
Abstract
Cardiac metastasis of germ cell tumors is extremely rare, particularly in females. We report a case of a 26-year-old previously healthy woman who presented with a 5-month history of abdominal pain, weight loss, fever, generalized lymphadenopathy, and acanthosis nigricans. Biopsy of cervical lymph nodes revealed a poorly differentiated neoplasm. Immunohistochemical staining was positive for alpha-fetoprotein suggesting the diagnosis of a germ cell tumor. During the investigation, the patient developed heart failure and a mass attached to the right ventricle was detected by the echocardiogram. In a few days, she developed multiple organ failure and died. Post-mortem examination revealed a malignant mixed germ cell tumor of the right ovary with extensive hematogenic and lymphatic dissemination, a polypoid mass attached to the right ventricle, emboli in the endocardial and epicardial vessels, and infiltration surrounding the coronary arteries. To the best of our knowledge this is the third report of grossly visible heart metastases from a yolk sac tumor in a female patient. A summary of all published cases of germ cell tumors with cardiac metastasis over the last 20 years is also presented.
Similar content being viewed by others


Background
Ovarian germ cell neoplasm includes tumors with multiple histological patterns, and variable biologic behaviors [1]. These tumors grow rapidly, are usually unilateral and confined to one ovary in two thirds of the cases, and predominate in girls and young women. Mixed germ cell tumors consist of two or more admixed types of ovarian germ cell neoplasms and account for 5.3% of all malignant ovarian germ cell tumors [2]. Components of dysgerminoma mixed with endodermal sinus tumor (also called yolk sac tumors) are found most commonly. As a highly malignant neoplasm, yolk sac tumors metastasize at an early stage as well invade the surrounding structures and organs [1, 3–6].
Although cardiac metastases can arise from different cancers, they are more frequently associated with carcinoma of the lung, breast and esophagus (due to the higher prevalence of these tumors), hematological malignancies including lymphoma and leukemia, and malignant melanoma, which shows the highest affinity to metastasize to the heart [4]. Cardiac metastasis of germ cell tumors is extremely rare, particularly in the female gender. We hereby report a case of a 26-year-old woman with mixed germ cell tumor of the right ovary who presented with widespread metastases including to the right ventricle. Post-mortem examination also showed neoplastic emboli in the endocardial and epicardial vessels and infiltration surrounding the coronary arteries.
Case presentation
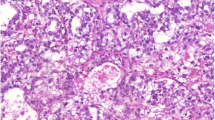
A 26-year-old previously health woman presented with a 5-month history of abdominal pain, weight loss, fever, generalized lymphadenopathy, and acanthosis nigricans. Except for anemia (hemoglobin 11.1 g/dl), blood counts were within the normal ranges. Serological tests for human immunodeficiency virus (HIV), hepatitis viruses, syphilis, toxoplasmosis and cytomegalovirus were negative. Blood chemistry was unremarkable, and blood and urine cultures were negative. Thoracic, abdominal and pelvic computed tomography (CT) showed extensive lymphadenopathy and a solid mass with ill-defined borders near the uterus. The ovaries were not seen. Biopsy of cervical lymph nodes revealed a poorly differentiated neoplasm. Immunohistochemical staining was positive for alpha-fetoprotein suggesting the diagnosis of a germ cell tumor. During the investigation, the patient developed heart failure. A transthoracic echocardiography showed right ventricular (RV) dilatation, pericardial effusion, and a mobile mass attached to the endocardial surface of the apex of the RV (Figure 1, panel A). In the following days, she developed multiple organ failure and died before she could be subjected to any type of anticancer treatment. Post-mortem examination revealed a malignant mixed germ cell tumor of the right ovary with predominance of endodermal sinus (yolk sac) tumor elements, and extensive hematogenic and lymphatic dissemination to the lungs, kidneys, liver, intestines, uterine tube, mediastinum, and thyroid gland. A polypoid mass was found attached to the apex of the RV (Figure 1, panels B and C). Neoplastic emboli in the endocardial and epicardial vessels, and infiltration surrounding the coronary arteries were also detected (Figure 1, panel D).

Cardiac involvement by the tumor. A: Image from transthoracic echocardiogram showing a mass attached to the apex of the right ventricle with a pericardial effusion (white arrow). RV = right ventricle; RA = right atrium; LV = left ventricle; LA = left atrium; PE = pericardial effusion. B: Photography derived from the autopsy showing opened right ventricle with a mass attached to the endocardial surface of the right ventricle (white arrow). RV = right ventricle. C: Polypoid cardiac mass (× 250) (black arrow). D: Emboli of neoplastic cells in myocardial and endocardial vessels (× 400) (black arrows).
The guardian of the patient provided written informed consent in accordance with the Declaration of Helsinki.
Conclusions
Intracardiac metastasis is an extremely rare manifestation of germ cell tumors. It occurs by hematogenous spread, direct invasion from neighboring chest tumors or through the pericardial space, usually to the right side of the heart [3–6]. In our case, the neoplastic cells probably reached the heart hematogenously, through the inferior vena cava. Although there were mediastinal metastases, they did not present any continuity with the cardiac lesions.
