
Abstract
Background
Social cognition refers to all mental operations to decipher information needed in social interactions. Here we aimed to outline the socio-cognitive profile of Chronic Migraine with Medication Overuse (CM + MO), given they are recognized to be at risk of socio-cognitive difficulties. Given the multidimensionality of this construct, we considered: (1) socio-cognitive abilities, (2) socio-cognitive beliefs, (3) alexithymia and autism traits, and (4) social relationships.
Methods
Seventy-one patients suffering from CM + MO, 61 from episodic migraine (EM), and 80 healthy controls (HC) were assessed with a comprehensive battery: (1) the Faux Pas test (FP), the Strange Stories task (SS), the Reading Mind in the Eyes test (RMET), (2) the Tromsø Social Intelligence Scale, (3) the Toronto Alexithymia Scale, the Autism Spectrum Quotient, (4) the Lubben Social Network Scale, the Friendship Scale.
Results
CM + MO: (1) performed similar to EM but worse than HC in the FP and SS, while they were worse than EM and HC in the RMET; (2) were similar to EM and HC in social intelligence; (3) had more alexithymic/autistic traits than EM and HC; (4) reported higher levels of contact with their family members but felt little support from the people around them than HC.
Conclusions
CM + MO results characterized by a profile of compromised socio-cognitive abilities that affects different dimensions. These findings may have a relevant role in multiple fields related to chronic headache: from the assessment to the management.
Similar content being viewed by others


Introduction
Migraine is among the most common and disabling neurological disorders [1]. In many sufferers, attacks recur less than 15 days/month (episodic migraine – EM), however in a small but significant portion of patients the disease evolves into a chronic pattern (chronic migraine—CM). Transition from EM to CM often occurs in association with a Medication Overuse (CM + MO) [2]. Current evidence suggests that psychological aspects may play a relevant role in CM, in particular in case of MO. Indeed, the existing association between CM + MO and psychopathologies [3-8]—which may have an impact on the outcome of treatment [9-12]- is well established. Moreover, most of the CM + MO patients tend to present alexithymia [13-15], i.e., a cognitive-affective disturbance affecting how individuals experience and express their internal states [16, 17].
Besides psychopathological comorbidities, additional factors have been emerging as linked to CM + MO. The biopsychosocial model suggests the existence of a complex interrelationship among biological, psychological, and psychosocial vulnerabilities [18]. Thus, the diversity in migraine expression results from the interplay among these factors, able to shape perceptions and response to disease [19].
When referring to psychosocial vulnerabilities, it is important to include also all those activity limitations and social-interactions restrictions being impacted by chronic pain [20]. Recent evidence showed an association between migraine and social cognitive functioning [21-23], whose decline could be responsible for dysfunctional social behaviors and personal distress. The term “social cognition” is a wide construct that refers to all mental operations that allow to decipher information about the intentions and affective states of social partners [24]. One of these social cognitive abilities is the capacity to infer one’s own and others’ mental states such as desires, emotions, and beliefs [25] (Theory of Mind, ToM).
In pediatric migraine [26-30], it has been showed an association between physical sickness and mental representation and way to think [31, 32], resulting in difficulties in expressing emotional states [33] and higher level of alexithymia [34, 35]. Less evidence is available in adult migraine. Bouteloup [21] comparing severe EM and CM patients with healthy controls (HC) found difficulties in the clinical populations in social and emotional cognition, which was explained as due to high alexithymic levels. Raimo [23] explored the neuropsychological correlates of ToM and found that CM patients had evident difficulties in the cognitive dimension involved in inferring other’s mental states. Romozzi [22] compared CM + MO, EM, and HC in complex emotion recognition, knowledge about one’s own and other person’s mental states, and alexithymic levels and found an impairment in all considered dimensions in CM + MO patients. Therefore, it appears that a dysfunction in social cognitive abilities may represent a critical characteristic of CM/CM + MO. The limited number of studies in adult samples calls for additional and more fine-grained investigations.
Regarding the ToM construct, one of the main distinctions refers to the affective (i.e., attributions regarding others' emotional mental states) and cognitive (i.e., knowledge of others' mental states such as beliefs, thoughts and intentions) components [36, 37]. One might expect these two components to be altered in CM + MO [21-23], but to what extent has not been explored yet. As socio-cognitive functioning also includes other aspects, such as difficulty in expressing one’s emotional states [33], what one thinks about one’s abilities in social situations [38], and the perception of social engagement [39], personal beliefs about social interactions represent a further field of investigation.
The present study aimed to characterize the socio-cognitive profile of CM + MO patients compared to EM and HC individuals by investigating four different aspects of social cognition: (a) affective and cognitive components of socio-cognitive abilities; (b) beliefs about one’s social cognitive functioning; (c) alexithymia and autism traits; (d) levels of social relationships experienced in everyday life. As in different clinical conditions [40, 41] association between social cognitive abilities and psychological distress and reduced quality of life (QoL) emerged, we also investigated this relationship. Our hypothesis is that CM + MO patients are characterized by a specific socio-cognitive profile that differentiate them from both EM and HC.
