
Abstract
Allogeneic stem cell transplantation (alloSCT) is the most robust form of adoptive cellular therapy (ACT) and has been tremendously effective in the treatment of leukemia. It is one of the original forms of cancer immunotherapy and illustrates that lymphocytes can specifically recognize and eliminate aberrant, malignant cells. However, because of the high morbidity and mortality that is associated with alloSCT including graft-versus-host disease (GvHD), refining the anti-leukemia immunity of alloSCT to target distinct antigens that mediate the graft-versus-leukemia (GvL) effect could transform our approach to treating leukemia, and possibly other hematologic malignancies. Over the past few decades, many leukemia antigens have been discovered that can separate malignant cells from normal host cells and render them vulnerable targets. In concert, the field of T-cell engineering has matured to enable transfer of ectopic high-affinity antigen receptors into host or donor cells with greater efficiency and potency. Many preclinical studies have demonstrated that engineered and conventional T-cells can mediate lysis and eradication of leukemia via one or more leukemia antigen targets. This evidence now serves as a foundation for clinical trials that aim to cure leukemia using T-cells. The recent clinical success of anti-CD19 chimeric antigen receptor (CAR) cells for treating patients with acute lymphoblastic leukemia and chronic lymphocytic leukemia displays the potential of this new therapeutic modality. In this review, we discuss some of the most promising leukemia antigens and the novel strategies that have been implemented for adoptive cellular immunotherapy of lymphoid and myeloid leukemias. It is important to summarize the data for ACT of leukemia for physicians in-training and in practice and for investigators who work in this and related fields as there are recent discoveries already being translated to the patient setting and numerous accruing clinical trials. We primarily focus on ACT that has been used in the clinical setting or that is currently undergoing preclinical testing with a foreseeable clinical endpoint.
Similar content being viewed by others


Introduction
T-lymphocytes are critical cells of the immune system that eliminate both infectious pathogens and abnormal, malignant cells. The importance of T-cells in the elimination of leukemia was first supported by trials comparing T-cell replete versus T-cell depleted allogeneic stem cell transplant (alloSCT), where a higher incidence of disease relapse was observed for recipients of T-cell depleted transplants, but with the advantage of a lower incidence of graft-versus-host disease (GvHD)[1–6]. The data for this effect are strongest in chronic myeloid leukemia (CML), though evidence for T-lymphocyte targeting of malignant cells within other leukemia diagnoses – acute myeloid leukemia (AML), chronic lymphocytic leukemia (CLL), and acute lymphoblastic leukemia (ALL) - also comes from trials demonstrating success with donor lymphocyte infusion (DLI) for relapsed leukemia after alloSCT[7–11]. DLI is a treatment comprised of unselected, polyclonal donor lymphocytes and is frequently administered in the absence of preparative conditioning. It provides the most direct proof of the potent graft-versus-leukemia (GvL) effect mediated by allogeneic T-cells, but GvHD complicates DLI in up to 60% of patients[12]. Thus, adoptive cellular therapy (ACT) has arisen from the desire to isolate and enhance the GvL effect that accounts for the efficacy of alloSCT and DLI while minimizing GvHD toxicity, which causes significant morbidity and mortality. ACT is a type of cancer treatment that involves infusing patients with large numbers of autologous or allogeneic lymphocytes that have undergone ex vivo selection and modification. The goal of ACT for leukemia is to administer T-cells that target leukemia antigens with minimal impact on normal tissues.
It is important to highlight that GvL and GvHD both refer to the allogeneic setting where donor T-cells are presumed to recognize both tumor-associated antigens (nonpolymorphic self antigens that are overexpressed in malignant cells), minor histocompatibility antigens (polymorphic host antigens that are foreign to the donor) and tumor-specific antigens (antigens that are mutated or solely expressed by the tumor cell)[13, 14]. Graft-versus-tumor effects are not exclusive to allogeneic T-cells, however, and Rosenberg et al. have pioneered efforts to use a patient’s autologous T-cells to combat melanoma, and more recently carcinoma, using several strategies with much success[15, 16]. With regard to hematologic disease, using ACT is a natural extension of standard of care approaches that are currently employed to treat leukemia, lymphoma, and myeloma - specifically autologous and alloSCT. Limiting this approach, though, are a lack of known tumor antigens and mechanisms of central and peripheral T-cell tolerance whereby T-cells with high affinity for self-antigens are deleted in the thymus or are rendered hyporesponsive through various mechanisms that can be exploited by the immunosuppressive tumor microenvironment[17]. Numerous high throughput methodologies are being explored for the identification of novel tumor antigens, and, to bypass T-cell tolerance, research is now capitalizing on advances made in synthetic biology and basic immunology to engineer and redirect T-cells to eliminate tumor cells. The purpose of this review is to provide an overview of various strategies being developed to improve the adoptive transfer of T-cells for immunotherapy of leukemia, with a focus on the approaches being tested in clinical trials.
Review
Leukemia antigens
Arguably, the most important aspect of ACT is the targeted antigen, and this is becoming increasingly true as methods to enhance the T-cell receptor (TCR) affinity and to lower T-cell activation thresholds are incorporated. These improvements narrow the therapeutic window for ACT and necessitate careful antigen selection. Many, but not all, tumor antigens arise from intracellular proteins that must be processed and presented by a cell’s major histocompatibility complex (MHC) in order to trigger TCR-binding and provoke an immune response. In contrast, the implementation of chimeric antigen receptors (CARs) has now broadened the pool of potential antigens to include extracellular, non-MHC bound molecules. The ideal tumor antigen is expressed on all malignant cells including cancer stem cells, demonstrates high immunogenicity, is absent in normal tissue, and derives from a protein required for maintenance of the malignant phenotype, which prevents a leukemic subclone from escaping T-cell detection by downregulating the antigen’s expression[18].
There are several classes of tumor antigens (Table 1). Many are tumor-associated antigens (TAAs) derived from self-proteins that are expressed at low levels in normal tissue and overexpressed or aberrantly expressed in malignant cells, such as Wilms tumor-1 (WT-1)[19]. Tumor differentiation antigens are a subset of TAAs that arise from self-proteins and are expressed in a distinct subset of normal cells and often at higher levels in their malignant cell counterpart. PR1, a peptide from neutrophil elastase and proteinase 3, is an example of a tumor differentiation antigen as its source proteins are induced during the promyelocyte stage and are overexpressed in myeloid leukemias[20–22]. Targeting these classes of self-antigens has shown promise in preclinical models, vaccine trials, and early adoptive T-cell trials, but risks toxicity to normal tissues as the antigens are not strictly found on malignant cells. This is also true for the cancer-testis antigens, a family of proteins expressed primarily by germ cells and in various malignancies[23]. Several recent trials highlight the risks of targeting TAAs, including a trial at the National Institutes of Health (NIH) that tested the adoptive transfer of autologous T-cells engineered to express a murine TCR with specificity for an HLA-A2-restricted peptide from carcinoembryonic antigen (CEA)[24]. Anti-CEA T-cells were administered to 3 patients with metastatic colon cancer. The treatment caused tumor regression, including 1 partial response (PR), but severe, dose-limiting toxicity in the form of inflammatory colitis was observed in all patients and caused the trial to be halted. The colitis was an on-target adverse effect resulting from T-cells recognizing the CEA epitope on normal colonic epithelium, illustrating that the targeting of self-antigens with modified T-cells is not without consequence.
In the allogeneic setting, minor histocompatibility antigens (mHAs) are endogenous polymorphic proteins that differ between donor and recipient and can serve as targets for GvL and GvHD[13]. These represent important antigens because donor cells are not tolerized to these ‘foreign’ peptides enabling them to elicit higher avidity T-cell responses. One goal is to identify mHAs that are confined to the hematopoietic compartment, because in this scenario, after the host blood system is replaced with donor cells by alloSCT, the only mHA-expressing cells remaining are malignant host cells. At least 12 such hematopoietic-predominant mHAs have been identified thus far and one such antigen, HA-1, has been targeted in a pilot clinical trial[35, 46].
Also in the category of "non-self" antigens are neoantigens, otherwise known as tumor-specific antigens. These are novel peptides that result from chromosomal translocations, point mutations, deletions, or insertions within a malignant cell’s genome. Neoantigens theoretically represent ideal targets as they should elicit high avidity T-cells, they are absent on normal cells, and they may originate from "driver" genes that are leukemogenic. In melanoma, a highly mutated disease, it is thought that neoantigens constitute much of the anti-tumor immune response[47–49]. Leukemias, however, are among cancers with the lowest mutation rate, making such antigens difficult to identify[50, 51]. In CML, the BCR-ABL translocation does represent one source for leukemic neoantigens, and several epitopes from this fusion protein have been shown to elicit a T-cell response[52–55]. Early trials of adoptively transferred anti-BCR-ABL T-cells have proven safe with some evidence of disease response, however, the success of tyrosine kinase inhibitors in CML has largely overshadowed the development of ACT for this disease[56, 57].
Tumor-specific antigens (neoantigens) can also be found within the clonal idiotypes unique to B-cell malignancies, which contain the variable regions of the B-cell receptor immunoglobulin heavy and light chains[58]. Vaccination strategies against these epitopes have demonstrated success in lymphoma[41]. These antigens are patient-specific, though, which raises questions about the feasibility of using these epitopes and other highly individualized neoantigens as targets. With advances in whole exome sequencing and T-cell engineering, though, they will likely gain importance.
The last class of "non-self" intracellular antigens are oncoviral peptides, which are being investigated as immunotherapeutic targets in human papillomavirus-initiated cervical cancer, Epstein Barr Virus (EBV)-related post-alloSCT B-cell lymphoproliferative disease, and EBV-associated lymphomas[59–61]. They may also be applicable in the setting of virally-induced hematologic malignancies, such as HTLV-1 associated T-cell leukemia/lymphoma[42, 62]. The advantage of these viral peptides is that they elicit very high avidity T-cell responses in contrast to endogenous human epitopes[63].
Finally, it is important to emphasize that all of the tumor antigens discussed thus far are intracellular antigens, which rely on intact, functional cellular machinery for their processing and MHC-restricted presentation. This is a fundamental limitation of TCR-based T-cell therapy because human leukocyte antigen (HLA) subtypes are highly polymorphic and labor-intensive strategies that target a single epitope will only apply to the subset of patients expressing that particular HLA allele. Furthermore, malignant cells are known to evade the immune system by altering antigen processing and downregulating their MHC expression[64]. One strategy to bypass these constraints is through use of CAR T-cells that target broadly expressed membrane-bound molecules. A CAR links a portion of the antibody binding domain to T-cell costimulatory and signaling domains[65]. Because the recognition domain is engineered from an immunoglobulin, the CAR recognizes extracellular, membrane-bound epitopes that are not confined to an MHC, and this groundbreaking development has added a new class of leukemia antigens and vastly expanded the number of targetable epitopes. Dozens of extracellular molecules are now being investigated for their value as tumor antigens and, in leukemia, these include CD19, CD20, CD22, CD30, Lewis Y antigen, among others[66]. However, although the immune response can be effectively engineered using this technology, the antigens that CAR T-cells target must still be evaluated for their expression in normal tissues and for their importance in leukemogenesis to limit the possibility of selecting for antigen escape variants. Lastly, even though the majority of CAR T-cells developed to date have targeted broadly expressed cell surface receptors, CAR T-cells that target peptides presented on HLA molecules are also currently being investigated and work by integrating TCR-mimicking antibodies[67]. It is likely that successful immunotherapy for leukemia will require targeting many of these antigens in multiple pathways, which likely accounts for the success of the graft-versus-leukemia effect.
Adoptive T-cell Transfer Strategies for Leukemia
Although this review focuses specifically on modifications and ex vivo manipulation of CD4+ and CD8+ αβ T-lymphocytes for adoptive transfer and treatment of leukemia, ACT using other effector cell types – including γδ T-cells, natural killer (NK) cells, NK T-cells, and invariant NK T cells - is also an area of active investigation[68–71]. Adoptive T-cell therapy represents a natural extension of current treatment for leukemia because allogeneic transplant and DLI already involve the transfer of large numbers of T lymphocytes. Further, adoptive T-cell transfer to prevent CMV, adenovirus, and Aspergillus infections in the context of alloSCT has been well studied and provides a valuable foundation for T-cell transfer strategies[72–78]. T-cells have many properties of an ideal therapeutic - their area of biodistribution is broad and includes the central nervous system, they can expand and increase their potency in vivo, and they can acquire long half-lives by establishing memory, ideally providing a reservoir of antitumor immunity that leads to actual cancer cures[79, 80].
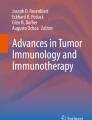
There are numerous strategies being developed to target malignant cells via adoptive T-cell transfer (Figure 1). A major division within current ACT approaches is whether or not T-cells undergo genetic modification prior to infusion. T-cells that do not undergo this additional step (conventional T-cells) must undergo ex vivo manipulation and expansion prior to administration, an extensive process where cells may spend a month or more in culture. The goal of this step is to generate large numbers of T-cells that are specific for one or more tumor antigens from an infrequent and polyclonal population. In contrast, genetic modification of T-cells bypasses these lengthy enrichment protocols by direct transfer of either TCR α and β chains or a CAR, thereby endowing lymphocytes with a secondary, engineered specificity. The rationale, advantages, and disadvantages for the most common strategies are presented here.