In a review of the cases of germ cell tumors with cardiac metastasis published over the last 20 years (Table 1) [7–24] we found 17 cases: 16 of them were male with testicular seminoma or nonseminomatous germ cell tumor, and only one case of a yolk sac tumor was reported in a female child of 18 months old. In 11 of these reported cases, the metastasis was located in the right-side of the heart; in four, in a left-side chamber; and in two, in the pericardium. Five of the 17 patients died early in the chemotherapy treatment, and in eight, the disease was in remission at the time of the publication. Surgical resection of the metastasis followed by chemotherapy was the therapeutic approach performed in most cases.
A more extensive review, without limiting period of time, revealed just another case of germ cell tumor with cardiac metastasis in female. It was a primary chorion carcinoma of the right ovary with metastases to the left atrium in a 35-year-old woman, who presented with multiple metastases and died of respiratory failure, three months after the diagnosis [25].
A high level of suspicion is needed to establish the diagnosis of cardiac tumors. Frequently, the tumor is found incidentally during evaluation for a seemingly unrelated problem. Cardiac metastases often occur late in the course of a malignant disease and produce clinical symptoms in only about 10% of the affected patients [4–6]. Site, size, and tendency to cause embolism determine the clinical findings. In symptomatic patients, a mass is commonly detected by imaging methods, especially echocardiography. As the symptoms may mimic other cardiac conditions, the clinical challenge is to consider the possibility of a cardiac tumor; so that the appropriate diagnostic test can be conducted. Specific signs and symptoms are generally determined by the location of the tumor in the heart and not by the histological type [4–6]. Cardiac tamponade is one of the earliest and most frequent symptoms. Cardiac malignant disease may also cause arrhythmias and heart failure. The classic triad includes: symptoms resulting from intracardiac obstruction, signs of systemic embolization, and systemic symptoms [5, 6].
Recommended treatment for patients with advanced malignant ovarian germ cell tumors and non-dysgerminoma histology is maximal cytoreduction followed by platinum-based combination chemotherapy [26, 27]. Emergency surgical resection of intra-cardiac metastases has been recommended in the compromised patient and can be lifesaving [21]. New technical modalities (e.g., modern echocardiography, computed tomography, magnetic resonance imaging) provide noninvasive visualization of the intracardiac mass, which assists in designing the surgical approach not only to eliminate tumor tissue, but also to restore or maintain the hemodynamic status [14, 24]. Most patients treated aggressively will be long-term survivors even if they have advanced disease. However, despite the sensitivity of ovarian germ cell tumors to platinum-based chemotherapy, tumor volume still remains one of the most important prognostic factors for outcome, as evident in the case presented, where outcome was poor due to highly disseminated metastatic disease.
To the best of our knowledge this is the third report of grossly visible heart metastases from a yolk sac tumor in a female patient.
Consent
Written informed consent was obtained from the mother of the patient for publication of this case report and any accompanying images.
References
Gershenson DM: Management of ovarian germ cell tumors. J Clin Oncol 2007, 25: 2938–2943. 10.1200/JCO.2007.10.8738
Smith HO, Berwick M, Verschraegen CF, Wiggins C, Lansing L, Muller CY, Qualls CR: Incidence and survival rates for female malignant germ cell tumors. Obstet Gynecol 2006, 107: 1075–1085. 10.1097/01.AOG.0000216004.22588.ce
Mahdi H, Swensen RE, Hanna R, Kumar S, Ali-Fehmi R, Semaan A, Tamimi H, Morris RT, Munkarah AR: Prognostic impact of lymphadenectomy in clinically early stage malignant germ cell tumour of the ovary. Br J Cancer 2011, 105: 493–497. 10.1038/bjc.2011.267
Reynen K, Kockeritz U, Strasser RH: Metastases to the heart. Ann Oncol 2004, 15: 375–381. 10.1093/annonc/mdh086
Butany J, Nair V, Naseemuddin A, Nair GM, Catton C, Yau T: Cardiac tumours: Diagnosis and management. Lancet Oncol 2005, 6: 219–228. 10.1016/S1470-2045(05)70093-0
Neragi-Miandoab S, Kim J, Vlahakes GJ: Malignant tumours of the heart: a review of tumour type, diagnosis and therapy. Clin Oncol (R Coll Radiol) 2007, 19: 748–756. 10.1016/j.clon.2007.06.009
Savarese DM, Rohrer MJ, Pezzella AT, Davidoff A, Fraire AE, Menon M: Successful management of intracardiac extension of tumor thrombus in a patient with advanced nonseminomatous germ cell testicular cancer. Urology 1995, 46: 883–887. 10.1016/S0090-4295(99)80366-5
Sarjeant JM, Butany J, Cusimano RJ: Cancer of the heart: epidemiology and management of primary tumors and metastases. Am J Cardiovasc Drugs 2003, 3: 407–421. 10.2165/00129784-200303060-00004
Bath LE, Walayat M, Mankad P, Godman MJ, Wallace WH: Stage iv malignant intrapericardial germ cell tumor: a case report. Pediatr Hematol Oncol 1997, 14: 451–455. 10.3109/08880019709028775
Vohra A, Saiz E, Davila E, Burkle J: Metastatic germ cell tumor to the heart presenting with syncope. Clin Cardiol 1999, 22: 429–433. 10.1002/clc.4960220615
Low LL, Yip SK, Ang PC, Cheah FK: Testicular carcinoma with superior vena cava obstruction and atrial extension. Urology 1999, 54: 363–364. 10.1016/S0090-4295(99)00088-6
Deck AJ, True LD, Higano CS: Tricuspid valve metastasis from testicular carcinoma: a case report and review of the literature. Urology 2000, 56: 330.