Methods
Participants
This is a cross-sectional case–control study conducted at the Headache Science and Neurorehabilitation Center (a tertiary referral center) of the Mondino Foundation in Pavia, Italy. We enrolled consecutive patients with stable (i.e., migraine duration ≥ 10 years) EM and patients with CM + MO. An expert neurologist verified the eligibility criteria during the recruitment process based on history, headache diaries, and neurological evaluation. A group of HC was enrolled as well and were community-based volunteers recruited from the general population. All participants completed a vocabulary test (drawn by Primary Mental Abilities test [42]) as a cognitive control variable of semantic knowledge. The study was approved by the Ethics Committee of San Matteo Hospital (Pavia, Italy) and written informed consent was obtained from all patients. Inclusion and exclusion criteria are reported in Table 1. The protocol followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines for cross-sectional investigations [43].
Procedure
Each consultation was performed by a headache expert that diagnosed the headache type, collected socio-demographic data, and migraine characteristics. Participants also underwent an interview with a psychologist during which they filled a series of tests and scales (a detailed description is reported below and in Table 2).
Socio-cognitive measures
Socio-cognitive abilities
Faux pas test (FP [44]; Italian version [45]) consisted of 4 short stories containing a faux pas assessing both the cognitive (i.e., False Beliefs) and the affective components of ToM.
Strange Stories task (SS [46]) consisted of 4 Mentalistic stories and 4 Physical stories. After having read the stories, participants were asked to answer the test question explaining the reasons why the characters behaved as they did.
Reading Mind in the Eyes Test (RMET [47]) consisted of 36 black-and-white photographs of the eye-region of the face, depicting a specific mental state. Participants were required to choose which one among four adjectives best described what the person in the photograph was feeling (experimental test) and to judge his/her gender (control test).
Socio-cognitive beliefs
Tromsø Social Intelligence Scale (TSIS [48]; Italian version [49]) was a self-report inventory including 21 items with three subscales: Social Information processing, Social Skills, and Social Awareness.
Alexithymia and autism traits
The presence of alexithymia was investigated using the 20-item version of the Toronto Alexithymia Scale (TAS-20; Italian version [50]) consisting of three factors: Factor 1, Factor 2, and Factor 3.
The presence of autistic traits was investigated using the Social Skills subscale of the Autism Spectrum Quotient (AQ [51]; Italian validation [52]).
Social relationships
Lubben Social Network Scale-Revised (LSNS-R [53]) was used to measure people’s social relationships with relatives and friends.
The Friendship Scale (FS [54]) was a 6-item scale assessing perceived social support.
Psychological and quality of life assessment
Levels of depression and anxiety were evaluated using the Hospital Anxiety and Depression Scale (HADS [55]) whereas QoL was assessed by using the World Health Organization Quality of Life Brief Version (WHOQOL-BREF [56]).
Statistical analyses
Performance on the FP was considered as primary outcome given it allows to assess both cognitive and affective components of socio-cognitive abilities. The sample size was calculated on this outcome, showing that a total of 206 participants was needed to discover an effect size of 0.25 with 0.90 statistical power and α = 0.05 in mixed ANOVA.
Data are presented as means ± SD for continuous data and n/% for frequency data. The differences between groups were examined with χ2 tests for categorical variables and analysis of variance (ANOVA) for quantitative variables. We first checked the equivalence of groups on demographic variables. We then examined group differences on socio-cognitive variables and psychological assessment with one-way and mixed Analysis of Covariance (ANCOVA). Then, we ran correlation analyses to examine the relationship between socio-cognitive and psychological variables for every separate diagnostic category. Two binary logistic regression models were performed to identify those socio-cognitive and psychological variables which best differentiate CM + MO patients from the other two groups (first model: CM + MO vs HC; second model: CM + MO vs EM). The criterion for predictors’ inclusion in the regression models was the existence of significant group differences at the level of p < 0.05 at univariate analysis.
Results
Study population
Two hundred and twelve subjects were enrolled (see descriptives in Table 1). We observed an older age in CM + MO than HC, whereas EM did not differ from the other two groups. No other significant differences between groups resulted in the demographic variables.
Socio-cognitive measures
Descriptives and statistics for socio-cognitive measures are reported in Table 3.
Socio-cognitive abilities
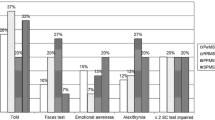
Looking at the FP, the analyses showed group differences for both the cognitive and the affective components. For the cognitive component, the HC group outperformed the group of EM, and for the affective component HC outperformed the CM + MO and EM groups.
For the SS, the analyses revealed group differences for the Mentalistic condition, with HC group outperforming the CM + MO and EM groups, and not for the Physical condition.
For the RMET, results showed group differences in the Experimental condition, with the HC and the EM groups outperforming the CM + MO group, and not for the Control condition. Detailed analyses are reported in Supplementary Table 1.
Socio-cognitive beliefs
Results did not show significant group differences nor in the TSIS total score neither in the subscales, ps ≥ 0.097.
