
Abstract
Background
Paratesticular fibrous pseudotumour is a rare benign growth with unclear pathogenesis and clinical management. It has been linked to Serum IgG4-related disease. This mass can notoriously masquerade around as a malignancy; however, a conservative (testis sparing) approach is sufficient as surgical management.
Case presentation
We present the case of a 35-year-old gentleman who presented with a slow growing paratesticular mass, raising the suspicion of a malignancy. However, normal tumour markers and benign appearance on imaging modalities compelled us to give trial of local excision with intra-operative frozen section analysis. After confirmation of benign pathology of the mass, the incision was closed. Final histopathology confirmed the diagnosis of benign paratesticular fibrous pseudotumour, and serum IgG levels were noted to be elevated.
Conclusion
Thus, using tumour markers, radiological imaging and intraoperative frozen section, a potential radical resection can be avoided, testis sparing surgery, employed.
Similar content being viewed by others


1 Background
Paratesticular fibrous pseudotumour (PFP) is a rare tumour-like lesion accounting for around 6% of all paratesticular masses which has been recently associated with Serum IgG4-related disease (IgG4-RD). Through the course of history, it has been called by numerous names like chronic proliferative periorchitis and fibromatous periorchitis [1]. Even though these lesions are uniformly benign, they are of concern and due clinical relevance because they mimic neoplastic processes and can often result in an overzealous resection. We report a case, which helps to corroborate our finding of a PFP with Serum IgG4-related disease.
2 Case presentation
A gentleman, aged 35 years, presented with chief complaints of a left-sided hemiscrotal mass since 3 years which he noticed following a trivial trauma. No significant details were noted in past medical and surgical history. On physical examination, a single, firm, non-tender, bosselated mass located inferior to the left testis was palpable separate from the left testis. Inguinal lymph nodes were not palpable. Scrotal ultrasound revealed a 6 × 6x5cm hypoechoic lesion, devoid of vascularity located caudal to the left testicle with no intratesticular extension and no enlarged inguinal lymph nodes. Pre-operative blood parameters including tumour markers like beta-human chorionic gonadotropin, alpha fetoprotein and lactate dehydrogenase were within normal limits.
Surgical excision was planned with intraoperative frozen section analysis (Fig. 1a). A left-sided pararaphian trans-scrotal incision was taken, and on further scrotal exploration, a bosselated paratesticular mass with no extension into any other adjoining structure was noted (Fig. 1b). It was completely excised sparing the left testicle and sent for frozen section. After frozen section was reported negative for malignancy, the incision was closed in layers. The patient had an uneventful post-operative stay and was discharged the following evening. He had no recurrence on 12 months of follow-up.

a Pre-operative clinical image of the scrotum showing the paratesticular mass, b Intra operative image showing paratesticular mass separate from the testis
Histopathology of the specimen on hematoxylin and eosin staining revealed dense lymphoplasmacytic infiltration without any atypia over a background of patchy areas of hyalinised collagen and storiform fibrosis with an atypical picture of obstructive venulitis (Fig. 2). On immunostaining with IgG4 antibodies, IgG4 positive plasma cells comprised of more than 40% of the cells per high power field confirming the microscopic diagnosis of paratesticular fibrous pseudotumour secondary to IgG4-related disease. Retrospectively, serum IgG4 levels were done for the patient, which were elevated.

Histopathology images of the lesion showing a dense lymphocytic infiltrate, b storiform fibrosis with hyalinised collagen, c plasma cell infiltration, d immunohistochemistry showing more than 40% infiltration by IgG4 positive plasma cells
3 Discussion
PFP is an exceptionally rare lesion with fewer than 200 cases reported to date and is hence poorly understood. It was first reported by Sir Astley Cooper et al. [1] in 1830. It is usually found in young to middle-aged adults and can present either as a single discreet nodule or diffuse multinodular hemiscrotal mass. This lesion is notorious for masquerading as a malignancy due to its location and typical hard consistency.
IgG4-RD is a recently defined systemic disease characterised by diffuse fibrosis and pseudotumors with infiltration of IgG4 + plasma cells. IgG4-RD often mimics neoplastic diseases and involves multiple organs including the submandibular gland, lung, pancreas, retroperitoneum, kidney and prostate. Testis and its adnexal structures rarely show any involvement however. Our patient did not show any systemic manifestations of IgG4-RD and presented with an isolated paratesticular mass. The inflammatory process resulting in formation of this mass can be stimulated by surgery, trauma or infections. The predominance of plasma cells with dense lymphocytic infiltrate and raised serum IgG4 levels in these patients point towards a likely association with IgG4-RD. Bosumuller et al. [2] were the first to note an association between PFP and IgG4-RD.
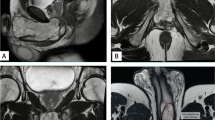
The typical ultrasonographic features of PFP involve well-defined margins of the lesion and an extra testicular location. The lesion is usually homogenously hypoechoic and can show small foci of calcification. MRI shows low signal density on T2-weighted imaging, intermediate signal density on T1 weighted scanning with low and inhomogeneous uptake of gadolinium contrast agent [3, 4]. Suspicion of testicular or adnexal malignancy prompted admission to hospital in our case. Pre-operative imaging and haematological investigation were not in favour of malignancy and therefore a decision of excision of the mass with intraoperative frozen section analysis was taken. The mass was attached to testis by a stalk which was removed along with a rim of macroscopically uninvolved testis. Once the frozen section came negative for malignancy, the incision was closed in layers thereby safely avoiding a radical surgery.
Histologically, PFPs present with the typical histomorphological features of paucicellular hyalinised tissue with interspersed bundles of collagen fibres. Spindle cells, lymphocytes and plasma cells are also noted. Increased plasma cells and storiform fibrotic changes also raise the suspicion of IgG4-RD. For establishing the diagnosis of IgG4-RD, four morphological features are required: (1) a proportion of (at least) 40% IgG4-positive cells among IgG-producing plasma cells, (2) a predominantly T-lymphocytic, often lymphofollicular infiltrate, (3) storiform fibrosis and (4) venulitis [5]. If three out of four criteria are met, the disease is highly probable. Yet, the extent of fibrosis and the density of the cellular infiltrate may vary considerably according to the involved organ. In the present case, there is evidence of all of the four characteristic features thereby confirming our diagnosis. Histological result obtained in our case along with raised serum IgG4 levels lends support to the theory of PFPs being an IgG4-related sclerosing disorder.
4 Conclusion
Serum IgG4 disease is a poorly understood disease with a varied spectrum of presentation which can manifest as a tumour-like lesion in the paratesticular region. Despite its rarity, PFP should be a part of differentials for all testicular adnexal masses. A high index of suspicion along with prudent pre-operative blood work up and imaging studies could help in its timely diagnosis. A gonad sparing surgery is sufficient and can represent the treatment of choice for this lesion avoiding an overzealous resection.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- PFP:
-
Paratesticular fibrous pseudotumour
- IgG4-RD:
-
Serum IgG4-related disease
- MRI:
-
Magnetic resonance imaging
References
Zhang Z, Yang J, Li M, Cai W, Liu Q, Wang T, Guo X, Wang S, Liu J, Ye Z (2014) Paratesticular fibrous pseudotumor: a report of five cases and literature review. Front Med 8(4):484–488. https://doi.org/10.1007/s11684-014-0325-3 (Epub 2014 Mar 14 PMID: 24627288)
Bösmüller H, von Weyhern CH, Adam P, Alibegovic V, Mikuz G, Fend F (2011) Paratesticular fibrous pseudotumor–an IgG4-related disorder? Virchows Arch 458(1):109–113. https://doi.org/10.1007/s00428-010-0995-4 (Epub 2010 Oct 19 PMID: 20957491)
Grebenc ML, Gorman JD, Sumida FK (1995) Fibrous pseudotumor of the tunica vaginalis testis: imaging appearance. Abdom Imaging. 20(4):379–80. https://doi.org/10.1007/BF00203377 (PMID: 7549749)
Dieckmann KP, Struss WJ, Frey U et al (2013) Paratesticular fibrous pseudotumor in young males presenting with histological features of IgG4-related disease: two case reports. J Med Case Rep 7:225. https://doi.org/10.1186/1752-1947-7-225
Deshpande V, Zen Y, Chan JK, Yi EE, Sato Y, Yoshino T, Klöppel G, Heathcote JG, Khosroshahi A, Ferry JA, Aalberse RC, Bloch DB, Brugge WR, Bateman AC, Carruthers MN, Chari ST, Cheuk W, Cornell LD, Fernandez-Del Castillo C, Forcione DG, Hamilos DL, Kamisawa T, Kasashima S, Kawa S, Kawano M, Lauwers GY, Masaki Y, Nakanuma Y, Notohara K, Okazaki K, Ryu JK, Saeki T, Sahani DV, Smyrk TC, Stone JR, Takahira M, Webster GJ, Yamamoto M, Zamboni G, Umehara H, Stone JH (2012) Consensus statement on the pathology of IgG4-related disease. Mod Pathol 25(9):1181–1192. https://doi.org/10.1038/modpathol.2012.72 (Epub 2012 May 18 PMID: 22596100)
Acknowledgements
The authors are grateful to Department of General Surgery for providing support throughout the publication of this case.
Funding
All the expenditure was borne by the authors.
Author information
Authors and Affiliations
Contributions
JRK was the primary investigator who worked up the patient, did literature review and prepared the manuscript. ND and GS were the surgeons for the procedure. Manuscript review, collection of data and literature review were done by ND, GS and SH. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethics approval was taken from the Institutional Ethics Committee and a written consent to participate was taken from the patient.
Consent for publication
Written consent to participate in the case report was taken from the patient.
All the authors give their consent for publication of this case report in African Journal of Urology.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Kudunthail, J.R., Dhimole, N., Singh, G. et al. Paratesticular fibrous pseudotumour: case report of a rare manifestation of IgG4-related disease. Afr J Urol 27, 118 (2021). https://doi.org/10.1186/s12301-021-00220-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12301-021-00220-3