Graphic representations of the various T-cell approaches used to target leukemia antigens. (a) Conventional T-cells target peptides that are presented in the context of an MHC molecule. (b) Modified Ectopic α/β T-cells target the same epitope as a conventional TCR (MHC-peptide) but with an engineered (often higher affinity) TCR from an autologous, allogeneic, or xenogeneic cell. (c) CAR T-cells contain a synthetic polypeptide that contains the single chain variable fragment (scFv) of an antibody as the antigen-binding domain, a hinge, a transmembrane region, a costimulatory (Costim) domain, and a CD3ζ signaling domain. CARs recognize extracellular antigens that are not MHC-bound. (d) A TCR-like CAR utilizes the scFv fragment of a TCR-mimicking Ab, which recognizes a peptide antigen in the context of an MHC molecule, but with a much higher affinity than conventional or most engineered TCRs.
Transfer of unmodified, conventional T-cells includes both autologous and allogeneic lymphocytes that range in antigen specificity from polyclonal populations to antigen-enriched subsets to antigen-specific T-cell clones. Transfer of allogeneic polyclonal T-cells describes a DLI, which can be effective for treating relapsed leukemia after alloSCT though with a high risk of GvHD[12]. Adoptive transfer of bulk, ex vivo activated, autologous polyclonal lymphocytes has been tested by Rapoport et al. and, when administered with tumor vaccines, can generate antitumor immunity[81]. However, both central and peripheral tolerance hinder this approach and T-cells with specificity for tumor antigens are infrequent, have low avidity, and can be rendered anergic by the immunosuppressive tumor microenvironment[17, 63]. A number of tumor-specific T-cell enrichment strategies exist and include culturing lymphocytes in the presence of irradiated tumor cells, stimulating mHA-naive allogeneic T-cells in the presence of mHA-positive host antigen-presenting cells (APCs), or extracting T-cells from tumor specimens and subsequently expanding them for reinfusion. For example, a recent trial at the NIH tested the adoptive transfer of polyclonal tumor-derived lymphocytes for the treatment of relapsed CLL or lymphoma after alloSCT[82]. The rationale underlying this approach is that T-cells found within tumor specimens are enriched for tumor antigen-specific cytotoxic T-lymphocytes (CTLs), which can be made more potent by ex vivo costimulation and expansion. This is analogous to tumor-infiltrating lymphocyte (TIL) therapy for melanoma, which has demonstrated overall response rates of up to 72%[83]. In the lymphoma/CLL trial, 8 patients were treated with lymphocytes that were first extracted from their tumor biopsy specimens and subsequently activated and expanded with anti-CD3/anti-CD28 Ab-coated magnetic beads. No GvHD was observed and modest anti-tumor activity was seen in 4 patients[82]. Additionally, towards the goal of targeting multiple antigens simultaneously, a recent study demonstrated that autologous, functional T cells from ALL patients could be generated with specificities enriched for multiple TAA (PRAME, WT-1, MAGE-A3, and Survivin) by stimulating lymphocytes using autologous APCs pulsed with complete peptide pools spanning the entire amino acid sequences of the tumor-associated proteins[84].
The most precise approach using conventional T-cells is transfer of antigen-specific CTL clones, which are generated by labor-intensive limiting dilution cloning techniques[85]. These methods produce large numbers of monoclonal T-cells that recognize a defined HLA-restricted tumor epitope. Autologous or allogeneic CTL clones can be generated using a variety of stimulator cells. For example, large numbers of CTL clones with specificity for an immunodominant HLA-A2-restricted epitope from WT-1 were generated by stimulating donor T-cells repeatedly with peptide-pulsed autologous DCs for use in a recent clinical trial (discussed below)[25]. There are benefits to using conventional T-cells over T-cells genetically engineered to express an ectopic TCR α and β chain. With conventional T-cells, there are no concerns for ectopic and endogenous TCR α/β mispairing, which has the potential to generate new specificities and cause harm by nonspecifically reacting with normal tissues[86]. Also, though viral transduction of TCRs into mature cells has thus far proven safe, the use of conventional T-cells also eliminates the worry for insertional oncogenesis of transduced lymphocytes[87, 88]. Additionally, with conventional allogeneic CTL clones, there is no secondary specificity of the T-cells and thus a much lower risk for off-target GvHD. Finally, conventional T-cells – whether autologous or allogeneic – have been educated in the human thymus and have toxicities that are more predictable than those for murine TCRs and affinity-enhanced TCRs, which have exhibited deleterious off-target effects[89]. On the other hand, the efficacy of adoptive transfer of conventional T-cells is limited by several factors. Tumor antigen-specific T-cells, particularly those that recognize "self" antigens, are generally of low avidity - a problem that can be exacerbated in patients with leukemia[90]. Moreover, generating large numbers of clones requires weeks of repetitive stimulation in culture, which can further reduce T-cell avidity while allowing time for tumors to progress. Similarly, extensive ex vivo manipulation can select for T-cells with more differentiated, exhausted effector phenotypes that are less likely to mediate durable, potent tumor regression after adoptive transfer[91].
To bypass many of these limitations, methods have been developed to deliver the genes for full-length TCR α and β chains into autologous or allogeneic peripheral blood mononuclear cells (PBMC), creating bispecific T-cells with specificities determined by both the cell’s endogenous TCR and the engineered TCR[92]. This approach dramatically shortens the ex vivo manipulation process and allows for generation of high avidity clones. This strategy also allows for pre-selection of a desired subset of lymphocytes for TCR transduction (central memory T-cells, stem cell memory T-cells, etc.), which have demonstrated better persistence and expansion in vivo relative to the terminally differentiated, effector lymphocytes often generated by lengthy limiting dilution cloning protocols[93–96]. Retroviruses, lentiviruses, transposons, and other constructs are all being actively investigated as means to deliver the TCR (or CAR – see below), and the pros and cons of each of these methods are outside the scope of this discussion but have been reviewed by others[97, 98]. Many refinements to TCR-engineering protocols have already been developed and include the addition of disulfide bonds to prevent TCR α/β mispairing and codon optimization to facilitate better TCR expression[99, 100]. Additionally, very high affinity xenogeneic TCRs from HLA-A2 transgenic mice can be transferred into human PBMC using these methods[101–104]. TCR affinity can be further enhanced via site-directed mutagenesis of the TCR antigen-binding region[105]. Unfortunately, some of these "supercharged" T-cells have demonstrated unpredictable toxicities in patients, and new safety measures for testing high-affinity, modified T-cells against human tissue samples prior to their use in clinical trials will need to be implemented[89, 106, 107]. Nevertheless, several TCR constructs derived from conventional, human T-cells with physiologic avidities have undergone extensive preclinical testing and will now be studied in human leukemia trials including those that redirect T-cells against HLA-A2 restricted epitopes of HA-1 and WT-1[100, 108]. One potential drawback to all types of TCR-based ACT is that the binding between the TCR and MHC/peptide complex is inherently degenerate, meaning that a given TCR can recognize more than 1 peptide-MHC ligand[109]. This could result in unforeseen toxicity in the form of off-target tissue effects, particularly when large numbers of cells with affinity enhanced or xenogeneic TCRs are infused. Lastly, though ectopic TCR transfer overcomes many of the limitations posed by conventional T-cells, the targeted epitopes must still be successfully processed within the proteasome and subsequently presented in the context of an MHC molecule, which may afford malignant cells the opportunity to escape this therapy via downregulation of surface MHC or aberrant antigen processing.
As alluded to above, CARs represent a unique strategy designed to circumvent many drawbacks of TCR-based ACT. The antigen-recognition domain of the CAR is derived from an antibody’s single-chain variable fragment (scFv), which recognizes epitopes within membrane-bound molecules. The majority of CARs developed to date target broadly expressed surface molecules that are independent of MHC, though CARs can be engineered to recognize peptide-HLA epitopes as well[67]. The scFv fragment is linked to a transmembrane region, a signaling protein (typically CD3ζ), and a costimulatory domain (CD28, 4-1BB, OX-40, ICOS, and others). The CARs are delivered using vehicles similar to those discussed above for ectopic TCRs (lentiviruses, retroviruses, etc.). CARs were first reported by Gross et al. in 1989[65]. Early clinical trials using CARs demonstrated disappointing efficacy, largely due to the lack of persistence of the modified cells[110–112]. These 1st generation CARs lacked a costimulatory domain. The addition of a costimulatory domain (initially CD28 or 4-1BB) has revolutionized the field and these 2nd generation CARs have begun to demonstrate impressive clinical responses, particularly using anti-CD19 CARs for treatment of B-cell malignancies (see CD19 section below). Now, 3rd generation CARs (those with >1 engineered costimulatory domain) are reaching clinical testing and may further enhance the redirected T-cells’ activity. By targeting extracellular epitopes, CARs have the distinct advantage of thwarting many mechanisms of tumor immunoevasion including MHC downregulation and altered protein processing. The problem of tumor escape is not solved completely, however, and malignant cells with little or no expression of the targeted antigen may evade this approach, underscoring the importance of targeting proteins that are critical in leukemogenesis[79]. Another important advantage of CARs is that they are very high-affinity receptors that mediate eradication of malignant cells with low levels of antigen expression. A consequence of this enhanced affinity is that normal cells with low antigen expression will also be targeted resulting in increased on-target, off-tissue adverse effects[24, 113, 114]. CAR and ectopic TCR approaches share many of the same advantages over conventional T-cell ACT. For example, the subset of T-cells to be transduced with either artificial receptor can be pre-enriched for central memory T-cells, stem cell memory T-cells, or virus-specific T-cells and either allogeneic or autologous cells can be used for transduction. A fundamental difference between CARs and ectopic TCRs is that they target extracellular or intracellular antigens, respectively, but even this line is being blurred. TCR-mimicking antibodies against PR1 and WT-1 have been generated and are now being tested in TCR-like CAR constructs in preclinical mouse models[67, 115, 116]. These receptors function like TCRs since they recognize a peptide antigen in the context of an MHC molecule, but they have the benefit of binding with higher affinity than a TCR. These and other recent advances illustrate how the field of ACT is rapidly evolving, and it is likely that genetically modified T-cells will overtake conventional T-cells within the field of ACT.
Additional T-cell modifications
Specificity is not the only focus of T-cell engineering. Though outside the scope of this review, other authors have outlined the many ways by which researchers are aiming to build a better T-cell[66, 97, 117–119]. Examples of these strategies include incorporating additional chemokines to improve T-cell trafficking, artificially upregulating anti-apoptotic proteins, increasing resistance to immunosuppressive cytokines, and adding suicide genes to delete the modified lymphocytes in the event of significant toxicity[120–126].
Allogeneic SCT platform
In many ways, ACT for leukemia lends itself to the allogeneic SCT setting where large numbers of allogeneic T-cells are infused along with CD34+ progenitor cells after conditioning chemotherapy. ACT is not limited to this setting, however, and anti-CD19 CAR therapy in the absence of transplant and in the autologous setting has demonstrated success in heavily pretreated and refractory CLL patients[80]. Many questions will need to be answered to utilize ACT most effectively and to properly position it alongside current treatments including cytotoxic chemotherapy, molecular-targeted agents, and alloSCT (Figure 2). Cost and manufacturing capabilities will undoubtedly factor into these decisions as well. It is conceivable that ACT could become initial, first-line therapy for certain leukemia subtypes in contrast to the challenging, post-alloSCT relapse setting where it is typically tested today. Moreover, progress continues to be made in other types of therapy making treatment decisions a moving target. For example, alloSCT has historically been reserved for young, healthy patients with relapsed or high-risk disease, but this is changing with the advent of nonmyeloablative transplant and improved supportive care[127, 128].

Diagram of ACT within the alloSCT platform. T-cell depleted SCT would eliminate the need for post-SCT immunosuppressive medications that can limit the efficacy of modified T-cells. Since allogeneic cells are used, the endogenous specificity of the T-cells would be pre-selected (CMV, EBV, varicella, etc.) or other GvHD prevention measures would need to be incorporated, such as naïve T cell depletion.
One aspect of ACT that is established and relevant to leukemia is the benefit achieved with lymphodepletion. This has been studied in the non-transplant setting where depleting host lymphocytes prior to adoptive T-cell transfer improves T-cell expansion and persistence by freeing up important cytokines (IL-7, IL-15), encouraging homeostatic peripheral expansion, and depleting regulatory T-cells[129–133]. Conditioning chemotherapy prior to alloSCT would then serve a dual purpose in this setting – eradication of disease and creation of space for transferred leukemia-specific T-cells. Additionally, it may be advantageous for patients to be in a state of minimal residual disease (MRD) at the time of ACT, which is often the situation after alloSCT. This may be especially true for aggressive malignancies like AML and ALL, where the leukemia burden can quickly increase. The reasons for this are two-fold: first, it has been observed in early clinical trials that ACT-associated toxicities such as the cytokine-release syndrome are more severe in patients with larger disease burdens and second, it can take days to weeks for modified T-cells to expand in vivo and so an MRD state affords the modified T-cells time to proliferate and potentially overtake the malignant cell population. Unfortunately, it is not always possible for patients to reach a state of MRD, and early trials have shown that anti-CD19 CAR therapy can mediate dramatic leukemia responses even in patients with very advanced disease, proving its versatility[79, 134, 135].