Singh A, Jenkins DP, Dahdal M, Dhar S, Ratnatunga CP: Recurrent arterial embolization from a metastatic germ cell tumor invading the left atrium. Ann Thorac Surg 2000, 70: 2155–2156. 10.1016/S0003-4975(00)01899-3
Alaeddini J, Chandra M, Tang J, Ilercil A, Shirani J: Cardiac metastasis from testicular mixed germ cell tumor. Clin Cardiol 2001, 24: 689. 10.1002/clc.4960241010
Stefka J, Cleveland JC, Lucia MS, Singh M: Sarcomatoid intracardiac metastasis of a testicular germ cell tumor closely resembling primary cardiac sarcoma. Hum Pathol 2003, 34: 1074–1077. 10.1053/S0046-8177(03)00415-5
Weinberg NM, Zwas DR, Owen AN, Zangrilli JG, Van Tassell P: Left ventricular intracardiac metastatic germ cell tumor presenting with hemorrhagic cerebrovascular event. J Am Soc Echocardiogr 2004, 17: 1080–1083. 10.1016/j.echo.2004.05.015
May M, Finkbeiner Y, Gunia S, Seehafer M, Knorig J, Hetzer R: Metastasizing testicular germ-cell tumor with infiltration of the right heart: Indication for primary metastasectomy. Hear Vessel 2006, 21: 63–65. 10.1007/s00380-005-0829-5
Fujimura T, Minowada S, Kishi H, Hamasaki K, Saito K, Kitamura T: Acute pericarditis as a result of unusual metastasis of the visceral pleura in a patient with testicular seminoma. Int J Urol 2006, 13: 653–654. 10.1111/j.1442-2042.2006.01370.x
Liu JX, Eftimie B, Mortimer J: Intracardiac metastasis of germ cell tumor complicated by pulmonary hypertension and thrombocytopenia. J Clin Oncol 2007, 25: 3547–3549. 10.1200/JCO.2007.12.3562
Avasthi R, Chaudhary SC, Mohanty D, Mishra K: Testicular mixed germ cell tumor metastasizing to heart. J Assoc Physicians India 2008, 56: 812–815.
Taghavi F, Markar S, Williams M, Large S: Intra-cardiac metastasis from testicular non-seminoma germ cell tumour; to resect or not to resect. Interact Cardiovasc Thorac Surg 2010, 11: 843–845. 10.1510/icvts.2010.242198
Gursu O, Isbir S, Ak K, Ozben B, Turkoz HK, Dal D, Arsan S: Testicular germ cell tumor metastatic to the right atrium. J Card Surg 2011, 26: 276–279. 10.1111/j.1540-8191.2011.01233.x
Achouh P, Grinda JM, Emmerich J, Fabiani JN: Right atrial metastasis of a testicular cancer. Eur J Cardiothorac Surg. 2012, 41: 712. 10.1093/ejcts/ezr044
Jonjev ZS, Rajic J, Majin M, Donat D: Intracardiac metastasis from germ cell testicular tumor. Herz 2012, 37: 709–711. 10.1007/s00059-012-3595-z
Hepp A, Larbig D, Bader H: Left atrial metastasis of chorion carcinoma, presenting as mitral stenosis. Br Heart J 1977, 39: 1154–1156. 10.1136/hrt.39.10.1154
Williams SD, Blessing JA, Moore DH, Homesley HD, Adcock L: Cisplatin, vinblastine, and bleomycin in advanced and recurrent ovarian germ-cell tumors. A trial of the gynecologic oncology group. Ann Intern Med 1989, 111: 22–27. 10.7326/0003-4819-111-1-22
Gershenson DM, Morris M, Cangir A, Kavanagh JJ, Stringer CA, Edwards CL, Silva EG, Wharton JT: Treatment of malignant germ cell tumors of the ovary with bleomycin, etoposide, and cisplatin. J Clin Oncol 1990, 8: 715–720.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
All authors have made important contributions to the manuscript and have approved this final version.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Nunes, M.C.P., Moreira, D.R. & Ferrari, T.C.A. Cardiac metastasis from yolk sac tumor: case report and review. Exp Hematol Oncol 2, 13 (2013). https://doi.org/10.1186/2162-3619-2-13
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/2162-3619-2-13