication 2017.
Pance A. Diversify and conquer: the vaccine escapism of Plasmodium Falciparum. Microorganisms. 2020;8(11):1748.
Wilson KL, Flanagan KL, Prakash MD, Plebanski M. Malaria vaccines in the eradication era: current status and future perspectives. Expert Rev Vaccines. 2019;18(2):133–51.
Tangteerawatana P, Montgomery SM, Perlmann H, Looareesuwan S, Troye-Blomberg M, Khusmith S. Differential regulation of IgG subclasses and IgE antimalarial antibody responses in complicated and uncomplicated Plasmodium falciparum malaria. Parasite Immunol. 2007;29(9):475–83.
Cabrera G, Cot M, Migot-Nabias F, Kremsner PG, Deloron P, Luty AJ. The sickle cell trait is associated with enhanced immunoglobulin G antibody responses to Plasmodium falciparum variant surface antigens. J Infect Dis. 2005;191(10):1631–8.
Crompton PD, Moebius J, Portugal S, Waisberg M, Hart G, Garver LS, Miller LH, Barillas-Mury C, Pierce SK. Malaria immunity in man and mosquito: insights into unsolved mysteries of a deadly infectious disease. Annu Rev Immunol. 2014;32:157–87.
Band G, Leffler EM, Jallow M, Sisay-Joof F, Ndila CM, Macharia AW, Hubbart C, Jeffreys AE, Rowlands K, Nguyen T, Gonçalves S. Malaria protection due to sickle haemoglobin depends on parasite genotype. Nature. 2022;602(7895):106–11.
Goheen MM, Campino S, Cerami C. The role of the red blood cell in host defence against falciparum malaria: an expanding repertoire of evolutionary alterations. Br J Haematol. 2017;179(4):543–56.
Acquah FK, Donu D, Bredu D, Eyia-Ampah S, Amponsah JA, Quartey J, Obboh EK, Mawuli BA, Amoah LE. Asymptomatic carriage of Plasmodium Falciparum by individuals with variant blood groups and haemoglobin genotypes in southern Ghana. Malar J. 2020;19(1):1–8.
Amoah LE, Asare KK, Dickson D, Abankwa J, Busayo A, Bredu D, Annan S, Asumah GA, Peprah NY, Asamoah A. Laurencia Malm K. Genotypic glucose-6-phosphate dehydrogenase (G6PD) deficiency protects against Plasmodium falciparum infection in individuals living in Ghana. PLoS ONE. 2021;16(9):e0257562.
Fowkes FJ, Allen SJ, Allen A, Alpers MP, Weatherall DJ, Day KP. Increased microerythrocyte count in homozygous α+-thalassaemia contributes to protection against severe malarial anaemia. PLoS Med. 2008;5(3):e56.
Ouédraogo AL, Roeffen W, Luty AJ, de Vlas SJ, Nebie I, Ilboudo-Sanogo E, Cuzin-Ouattara N, Teleen K, Tiono AB, Sirima SB, Verhave JP, Bousema T, Sauerwein R. Naturally acquired immune responses to Plasmodium Falciparum sexual stage antigens Pfs48/45 and Pfs230 in an area of seasonal transmission. Infect Immun. 2011;79(12):4957–64. Epub 2011 Oct 3. PMID: 21969000; PMCID: PMC3232645.
Amoah LE, Abagna HB, Akyea-Mensah K, Lo AC, Kusi KA, Gyan BA. Characterization of anti-EBA175RIII-V in asymptomatic adults and children living in communities in the Greater Accra Region of Ghana with varying malaria transmission intensities. BMC Immunol. 2018;19(1):1–9.
Badu K, Siangla J, Larbi J, Lawson BW, Afrane Y, Ong’echa J, Remoue F, Zhou G, Githeko AK, Yan G. Variation in exposure to Anopheles gambiae salivary gland peptide (gSG6-P1) across different malaria transmission settings in the western Kenya highlands. Malar J. 2012;11:1–9.
Antelo GT, Vila AJ, Giedroc DP, Capdevila DA. Molecular evolution of transition metal bioavailability at the host–pathogen interface. Trends Microbiol, 29(5), 441–57.
Amoah LE, Asare KK, Dickson D, Anang SF, Busayo A, Bredu D, Asumah G, Peprah N, Asamoah A, Abuaku B, Malm KL. Nationwide molecular surveillance of three Plasmodium species harboured by symptomatic malaria patients living in Ghana. Parasites Vectors. 2022;15(1):40.
Acquah FK, Obboh EK, Asare K, Boampong JN, Nuvor SV, Singh SK, Theisen M, Williamson KC, Amoah LE. Antibody responses to two new Lactococcus lactis-produced recombinant Pfs48/45 and Pfs230 proteins increase with age in malaria patients living in the Central Region of Ghana. Malar J. 2017;16(1):1–1.
Kwapong SS, Asare KK, Kusi KA, Pappoe F, Ndam N, Tahar R, Poinsignon A, Amoah LE. Mosquito bites and stage-specific antibody responses against Plasmodium Falciparum in southern Ghana. Malar J. 2023;22:126. https://doi.org/10.1186/s12936-023-04557-8.
Jaisson S, Leroy N, Meurice J, Guillard E, Gillery P. First evaluation of Capillarys 2 flex Piercing®(Sebia) as a new analyzer for HbA1c assay by capillary electrophoresis. Clin Chem Lab Med. 2012;50(10):1769–75.
Poventud-Fuentes I, Garnett E, Vispo B, Elghetany MT, Devaraj S. Hemoglobin fractionation by Sebia Capillarys 2 flex piercing System as primary method for evaluation of hemoglobinopathies. Clin Chim Acta. 2021;519:193–7.
Doucoure S, Cornelie S, Drame PM, Marie A, Elanga Ndille E, Mathieu-Daudé F, Springer. Springer. Biomarkers of vector bites: Arthropod immunogenic salivary proteins in vector-borne diseases control. Gen. Methods Biomark. Res. their Appl. 2015 Jun 19:1177 – 205.
Drame PM, Poinsignon A, Besnard P, Le Mire J, Dos-Santos MA, Sow CS, Cornelie S, Foumane V, Toto JC, Sembene M, Boulanger D. Human antibody response to Anopheles gambiae saliva: an immuno-epidemiological biomarker to evaluate the efficacy of insecticide-treated nets in malaria vector control. Am J Trop Med Hyg. 2010;83(1):115.
Sagna AB, Gaayeb L, Sarr JB, Senghor S, Poinsignon A, Boutouaba-Combe S, Schacht AM, Hermann E, Faye N, Remoue F, Riveau G. Plasmodium Falciparum infection during dry season: IgG responses to Anopheles gambiae salivary gSG6-P1 peptide as sensitive biomarker for malaria risk in Northern Senegal. Malar J. 2013;12(1):1–0.
Asare KK. The submicroscopic Plasmodium falciparum malaria in sub-Saharan Africa—current understanding of the host immune system and new perspectives. In: Piccaluga PP, editor. Malaria—recent advances and new perspectives. IntechOpen. 2022. https://www.intechopen.com/online-first/81972.
Cheteug G, Elanga-Ndille E, Donkeu C, Ekoko W, Oloume M, Essangui E, Nwane P, NSango SE, Etang J, Wanji S, Ayong L. Preliminary validation of the use of IgG antibody response to Anopheles gSG6-p1 salivary peptide to assess human exposure to malaria vector bites in two endemic areas of Cameroon in Central Africa. PLoS ONE. 2020;15(12):e0242510.
Hurd A, Anderson DM, Mainieri T. Kraus’ recreation and leisure in modern society. Jones & Bartlett Learning; 2021. Aug 6.
Matz CJ, Stieb DM, Davis K, Egyed M, Rose A, Chou B, Brion O. Effects of age, season, gender and urban-rural status on time-activity: Canadian Human Activity Pattern Survey 2 (CHAPS 2). Int J Environ Res Public Health. 2014;11(2):2108–24.
Degefa T, Githeko AK, Lee MC, Yan G, Yewhalaw D. Patterns of human exposure to early evening and outdoor biting mosquitoes and residual malaria transmission in Ethiopia. Acta Trop. 2021;216:105837.
Nasr A, Saleh AM, Eltoum M, Abushouk A, Hamza A, Aljada A, El-Toum ME, Abu-Zeid YA, Allam G, ElGhazali G. Antibody responses to P. falciprum apical membrane Antigen 1 (AMA-1) in relation to haemoglobin S (HbS), HbC, G6PD and ABO blood groups among Fulani and Masaleit living in Western Sudan. Acta Trop. 2018;182:115–23.
Kassam NA, Kulaya N, Kaaya RD, Schmiegelow C, Wang CW, Kavishe RA, Alifrangis M. Use of anti-gSG6-P1 IgG as a serological biomarker to assess temporal exposure to Anopheles’ mosquito bites in Lower Moshi. PLoS ONE. 2021;16(10):e0259131.
Ndo C, Elanga-Ndille E, Cheteug G, Metitsi RD, Wanji S, Moukoko CE. IgG antibody responses to Anopheles gambiae gSG6-P1 salivary peptide are induced in human populations exposed to secondary malaria vectors in forest areas in Cameroon. PLoS ONE. 2022;17(11):e0276991.
Gonçalves BP, Sagara I, Coulibaly M, Wu Y, Assadou MH, Guindo A, Ellis RD, Diakite M, Gabriel E, Prevots DR, Doumbo OK. Hemoglobin variants shape the distribution of malaria parasites in human populations and their transmission potential. Sci Rep. 2017;7(1):1–9.
Drakeley C, Gonçalves B, Okell L, Slater H. Understanding the importance of asymptomatic and low-density infections for malaria elimination. Towards Malaria Elimination-A Leap Forward. Jul. 2018;18:1–20.
Ringelhann B, Hathorn MK, Jilly P, Grant F, Parniczky G. A new look at the protection of hemoglobin AS and AC genotypes against plasmodium falciparum infection: a census tract approach. Am J Hum Genet. 1976;28:270–9.
Gouagna LC, Bancone G, Yao F, Yameogo B, Dabiré KR, Costantini C, Simporé J, Ouedraogo JB, Modiano D. Genetic variation in human HBB is associated with Plasmodium Falciparum transmission. Nat Genet. 2010;42(4):328–31.
Miura K, Deng B, Wu Y, Zhou L, Pham TP, Diouf A, Wu CK, Lee SM, Plieskatt JL, Morin MJ, Long CA. ELISA units, IgG subclass ratio and avidity determined functional activity of mouse anti-Pfs230 antibodies judged by a standard membrane-feeding assay with Plasmodium Falciparum. Vaccine. 2019;37(15):2073–8.
Amaratunga C, Lopera-Mesa TM, Brittain NJ, Cholera R, Arie T, Fujioka H, Keefer JR, Fairhurst RM. A role for fetal hemoglobin and maternal immune IgG in infant resistance to Plasmodium Falciparum malaria. PLoS ONE. 2011;6(4):e14798.
Fairhurst RM, Bess CD, Krause MA. Abnormal PfEMP1/knob display on Plasmodium falciparum-infected erythrocytes containing hemoglobin variants: fresh insights into malaria pathogenesis and protection. Microbes Infect. 2012;14(10):851–62.
Lell B, Mordmüller B, Agobe JC, Honkpehedji J, Zinsou J, Mengue JB, Loembe MM, Adegnika AA, Held J, Lalremruata A, Nguyen TT. Impact of sickle cell trait and naturally acquired immunity on uncomplicated malaria after controlled human malaria infection in adults in Gabon. Am J Trop Med Hyg. 2018;98(2):508.
Acknowledgements
We thank all the study participants for willingly participating in the study.
Consent to participate
Written informed consent including assent for adolescents aged from 11 to 17, and parental consent for children aged 17 years and below were obtained for all the recruited study participants.
Funding
This project was supported in part by the West African Genetic Medicine Center (WAGMC).
Author information
Authors and Affiliations
Contributions
Conceptualization, LEA; Formal analysis, KKA, LEA, BA; Methodology, BA; Supervision, LEA, NAA, FSOA; Validation, KKA, WK, NAA; Visualization, KKA, BA; Writing – original draft, KKA, BA, LEA; Writing – review & editing; KKA, LEA, BA, FSOA, WK, NAA.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Institutional Review Board (IRB) of the Noguchi Memorial Institute for Medical Research (NMIMR no. 024/14–15 & 089/14–15). All the methods were straightly carried out as approved by the IRB and in accordance with the relevant guidelines and regulations of the Helsinki Declaration 2013 (64th WMA General Assembly, Fortaleza, Brazil, October 2013).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Asare, K.K., Agrah, B., Ofori-Acquah, F.S. et al. Immune responses to P falciparum antibodies in symptomatic malaria patients with variant hemoglobin genotypes in Ghana. BMC Immunol 25, 14 (2024). https://doi.org/10.1186/s12865-024-00607-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12865-024-00607-1