Alexithymia and autism traits
Concerning alexithymia, analyses revealed significant group differences on the TAS-20 total score, F1, and F2 subscales. Post-hoc tests revealed that for the TAS-20 total score and F1 subscale, the CM + MOH group showed higher scores compared to the EM patient and HC group. For the F2 subscale, CM + MO group reported significantly higher scores compared to the HC group. No significant group differences emerged for the F3 subscale.
For the AQ test, results showed significant group differences: the CM + MO group had significantly higher scores compared to the EM patients and HC group.
Social relationships
Concerning the LSNS-R, analyses did not report significant group differences for the total score and friends’ subscale. Significant group differences emerged in the family subscale where CM + MO group showed significantly higher scores than the HC group.
No group differences emerged in the FS total score. However, looking at the frequency of participants falling in the category of low, moderate, and high social support, χ2 revealed significant group differences. The frequency of CM + MO patients falling in the low social support category was higher than the other two groups and the frequency of HC subjects falling into the moderate social support category was higher compared to CM + MO and EM patients.
Psychological and QoL assessment
Descriptives and statistics for Psychological and QoL assessment are reported in Table 3. Significant group differences were found in the HADS depression subscale and not in the HADS anxiety subscale, where the CM + MO group had significantly higher depression scores than the EM patient and HC group. Concerning QoL, group differences emerged in the WHOQOL-BREF where CM + MO group had significantly lower scores compared to the EM patient and HC group.
Correlation analyses
To verify whether socio-cognitive abilities were associated with the other variables in which group differences were found, we ran correlation analyses separately for each group (see Table 4). For the CM + MO group, the Mentalistic SS correlated negatively with the AQ and the HADS depression subscale, and positively with the FS categories and the WHOQOL-BREF. Regarding the EM group, the Mentalistic SS correlated negatively with the AQ and HADS depression subscale, and positively with the LSNS-R family subscale. For the HC group, the FP Cognitive component correlated positively with the LSNS-R family subscale. No other correlations were found.
Predictors of CM + MO
The binary logistic regression models’ results are summarized in Table 5.
For the first model, significant predictors that increased the odds to be in the CM + MO group than the HC group were: lower performance in the FP Affective component and the RMET experimental condition, lower prevalence of moderate social support in the LS, higher scores in the family subscale of the LSNS-R, and lower scores in the WHOQOL-BREF. This logistic regression model was statistically significant and it explained 65% (Nagelkerke R2) of the variance. This model correctly classified 90% of the CM + MO patients, and 90% of the HC group.
In the second model, significant predictors that increased the odds to be in the CM + MO group than the EM group were lower performance in the RMET Experimental condition, lower scores in the WHOQOL-BREF, and higher score in the AQ. The model was statistically significant and it explained 42% (Nagelkerke R2) of the variance. This model correctly classified 87.1% of the CM + MO patients, and 62.2% of the EM patients.
Discussion
The present study aimed to outline the socio-cognitive profile of CM + MO. For what concerns socio-cognitive abilities, we had two interesting findings. First, when looking at the differences across socio-cognitive components, a more evident impairment resulted in the affective dimension for CM + MO patients. Second, the HC outperformed both migraine groups, which resulted almost always – with the only exception of the RMET – similar to each other. Such a similitude between CM + MO and EM populations is not surprising if we consider that they represent two different expressions of the same disease. In addition, our EM population had a long history of disease, which was serious enough to push them to seek care in a tertiary referral center. Thus, it is possible that a long exposure to a disabling pain condition may have affected patients’ ability to infer others’ mental states. However, although the two migraine groups were similar in several aspects, a more marked impairment resulted for those with CM + MO with respect to EM in the affective dimension of socio-cognitive abilities. Such results are partially in contrast with Raimo [23] that showed slightly greater difficulties of CM for the cognitive component than the affective one. However, in that study [23], CM patients were compared only with HC, and not with EM as we did. We believe that these affective difficulties should be considered in light of the greater levels of alexithymic and autism traits characterizing CM + MO. Autism research has shown that difficulties in identifying and describing feelings are associated to impairments in recognizing verbal and non-verbal emotional expressions [57-59], and difficulties in experiencing and understanding emotions [60].
Regarding socio-cognitive beliefs, a new topic in migraine research, we found no differences between groups in participants’ perception of how successfully they manage social relationships [61]. Our data for the three groups are in line with the norms of TSIS [48], suggesting that all participants had positive beliefs about their social abilities. If we consider this result in light of the group differences found in the performances, it could be argued that CM + MO patients did not have a clear awareness of their socio-cognitive competencies.
Regarding alexithymia, our results, as found in the literature [13-15], showed an impairment in CM + MO. It corroborates the idea that alexithymia represents a risk factor increasing susceptibility to disease [62]. This is also supported by the differences across groups we found in the autism traits, since it exists a strong association between alexithymic and autism traits, which could be explained by shared characteristics [63, 64]. It is important to consider that these aspects are critical for successful social interactions in everyday life [65]. Interestingly, the CM + MO patients differed significantly from EM and HC individuals in a specific alexithymic facet, which is the difficulty in identifying feelings and distinguishing between feelings and the bodily sensations. Indeed, individuals with high levels of alexithymic traits experience difficulties also for what concerns their non-affective interoceptive state [66]. The inaccurate identification of their bodily sensations [60] could determine a delay in seeking medical treatment [67] and favor substance use disorders [68]. In conclusion, more marked group differences in this alexithymic trait in disfavor of the CM + MO group seems to corroborate previous findings on non-affective interoceptive deficits [66], and may explain MO.
Data regarding social relationships are particularly interesting. On the one hand, we found that the CM + MO group reported higher levels of contact with their family members than the HC did, highlighting chronic patients’ need to maximize the interactions with their relatives. On the other hand, these same patients perceived that they were little supported from the people around them. These findings, although they might seem at odds, actually further highlight patients’ social difficulties. The topic of social relationships in migraine is much debated. There is evidence reporting that migraine patients are less satisfied with social support than the general population [69-71]. Belot [71] found that patients with severe migraine judged the social support they received worse than the general population did. Others [72] reported that poor social support and loneliness in CM were associated with a tendency to MO. Our research group [73] has also shown that both CM and EM patients felt emotionally lonely and less supported than HC after the COVID-19 outbreak. By contrast, it has been shown that headache sufferers had slightly more social support from their families than non-headaches sufferers [74]. Hence, it is difficult to draw definitive conclusions given the heterogeneity of the clinic populations [69-72, 74]. Moreover, these social difficulties should be interpreted at the light of the stigma experienced by CM + MO patients, perceiving a sort of discrimination against their health condition [75-77]. Indeed, our results suggest that CM + MO patients place importance on tangible support from their family members, although they do not feel much satisfied with the support received from social networks [69, 78, 79].
As the importance of socio-cognitive components in defining patients’ profile, we also searched for variables that may predict CM + MO. Patients scored lower in two affective socio-cognitive abilities tests, reported lower prevalence of moderate vs high social support, higher levels of contacts with family members, and lower QoL when compared with HC. It may be that chronic pain has affected social interactions, making patients less adept at inferring others’ mental states. It may also be that long-standing migraine has resulted in less interest in others’ mental and affective states, which in turn may have caused a reduction of social interactions. Both interpretations can be taken as true, in a circular relationship, according to the biopsychosocial model [19].
A similar pattern, albeit less pronounced, was found in the second logistic regression analysis: CM + MO was predicted by lower performances in the ability to infer others’ affective state from looking at the eyes, higher levels of autism traits, and lower QoL than EM. Even if the two migraine groups resulted similar in many socio-cognitive aspects, CM + MO patients were found to be more affected and with lower well-being due to their clinical condition, with negative consequences on understanding others. These factors may act together and predispose the development of this complex clinical condition.
Our study is not without limitations. First, we have not included a screening scale of cognitive functioning and we did not control for prophylaxis treatment that may have impact on cognition, such as topiramate [80]. However, it should be noted that we assessed participants’ semantic knowledge as a cognitive control variable that was previously associated with better performance in socio-cognitive abilities [81, 82]. Moreover, the fact itself that CM + MO showed a differentiated pattern of performance in socio-cognitive abilities, being more impaired in the affective that in the cognitive dimension, could allow us to exclude a generalized deficit due to pharmacological treatments. Second, we did not collect a comprehensive psychopathological assessment. However, we believe that it is important to focus on additional components beside psychopathologies [3-8]. Third, since this was a cross-sectional study, we are unable to define the causal trajectory involving socio-cognitive components in CM + MO. Fourth, because we did not include a group of CM patients without MO, we cannot definitively conclude that the impairment of social cognition we found is a critical feature of CM + MO rather than CM alone. Sixth, the data collection procedure did not reflect the general migraine population, as participants were recruited from a tertiary referral center. Therefore, the transferability of these results to general practice will require confirmation on larger subgroups of patients, in multicenter studies, and with different cultures.
Conclusions
Among the causal aspects that could determine the transition to chronic migraine, we believe that a critical role should be attributed to socio-cognitive factors. Specifically, our results showed that socio-cognitive abilities, traits of alexithymia and autism, and a particular pattern of social relationships are associated with CM + MO. From a theoretical point of view, our data add an important element to the identification of risk factors for the development of this disabling condition. From a practical point of view, they have a multifold relevance: i) they provide tangible data on the social impairments associated to the condition of EM and, even more severely, of CM + MO and ii) they underscore the importance of optimizing the management of patients through a thorough preliminary assessment of their socio-cognitive profile; ii) they call for adequate public health interventions to prevent the evolution of EM into CM + MO.
Availability of data and materials
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: [Zenodo; Reservation 10.5281zenodo.7713963].
Abbreviations
- ANCOVA:
-
Analysis of Covariance
- ANOVA:
-
Analysis of Variance
- AQ:
-
Autism Spectrum Quotient
- CM:
-
Chronic Migraine
- EM:
-
Episodic Migraine
- FP:
-
Faux Pas test
- FS:
-
Friendship Scale
- HADS:
-
Anxiety and Depression Scale
- HC:
-
Healthy Control
- LSNS-R:
-
Lubben Social Network Scale-Revised
- MO:
-
Medication Overuse
- NSAIDs:
-
nonsteroidal anti-inflammatory drugs
- QoL:
-
Quality of Life
- RMET:
-
Reading Mind in the Eyes Test
- SS:
-
Strange Stories task
- STROBE:
-
Strengthening the Reporting of Observational Studies in Epidemiology
- TAS-20:
-
Toronto Alexithymia Scale
- ToM:
-
Theory of Mind
- TSIS:
-
Tromsø Social Intelligence Scale
- WHOQOL-BREF:
-
World Health Organization Quality of Life Brief Version
References
Vos T, Lim SS, Abbafati C et al (2020) Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 396:1204–1222. https://doi.org/10.1016/S0140-6736(20)30925-9
Olesen J (2018) Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia 38:1–211
Viana M, Bottiroli S, Sances G et al (2018) Factors associated to chronic migraine with medication overuse : A cross-sectional study. Cephalalgia 38:2045–2057. https://doi.org/10.1177/0333102418761047
Bottiroli S, Galli F, Ballante E, et al (2021) Validity of the severity of dependence scale for detecting dependence behaviours in chronic migraine with medication overuse. Cephalalgia 033310242110398. https://doi.org/10.1177/03331024211039817
Galli F, Tanzilli A, Simonelli A, et al (2019) Personality and personality disorders in medication-overuse headache: a controlled study by SWAP-200. Pain Res Manag 2019. https://doi.org/10.1155/2019/1874078
Sances G, Galli F, Anastasi S et al (2010) Medication-overuse headache and personality: A controlled study by means of the MMPI-2: Research submission. Headache 50:198–209. https://doi.org/10.1111/j.1526-4610.2009.01593.x
Sances G, Galli F, Ghiotto N, et al (2013) Factors associated with a negative outcome of medication-overuse headache: a 3-year follow-up (the ‘CARE’ protocol). 0:1–13. https://doi.org/10.1177/0333102413477737
Baskin SM, Lipchik GL, Smitherman TA (2006) Mood and Anxiety Disorders in Chronic Headache. Headache J Head Face Pain 46:S76–S87. https://doi.org/10.1111/j.1526-4610.2006.00559.x
Bottiroli S, Allena M, Sances G et al (2019) Psychological, clinical, and therapeutic predictors of the outcome of detoxification in a large clinical population of medication-overuse headache: A six-month follow-up of the COMOESTAS Project. Cephalalgia 39:135–147. https://doi.org/10.1177/0333102418783317
Bottiroli S, Viana M, Sances G et al (2016) Psychological factors associated with failure of detoxification treatment in chronic headache associated with medication overuse. Cephalalgia 36:1356–1365. https://doi.org/10.1177/0333102416631960
Bottiroli S, Galli F, Viana M et al (2019) Negative short-term outcome of detoxification therapy in chronic migraine with medication overuse headache: Role for early life traumatic experiences and recent stressful events. Front Neurol 10:1–11. https://doi.org/10.3389/fneur.2019.00173
Bottiroli S, De Icco R, Vaghi G et al (2021) Psychological predictors of negative treatment outcome with Erenumab in chronic migraine: data from an open label long-term prospective study. J Headache Pain 22:114. https://doi.org/10.1186/s10194-021-01333-4
Galli F, Caputi M, Sances G et al (2017) Alexithymia in chronic and episodic migraine: a comparative study. J Ment Heal 26:192–196. https://doi.org/10.3109/09638237.2015.1124404
Ghiggia A, Bottiroli S, Lingiardi V et al (2022) Alexithymia and psychological distress in fibromyalgia and chronic migraine: a cross-sectional study. J Psychosom Res 163:111048. https://doi.org/10.1016/j.jpsychores.2022.111048
Bottiroli S, Galli F, Viana M et al (2018) Traumatic experiences, stressful events, and alexithymia in chronic migraine with medication overuse. Front Psychol 9:1–9. https://doi.org/10.3389/fpsyg.2018.00704
Griffith JL (1998) Disorders of affect regulation: alexithymia in medical and psychiatric illness. Psychosomatics 39:554–555. https://doi.org/10.1016/s0033-3182(98)71291-5
Taylor GJ (2000) Recent developments in alexithymia theory and research. Can J Psychiatry 45:134–142
Andrasik F, Flor H, Turk DC (2005) An expanded view of psychological aspects in head pain: the biopsychosocial model. Neurol Sci 26:s87–s91. https://doi.org/10.1007/s10072-005-0416-7
Rosignoli C, Ornello R, Onofri A et al (2022) Applying a biopsychosocial model to migraine: rationale and clinical implications. J Headache Pain 23:100. https://doi.org/10.1186/s10194-022-01471-3
Raggi A, Giovannetti AM, Quintas R et al (2012) A systematic review of the psychosocial difficulties relevant to patients with migraine. J Headache Pain 13:595–606. https://doi.org/10.1007/s10194-012-0482-1
Bouteloup M, Belot R-A, Noiret N et al (2021) Social and emotional cognition in patients with severe migraine consulting in a tertiary headache center: A preliminary study. Rev Neurol (Paris) 177:995–1000. https://doi.org/10.1016/j.neurol.2020.09.013
Romozzi M, Di Tella S, Rollo E, et al (2022) Theory of mind in migraine and medication-overuse headache: a cross-sectional study. Front Neurol 13. https://doi.org/10.3389/fneur.2022.968111
Raimo S, D’Onofrio F, Gaita M et al (2022) Neuropsychological correlates of theory of mind in chronic migraine. Neuropsychology 36:753–763. https://doi.org/10.1037/neu0000852
Beaudoin C, Beauchamp MH (2020) Social cognition. pp 255–264
Premack D, Woodruff G (1978) Does the chimpanzee have a theory of mind? Behav Brain Sci 1:515–526. https://doi.org/10.1017/S0140525X00076512
Faedda N, Natalucci G, Calderoni D, et al (2017) Metacognition and headache: which is the role in childhood and adolescence? Front Neurol 8. https://doi.org/10.3389/fneur.2017.00650
Natalucci G, Faedda N, Quinzi A, et al (2019) Alexithymia, metacognition, and theory of mind in children and preadolescents with migraine without aura (MWoA): a case-control study. Front Neurol 10. https://doi.org/10.3389/fneur.2019.00774
Natalucci G, Faedda N, Quinzi A et al (2019) Metacognition and theory of mind in children with migraine and children with internalizing disorders. Neurol Sci 40:187–189. https://doi.org/10.1007/s10072-019-03805-7
Operto FF, Scuoppo C, Padovano C et al (2022) Migraine and epilepsy: Social cognition skills in pediatric population. Eur J Paediatr Neurol 37:68–74. https://doi.org/10.1016/j.ejpn.2022.01.011
La Grutta S, Lo Baido R, Schiera G et al (2007) Symbolic function explored in children with epilepsy and headache. Minerva Pediatr 59:745–754
Tietjen GE, Buse DC, Fanning KM et al (2014) Recalled maltreatment, migraine, and tension-type headache results of the AMPP study. pp 132–140
Tietjen GE (2016) Childhood maltreatment and headache disorders. Curr Pain Headache Rep 20:26. https://doi.org/10.1007/s11916-016-0554-z
Mazzone L, Vitiello B, Incorpora G, Mazzone D (2006) Behavioural and temperamental characteristics of children and adolescents suffering from primary headache. Cephalalgia 26:194–201. https://doi.org/10.1111/j.1468-2982.2005.01015.x
Gatta M, Canetta E, Zordan M, et al (2011) Alexithymia in juvenile primary headache sufferers: a pilot study. 71–80. https://doi.org/10.1007/s10194-010-0248-6
Cerutti R, Valastro C, Tarantino S et al (2016) Alexithymia and psychopathological symptoms in adolescent outpatients and mothers suffering from migraines: a case control study. J Headache Pain 17:39. https://doi.org/10.1186/s10194-016-0640-y
Shamay-Tsoory SG, Shur S, Barcai-Goodman L et al (2007) Dissociation of cognitive from affective components of theory of mind in schizophrenia. Psychiatry Res 149:11–23. https://doi.org/10.1016/j.psychres.2005.10.018
Shamay-Tsoory SG, Aharon-Peretz J (2007) Dissociable prefrontal networks for cognitive and affective theory of mind: a lesion study. Neuropsychologia 45:3054–3067. https://doi.org/10.1016/j.neuropsychologia.2007.05.021
Dimaggio G, Lysaker PH (2015) Metacognition and Mentalizing in the Psychotherapy of Patients With Psychosis and Personality Disorders. J Clin Psychol 71:117–124. https://doi.org/10.1002/jclp.22147
Schneider M, Myin E, Myin-Germeys I (2020) Is theory of mind a prerequisite for social interactions? A study in psychotic disorder. Psychol Med 50:754–760. https://doi.org/10.1017/S0033291719000540
Bourke JH, Langford RM, White PD (2015) The common link between functional somatic syndromes may be central sensitisation. J Psychosom Res 78:228–236. https://doi.org/10.1016/j.jpsychores.2015.01.003
Luyten P, van Houdenhove B, Lemma A et al (2012) A mentalization-based approach to the understanding and treatment of functional somatic disorders. Psychoanal Psychother 26:121–140. https://doi.org/10.1080/02668734.2012.678061
Thurstone LL, Thurstone TG (1963) Primary mental abilities. Science Research, Chicago
von Elm E, Altman DG, Egger M et al (2007) The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Ann Intern Med 147:573–577. https://doi.org/10.7326/0003-4819-147-8-200710160-00010
Stone VE, Baron-cohen S, Knight RT (1995) Frontal lobe contributions to theory of mind. pp 640–656
Liverta Sempio O, Marchetti A, & Lecciso F (2008) Faux pas: traduzione italiana. Department of Psychology, Catholic University of the Sacred Heart, Milan
White S, Hill E, Happé F, Frith U (2009) Revisiting the strange stories: revealing mentalizing impairments in autism. Child Dev 80:1097–1117. https://doi.org/10.1111/j.1467-8624.2009.01319.x
Baron-Cohen S, Wheelwright S, Hill J et al (2001) The “Reading the Mind in the Eyes” Test revised version: a study with normal adults, and adults with Asperger syndrome or high-functioning autism. J Child Psychol Psychiatry 42:241–251
Silvera D, Martinussen M, Dahl TI (2001) The Tromsø Social Intelligence Scale, a self-report measure of social intelligence. Scand J Psychol 42:313–319. https://doi.org/10.1111/1467-9450.00242
Gini G, Iotti G (2008) Una misura multidimensionale dell’intelligenza sociale: validazione preliminare della versione italiana della Tromsø Social Intelligence Scale. G Ital di Psicol 35:665–678
Bressi C, Taylor G, Parker J et al (1996) Cross validation of the factor structure of the 20-item Toronto Alexithymia Scale: an Italian multicenter study. J Psychosom Res 41:551–559. https://doi.org/10.1016/S0022-3999(96)00228-0
Baron-Cohen S, Wheelwright S, Skinner R et al (2001) The Autism-Spectrum Quotient (AQ): Evidence from Asperger Syndrome/high-functioning autism, males and females, scientists and mathematicians. J Autism Dev Disord 31:5–17. https://doi.org/10.1023/A:1005653411471
Ruta L, Mazzone D, Mazzone L et al (2012) The Autism-spectrum quotient—Italian version: a cross-cultural confirmation of the broader autism phenotype. J Autism Dev Disord 42:625–633. https://doi.org/10.1007/s10803-011-1290-1
Lubben J, Gironda M (2004) Measuring social networks and assessing their benefits. In: Phillipson C, Allan G, Morgan DA (eds) Social Networks and Social Exclusion: Sociological and Policy Perspectives. Ashgate Publishing Limited, Hant, p 2035
Hawthorne G (2006) Measuring social isolation in older adults: development and initial validation of the friendship scale. Soc Indic Res 77:521–548. https://doi.org/10.1007/s11205-005-7746-y
Upadhyaya AK, Stanley I (1993) Hospital anxiety depression scale. Br J Gen Pract 43:349–350
THE Whoqol GROUP (1998) Development of the World Health Organization WHOQOL-BREF Quality of Life Assessment. Psychol Med 28:551–558. https://doi.org/10.1017/S0033291798006667
Heaton P, Reichenbacher L, Sauter D et al (2012) Measuring the effects of alexithymia on perception of emotional vocalizations in autistic spectrum disorder and typical development. Psychol Med 42:2453–2459. https://doi.org/10.1017/S0033291712000621
Oakley BFM, Jones EJH, Crawley D et al (2022) Alexithymia in autism: cross-sectional and longitudinal associations with social-communication difficulties, anxiety and depression symptoms. Psychol Med 52:1458–1470. https://doi.org/10.1017/S0033291720003244
Cook R, Brewer R, Shah P, Bird G (2013) Alexithymia, not autism, predicts poor recognition of emotional facial expressions. Psychol Sci 24:723–732. https://doi.org/10.1177/0956797612463582
Herbert BM, Herbert C, Pollatos O (2011) On the relationship between interoceptive awareness and alexithymia: is interoceptive awareness related to emotional awareness? J Pers 79:1149–1175. https://doi.org/10.1111/j.1467-6494.2011.00717.x
Friborg O, Barlaug D, Martinussen M et al (2005) Resilience in relation to personality and intelligence. Int J Methods Psychiatr Res 14:29–42. https://doi.org/10.1002/mpr.15
Weiner H (1982) Contributions of psychoanalysis to psychosomatic medicine. J Am Acad Psychoanal 10:27–46. https://doi.org/10.1521/jaap.1.1982.10.1.27
Shah P, Hall R, Catmur C, Bird G (2016) Alexithymia, not autism, is associated with impaired interoception. Cortex 81:215–220. https://doi.org/10.1016/j.cortex.2016.03.021
Nicholson TM, Williams DM, Grainger C et al (2018) Interoceptive impairments do not lie at the heart of autism or alexithymia. J Abnorm Psychol 127:612–622. https://doi.org/10.1037/abn0000370
Trevisan DA, Bowering M, Birmingham E (2016) Alexithymia, but not autism spectrum disorder, may be related to the production of emotional facial expressions. Mol Autism 7:46. https://doi.org/10.1186/s13229-016-0108-6
Brewer R, Cook R, Bird G (2016) Alexithymia: a general deficit of interoception. R Soc Open Sci 3:150664. https://doi.org/10.1098/rsos.150664
Carta MG, Sancassiani F, Pippia V et al (2013) Alexithymia is associated with delayed treatment seeking in acute myocardial infarction. Psychother Psychosom 82:190–192. https://doi.org/10.1159/000341181
de Haan HA, van der Palen J, Wijdeveld TGM et al (2014) Alexithymia in patients with substance use disorders: State or trait? Psychiatry Res 216:137–145. https://doi.org/10.1016/j.psychres.2013.12.047
Martin PR, Soon K (1993) The relationship between perceived stress, social support and chronic headaches. Headache J Head Face Pain 33:307–314. https://doi.org/10.1111/j.1526-4610.1993.hed3306307.x
Blomkvist V, Hannerz J, Katz L, Theorell T (2002) Coping style and social support in men and women suffering from cluster headache or migraine. Headache J Head Face Pain 42:178–184. https://doi.org/10.1046/j.1526-4610.2002.02049.x
Belot R-A, Bouteloup M, Bonnet M, et al (2021) Evaluation of attachment style and social support in patients with severe migraine. Applications in doctor-patient relationships and treatment adherence. Front Neurol 12. https://doi.org/10.3389/fneur.2021.706639
Westergaard ML, Lau CJ, Allesøe K et al (2021) Poor social support and loneliness in chronic headache: Prevalence and effect modifiers. Cephalalgia 41:1318–1331. https://doi.org/10.1177/03331024211020392
Cerami C, Crespi C, Bottiroli S et al (2021) High perceived isolation and reduced social support affect headache impact levels in migraine after the Covid-19 outbreak: a cross sectional survey on chronic and episodic patients. Cephalalgia 41:1437–1446. https://doi.org/10.1177/03331024211027568
Teoh H, Tam C (2008) A comparison of headache and non-headache sufferers on measures of social support and mental health problems. Malaysian Fam physician Off J Acad Fam Physicians Malaysia 3:82–86
Perugino F, De Angelis V, Pompili M, Martelletti P (2022) Stigma and chronic pain. Pain Ther 11:1085–1094. https://doi.org/10.1007/s40122-022-00418-5
Gross E, Ruiz de la Torre E, Martelletti P (2023) The migraine stigma kaleidoscope view. Neurol Ther. https://doi.org/10.1007/s40120-023-00456-x
Shimizu T, Sakai F, Miyake H et al (2021) Disability, quality of life, productivity impairment and employer costs of migraine in the workplace. J Headache Pain 22:29. https://doi.org/10.1186/s10194-021-01243-5
Martin PR, Theunissen C (1993) The role of life event stress, coping and social support in chronic headaches. Headache J Head Face Pain 33:301–306. https://doi.org/10.1111/j.1526-4610.1993.hed3306301.x
Martin R, Davis GM, Baron RS et al (1994) Specificity in social support: Perceptions of helpful and unhelpful provider behaviors among irritable bowel syndrome, headache, and cancer patients. Heal Psychol 13:432–439. https://doi.org/10.1037/0278-6133.13.5.432
Thompson PJ (2000) Effects of topiramate on cognitive function. J Neurol Neurosurg Psychiatry 69:636–641. https://doi.org/10.1136/jnnp.69.5.636
Li X, Wang K, Wang F et al (2013) Aging of theory of mind: the influence of educational level and cognitive processing. Int J Psychol 48:715–727. https://doi.org/10.1080/00207594.2012.673724
Szepietowska EM, Filipiak S (2021) Interpretation of familiar metaphors and proverbs by Polish people in middle and late adulthood. Int J Lang Commun Disord 56:841–857. https://doi.org/10.1111/1460-6984.12631
Acknowledgements
This study was supported by the Italian Ministry of Health (Bando di Ricerca Finalizzata Giovani Ricercatori 2016, GR-2016-02363848). The study funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Contributions
SB performed patient’s socio-cognitive evaluations, while RDI, MA, and GS performed clinical evaluations for enrollment. SB and AR did statistical analyses and interpreted results. SB, AR wrote the first draft. EC and CT performed revisions. All authors contributed to the planning and development of the study, supervised by EC, AM, and CT. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was performed in accordance with the guidelines of the Declaration of Helsinki. Authors obtained local ethics committee (San Matteo Hospital, Pavia, Italy—reference code p-20170016073) approval of the protocol. All patients provided written informed consent in advance of study participation.
Consent for publication
Not applicable.
Competing interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CT received honoraria for the participation in advisory boards or for lecturing from: Allergan, Eli-Lilly, Novartis, and Teva. CT and GS has no ownership interest and does not own stocks of any pharmaceutical company. CT is on the editorial board of The Journal of Headache and Pain. GS received honoraria for the participation in advisory boards or for lecturing from: Eli-Lilly, Novartis, and Teva. The remaining authors have no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
STROBE Statement—checklist of items that should be included in reports of observational studies.
Additional file 2: Table S1.
Correlation between socio-cognitive abilities and other variables in which we found group differences, separately for each group.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Bottiroli, S., Rosi, A., Sances, G. et al. Social cognition in chronic migraine with medication overuse: a cross-sectional study on different aspects of mentalization and social relationships. J Headache Pain 24, 47 (2023). https://doi.org/10.1186/s10194-023-01578-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s10194-023-01578-1