Two main concerns will need to be addressed to successfully apply ACT to the alloSCT setting: the potential for triggering GvHD and interference caused by immunosuppressive medications. Since the recipient’s hematopoietic system is replaced by donor cells after alloSCT, conventional or modified adoptively transferred T-lymphocytes will need to be of donor origin. This being said, in the future it may be possible to use universal or 3rd party donor T-cells by incorporating zinc-finger nuclease technology that can be used to knockdown a T-cell’s MHC class I/II expression as well as its endogenous TCR[136]. Nevertheless, it is well established that infusing large numbers of allogeneic T-cells into patients shortly after transplant results in unacceptable rates and severity of GvHD[137]. Therefore, it will not be possible to simply transduce bulk donor T-cells with the desired antigen-specific TCR or CAR construct and infuse these cells at the time of transplant since the endogenous allogeneic polyclonal TCRs would trigger GvHD. This problem can be approached from many angles. One possibility is to isolate donor lymphocytes with defined, known specificities (EBV, CMV, varicella, etc.) and to subsequently transduce only these oligoclonal T-cells with a synthetic receptor (CAR or ectopic TCR) and then infuse them at the time of transplant[138, 139]. Another option is to deplete naïve donor T-cells prior to ex vivo TCR/CAR transduction since naive T-cells have been shown to play an important role in GvHD[140–142]. In contrast, if bulk polyclonal donor cells are used, delayed, low-dose administration of ACT at time of relapse or many months after alloSCT may mitigate GvHD. This is based on trials of DLI, where administration of low dose donor T-cells more than 9 months after transplant resulted in a GvHD rate of only 10%[143, 144]. Encouragingly and along these same lines, in early trials of anti-CD19 CAR therapy, infusions of modified, polyclonal donor-derived cells that were collected from the recipient (post-transplant) did not cause GvHD, possibly because of tolerance developed within the host[145, 146].
A separate platform for ACT that should be considered is T-cell depleted alloSCT. Though opportunistic infections would be expected to increase, this approach might be advantageous because it would eliminate the need for immunosuppressive agents, which are known to abrogate the effects of adoptively transferred T-cells[134, 135]. Otherwise, for T-cell replete alloSCT, an attractive strategy is to arm modified, antigen-specific T-cells with resistance to immunosuppressive drugs (calcineurin inhibitors, mycophenolate mofetil, methotrexate, or glucocorticoids)[46, 147–149]. Still, it must be kept in mind that the rationale for using allogeneic rather than autologous transplants for leukemia is both to avoid infusion of malignant cells and to harness the GvL effect. If the GvL effect is successfully condensed to a handful of tumor antigens, then tumor-restricted, antigen-specific TCR and/or CAR constructs could be developed to target these antigens. This would permit the use of autologous grafts and autologous ACT (minor histocompatibility antigens excluded), which could significantly reduce (if not eliminate) GvHD. As outlined, the rapid pace of discovery in the field of ACT is exciting. Developing the most effective ACT will require careful consideration of the optimal antigens to target (likely in combination), the T-cell approach to utilize, and which of the myriad additional modifications to incorporate into the engineered lymphocytes.
Challenges and limitations
Though immunotherapy is typically characterized as less toxic and more specific than chemotherapy and other cancer therapies, multiple serious adverse effects in early clinical trials using ACT underscore its tremendous potency and risks. Adverse effects have resulted from multiple mechanisms. On-target, off-tissue toxicity describes the situation where a T-cell appropriately recognizes an antigen of interest (via TCR or CAR), but in the case where this antigen is also expressed on healthy tissues. One example of on-target, off-tissue toxicity was reported in a Phase I clinical trial of renal cell carcinoma patients treated with autologous CAR T-cells engineered to recognize an epitope within the carbonic anhydrase IX (CAIX) tumor-associated protein[113]. Multiple patients experienced significant liver toxicity due to the expression of CAIX on normal bile duct epithelium requiring cessation of treatment in 4 patients. This on-target, off-tissue toxicity can be mediated either by a CAR or a TCR, however, CAR T-cells may prove the worst offenders because of their inherent high affinity and built-in costimulation. Off-target toxicity occurs when the antigen receptor (CAR or TCR) recognizes a different epitope than is intended. This form of toxicity has been more common with TCRs, which are inherently degenerate, and particularly with mutated and xenogeneic TCRs that bypass education in the thymus and can have unpredictable specificities. For example, a patient-derived TCR with specificity for the cancer-testis antigen HLA-A*01-MAGE-A3 first underwent site-directed mutagenesis resulting in enhanced affinity of the receptor, was subsequently incorporated into a lentiviral vector, and was then used in a clinical trial testing the construct against myeloma and melanoma. Unfortunately, the first 2 patients treated experienced fatal cardiac toxicity that was incited by an off-target epitope within the normal cardiac myocyte protein titin (off-target titin peptide: ESDPIVAQY; on-target MAGE-A3 peptide: EVDPIGHLY)[89, 106]. These adverse events have since been carefully analyzed and have generated much discussion about strategies to predict on and off-target toxicity.
Issues of specificity and antigen selection are paramount to the success of ACT but other challenges remain. Even in the context of a highly avid T-cell and a tumor-restricted antigen, T-cell persistence, trafficking, and diminishing receptor transgene expression can all be problematic[150]. Furthermore, the tumor microenvironment is an inhospitable place for T-cells and adoptively transferred cells will need to resist inhibitory signals from tumor and stromal cells to remain effective[151]. Even after initial recognition and lysis of tumor cells, the adoptively transferred lymphocytes must then outcompete the tendency of malignant subclones to evade killing via downregulation of MHC molecules, altered antigen processing, and epigenomic and genomic evolution[64]. And on a broader scale, issues of cost, manufacturing, and standardization will also be important to the applicability of ACT and have been reviewed by others[97, 152]. Finally, even patients who experience durable, complete remissions from ACT can experience adverse effects in the form of cytokine release syndrome, tumor lysis syndrome, hemophagocytic lymphohistiocytosis, and B-cell aplasia though investigators and clinicians are learning a great deal about how to limit these toxicities. It must be kept in mind, though, that many of the patients treated with ACT thus far have dismal prognoses and limited to no treatment options in the absence of clinical trials. Furthermore, ACT is still in its infancy and if the current pace of innovation is sustained, it promises to grow in importance. Along these lines, below is a discussion of current strategies being tested in clinical trials.
Targeting leukemia antigens in the clinic
CD19
Trials of anti-CD19 CAR T-cell therapy in patients with B-cell malignancies have generated exciting clinical results and underscore the tremendous potential of antigen-specific ACT for leukemia. These trials – spearheaded by groups at the NIH, Baylor College of Medicine, the University of Pennsylvania, and at Memorial Sloan Cancer Center (MSKCC) – have laid the foundation for this new therapeutic modality that is certain to gain importance in the treatment of ALL, CLL and B-cell lymphomas.
CD19 functions as a component of the B-cell co-receptor that enhances B-cell receptor signaling upon antigen encounter and CD19 expression is restricted to malignant and normal cells of the B-cell lineage[153, 154]. In numerous preclinical studies, anti-CD19 CAR T-cells demonstrated selective lysis of B-lineage tumor lines and primary leukemia/lymphoma cells in vitro and also showed potent antitumor activity in murine xenograft and immunocompetent mouse models[152, 155–164]. Subsequently in 2010, Kochenderfer et al. at the NIH reported the first successful use of anti-CD19 CAR T-cell treatment in a patient with advanced follicular lymphoma who received cyclophosphamide and fludarabine conditioning followed by a single infusion of autologous T-cells retrovirally transduced with a 2nd generation CD19 CAR (CD28 costimulatory domain) along with IL-2[165]. This patient experienced a dramatic partial response as well as B-cell aplasia in weeks 9 through 39 after CAR infusion, demonstrating the potency and CD19 specificity of this approach. In the expanded NIH cohort, which included 8 patients with lymphoma or CLL, 6 of 7 evaluable patients achieved objective disease responses, though in the context of concurrent cyclophosphamide/fludarabine chemotherapy[166]. Directly attributable to the CD19 CAR therapy, B-cell aplasia was observed in 4 of 8 patients for 6 months or more, demonstrating the persistence (and toxicity) of anti-CD19 CAR T-cells. Shortly thereafter, impressive responses for CLL patients were reported in a separate Phase I trial, where 3 patients were treated with a 2nd generation anti-CD19 CAR that differed from the NIH construct in both the costimulatory domain (4-1BB in contrast to CD28) and the virus used for transduction (lentivirus as opposed to retrovirus)[80, 134]. Despite all 3 patients having extensive and chemorefractory disease at the time of CAR infusion, all 3 experienced objective responses – 2 complete responses (CRs)– and the CAR T-cells expanded in vivo more than 1000-fold and persisted beyond 6 months. A recent update for 14 heavily pretreated and refractory CLL patients treated on this protocol described an overall major response rate of 57% - including 3 patients with durable CRs that have lasted up to 35 months and 5 patients with partial responses (PRs)[167].
Encouraging results have also been demonstrated in both pediatric and adult acute lymphoblastic leukemia, a more aggressive malignancy that is less immune-susceptible and responds poorly to DLI. This is partly due to low expression of costimulatory molecules by ALL cells[8, 9, 168, 169]. One of the first CD19 CAR trials conducted in ALL patients was a Phase I study that used autologous T-cells retrovirally transduced to express an anti-CD19 CAR with a CD28 costimulatory protein. This trial enrolled 5 adult patients with relapsed disease[135]. Prior to CAR T-cell infusion, 2 patients had overt disease, 2 had MRD, and 1 was MRD negative. All patients underwent lymphodepletion with cyclophosphamide followed by a split-dose infusion of CAR-modified T-lymphocytes. All 4 patients with detectable disease had CRs and became MRD negative between days 8–59 after infusion, enabling eligible patients to receive allogeneic SCT. One patient with overt disease prior to CAR infusion relapsed with CD19+ disease 90 days after treatment, and all patients showed signs of normal CD19+ B-cell recovery, highlighting that CAR T-cells in these patients did not persist indefinitely in contrast to those in the aforementioned CLL trial that harbored the 4-1BB costimulatory domain. Importantly in this ALL trial, toxicity in the form of cytokine release syndrome was associated with a larger burden of disease at the time of CAR infusion, and the 2 patients with morphologic disease prior to treatment required high-dose steroid therapy for cytokine release syndrome, which likely abrogated the therapeutic effects of the CAR-modified lymphocytes. The initial promising results from this trial were recently updated to include responses for 16 adult patients with relapsed or refractory ALL who have been treated on this protocol[170]. The overall complete response rate to date is 88%. In those patients with gross morphologic disease prior to CAR infusion, 78% have experienced a CR, allowing many to receive alloSCT. In this trial, the benefit of treating the cytokine release syndrome with the IL-6 monoclonal antibody, tocilizumab, was demonstrated, and it was shown to relieve symptoms with a less profound impact on CAR T-cell expansion when compared to high-dose steroids.
Impressive response rates have similarly been observed in a separate ongoing Phase I trial for pediatric and adult relapsed ALL patients, which incorporates the identical CAR construct used in the above-referenced CLL trial (lentiviral transduction with 4-1BB costimulatory domain). Results were first reported for 2 pediatric patients who both demonstrated complete morphologic response to CAR therapy within 1 month despite recalcitrant disease, though 1 child relapsed 2 months later with CD19 negative lymphoblasts[79]. Both patients experienced significant toxicity, and the first child that was treated demonstrated severe but reversible cytokine release syndrome necessitating mechanical ventilation, vasopressor support, and aggressive medical therapy. Despite this, the tremendous expansion of anti-CD19 CAR T-cells to > 1000-fold in vivo and their persistence in 1 patient for >180 days is incredibly promising. Updates from this trial were also reported at a recent ASH meeting[145]. A total of 16 children and 4 adults with relapsed ALL have been treated and 82% of patients have experienced CRs - 3 patients are still pending evaluation. Unfortunately, 3 patients with an initial CR have since relapsed, reportedly with CD19+ disease. All patients in this trial experienced some degree of cytokine release syndrome and, as shown in previous trials, tocilizumab proved beneficial.
Importantly, 11 of the patients in this ALL trial had received prior allogeneic SCT[145]. For this cohort, the cells used to generate the anti-CD19 CAR treatment were collected from the recipient, however depending on the degree of chimerism at the time of pheresis, the majority of these cells were of donor origin. Encouragingly, GvHD was not observed in this group despite pre-treatment with cyclophosphamide, a phenomenon that could be attributable to the donor cells having acquired tolerance in the host as all patients were at least 6 months post-SCT[145]. In the alloSCT setting, investigators have already undertaken the next logical step, which is to determine whether allogeneic cells collected from healthy donors can be modified with an anti-CD19 CAR construct and used to treat leukemia patients. The advantage of this method is twofold: first, there is no leukemic contamination of the infused cells and, second, healthy donor lymphocytes are potentially more potent cytotoxic effectors since they have not been exposed to multiple rounds of chemotherapy and immunosuppressive agents. The primary concern with infusing large numbers of allogeneic cells is for GvHD, the most frequent complication of donor lymphocyte infusion (DLI), and thus investigators have proceeded cautiously with this approach[9, 171]. In one study, 8 patients with relapsed ALL or CLL were treated with healthy donor allogeneic T-cells that were first enriched for virus-specific lymphocytes (cytomegalovirus (CMV), EBV, or adenovirus) prior to their transduction with a 2nd generation anti-CD19 CAR containing the CD28 costimulatory domain[138]. This approach is advantageous because the specificity of the endogenous TCR is for viral antigens and thus infusion of bispecific T-cells, those with endogenous TCRs specific for viral antigens and ectopic TCRs specific for CD19, poses less risk for GvHD. Furthermore, viral reactivation is common in the post-SCT setting and could expand modified, CAR-expressing T-cells through viral TCR-signaling and potentially enhance their antitumor effect. In this pilot trial, the bispecific T-cells persisted for a median of 8 weeks and resulted in 2 objective responses -1 CR for 3 months and 1 PR for 2 months. No GvHD was observed. As predicted, EBV reactivation in 2 patients resulted in a concomitant increase of CD19 CAR transgene expression.
Lastly, a recent trial at a separate center investigated the safety of treating relapsed post-SCT patients with anti-CD19-CAR T-cells collected from their healthy donors; however, in this trial the modified donor T-cells were not enriched for any particular endogenous specificity[146]. Ten patients with either relapsed CLL or lymphoma who had undergone prior alloSCT and at least 1 DLI were enrolled and underwent a single infusion of allogeneic CAR T-cells without any preparative lymphodepletion. Surprisingly, no GvHD was observed though CAR cells were largely undetectable after 1 month. Three patients experienced regressions of their malignancy, with 1 ongoing CR in a CLL patient at 9 months. The next planned trial of this allogeneic CD19 CAR-modified therapy will incorporate preparative lymphodepletion, which would be predicted to both increase the antitumor potency and potentially heighten the risk for GvHD.
Currently, there are 20 open trials listed on the clinicaltrials.gov website as of June 2014 that are studying anti-CD19 CAR therapy in various permutations. For example, one study is using autologous anti-CD19 CAR cells for children with relapsed ALL that incorporate an EGFRt tracking/suicide construct and a methotrexate-resistance gene (clinicaltrials.gov identifier NCT01683279). Several CD19 CAR trials are recruiting at Baylor including a Phase 1 trial that will study the simultaneous infusion of both 2nd and 3rd generation CARs in patients with Non-Hodgkin Lymphoma (NHL) or CLL (clinicaltrials.gov identifier NCT01853631). CARs targeting the CD19 antigen are leading the way in the clinic and insights gained from these trials will be invaluable for the entire field.
Wilms tumor antigen 1
The Wilms tumor protein (WT-1) is a zinc-finger transcription factor that is important in normal cellular development and cell survival. In the human embryo, WT-1 is required for normal kidney development and, in adults, WT-1 has low expression levels in hematopoietic progenitor cells and in the ovary, testis, podocytes of the kidney, and peritoneal and pleural mesothelium[172, 173]. Alternative splicing generates several isoforms of WT-1 and depending upon the cell in which the gene is expressed, it can function as either an oncogene or a tumor suppressor[174]. WT-1 represents a TAA as it is overexpressed in both leukemias (AML, CML, myelodysplastic syndrome [MDS], and ALL) and various solid tumors (ovary, breast, renal cell, colon, lung), where it acts as a putative oncogene[175–179]. Up to 70% of AML cases overexpress WT-1, where it is a marker of poor prognosis and minimal residual disease[180–183]. Although its precise biologic role in leukemia remains unknown, Yamagami et al. demonstrated that knockdown of WT-1 via antisense oligomers significantly inhibited the growth of primary leukemic clones, suggesting that the protein plays an important role in leukemogenesis[184]. Thus, WT-1 represents an attractive immunotherapeutic target, and there are currently 3 open clinical trials for adult leukemia patients that center around this unique antigen.
There are numerous preclinical studies that have demonstrated diverse and feasible approaches to target WT-1 in the clinic, and these have been expertly reviewed by O’Reilly et al. from MSKCC[185]. Briefly, several groups have demonstrated that WT-1-specific, functional CD4 and CD8 T-cells can be generated from healthy donor PBMC by stimulation with various WT-1 peptides[186–190]. Spontaneous autologous T-cell responses against WT-1 can also be detected in the peripheral blood of leukemia patients, providing rationale for either allogeneic or autologous ACT approaches[191, 192]. More recently, Xue et al. have engineered a retroviral vector encoding the T-cell receptor alpha and beta chains derived from a WT-1 TCR specific for the HLA-A0201-restricted RMF peptide. This TCR construct was optimized by incorporating a disulfide bond to prevent alpha/beta mispairing and, when transduced into a CML patient’s T-cells, mediated prevention of autologous leukemia engraftment in an immunocompromised mouse model[100, 193]. This TCR is now in clinical testing in London (see below). To broaden WT-1 specific ACT to patients with less common HLA subtypes, investigators have developed an elegant system in which donor T-cells are stimulated with pools of overlapping WT-1 peptides generating WT-1 specific T-cells with specificities that can be decoded using IFN-gamma secretion and a matrix of known peptide sequences. Using this approach T-cells specific for 27 different WT-1 peptides with diverse HLA-restriction were shown to lyse WT-1+ leukemic targets[194]. This approach, too, is now being tested in the clinic. As a final mention in the preclinical realm, Dao et al. have developed a full-length humanized TCR-mimic antibody from a phage display library that is specific for the WT-1 RMF peptide in the context of HLA-A0201. This antibody (ESK1) was shown to be highly avid and in 2 different mouse models, nearly ablated leukemia xenografts from 2 ALL cell lines, both alone and in concert with adoptive transfer of human effector cells[115]. The scFv from an affinity matured WT-1 TCR-mimic antibody has since been integrated into a CAR construct that has demonstrated lysis of solid tumor and B-cell leukemia cell lines[67].
As of June 2014, the clinicaltrials.gov website lists 3 Phase 1/2 trials that are using ACT to target the WT-1 antigen in leukemia patients. The first is based at University College in London and uses the retroviral vector developed by Xue et al. (discussed above) to redirect autologous T-cells from HLA-A0201-positive CML and AML patients via coexpression of a TCR specific for the A2-restricted WT-1 RMF peptide (clinicaltrials.gov identifier NCT01621724). This group hypothesizes that transducing and infusing fresh autologous, engineered T-cells will result in greater persistence of the WT-1 redirected cells compared to those from long-term culture. The second trial is sponsored by MSKCC and builds upon their success in generating functional, WT-1 specific T-cells from healthy donors with diverse HLA subtypes by in vitro stimulation with APCs pulsed with pools of overlapping WT-1 peptides[185, 194]. This trial includes patients with AML, MDS, CML or ALL who are at high risk of relapse after alloSCT and utilizes infusions of WT-1-specific donor T-cells that are expanded in vitro, cryopreserved, and then infused at the time of recurrence or appearance of MRD. Reportedly, these infusions have been well tolerated without renal, hematopoietic, or GvHD toxicity, and they can transiently reduce or eliminate WT-1-expressing cells from the circulation[185] (clinicaltrials.gov identifier NCT00620633). The third trial is based at the Fred Hutchinson Cancer Research Center in Seattle and builds upon this center’s success in an earlier pilot trial. In the pilot trial, 11 HLA-A201-positive patients with AML or ALL who had received alloSCT were treated with adoptive transfer of donor-derived, in vitro expanded WT-1 RMF peptide-specific CD8+ T-cells. Here, the addition of the cytokine IL-21 to the ex vivo T-cell expansion protocol for the last 4 patients resulted in improved persistence of the WT-1-specific T-cells and expression of phenotypic markers associated with long-lived memory[25]. The infusions of large numbers of WT-1 specific T-cells (up to 1 × 1010 cells/m2) were safe and no GvHD, hematologic, or renal toxicity was observed. Encouragingly, of the 4 patients treated with antigen-specific T-cells generated in the presence of IL-21, all 4 experienced persistence of the WT-1 specific T-cells and demonstrated durable CRs (22–38 months post SCT) despite a ~90-95% risk of recurrence, though 1 patient has since relapsed. In the current Phase 1/2 trial, a TCR isolated from a very high avidity T-cell clone specific for the A2-restricted RMF WT-1 peptide has been isolated and is being retrovirally transduced into donor T-cells (similar to the London trial except in an allogeneic setting). In this trial, eligible patients are those with AML, CML, or MDS who are post-SCT, HLA-A0201-positive, and are at high-risk of relapse or who recur with overt or MRD positive disease. These patients will be treated with multiple infusions of donor EBV or CMV-specific T-cells that are transduced to coexpress the WT-1 specific TCR. The rationale for transducing only virus-specific T-cells is that in the allogeneic setting, transduction of T-cells with unknown secondary specificities would likely result in considerable GvHD. Patients will also receive IL-2 infusions to boost persistence of the antigen-specific cells.
Lewis Y
The Lewis Y antigen (LeY) is a difucosylated carbohydrate present on various cell surface proteins and lipids[195]. It is related to the Lewis blood group of antigens but is not expressed on red blood cells. In normal tissues, the LeY antigen shows low levels of surface expression on the gastrointestinal mucosa, ciliated epithelium of the trachea and bronchus, and on neutrophils[196, 197]. It is primarily studied as a potential tumor-associated antigen (TAA) in the context of solid malignancies since the LeY antigen is highly expressed in 60-90% of epithelial cancers including those of the breast, pancreas, ovary, colon, stomach and lung[198, 199]. A recent study also showed expression of the Lewis Y antigen in ~ 50% of AML and multiple myeloma (MM) cases, suggesting it could be a targetable TAA in a wide range of malignancies[200]. Its biologic function remains unknown though higher expression of LeY correlates with poorer prognosis in lung cancer, suggesting a potential role for Lewis Y in maintaining a malignant phenotype[201].
Preclinical validation of the LeY antigen gained momentum when Kitamura et al. developed an anti-LeY humanized monoclonal antibody – known as Hu3S193[202]. This antibody was used alone and as an immunoconjugate in several early phase clinical trials targeting the Lewis Y antigen in patients, first in those with solid malignancies. The humanized monoclonal antibody Hu3S193 (also used to generate the anti-LeY CAR discussed below) was tested in a Phase I trial in 15 patients with primarily breast, colorectal, or lung cancer. There were no objective tumor responses, however, there was significant uptake of the antibody in tumor metastases and no uptake in normal tissue. Critically, the antibody infusion was safe with only one Grade 3 or 4 adverse effect - an elevated alkaline phosphatase in a patient with extensive hepatic metastases[203]. In an effort to increase the potency of tumor response, two Phase I trials were conducted using the Lewis Y antibody, Hu3S193, conjugated to either doxorubicin or calicheamicin. In the Hu3S193-doxorubicin immunoconjugate trial, 66 patients with mainly metastatic colon or breast cancer were treated, and significant, dose-limiting GI toxicity was observed, likely due to Lewis Y expression on normal GI epithelium. Objective responses were seen in only 2 patients[204]. In the Hu3S193-calicheamicin immunoconjugate trial, 9 patients with solid tumors were enrolled. Disappointingly, this conjugate showed primary localization to the liver instead of tumor and demonstrated rapid hepatic clearance from the circulation[205].
The promising yet limited effects of the Hu3S193 antibody laid the foundation for the targeting of LeY using ACT. In preclinical studies, Hu3S193 was used to generate a 2nd generation anti-LeY CAR, which was first tested against various malignant epithelial-derived cell lines and in a mouse xenograft model of ovarian cancer. The anti-LeY CAR T-cells lysed breast and colorectal cell lines in vitro, and lysis correlated positively with the level of LeY expression. Importantly, no IFN-γ release or lysis was observed against neutrophils, which have been shown to express Lewis Y at low levels. Further, in immunocompromised mice anti- LeY CAR T-cells mediated regression of established human ovarian tumors, though tumors did eventually recur[198]. More recently, this same CAR was used in preclinical testing against AML and MM, which also show overexpression of the Lewis Y antigen. The CAR T-cells lysed human MM and AML cell lines in vitro and delayed the incidence of plasmacytomas in a NOD/SCID mouse model, though no lysis of primary malignant cells or rejection of established myeloma or AML was demonstrated[200].
The first and (thus far) only ACT clinical trial targeting the LeY antigen in patients utilized the 2nd generation anti-LeY CAR mentioned above, which demonstrated activity against both solid and hematologic tumors in preclinical studies. Results from the first 5 enrolled patients, all with AML, were recently published and are summarized here[43]. This Phase I trial enrolled patients with high-risk or relapsed/refractory AML or MM whose tumors demonstrated expression of LeY on at least 20% of blasts, with a median fluorescence intensity twice that of normal lymphocytes. It is worth noting that the first 5 patients enrolled had relatively low Lewis Y expression compared to the patient samples used in the study that first described the presence of Lewis Y antigen in AML and MM[200]. Three of the four patients who underwent CAR T-cell infusion (one patient died from induction chemotherapy) had cytogenetic MRD prior to CAR T-cell infusion; the fourth patient had 70% blasts in the bone marrow as well as circulating disease. Patients were preconditioned with fludarabine and cytarabine and then infused with a median of 4.45 × 106 anti-LeY CAR T-cells/kg. As a comparison, these cell doses are comparable to those administered in the successful CD19 CAR clinical trials[134]. There were no grade 3 or 4 toxicities, and there was evidence of biologic activity though responses were modest at best. Of the 3 patients with MRD prior to CAR T-cell infusion, 1 demonstrated a sustained morphologic remission of 23 months though cytogenetic clones remained detectable, the 2nd patient showed a transient cytogenetic remission of 5 months, and the 3rd patient did not respond and relapsed 49 days after infusion. The 4th patient who had significant disease prior to anti-LeY CAR treatment had a very transient reduction in blasts, though the effect attributable to the CAR cells in the context of pretreatment with fludarabine and cytarabine is difficult to discern. Encouragingly, the CAR T-cells did show trafficking to the bone marrow and persisted in 3 of the 4 patients for 2, 4 and 10 months, though with variable transgene copy number by qualitative PCR. Perhaps most disappointingly, the 3 patients who showed some biologic response all relapsed with myeloblasts that still expressed the Lewis Y antigen with comparable MFIs to their pre-CAR treatment disease; there was no antigenic shift despite persistence of the CAR cells. The authors hypothesize that this could be due to an immunosuppressive microenvironment or downregulation in transgene expression. It might simply be related to the relatively low expression of Lewis Y on the myeloblasts and inadequate activation of the modified cells. The authors suggest the next anti-LeY CAR T-cell trial will be performed in lung cancer patients, where there is a more dense and uniform expression of the LeY antigen.
κ Light chain
The major long-term toxicity associated with the successful anti-CD19 CAR T-cell trials discussed above has been B-cell aplasia, which is secondary to the expression of CD19 on normal and B-cell precursors[79, 80, 134, 135, 164]. A strategy to avoid this adverse effect has been developed using engineered 2nd generation CAR T-cells with specificity for the κ light chain of surface immunoglobulin (sIg) within the B-cell receptor[206]. The concept behind this approach is that B-cell malignancies are clonal disorders wherein a patient’s malignant cells express a κ or λ-restricted sIg, but not both. In those patients with a κ-restricted malignancy, the anti-κ CAR T-cells would ideally eliminate all malignant cells and, consequently, normal B-cells with κ expression; however, normal λ-restricted B cells would be left untouched providing these patients with adequate B-cell immunity[207, 208].
In preclinical studies, the κ-light chain specific CAR T-cells selectively lysed κ-expressing lymphoma and leukemic cell lines as well as autologous and allogeneic κ-restricted primary CLL cells[206]. In vivo, human T-cells retrovirally transduced with the anti-κ CAR mediated regression of lymphoma xenografts. As an aside, this was among the first reports to show the importance of a CD28 costimulatory domain in the CAR construct, and it confirmed in this preclinical study that CD28 improved the expansion of the engineered anti-κ T-cells[206, 209]. A Phase I trial is currently recruiting patients with relapsed CLL, NHL, or MM to study treatment with autologous 2nd-generation anti-κ CAR T-cells (clinicaltrials.gov identifier NCT00881920). The trial will assess the safety and, as a secondary measure, the survival and function of anti-κ T-cells at 3 escalating T-cell doses after lymphodepletion with cyclophosphamide. It will be important to see whether antigen escape limits the success of this approach since MM and CLL are known to have variable expression of sIg[210–212]. Moreover, the antibody portion of the CAR construct is derived from a mouse, and the immunogenicity of this CAR in humans remains to be seen. Conversely and in support of this approach, targeting the B-cell receptor in lymphoma through idiotype vaccines has shown great promise and points to the feasibility of using the B-cell receptor (whether the idiotype or the light chain portion) as a TAA[41].
HA-1 and other minor histocompatibility antigens
As defined above, minor histocompatibility antigens (mHAs) are peptides derived from endogenous, polymorphic proteins that differ between donor and recipient and are thought to account for much of the GvL effect within HLA-matched donor-recipient pairs[213]. These antigens can also trigger GvHD, and therefore the major goal with mHAs has been to identify and target mHAs that show predominant expression in the hematopoietic compartment. Strong preclinical evidence for targeting these mHAs was demonstrated in an immunocompetent mouse model where targeting a single mHA (B6dom1) resulted in complete eradication of leukemia without GvHD[214]. Two recent clinical trials have investigated unique approaches towards this common objective of treating leukemia by targeting hematopoietic-restricted mHAs.
In one clinical trial utilizing adoptive transfer of mHA-specific T-cells, investigators first designed an in vitro culture system to enrich for mHA-specific donor T-cells[215]. In this trial, PBMC were collected from patients at post-transplant timepoints when their hematopoietic system had been replaced by donor cells. These donor-derived cells were then stimulated in vitro with pre-transplant, irradiated recipient PBMC and recipient EBV-LCLs (Epstein Barr Virus-transformed B lymphoblastoid cell lines) in an effort to generate donor T-cells specific for hematopoietic mHAs[216]. CD8+ T-cell clones were then generated using limiting dilution cloning. Donor CD8+ clones that lysed recipient EBV-LCLs but neither donor EBV-LCLs nor recipient fibroblasts were selected for treatment of 7 patients with relapsed MDS or ALL after alloSCT. Patients received cytoreductive chemotherapy but not specific lymphodepletion prior to T-cell infusions, which were administered in a dose-escalation protocol. Unfortunately, most of the patients had GvHD prior to treatment so it was difficult to grade the degree of GvHD caused by these T-cells, though no cases were directly attributable to the clones. Surprisingly, the major toxicity observed was pulmonary toxicity, which occurred in 3 patients and underscores the reality that adoptively transferred T-cells tend to initially accumulate in the lungs making this a vulnerable site for adverse effects[217]. Five of 7 patients achieved transient CRs, and 3 of these responses were directly attributable to the CTL clones and not the cytoreductive chemotherapy. A genome-wide, single nucleotide polymorphism-based correlation was used to identify the mHA targeted by 3 of the generated clones - 2 that were novel[218]. Interestingly, mRNA expression analysis suggested that leukemic blasts downregulated expression of 1 of the targeted mHAs after CTL treatment, again illustrating that it may be important to target proteins directly involved in leukemogenesis. Two of the patients who demonstrated significant pulmonary toxicity were infused with clones that recognized epitopes from proteins also expressed on the pulmonary alveolar epithelium, and the CTLs were shown to be directly causative in these adverse reactions. The CTLs showed potent effector function but did not persist past 21 days, possibly as a result of their extended time in culture that resulted in a differentiated, effector population of CD8+ T-cells. Unfortunately, all patients who demonstrated an initial response relapsed and succumbed to their disease.
In a more recent Phase I study, Meij et al. tested the feasibility and safety of treating relapsed post-SCT AML and CML patients with donor-derived T-cells specific for the mHA, HA-1[35, 219]. HA-1-specific T-cells were generated from healthy donor PBMC using donor dendritic cells pulsed with the HLA-A2 restricted HA-1 peptide during a 5-week in vitro culture period. The cells were then infused into patients in the absence of preconditioning or in vivo cytokine administration. The cells were primarily from the effector memory subset and 6-27% were tetramer positive (i.e. HA-1-specific). Unfortunately, no objective responses were demonstrated though a patient with CML did have stable disease for 3 months. HA-1 specific T-cells were detected only in this CML patient and were present for ~ 8 weeks. No GvHD was reported. The authors concluded that more potent responses might be generated by shortening the in vitro culture process possibly via ectopic TCR alpha/beta transfer and also through use of physiologic concentrations of cytokines during the in vitro expansion. Towards this goal, a codon optimized and cysteine modified HA-1-TCR α/β retroviral construct has been designed for use in clinical trials[108].
BCR-ABL
Tumor-specific antigens (neoantigens) within the BCR-ABL1 fusion tyrosine kinase have also been investigated as targets for ACT of CML. Several groups have shown that CML patients have functional, circulating T-cells specific for these neoantigens that can be expanded with a peptide vaccine[39, 53, 220]. A recent clinical trial investigated the feasibility and safety of prophylactically administering donor CD8+ T-cells enriched for specificities against peptides from WT-1, PR1, and BCR-ABL to CML patients after T-cell depleted alloSCT[57]. Five patients were treated with cells enriched for CTL with specificity for HLA-A3, A11, or B8-restricted BCR-ABL neopeptides. In these patients, the cells infused were largely polyclonal DLIs with wide ranges in the percentage of BCR-ABL-specific cells actually administered – from 0.1 – 17%. Though few patients were enrolled and the effects of therapy attributable to ACT are indiscernible from those related to alloSCT, 1 patient who received large numbers of BCR-ABL specific donor T-cells that exhibited robust in vitro cytotoxicity has remained in molecular remission for > 40 months and antigen-specific cells have persisted at high frequencies for >1 year.
A separate report described the successful treatment of a CML patient with leukemia-reactive CTL in 1999, prior to the advent of many of the engineering techniques now available. In this study, the CML patient had relapsed with accelerated-phase disease after alloSCT and DLI and was treated with donor cells enriched for leukemia-specific antigens via multiple rounds of in vitro stimulation with patient leukemia cells. The T-cells were not fully characterized but potentially recognized neoepitopes from BCR-ABL among others. This patient experienced molecular remission for 2 years until she later died of ischemic heart disease[221]. These studies offer proof-of-principle for targeting leukemia neoantigens though larger scale studies are needed using modified T-cells or updated in vitro expansion protocols. Table 2 summarizes the antigens discussed in the section.
Conclusions
In summary, ACT represents a promising strategy for treating leukemia patients. The list of antigens discussed above is by no means exhaustive and many ACT strategies are in the pipeline to target other leukemia antigens including PR1[29], human telomerase reverse transcriptase (hTERT)[26], receptor tyrosine kinase-like orphan receptor 1 (ROR1)[45], CD23[223], CD123[224], preferentially expressed antigen in melanoma (PRAME)[27], hyaluronan-mediated motility receptor (HMMR/Rhamm)[28], CD22[44], cathepsin G[30] and aurora kinase a (AURKA)[225] among others. The clinical success achieved using anti-CD19 CARs has shifted momentum in favor of this type of engineered receptor, but exciting clinical trials utilizing ectopic TCR α/β receptors and even conventional T-cells are also underway. Significant challenges remain in outlining the best setting for ACT of leukemia, though this will likely vary by disease type, targeted antigen, and T-cell approach. Moreover, incorporating automation and standardization will be critical to shifting the ACT field away from intricate protocols and small, single-center trials towards broader applicability. The goal is to harness and refine the tremendous specificity and potency of lymphocytes, best evidenced by the ability of alloSCT and DLI to cure otherwise incurable diseases (CML, CLL), into a T-cell treatment for leukemia that is more effective and less toxic than current standard of care therapies.
Abbreviations
- ALL:
-
Acute lymphoblastic leukemia
- AML:
-
Acute myeloid leukemia
- ACT:
-
Adoptive cellular therapy
- alloSCT:
-
Allogeneic stem cell transplantation
- APCs:
-
Antigen presenting cells
- CAR:
-
Chimeric antigen receptor
- CLL:
-
Chronic lymphocytic leukemia
- CML:
-
Chronic myeloid leukemia
- CR:
-
Complete response
- CMV:
-
Cytomegalovirus
- CTLs:
-
Cytotoxic T-lymphocytes
- DLI:
-
Donor lymphocyte infusion
- EBV:
-
Epstein Barr Virus
- GvHD:
-
Graft-versus-host disease
- GvL:
-
Graft-versus-leukemia
- HLA:
-
Human leukocyte antigen
- MHC:
-
Major histocompatibility complex
- MRD:
-
Minimal residual disease
- mHA:
-
Minor histocompatibility antigen
- MM:
-
Multiple myeloma
- MDS:
-
Myelodysplastic syndrome
- NK cell:
-
Natural killer cell
- NHL:
-
Non-Hodgkin Lymphoma
- PR:
-
Partial response
- PBMCs:
-
Peripheral blood mononuclear cells
- PTLD:
-
Post-allogeneic stem cell transplant lymphoproliferative disease
- scFv:
-
Single chain variable fragment
- sIg:
-
Surface immunoglobulin
- TCR:
-
T-cell receptor
- TAA:
-
Tumor-associated antigen
- TIL:
-
Tumor infiltrating lymphocyte
- WT-1:
-
Wilms tumor antigen.
References
Apperley JF, Jones L, Hale G, Waldmann H, Hows J, Rombos Y, Tsatalas C, Marcus RE, Goolden AW, Gordon-Smith EC: Bone marrow transplantation for patients with chronic myeloid leukaemia: T-cell depletion with Campath-1 reduces the incidence of graft-versus-host disease but may increase the risk of leukaemic relapse. Bone Marrow Transplant. 1986, 1: 53-66.
Horowitz MM, Gale RP, Sondel PM, Goldman JM, Kersey J, Kolb HJ, Rimm AA, Ringden O, Rozman C, Speck B: Graft-versus-leukemia reactions after bone marrow transplantation. Blood. 1990, 75: 555-562.
Wagner JE, Thompson JS, Carter SL, Kernan NA, Unrelated Donor Marrow Transplantation T: Effect of graft-versus-host disease prophylaxis on 3-year disease-free survival in recipients of unrelated donor bone marrow (T-cell Depletion Trial): a multi-centre, randomised phase II-III trial. Lancet. 2005, 366: 733-741.
Korngold R, Leighton C, Manser T: Graft-versus-myeloid leukemia responses following syngeneic and allogeneic bone marrow transplantation. Transplantation. 1994, 58: 278-287.
Marmont AM, Horowitz MM, Gale RP, Sobocinski K, Ash RC, van Bekkum DW, Champlin RE, Dicke KA, Goldman JM, Good RA: T-cell depletion of HLA-identical transplants in leukemia. Blood. 1991, 78: 2120-2130.
Pollard CM, Powles RL, Millar JL, Shepherd V, Milan S, Lakhani A, Zuiable A, Treleaven J, Helenglass G: Leukaemic relapse following Campath 1 treated bone marrow transplantation for leukaemia. Lancet. 1986, 2: 1343-1344.
Collins RH, Goldstein S, Giralt S, Levine J, Porter D, Drobyski W, Barrett J, Johnson M, Kirk A, Horowitz M, Parker P: Donor leukocyte infusions in acute lymphocytic leukemia. Bone Marrow Transplant. 2000, 26: 511-516.
Collins RH, Shpilberg O, Drobyski WR, Porter DL, Giralt S, Champlin R, Goodman SA, Wolff SN, Hu W, Verfaillie C, List A, Dalton W, Ognoskie N, Chetrit A, Antin JH, Nemunaitis J: Donor leukocyte infusions in 140 patients with relapsed malignancy after allogeneic bone marrow transplantation. J Clin Oncol. 1997, 15: 433-444.
Kolb HJ, Schattenberg A, Goldman JM, Hertenstein B, Jacobsen N, Arcese W, Ljungman P, Ferrant A, Verdonck L, Niederwieser D, van Rhee F, Mittermueller J, de Witte T, Holler E, Ansari H, European Group for B, Marrow Transplantation Working Party Chronic L: Graft-versus-leukemia effect of donor lymphocyte transfusions in marrow grafted patients. Blood. 1995, 86: 2041-2050.
Khouri IF, Lee MS, Saliba RM, Andersson B, Anderlini P, Couriel D, Hosing C, Giralt S, Korbling M, McMannis J, Keating MJ, Champlin RE: Nonablative allogeneic stem cell transplantation for chronic lymphocytic leukemia: impact of rituximab on immunomodulation and survival. Exp Hematol. 2004, 32: 28-35.
Levine JE, Braun T, Penza SL, Beatty P, Cornetta K, Martino R, Drobyski WR, Barrett AJ, Porter DL, Giralt S, Leis J, Holmes HE, Johnson M, Horowitz M, Collins RH: Prospective trial of chemotherapy and donor leukocyte infusions for relapse of advanced myeloid malignancies after allogeneic stem-cell transplantation. J Clin Oncol. 2002, 20: 405-412.
Kolb HJ: Graft-versus-leukemia effects of transplantation and donor lymphocytes. Blood. 2008, 112: 4371-4383.
Bleakley M, Riddell SR: Molecules and mechanisms of the graft-versus-leukaemia effect. Nat Rev Cancer. 2004, 4: 371-380.
Alatrash G, Molldrem JJ: Vaccines as consolidation therapy for myeloid leukemia. Expert Rev Hematol. 2011, 4: 37-50.
Rosenberg SA: Raising the bar: the curative potential of human cancer immunotherapy. Sci Transl Med. 2012, 4: 127ps128-
Tran E, Turcotte S, Gros A, Robbins PF, Lu YC, Dudley ME, Wunderlich JR, Somerville RP, Hogan K, Hinrichs CS, Parkhurst MR, Yang JC, Rosenberg SA: Cancer immunotherapy based on mutation-specific CD4+ T cells in a patient with epithelial cancer. Science. 2014, 344: 641-645.
Schietinger A, Greenberg PD: Tolerance and exhaustion: defining mechanisms of T cell dysfunction. Trends Immunol. 2014, 35: 51-60.
Cheever MA, Allison JP, Ferris AS, Finn OJ, Hastings BM, Hecht TT, Mellman I, Prindiville SA, Viner JL, Weiner LM, Matrisian LM: The prioritization of cancer antigens: a national cancer institute pilot project for the acceleration of translational research. Clin Cancer Res. 2009, 15: 5323-5337.
Inoue K, Ogawa H, Sonoda Y, Kimura T, Sakabe H, Oka Y, Miyake S, Tamaki H, Oji Y, Yamagami T, Tatekawa T, Soma T, Kishimoto T, Sugiyama H: Aberrant overexpression of the Wilms tumor gene (WT1) in human leukemia. Blood. 1997, 89: 1405-1412.
Pham CT: Neutrophil serine proteases: specific regulators of inflammation. Nat Rev Immunol. 2006, 6: 541-550.
Molldrem J, Dermime S, Parker K, Jiang YZ, Mavroudis D, Hensel N, Fukushima P, Barrett AJ: Targeted T-cell therapy for human leukemia: cytotoxic T lymphocytes specific for a peptide derived from proteinase 3 preferentially lyse human myeloid leukemia cells. Blood. 1996, 88: 2450-2457.
Molldrem JJ, Lee PP, Wang C, Felio K, Kantarjian HM, Champlin RE, Davis MM: Evidence that specific T lymphocytes may participate in the elimination of chronic myelogenous leukemia. Nat Med. 2000, 6: 1018-1023.
Hofmann O, Caballero OL, Stevenson BJ, Chen YT, Cohen T, Chua R, Maher CA, Panji S, Schaefer U, Kruger A, Lehvaslaiho M, Carninci P, Hayashizaki Y, Jongeneel CV, Simpson AJ, Old LJ, Hide W: Genome-wide analysis of cancer/testis gene expression. Proc Natl Acad Sci U S A. 2008, 105: 20422-20427.
Parkhurst MR, Yang JC, Langan RC, Dudley ME, Nathan DA, Feldman SA, Davis JL, Morgan RA, Merino MJ, Sherry RM, Hughes MS, Kammula US, Phan GQ, Lim RM, Wank SA, Restifo NP, Robbins PF, Laurencot CM, Rosenberg SA: T cells targeting carcinoembryonic antigen can mediate regression of metastatic colorectal cancer but induce severe transient colitis. Mol Ther. 2011, 19: 620-626.
Chapuis AG, Ragnarsson GB, Nguyen HN, Chaney CN, Pufnock JS, Schmitt TM, Duerkopp N, Roberts IM, Pogosov GL, Ho WY, Ochsenreither S, Wolfl M, Bar M, Radich JP, Yee C, Greenberg PD: Transferred WT1-reactive CD8+ T cells can mediate antileukemic activity and persist in post-transplant patients. Sci Transl Med. 2013, 5: 174ra127-
Miyazaki Y, Fujiwara H, Asai H, Ochi F, Ochi T, Azuma T, Ishida T, Okamoto S, Mineno J, Kuzushima K, Shiku H, Yasukawa M: Development of a novel redirected T-cell-based adoptive immunotherapy targeting human telomerase reverse transcriptase for adult T-cell leukemia. Blood. 2013, 121: 4894-4901.
Amir AL, van der Steen DM, van Loenen MM, Hagedoorn RS, de Boer R, Kester MD, de Ru AH, Lugthart GJ, van Kooten C, Hiemstra PS, Jedema I, Griffioen M, van Veelen PA, Falkenburg JH, Heemskerk MH: PRAME-specific Allo-HLA-restricted T cells with potent antitumor reactivity useful for therapeutic T-cell receptor gene transfer. Clin Cancer Res. 2011, 17: 5615-5625.
Spranger S, Jeremias I, Wilde S, Leisegang M, Starck L, Mosetter B, Uckert W, Heemskerk MH, Schendel DJ, Frankenberger B: TCR-transgenic lymphocytes specific for HMMR/Rhamm limit tumor outgrowth in vivo. Blood. 2012, 119: 3440-3449.
Ma Q, Wang C, Jones D, Quintanilla KE, Li D, Wang Y, Wieder ED, Clise-Dwyer K, Alatrash G, Mj Y, Munsell MF, Lu S, Qazilbash MH, Molldrem JJ: Adoptive transfer of PR1 cytotoxic T lymphocytes associated with reduced leukemia burden in a mouse acute myeloid leukemia xenograft model. Cytotherapy. 2010, 12: 1056-1062.
Zhang M, Sukhumalchandra P, Enyenihi AA, St John LS, Hunsucker SA, Mittendorf EA, Sergeeva A, Ruisaard K, Al-Atrache Z, Ropp PA, Jakher H, Rodriguez-Cruz T, Lizee G, Clise-Dwyer K, Lu S, Molldrem JJ, Glish GL, Armistead PM, Alatrash G: A novel HLA-A*0201 restricted peptide derived from cathepsin G is an effective immunotherapeutic target in acute myeloid leukemia. Clin Cancer Res. 2013, 19: 247-257.
Pizzitola I, Anjos-Afonso F, Rouault-Pierre K, Lassailly F, Tettamanti S, Spinelli O, Biondi A, Biagi E, Bonnet D: Chimeric antigen receptors against CD33/CD123 antigens efficiently target primary acute myeloid leukemia cells in vivo. Leukemia. 2014, Feb 7 [epub ahead of print]
Ochsenreither S, Majeti R, Schmitt T, Stirewalt D, Keilholz U, Loeb KR, Wood B, Choi YE, Bleakley M, Warren EH, Hudecek M, Akatsuka Y, Weissman IL, Greenberg PD: Cyclin-A1 represents a new immunogenic targetable antigen expressed in acute myeloid leukemia stem cells with characteristics of a cancer-testis antigen. Blood. 2012, 119: 5492-5501.
Klippel ZK, Chou J, Towlerton AM, Voong LN, Robbins P, Bensinger WI, Warren EH: Immune escape from NY-ESO-1-specific T-cell therapy via loss of heterozygosity in the MHC. Gene Ther. 2014, 21: 337-342.
Goodyear O, Agathanggelou A, Novitzky-Basso I, Siddique S, McSkeane T, Ryan G, Vyas P, Cavenagh J, Stankovic T, Moss P, Craddock C: Induction of a CD8+ T-cell response to the MAGE cancer testis antigen by combined treatment with azacitidine and sodium valproate in patients with acute myeloid leukemia and myelodysplasia. Blood. 2010, 116: 1908-1918.
Meij P, Jedema I, van der Hoorn MA, Bongaerts R, Cox L, Wafelman AR, Marijt EW, Willemze R, Falkenburg JH: Generation and administration of HA-1-specific T-cell lines for the treatment of patients with relapsed leukemia after allogeneic stem cell transplantation: a pilot study. Haematologica. 2012, 97: 1205-1208.
Akatsuka Y, Nishida T, Kondo E, Miyazaki M, Taji H, Iida H, Tsujimura K, Yazaki M, Naoe T, Morishima Y, Kodera Y, Kuzushima K, Takahashi T: Identification of a polymorphic gene, BCL2A1, encoding two novel hematopoietic lineage-specific minor histocompatibility antigens. J Exp Med. 2003, 197: 1489-1500.
Armistead PM, Liang S, Li H, Lu S, Van Bergen CA, Alatrash G, St John L, Hunsucker SA, Sarantopoulos S, Falkenburg JH, Molldrem JJ: Common minor histocompatibility antigen discovery based upon patient clinical outcomes and genomic data. PloS one. 2011, 6: e23217-
Stumpf AN, van der Meijden ED, van Bergen CA, Willemze R, Falkenburg JH, Griffioen M: Identification of 4 new HLA-DR-restricted minor histocompatibility antigens as hematopoietic targets in antitumor immunity. Blood. 2009, 114: 3684-3692.
Rezvani K, Grube M, Brenchley JM, Sconocchia G, Fujiwara H, Price DA, Gostick E, Yamada K, Melenhorst J, Childs R, Hensel N, Douek DC, Barrett AJ: Functional leukemia-associated antigen-specific memory CD8+ T cells exist in healthy individuals and in patients with chronic myelogenous leukemia before and after stem cell transplantation. Blood. 2003, 102: 2892-2900.
Graf C, Heidel F, Tenzer S, Radsak MP, Solem FK, Britten CM, Huber C, Fischer T, Wolfel T: A neoepitope generated by an FLT3 internal tandem duplication (FLT3-ITD) is recognized by leukemia-reactive autologous CD8+ T cells. Blood. 2007, 109: 2985-2988.
Schuster SJ, Neelapu SS, Gause BL, Janik JE, Muggia FM, Gockerman JP, Winter JN, Flowers CR, Nikcevich DA, Sotomayor EM, McGaughey DS, Jaffe ES, Chong EA, Reynolds CW, Berry DA, Santos CF, Popa MA, McCord AM, Kwak LW: Vaccination with patient-specific tumor-derived antigen in first remission improves disease-free survival in follicular lymphoma. J Clin Oncol. 2011, 29: 2787-2794.
Tamai Y, Hasegawa A, Takamori A, Sasada A, Tanosaki R, Choi I, Utsunomiya A, Maeda Y, Yamano Y, Eto T, Koh KR, Nakamae H, Suehiro Y, Kato K, Takemoto S, Okamura J, Uike N, Kannagi M: Potential contribution of a novel Tax epitope-specific CD4+ T cells to graft-versus-Tax effect in adult T cell leukemia patients after allogeneic hematopoietic stem cell transplantation. J Immunol. 2013, 190: 4382-4392.
Ritchie DS, Neeson PJ, Khot A, Peinert S, Tai T, Tainton K, Chen K, Shin M, Wall DM, Honemann D, Gambell P, Westerman DA, Haurat J, Westwood JA, Scott AM, Kravets L, Dickinson M, Trapani JA, Smyth MJ, Darcy PK, Kershaw MH, Prince HM: Persistence and efficacy of second generation CAR T cell against the LeY antigen in acute myeloid leukemia. Mol Ther. 2013, 21: 2122-2129.
Fry TJ, Mackall CL: T-cell adoptive immunotherapy for acute lymphoblastic leukemia. Hematology Am Soc Hematol Educ Program. 2013, 2013: 348-353.
Hudecek M, Lupo-Stanghellini MT, Kosasih PL, Sommermeyer D, Jensen MC, Rader C, Riddell SR: Receptor affinity and extracellular domain modifications affect tumor recognition by ROR1-specific chimeric antigen receptor T cells. Clin Cancer Res. 2013, 19: 3153-3164.
Bleakley M, Turtle CJ, Riddell SR: Augmentation of anti-tumor immunity by adoptive T-cell transfer after allogeneic hematopoietic stem cell transplantation. Expert Rev Hematol. 2012, 5: 409-425.
Robbins PF, Lu YC, El-Gamil M, Li YF, Gross C, Gartner J, Lin JC, Teer JK, Cliften P, Tycksen E, Samuels Y, Rosenberg SA: Mining exomic sequencing data to identify mutated antigens recognized by adoptively transferred tumor-reactive T cells. Nat Med. 2013, 19: 747-752.
Lu YC, Yao X, Li YF, El-Gamil M, Dudley ME, Yang JC, Almeida JR, Douek DC, Samuels Y, Rosenberg SA, Robbins PF: Mutated PPP1R3B is recognized by T cells used to treat a melanoma patient who experienced a durable complete tumor regression. J Immunol. 2013, 190: 6034-6042.
van Rooij N, van Buuren MM, Philips D, Velds A, Toebes M, Heemskerk B, van Dijk LJ, Behjati S, Hilkmann H, El Atmioui D, Nieuwland M, Stratton MR, Kerkhoven RM, Kesmir C, Haanen JB, Kvistborg P, Schumacher TN: Tumor exome analysis reveals neoantigen-specific T-cell reactivity in an ipilimumab-responsive melanoma. J Clin Oncol. 2013, 31: e439-442.
Mardis ER, Ding L, Dooling DJ, Larson DE, McLellan MD, Chen K, Koboldt DC, Fulton RS, Delehaunty KD, McGrath SD, Fulton LA, Locke DP, Magrini VJ, Abbott RM, Vickery TL, Reed JS, Robinson JS, Wylie T, Smith SM, Carmichael L, Eldred JM, Harris CC, Walker J, Peck JB, Du F, Dukes AF, Sanderson GE, Brummett AM, Clark E, McMichael JF: Recurring mutations found by sequencing an acute myeloid leukemia genome. N Engl J Med. 2009, 361: 1058-1066.
Wang L, Lawrence MS, Wan Y, Stojanov P, Sougnez C, Stevenson K, Werner L, Sivachenko A, DeLuca DS, Zhang L, Zhang W, Vartanov AR, Fernandes SM, Goldstein NR, Folco EG, Cibulskis K, Tesar B, Sievers QL, Shefler E, Gabriel S, Hacohen N, Reed R, Meyerson M, Golub TR, Lander ES, Neuberg D, Brown JR, Getz G, Wu CJ: SF3B1 and other novel cancer genes in chronic lymphocytic leukemia. N Engl J Med. 2011, 365: 2497-2506.
Bocchia M, Wentworth PA, Southwood S, Sidney J, McGraw K, Scheinberg DA, Sette A: Specific binding of leukemia oncogene fusion protein peptides to HLA class I molecules. Blood. 1995, 85: 2680-2684.
Butt NM, Rojas JM, Wang L, Christmas SE, Abu-Eisha HM, Clark RE: Circulating bcr-abl-specific CD8+ T cells in chronic myeloid leukemia patients and healthy subjects. Haematologica. 2005, 90: 1315-1323.
Clark RE, Dodi IA, Hill SC, Lill JR, Aubert G, Macintyre AR, Rojas J, Bourdon A, Bonner PL, Wang L, Christmas SE, Travers PJ, Creaser CS, Rees RC, Madrigal JA: Direct evidence that leukemic cells present HLA-associated immunogenic peptides derived from the BCR-ABL b3a2 fusion protein. Blood. 2001, 98: 2887-2893.
Yotnda P, Firat H, Garcia-Pons F, Garcia Z, Gourru G, Vernant JP, Lemonnier FA, Leblond V, Langlade-Demoyen P: Cytotoxic T cell response against the chimeric p210 BCR-ABL protein in patients with chronic myelogenous leukemia. J Clin Invest. 1998, 101: 2290-2296.
Bornhauser M, Thiede C, Babatz J, Schetelig J, Illmer T, Kiani A, Platzbecker U, Herr W, Rieber EP, Ehninger G, Schmitz M: Infusion of bcr/abl peptide-reactive donor T cells to achieve molecular remission of chronic myeloid leukemia after CD34+ selected allogeneic hematopoietic cell transplantation. Leukemia. 2006, 20: 2055-2057.
Bornhauser M, Thiede C, Platzbecker U, Kiani A, Oelschlaegel U, Babatz J, Lehmann D, Holig K, Radke J, Tuve S, Wermke M, Wehner R, Jahnisch H, Bachmann MP, Rieber EP, Schetelig J, Ehninger G, Schmitz M: Prophylactic transfer of BCR-ABL-, PR1-, and WT1-reactive donor T cells after T cell-depleted allogeneic hematopoietic cell transplantation in patients with chronic myeloid leukemia. Blood. 2011, 117: 7174-7184.
Stevenson GT, Stevenson FK: Antibody to a molecularly-defined antigen confined to a tumour cell surface. Nature. 1975, 254: 714-716.
de Vos van Steenwijk PJ, Heusinkveld M, Ramwadhdoebe TH, Lowik MJ, van der Hulst JM, Goedemans R, Piersma SJ, Kenter GG, van der Burg SH: An unexpectedly large polyclonal repertoire of HPV-specific T cells is poised for action in patients with cervical cancer. Cancer Res. 2010, 70: 2707-2717.
Heslop HE, Slobod KS, Pule MA, Hale GA, Rousseau A, Smith CA, Bollard CM, Liu H, Wu MF, Rochester RJ, Amrolia PJ, Hurwitz JL, Brenner MK, Rooney CM: Long-term outcome of EBV-specific T-cell infusions to prevent or treat EBV-related lymphoproliferative disease in transplant recipients. Blood. 2010, 115: 925-935.
Bollard CM, Gottschalk S, Leen AM, Weiss H, Straathof KC, Carrum G, Khalil M, Wu MF, Huls MH, Chang CC, Gresik MV, Gee AP, Brenner MK, Rooney CM, Heslop HE: Complete responses of relapsed lymphoma following genetic modification of tumor-antigen presenting cells and T-lymphocyte transfer. Blood. 2007, 110: 2838-2845.
Kurihara K, Shimizu Y, Takamori A, Harashima N, Noji M, Masuda T, Utsunomiya A, Okamura J, Kannagi M: Human T-cell leukemia virus type-I (HTLV-I)-specific T-cell responses detected using three-divided glutathione-S-transferase (GST)-Tax fusion proteins. J Immunol Methods. 2006, 313: 61-73.
Aleksic M, Liddy N, Molloy PE, Pumphrey N, Vuidepot A, Chang KM, Jakobsen BK: Different affinity windows for virus and cancer-specific T-cell receptors: implications for therapeutic strategies. Eur J Immunol. 2012, 42: 3174-3179.
Schreiber RD, Old LJ, Smyth MJ: Cancer immunoediting: integrating immunity's roles in cancer suppression and promotion. Science. 2011, 331: 1565-1570.
Gross G, Waks T, Eshhar Z: Expression of immunoglobulin-T-cell receptor chimeric molecules as functional receptors with antibody-type specificity. Proc Natl Acad Sci U S A. 1989, 86: 10024-10028.
Kershaw MH, Westwood JA, Darcy PK: Gene-engineered T cells for cancer therapy. Nat Rev Cancer. 2013, 13: 525-541.
Kuo T, Hasan A, Zhao Q, Selvakumar A: T Cells Expressing Cars Directed Against HLA-0201-Rmf WT-1 Peptide Complex Can Effectively Eradicate WT1+ A0201+ Tumor Cells In-Vitro. Biol Blood Marrow Transplant. 2014, 20: S132-S133.
Deniger DC, Switzer K, Mi T, Maiti S, Hurton L, Singh H, Huls H, Olivares S, Lee DA, Champlin RE, Cooper LJ: Bispecific T-cells expressing polyclonal repertoire of endogenous gammadelta T-cell receptors and introduced CD19-specific chimeric antigen receptor. Mol Ther. 2013, 21: 638-647.
Shimasaki N, Campana D: Natural killer cell reprogramming with chimeric immune receptors. Methods Mol Biol. 2013, 969: 203-220.
Sangiolo D, Mesiano G, Carnevale-Schianca F, Piacibello W, Aglietta M, Cignetti A: Cytokine induced killer cells as adoptive immunotherapy strategy to augment graft versus tumor after hematopoietic cell transplantation. Expert Opin Biol Ther. 2009, 9: 831-840.
East JE, Sun W, Webb TJ: Artificial antigen presenting cell (aAPC) mediated activation and expansion of natural killer T cells. J Vis Exp. 2012
Papadopoulos EB, Ladanyi M, Emanuel D, Mackinnon S, Boulad F, Carabasi MH, Castro-Malaspina H, Childs BH, Gillio AP, Small TN, Young JW, Kernan NA, O'Reilly RJ: Infusions of donor leukocytes to treat Epstein-Barr virus-associated lymphoproliferative disorders after allogeneic bone marrow transplantation. N Engl J Med. 1994, 330: 1185-1191.
Walter EA, Greenberg PD, Gilbert MJ, Finch RJ, Watanabe KS, Thomas ED, Riddell SR: Reconstitution of cellular immunity against cytomegalovirus in recipients of allogeneic bone marrow by transfer of T-cell clones from the donor. N Engl J Med. 1995, 333: 1038-1044.
Rooney CM, Smith CA, Ng CY, Loftin S, Li C, Krance RA, Brenner MK, Heslop HE: Use of gene-modified virus-specific T lymphocytes to control Epstein-Barr-virus-related lymphoproliferation. Lancet. 1995, 345: 9-13.
Riddell SR, Watanabe KS, Goodrich JM, Li CR, Agha ME, Greenberg PD: Restoration of viral immunity in immunodeficient humans by the adoptive transfer of T cell clones. Science. 1992, 257: 238-241.
Peggs KS, Verfuerth S, Pizzey A, Khan N, Guiver M, Moss PA, Mackinnon S: Adoptive cellular therapy for early cytomegalovirus infection after allogeneic stem-cell transplantation with virus-specific T-cell lines. Lancet. 2003, 362: 1375-1377.
Leen AM, Christin A, Myers GD, Liu H, Cruz CR, Hanley PJ, Kennedy-Nasser AA, Leung KS, Gee AP, Krance RA, Brenner MK, Heslop HE, Rooney CM, Bollard CM: Cytotoxic T lymphocyte therapy with donor T cells prevents and treats adenovirus and Epstein-Barr virus infections after haploidentical and matched unrelated stem cell transplantation. Blood. 2009, 114: 4283-4292.
Leen AM, Myers GD, Sili U, Huls MH, Weiss H, Leung KS, Carrum G, Krance RA, Chang CC, Molldrem JJ, Gee AP, Brenner MK, Heslop HE, Rooney CM, Bollard CM: Monoculture-derived T lymphocytes specific for multiple viruses expand and produce clinically relevant effects in immunocompromised individuals. Nat Med. 2006, 12: 1160-1166.
Grupp SA, Kalos M, Barrett D, Aplenc R, Porter DL, Rheingold SR, Teachey DT, Chew A, Hauck B, Wright JF, Milone MC, Levine BL, June CH: Chimeric antigen receptor-modified T cells for acute lymphoid leukemia. N Engl J Med. 2013, 368: 1509-1518.
Porter DL, Levine BL, Kalos M, Bagg A, June CH: Chimeric antigen receptor-modified T cells in chronic lymphoid leukemia. N Engl J Med. 2011, 365: 725-733.
Rapoport AP, Aqui NA, Stadtmauer EA, Vogl DT, Fang HB, Cai L, Janofsky S, Chew A, Storek J, Akpek G, Badros A, Yanovich S, Tan MT, Veloso E, Pasetti MF, Cross A, Philip S, Murphy H, Bhagat R, Zheng Z, Milliron T, Cotte J, Cannon A, Levine BL, Vonderheide RH, June CH: Combination immunotherapy using adoptive T-cell transfer and tumor antigen vaccination on the basis of hTERT and survivin after ASCT for myeloma. Blood. 2011, 117: 788-797.
Hardy NM, Fellowes V, Rose JJ, Odom J, Pittaluga S, Steinberg SM, Blacklock-Schuver B, Avila DN, Memon S, Kurlander RJ, Khuu HM, Stetler-Stevenson M, Mena E, Dwyer AJ, Levine BL, June CH, Reshef R, Vonderheide RH, Gress RE, Fowler DH, Hakim FT, Bishop MR: Costimulated tumor-infiltrating lymphocytes are a feasible and safe alternative donor cell therapy for relapse after allogeneic stem cell transplantation. Blood. 2012, 119: 2956-2959.
Rosenberg SA, Yang JC, Sherry RM, Kammula US, Hughes MS, Phan GQ, Citrin DE, Restifo NP, Robbins PF, Wunderlich JR, Morton KE, Laurencot CM, Steinberg SM, White DE, Dudley ME: Durable complete responses in heavily pretreated patients with metastatic melanoma using T-cell transfer immunotherapy. Clin Cancer Res. 2011, 17: 4550-4557.
Weber G, Caruana I, Rouce RH, Barrett AJ, Gerdemann U, Leen AM, Rabin KR, Bollard CM: Generation of tumor antigen-specific T cell lines from pediatric patients with acute lymphoblastic leukemia–implications for immunotherapy. Clin Cancer Res. 2013, 19: 5079-5091.
Mariotti S, Nisini R: Generation of human T cell clones. Methods Mol Biol. 2009, 514: 65-93.
Okamoto S, Mineno J, Ikeda H, Fujiwara H, Yasukawa M, Shiku H, Kato I: Improved expression and reactivity of transduced tumor-specific TCRs in human lymphocytes by specific silencing of endogenous TCR. Cancer Res. 2009, 69: 9003-9011.
Hacein-Bey-Abina S, Garrigue A, Wang GP, Soulier J, Lim A, Morillon E, Clappier E, Caccavelli L, Delabesse E, Beldjord K, Asnafi V, MacIntyre E, Dal Cortivo L, Radford I, Brousse N, Sigaux F, Moshous D, Hauer J, Borkhardt A, Belohradsky BH, Wintergerst U, Velez MC, Leiva L, Sorensen R, Wulffraat N, Blanche S, Bushman FD, Fischer A, Cavazzana-Calvo M: Insertional oncogenesis in 4 patients after retrovirus-mediated gene therapy of SCID-X1. J Clin Invest. 2008, 118: 3132-3142.
Scholler J, Brady TL, Binder-Scholl G, Hwang WT, Plesa G, Hege KM, Vogel AN, Kalos M, Riley JL, Deeks SG, Mitsuyasu RT, Bernstein WB, Aronson NE, Levine BL, Bushman FD, June CH: Decade-long safety and function of retroviral-modified chimeric antigen receptor T cells. Sci Transl Med. 2012, 4: 132ra153-
Linette GP, Stadtmauer EA, Maus MV, Rapoport AP, Levine BL, Emery L, Litzky L, Bagg A, Carreno BM, Cimino PJ, Binder-Scholl GK, Smethurst DP, Gerry AB, Pumphrey NJ, Bennett AD, Brewer JE, Dukes J, Harper J, Tayton-Martin HK, Jakobsen BK, Hassan NJ, Kalos M, June CH: Cardiovascular toxicity and titin cross-reactivity of affinity-enhanced T cells in myeloma and melanoma. Blood. 2013, 122: 863-871.
Molldrem JJ, Lee PP, Kant S, Wieder E, Jiang W, Lu S, Wang C, Davis MM: Chronic myelogenous leukemia shapes host immunity by selective deletion of high-avidity leukemia-specific T cells. J Clin Invest. 2003, 111: 639-647.
Klebanoff CA, Gattinoni L, Restifo NP: Sorting through subsets: which T-cell populations mediate highly effective adoptive immunotherapy?. J Immunother. 2012, 35: 651-660.
Morgan RA, Dudley ME, Wunderlich JR, Hughes MS, Yang JC, Sherry RM, Royal RE, Topalian SL, Kammula US, Restifo NP, Zheng Z, Nahvi A, de Vries CR, Rogers-Freezer LJ, Mavroukakis SA, Rosenberg SA: Cancer regression in patients after transfer of genetically engineered lymphocytes. Science. 2006, 314: 126-129.
Louis CU, Savoldo B, Dotti G, Pule M, Yvon E, Myers GD, Rossig C, Russell HV, Diouf O, Liu E, Liu H, Wu MF, Gee AP, Mei Z, Rooney CM, Heslop HE, Brenner MK: Antitumor activity and long-term fate of chimeric antigen receptor-positive T cells in patients with neuroblastoma. Blood. 2011, 118: 6050-6056.
Gattinoni L, Klebanoff CA, Restifo NP: Paths to stemness: building the ultimate antitumour T cell. Nat Rev Cancer. 2012, 12: 671-684.
Hinrichs CS, Borman ZA, Cassard L, Gattinoni L, Spolski R, Yu Z, Sanchez-Perez L, Muranski P, Kern SJ, Logun C, Palmer DC, Ji Y, Reger RN, Leonard WJ, Danner RL, Rosenberg SA, Restifo NP: Adoptively transferred effector cells derived from naive rather than central memory CD8+ T cells mediate superior antitumor immunity. Proc Natl Acad Sci U S A. 2009, 106: 17469-17474.
Olson JA, McDonald-Hyman C, Jameson SC, Hamilton SE: Effector-like CD8(+) T cells in the memory population mediate potent protective immunity. Immunity. 2013, 38: 1250-1260.
Kalos M, June CH: Adoptive T cell transfer for cancer immunotherapy in the era of synthetic biology. Immunity. 2013, 39: 49-60.
Ruella M, Kalos M: Adoptive immunotherapy for cancer. Immunol Rev. 2014, 257: 14-38.
Kuball J, Dossett ML, Wolfl M, Ho WY, Voss RH, Fowler C, Greenberg PD: Facilitating matched pairing and expression of TCR chains introduced into human T cells. Blood. 2007, 109: 2331-2338.
Xue SA, Gao L, Thomas S, Hart DP, Xue JZ, Gillmore R, Voss RH, Morris E, Stauss HJ: Development of a Wilms' tumor antigen-specific T-cell receptor for clinical trials: engineered patient's T cells can eliminate autologous leukemia blasts in NOD/SCID mice. Haematologica. 2010, 95: 126-134.
Stanislawski T, Voss RH, Lotz C, Sadovnikova E, Willemsen RA, Kuball J, Ruppert T, Bolhuis RL, Melief CJ, Huber C, Stauss HJ, Theobald M: Circumventing tolerance to a human MDM2-derived tumor antigen by TCR gene transfer. Nat Immunol. 2001, 2: 962-970.
Cohen CJ, Zheng Z, Bray R, Zhao Y, Sherman LA, Rosenberg SA, Morgan RA: Recognition of fresh human tumor by human peripheral blood lymphocytes transduced with a bicistronic retroviral vector encoding a murine anti-p53 TCR. J Immunol. 2005, 175: 5799-5808.
Johnson LA, Morgan RA, Dudley ME, Cassard L, Yang JC, Hughes MS, Kammula US, Royal RE, Sherry RM, Wunderlich JR, Lee CC, Restifo NP, Schwarz SL, Cogdill AP, Bishop RJ, Kim H, Brewer CC, Rudy SF, VanWaes C, Davis JL, Mathur A, Ripley RT, Nathan DA, Laurencot CM, Rosenberg SA: Gene therapy with human and mouse T-cell receptors mediates cancer regression and targets normal tissues expressing cognate antigen. Blood. 2009, 114: 535-546.
Friedman RS, Spies AG, Kalos M: Identification of naturally processed CD8 T cell epitopes from prostein, a prostate tissue-specific vaccine candidate. Eur J Immunol. 2004, 34: 1091-1101.
Robbins PF, Li YF, El-Gamil M, Zhao Y, Wargo JA, Zheng Z, Xu H, Morgan RA, Feldman SA, Johnson LA, Bennett AD, Dunn SM, Mahon TM, Jakobsen BK, Rosenberg SA: Single and dual amino acid substitutions in TCR CDRs can enhance antigen-specific T cell functions. J Immunol. 2008, 180: 6116-6131.
Cameron BJ, Gerry AB, Dukes J, Harper JV, Kannan V, Bianchi FC, Grand F, Brewer JE, Gupta M, Plesa G, Bossi G, Vuidepot A, Powlesland AS, Legg A, Adams KJ, Bennett AD, Pumphrey NJ, Williams DD, Binder-Scholl G, Kulikovskaya I, Levine BL, Riley JL, Varela-Rohena A, Stadtmauer EA, Rapoport AP, Linette GP, June CH, Hassan NJ, Kalos M, Jakobsen BK: Identification of a Titin-derived HLA-A1-presented peptide as a cross-reactive target for engineered MAGE A3-directed T cells. Sci Transl Med. 2013, 5: 197ra103-
Morgan RA, Chinnasamy N, Abate-Daga D, Gros A, Robbins PF, Zheng Z, Dudley ME, Feldman SA, Yang JC, Sherry RM, Phan GQ, Hughes MS, Kammula US, Miller AD, Hessman CJ, Stewart AA, Restifo NP, Quezado MM, Alimchandani M, Rosenberg AZ, Nath A, Wang T, Bielekova B, Wuest SC, Akula N, McMahon FJ, Wilde S, Mosetter B, Schendel DJ, Laurencot CM: Cancer regression and neurological toxicity following anti-MAGE-A3 TCR gene therapy. J Immunother. 2013, 36: 133-151.
van Loenen MM, de Boer R, Hagedoorn RS, van Egmond EH, Falkenburg JH, Heemskerk MH: Optimization of the HA-1-specific T-cell receptor for gene therapy of hematologic malignancies. Haematologica. 2011, 96: 477-481.
Reiser JB, Darnault C, Gregoire C, Mosser T, Mazza G, Kearney A, van der Merwe PA, Fontecilla-Camps JC, Housset D, Malissen B: CDR3 loop flexibility contributes to the degeneracy of TCR recognition. Nat Immunol. 2003, 4: 241-247.
Park JR, Digiusto DL, Slovak M, Wright C, Naranjo A, Wagner J, Meechoovet HB, Bautista C, Chang WC, Ostberg JR, Jensen MC: Adoptive transfer of chimeric antigen receptor re-directed cytolytic T lymphocyte clones in patients with neuroblastoma. Mol Ther. 2007, 15: 825-833.
Till BG, Jensen MC, Wang J, Chen EY, Wood BL, Greisman HA, Qian X, James SE, Raubitschek A, Forman SJ, Gopal AK, Pagel JM, Lindgren CG, Greenberg PD, Riddell SR, Press OW: Adoptive immunotherapy for indolent non-Hodgkin lymphoma and mantle cell lymphoma using genetically modified autologous CD20-specific T cells. Blood. 2008, 112: 2261-2271.
Kershaw MH, Westwood JA, Parker LL, Wang G, Eshhar Z, Mavroukakis SA, White DE, Wunderlich JR, Canevari S, Rogers-Freezer L, Chen CC, Yang JC, Rosenberg SA, Hwu P: A phase I study on adoptive immunotherapy using gene-modified T cells for ovarian cancer. Clin Cancer Res. 2006, 12: 6106-6115.
Lamers CH, Sleijfer S, van Steenbergen S, van Elzakker P, van Krimpen B, Groot C, Vulto A, den Bakker M, Oosterwijk E, Debets R, