
Abstract
Background
Some patients have demonstrated evidence of heterotopic ossification (HO) following total hip arthroplasty (THA). Selective and non-selective non-steroidal anti-inflammatory drugs (NSAIDs) are used as prophylaxis for HO following THA. This meta-analysis compared selective versus non-selective NSAIDs as prophylaxis for HO following THA.
Material and methods
The present study was conducted according to the PRISMA 2020 guidelines. All the clinical investigations comparing selective versus non-selective NSAIDs as prophylaxis for HO following THA were accessed in February 2022. An assessment of the methodological quality and statistical analyses were performed through the risk of bias summary tool of the Review Manager 5.3 software (Cochrane Collaboration, Copenhagen). The modified Brooker staging system was used to rate the efficacies of the interventions.
Results
Data from 8 studies and 1526 patients were collected. 60.8% were female. No difference was found in the sample size, mean age, and percentage of females between the two groups at baseline. No statistically significant difference was found between selective and non-selective NSAIDs in term of efficacy. 72% (1078 of 1502) of the patients were classified as Brooker 0, 21% (322 of 1502) as Brooker I, 5% (80 of 1502) as Brooker II, 1% (16 of 1502) as Brooker III, and 0.1% (2 of 1502) as Brooker IV.
Conclusion
Selective and non-selective NSAIDs were equally effective when used as prophylaxis for HO following THA.
Level of evidence
Level III, systematic review and meta-analysis.
Similar content being viewed by others


Introduction
In the absence of prophylaxis, the frequency of heterotopic ossification (HO) following total hip arthroplasty (THA) varies from 15 to 90% [1,2,3,4,5]. The exact cause and mechanism of bone formation after hip replacement remains unclear. Several approaches to reducing the occurrence of HO have been proposed, such as radiotherapy, non-steroidal anti-inflammatory drugs (NSAIDs), and diphosphonates [2, 5,6,7,8]. Evidence suggests that inhibition of the inflammation pathway may represent the underlying mechanism for ossification prevention [2]. The prophylactic effect of NSAIDs on HO was first documented when indomethacin was used as an analgesic after THA [9]. NSAIDs are typically divided into groups based on their cyclooxygenase (COX) selectivity: non-selective NSAIDs are directed to both COX-1 and COX-2, and selective NSAIDs are directed specifically to COX-2 [10]. Indomethacin is the NSAID most frequently used as prophylaxis for HO [11,12,13]. Other non-selective NSAIDs such as ketorolac, acetylsalicylic acid, meloxicam, naproxen, ibuprofen, and diclofenac have also been employed successfully [14,15,16,17]. Gastrointestinal complications are the most common reason for therapy discontinuation in patients treated with non-selective NSAIDs [18, 19]. Given their lack of interactions with platelet aggregation and gastrointestinal complications, selective NSAIDs are effective treatment alternatives to non-selective NSAIDs [4, 5, 20,21,22,23,24]. In selected patients, celecoxib is a valid alternative to non-selective NSAIDs, demonstrating efficacy, tolerability, and a lower rate of therapy discontinuation [20, 21, 25, 26]. Even rofecoxib was effective when used as prophylaxis for HO [7, 27]. However, many studies have shown an elevated risk of cardiovascular and renal complications with selective NSAID administration [4, 5, 20,21,22, 28]. The elevated cardiovascular risk was evidenced in patients treated with selective NSAIDs for longer than 6 months [22, 25]. However, whether the administration of selective NSAIDs for less than 20 days leads to an elevated risk of cardiovascular complication remains unclear [29]. Whether selective NSAIDs are equally as effective as non-selective NSAIDs for the prevention of HO following THA has also not been fully clarified. Therefore, a meta-analysis was conducted. This study compared selective versus non-selective NSAIDs as prophylaxis for HO following THA.
Methods
Eligibility criteria
All the clinical trials comparing selective versus non-selective NSAIDs as prophylaxis for HO following THA were accessed. Only studies with accessible full texts that are published in peer-reviewed journals were considered. Given the authors’ language capabilities, articles in English, German, Italian, French, and Spanish were eligible. Only prospective evidence level I and II studies, according to the Oxford Centre of Evidence-Based Medicine [30], were considered. Reviews, opinions, letters, and editorials were not considered. Animal, in vitro, biomechanical, computational, and cadaveric studies were all not eligible. Studies evaluating HO in locations other than the hip were not considered, nor were those evaluating procedures other than THA. Studies which evaluated radiation, hormonal therapy, or other experimental therapies were not considered. Only studies that evaluated the rate of HO following THA using the Brooker classification [31] in a clinical setting were eligible. Missing quantitative data for the outcome of interest warranted the exclusion of the study from the present investigation.
Search strategy
This systematic review was conducted according to the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [32]. The PICO algorithm was preliminarily pointed out:
-
P (population): patients following THA
-
I (intervention): prophylaxis of HO
-
C (comparison): selective versus non-selective NSAIDs
-
O (outcomes): Brooker classification [31].
In February 2022, the following databases were accessed: Pubmed, Web of Science, Google Scholar, and Embase. No time constraints were used in the search. The following keywords were used in combination with the Boolean operators AND/OR: hip, replacement, arthroplasty, prosthesis, heterotopic, ossification, impingement, indomethacin, naproxen, NSAIDs, selective, non-selective, prostaglandin, cyclooxygenase, acetylsalicylic acid, celecoxib, meloxicam, COX-inhibitors, rofecoxib, ibuprofen, diclofenac.
Selection and data collection
Two authors (A.P. and F.M.) independently performed the database search. All the resulting titles were screened and, if suitable, the abstract was accessed. The full texts of the abstracts that matched the topic were accessed. A cross-reference of the bibliographies of the full-text was also performed. Disagreements were debated, and the final decision was made by a third author (N.M.).
Data extraction
Two authors (A.P. and F.M.) performed data extraction independently. Study generalities and the patient demographics were extracted: author, year, length of the follow-up, type and protocol of the treatment, number of patients, mean age, and percentage of women. The outcome of interest was to compare the rate of HO following THA between selective and non-selective NSAIDs. The modified Brooker staging system was used to rate the efficacy of the interventions. This classification differs from the original by an additional grade of 0, in which there is no sign of HO [33] (Table 1).
Risk of study bias assessment
The risk of study bias was assessed by one author (A.P.) using Review Manager version 5.3 (Nordic Cochrane Collaboration, Copenhagen). The risk of bias graph was used to assess the methodological quality of the included studies. Allocation, randomization, blinding of the assessors, selective reporting, incomplete data, and an unknown source of bias were used for assessment. To assess the overall risk of publication bias, a funnel plot of the most reported endpoint was created and evaluated.
Synthesis methods
The statistical analyses were conducted by the main author (F.M.) using the Review Manager software (RevMan 5.3, Nordic Cochrane Collaboration, Copenhagen). For dichotomic data, the Mantel–Haenszel method with an odds ratio (OR) effect measure was adopted. The confidence interval was set at 95% in all comparisons. Higgin’s I2 test was conducted to evaluate heterogeneity. Values of I2 of greater than 50% indicated that the analysis may be affected by substantial heterogeneity. The \(\chi\)2 test was conducted to evaluate whether data were statistically significant. P < 0.05 indicated statistically significant heterogeneity. A fixed model effect was adopted as default. If I2 > 50% and P \(\chi\)2 < 0.05, a random effect model was adopted. Egger’s linear regression was performed using the STATA MP software (version 16; StataCorp, College Station, USA) to assess the asymmetry of the funnel plot, with values of P < 0.05 indicating statistically significant asymmetry.
Results
Study selection
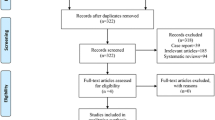
The literature search resulted in 6023 articles. Of those, 767 focused on prophylaxis for HO following THA. Of those, 507 were excluded as they were duplicates. A further 252 articles were excluded as they did not match the eligibility criteria: the full text was not accessible or published in peer-reviewed journals (N = 11); language limitation (N = 8); poor level of evidence (N = 29); inappropriate study design (N = 47); locations other than the hip or procedures other than THA were evaluated (N = 94); the comparison was not between selective and non-selective NSAIDs (N = 51); the Brooker classification was not used (N = 4); quantitative data on the outcome of interest were missing (N = 8). Finally, eight studies were included in the present investigation. The literature search results are shown in Fig. 1.

Flow chart of the literature search
Risk of study bias assessment
In the above-mentioned assessment of risk of bias, a very low risk of selection bias was evidenced. Similarly, the risk of attrition and reporting bias can be considered to be very low. The risk of detection bias scored low. This reflected the fact that randomization was present in most of the included studies. The risk of unknown bias was also moderate to low. Therefore, the methodological assessment of the bias in this work gave very good results. The Cochrane risk of bias summary tool is shown in Fig. 2.

Methodological quality assessment
Risk of publication bias
A funnel plot of the most reported comparison (Brooker class 0) was created and evaluated (Fig. 3). The plot evidenced adequate symmetry. Egger’s test evidenced any statistically significant asymmetry (P = 0.1).

Funnel plot of the most reported outcome
Study characteristics and results of individual studies
Data from 1526 patients were collected. 60.8% of those patients (928 of 1526 patients) were female. The mean age of the patients at baseline was 63.9 ± 3.6 years. No difference was found in the sample size, mean age, and percentage of females between non-selective and selective NSAID group at baseline (P > 0.5). Generalities of the included studies and the patient demographics are shown in Table 2.
Results of syntheses
Both selective and non-selective NSAIDs were effective in the prophylaxis of HO (Fig. 4). Both classes of NSAIDs were effective at preventing HO: 72% (1078 of 1502) of patients were classified as Brooker 0, 21% (322 of 1502) as Brooker I, 5% (80 of 1502) as Brooker II, 1% (16 of 1502) as Brooker III, and 0.1% (2 of 1502) as Brooker IV.

The graph shows that both types of NSAIDs were effective at preventing HO: 72% (1078 of 1502) of patients were classified as Brooker 0, 21% (322 of 1502) Brooker I, 5% (80 of 1502) Brooker II, 1% (16 of 1502) Brooker III, and 0.1% (2 of 1502) Brooker IV
No statistically significant difference was found between the selective and non-selective NSAIDs in terms of efficacy (Table 3).
Discussion
According to the main findings of the present study, selective and non-selective NSAIDs show similar efficacies when used as prophylaxis for HO following THA. 72% of the patients were classified as Brooker 0, 21% as Brooker I, 5% as Brooker II, 1% as Brooker III, and 0.1% as Brooker IV. However, selective NSAIDs have not been investigated at a large scale, and future high-quality trials are needed to validate these results in a clinical setting. The most commonly investigated drug for the prophylaxis of HO is indomethacin.
Three studies compared indomethacin and meloxicam [9, 17, 34]. Barthel et al. [17] showed that 25% of patients who received meloxicam developed HO, and 10% did so in the indomethacin group. On the contrary, two studies found a similar rate of HO in patients who received indomethacin or meloxicam [9, 34]. Also, celecoxib shows similar efficacy to indomethacin but higher efficacy than ibuprofen in the prevention of HO after THA, with a significantly lower rate of side effects [20, 25]. Very conclusive results came from two studies in which rofecoxib and indomethacin were compared [7, 36], with no significant difference in HO occurrence was observed between the two drugs. Furthermore, Winkler et al. [4] also found similar rates of HO in patients who received etoricoxib and those who received diclofenac. A recent meta-analysis of randomized controlled trials, which included 21 studies and 5995 patients, evaluated the efficacy and safety of NSAIDs for the prevention of HO after THA. The most common N-NSAIDs (indomethacin, ibuprofen, flurbiprofen, ketorolac, diclofenac) and S-NSAIDs (meloxicam, celecoxib, rofecoxib, tenoxicam) were used in the studies included. The authors observed that NSAIDs significantly decreased the occurrence of HO after THA when compared to placebo. However, there were no significant differences in the selective NSAIDs versus non-selective NSAIDs comparison [1].
A prevention protocol of 25 mg indomethacin was administered three times daily for 6 weeks following THA [13]. The same protocol prescribed for only 2 weeks yielded the same efficacy as 6 weeks of therapy [12]. More recently, 50 mg indomethacin administered two or three times daily showed good results for HO prevention [17, 20, 34]. Non-selective NSAID administration for 1 week was effective as well [3, 7, 36], even though some studies revealed a slightly increased risk of HO when the treatment period was shorter than 8 days [3, 16]. Other non-selective NSAIDs used for prophylaxis of HO after THA include ibuprofen and ketorolac. The efficacy of ibuprofen compared to placebo and indomethacin was evidenced in previous reports [37, 38]. The efficacy of ketorolac was analysed in a prospective, double-blind, randomized trial [39]. A total of 152 patients received 60 mg of ketorolac intraoperatively and 30 mg every 8 h for five doses postoperatively; another 151 patients received no prophylaxis for HO. There was significantly less HO in the ketorolac group. None of the patients developed clinically severe HO. A recent Bayesian network meta-analysis that included 26 studies and 6396 THAs demonstrated that prophylaxis with celecoxib was associated with the lowest rate of HO after THA, followed by prophylaxis with diclofenac and naproxen [40]. Celecoxib demonstrated the highest rate of Brooker class 0, followed by diclofenac. Naproxen demonstrated the lowest rate of Brooker I HO, followed by celecoxib. Celecoxib demonstrated the lowest rates of Brooker class II, class III, and class IV HO. On the other hand, tenoxicam, acetylsalicylic acid, and meloxicam were associated with the highest rates of HO following THA.
The present meta-analysis certainly has limitations. The small number of studies included and the heterogeneous drug administration protocols represent the most important limitations of the present study. The high variability in protocols increases the heterogeneity and may bias the conclusion of the present study. We used the modified Brooker staging system to rate the efficacy of the interventions. A limitation of this study is the relatively short length of the mean follow-up, which was shorter than 12 months. We must underline that, although HO formation is generally detectable early after surgery, its extent and Brooker grade cannot be definitively assessed until 12 months after surgery [40]. General health measures included were not reported. We did not consider the surgical approach used in THA in the various studies included, and this may be another risk of bias. The surgical approach used in THA may play an important role [41, 42]. Some studies have been conducted on the influence of the approach used in THA on HO formation [43]. The lowest incidence of HO formation was found after the posterior approach [43, 44]. Zran et al. [45] found a lower incidence of HO in patients undergoing a posterior approach (27.6%) compared to patients undergoing the direct lateral approach (47.7%). Alijanipour et al. [46] compared the direct anterior approach with the direct lateral approach and found a statistically significant greater rate of HO formation with the direct lateral approach. An important strength of our work is the type of study included, as seven of the eight studies were randomized controlled trials. Given these limitations, the results of the present study must be interpreted with caution.
Conclusion
Selective and non-selective NSAIDs were equally effective for the prevention of HO after THA.
Availability of data and materials
Not applicable.
References
Kan SL, Yang B, Ning GZ, Chen LX, Li YL, Gao SJ, Chen XY, Sun JC, Feng SQ (2015) Nonsteroidal anti-inflammatory drugs as prophylaxis for heterotopic ossification after total hip arthroplasty: a systematic review and meta-analysis. Medicine (Baltimore) 94(18):e828. https://doi.org/10.1097/MD.0000000000000828
Kienapfel H, Koller M, Wust A, Sprey C, Merte H, Engenhart-Cabillic R, Griss P (1999) Prevention of heterotopic bone formation after total hip arthroplasty: a prospective randomised study comparing postoperative radiation therapy with indomethacin medication. Arch Orthop Trauma Surg 119(5–6):296–302. https://doi.org/10.1007/s004020050414
Nilsson OS, Persson PE (1999) Heterotopic bone formation after joint replacement. Curr Opin Rheumatol 11(2):127–131. https://doi.org/10.1097/00002281-199903000-00008
Winkler S, Springorum HR, Vaitl T, Handel M, Barta S, Kehl V, Craiovan B, Grifka J (2016) Comparative clinical study of the prophylaxis of heterotopic ossifications after total hip arthroplasty using etoricoxib or diclofenac. Int Orthop 40(4):673–680. https://doi.org/10.1007/s00264-015-3077-z
Xue D, Zheng Q, Li H, Qian S, Zhang B, Pan Z (2011) Selective COX-2 inhibitor versus nonselective COX-1 and COX-2 inhibitor in the prevention of heterotopic ossification after total hip arthroplasty: a meta-analysis of randomised trials. Int Orthop 35(1):3–8. https://doi.org/10.1007/s00264-009-0886-y
Seegenschmiedt MH, Goldmann AR, Wolfel R, Hohmann D, Beck H, Sauer R (1993) Prevention of heterotopic ossification (HO) after total hip replacement: randomized high versus low dose radiotherapy. Radiother Oncol 26(3):271–274. https://doi.org/10.1016/0167-8140(93)90270-i
Grohs JG, Schmidt M, Wanivenhaus A (2007) Selective COX-2 inhibitor versus indomethacin for the prevention of heterotopic ossification after hip replacement: a double-blind randomized trial of 100 patients with 1-year follow-up. Acta Orthop 78(1):95–98. https://doi.org/10.1080/17453670610013484
Thomas BJ, Amstutz HC (1985) Results of the administration of diphosphonate for the prevention of heterotopic ossification after total hip arthroplasty. J Bone Jt Surg Am 67(3):400–403
van der Heide HJ, Spruit M, Slappendel R, Klooster N, van Limbeek J (2004) Prophylaxis for heterotopic ossification after primary total hip arthroplasty. A cohort study between indomethacin and meloxicam. Acta Orthop Belg 70(3):240–246
Ghlichloo I, Gerriets V (2021) Nonsteroidal anti-inflammatory drugs (NSAIDs). StatPearls, Treasure Island
Tozun R, Pinar H, Yesiller E, Hamzaoglu A (1992) Indomethacin for prevention of heterotopic ossification after total hip arthroplasty. J Arthroplasty 7(1):57–61. https://doi.org/10.1016/0883-5403(92)90033-m
Kjaersgaard-Andersen P, Nafei A, Teichert G, Kristensen O, Schmidt SA, Keller J, Lucht U (1993) Indomethacin for prevention of heterotopic ossification. A randomized controlled study in 41 hip arthroplasties. Acta Orthop Scand 64(6):639–642. https://doi.org/10.3109/17453679308994587
Schmidt SA, Kjaersgaard-Andersen P, Pedersen NW, Kristensen SS, Pedersen P, Nielsen JB (1988) The use of indomethacin to prevent the formation of heterotopic bone after total hip replacement. A randomized, double-blind clinical trial. J Bone Jt Surg Am 70(6):834–838
Vielpeau C, Joubert JM, Hulet C (1999) Naproxen in the prevention of heterotopic ossification after total hip replacement. Clin Orthop Relat Res 369:279–288. https://doi.org/10.1097/00003086-199912000-00029
Jockheck M, Willms R, Volkmann R, Sell S, Weller S, Kusswetter W (1998) Prevention of periarticular heterotopic ossification after endoprosthetic hip joint replacement by means of diclofenac. Arch Orthop Trauma Surg 117(6–7):337–340. https://doi.org/10.1007/s004020050261
Persson PE, Sodemann B, Nilsson OS (1998) Preventive effects of ibuprofen on periarticular heterotopic ossification after total hip arthroplasty. A randomized double-blind prospective study of treatment time. Acta Orthop Scand 69(2):111–115. https://doi.org/10.3109/17453679809117608
Barthel T, Baumann B, Noth U, Eulert J (2002) Prophylaxis of heterotopic ossification after total hip arthroplasty: a prospective randomized study comparing indomethacin and meloxicam. Acta Orthop Scand 73(6):611–614. https://doi.org/10.1080/000164702321039543
Laine L (2003) Gastrointestinal effects of NSAIDs and coxibs. J Pain Symptom Manage 25(2 Suppl):S32–40. https://doi.org/10.1016/s0885-3924(02)00629-2
Rahme E, Barkun AN, Adam V, Bardou M (2004) Treatment costs to prevent or treat upper gastrointestinal adverse events associated with NSAIDs. Drug Saf 27(13):1019–1042. https://doi.org/10.2165/00002018-200427130-00004
Romano CL, Duci D, Romano D, Mazza M, Meani E (2004) Celecoxib versus indomethacin in the prevention of heterotopic ossification after total hip arthroplasty. J Arthroplasty 19(1):14–18. https://doi.org/10.1016/s0883-5403(03)00279-1
Lavernia CJ, Contreras JS, Villa JM, Rossi MD (2014) Celecoxib and heterotopic bone formation after total hip arthroplasty. J Arthroplasty 29(2):390–392. https://doi.org/10.1016/j.arth.2013.06.039
Oni JK, Pinero JR, Saltzman BM, Jaffe FF (2014) Effect of a selective COX-2 inhibitor, celecoxib, on heterotopic ossification after total hip arthroplasty: a case-controlled study. Hip Int 24(3):256–262. https://doi.org/10.5301/hipint.5000109
Brunnekreef JJ, Hoogervorst P, Ploegmakers MJ, Rijnen WH, Schreurs BW (2013) Is etoricoxib effective in preventing heterotopic ossification after primary total hip arthroplasty? Int Orthop 37(4):583–587. https://doi.org/10.1007/s00264-013-1781-0
Xu BG, Xue DT, Wang XH, Yan SG (2014) Selective COX-2 inhibitor versus nonselective COX-1 and COX-2 inhibitor in the prevention of heterotopic ossification after total hip arthroplasty: a meta-analysis of randomised trials. Zhongguo Gu Shang 27(7):609–614
Saudan M, Saudan P, Perneger T, Riand N, Keller A, Hoffmeyer P (2007) Celecoxib versus ibuprofen in the prevention of heterotopic ossification following total hip replacement: a prospective randomised trial. J Bone Jt Surg Br 89(2):155–159. https://doi.org/10.1302/0301-620X.89B2.17747
Barbato M, D’Angelo E, Di Loreto G, Menna A, Di Francesco A, Salini V, Zoppi U, Cavasinni L, La Floresta P, Romano CL (2012) Adherence to routine use of pharmacological prophylaxis of heterotopic ossification after total hip arthroplasty: results from an Italian multicenter, prospective, observational survey. J Orthop Traumatol 13(2):63–67. https://doi.org/10.1007/s10195-012-0180-4
Legosz P, Otworowski M, Sibilska A, Starszak K, Kotrych D, Kwapisz A, Synder M (2019) Heterotopic ossification: a challenging complication of total hip arthroplasty: risk factors, diagnosis, prophylaxis, and treatment. Biomed Res Int 2019:3860142. https://doi.org/10.1155/2019/3860142
Whelton A (2002) COX-2-specific inhibitors and the kidney: effect on hypertension and oedema. J Hypertens Suppl 20(6):S31-35
Jones P, Lamdin R (2010) Oral cyclo-oxygenase 2 inhibitors versus other oral analgesics for acute soft tissue injury: systematic review and meta-analysis. Clin Drug Investig 30(7):419–437. https://doi.org/10.2165/11533350-000000000-00000
Howick JCI, Glasziou P, Greenhalgh T, Carl Heneghan, Liberati A, Moschetti I, Phillips B, Thornton H, Goddard O, Hodgkinson M (2011) The 2011 Oxford CEBM Levels of Evidence. Oxford Centre for Evidence-Based Medicine, Oxford. Available at https://www.cebmnet/indexaspx?o=5653.
van der Heide HJ, Koorevaar RC, Lemmens JA, van Kampen A, Schreurs BW (2007) Rofecoxib inhibits heterotopic ossification after total hip arthroplasty. Arch Orthop Trauma Surg 127(7):557–561. https://doi.org/10.1007/s00402-006-0243-1
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hrobjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372:n71. https://doi.org/10.1136/bmj.n71
Brooker AF, Bowerman JW, Robinson RA, Riley LH Jr (1973) Ectopic ossification following total hip replacement. Incidence and a method of classification. J Bone Jt Surg Am 55(8):1629–1632
Legenstein R, Bosch P, Ungersbock A (2003) Indomethacin versus meloxicam for prevention of heterotopic ossification after total hip arthroplasty. Arch Orthop Trauma Surg 123(2–3):91–94. https://doi.org/10.1007/s00402-003-0487-y
Reis HJ, Kusswetter W, Schellinger T (1992) The suppression of heterotopic ossification after total hip arthroplasty. Int Orthop 16(2):140–145. https://doi.org/10.1007/BF00180205
van der Heide HJ, Rijnberg WJ, Van Sorge A, Van Kampen A, Schreurs BW (2007) Similar effects of rofecoxib and indomethacin on the incidence of heterotopic ossification after hip arthroplasty. Acta Orthop 78(1):90–94. https://doi.org/10.1080/17453670610013475
Elmstedt E, Lindholm TS, Nilsson OS, Tornkvist H (1985) Effect of ibuprofen on heterotopic ossification after hip replacement. Acta Orthop Scand 56(1):25–27. https://doi.org/10.3109/17453678508992973
Sodemann B, Persson PE, Nilsson OS (1988) Prevention of heterotopic ossification by nonsteroid antiinflammatory drugs after total hip arthroplasty. Clin Orthop Relat Res 237:158–163
Pritchett JW (1995) Ketorolac prophylaxis against heterotopic ossification after hip replacement. Clin Orthop Relat Res 314:162–165
Migliorini F, Trivellas A, Eschweiler J, Driessen A, Tingart M, Maffulli N (2021) NSAIDs for prophylaxis for heterotopic ossification after total hip arthroplasty: a Bayesian network meta-analysis. Calcif Tissue Int 108(2):196–206. https://doi.org/10.1007/s00223-020-00763-7
Rockwood PR, Horne JG (1990) Heterotopic ossification following uncemented total hip arthroplasty. J Arthroplasty 5(Suppl):S43-46. https://doi.org/10.1016/s0883-5403(08)80024-1
Postel M (1975) Ossification. Rev Chir Orthop Reparatrice Appar Mot 61(Suppl 2):43–46
van Erp JHJ, Massier JRA, Truijen S, Bekkers JEJ, Snijders TE, de Gast A (2021) Heterotopic ossification in primary total hip arthroplasty using the posterolateral compared to the direct lateral approach. Arch Orthop Trauma Surg 141(7):1253–1259. https://doi.org/10.1007/s00402-021-03783-6
Morrey BF, Adams RA, Cabanela ME (1984) Comparison of heterotopic bone after anterolateral, transtrochanteric, and posterior approaches for total hip arthroplasty. Clin Orthop Relat Res 188:160–167
Zran N, Joseph E, Callamand G, Ohl X, Siboni R (2020) Heterotopic ossification after total hip arthroplasty: radiological comparison between a direct anterior approach without an orthopaedic table and a posterior approach. Hip Int. https://doi.org/10.1177/1120700020970793
Alijanipour P, Patel RP, Naik TU, Parvizi J (2017) Heterotopic ossification in primary total hip arthroplasty using the direct anterior vs direct lateral approach. J Arthroplasty 32(4):1323–1327. https://doi.org/10.1016/j.arth.2016.11.030
Acknowledgements
None.
Funding
Open Access funding enabled and organized by Projekt DEAL. The authors received no financial or material support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Contributions
FM: writing, revising, study selection, data collection, data extraction, synthesis methods, final approval; AP: writing, revising, study selection, data collection, data extraction, risk of study bias assessment, final approval; AB: writing, revising, final approval; TP: writing, revising, final approval; FH: writing, revising, risk of study bias assessment, final approval; NM: writing, revising, final approval. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
None.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Migliorini, F., Pintore, A., Baroncini, A. et al. Selective versus non-selective NSAIDs as prophylaxis for heterotopic ossification following hip arthroplasty: a meta-analysis. J Orthop Traumatol 23, 30 (2022). https://doi.org/10.1186/s10195-022-00646-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s10195-022-00646-7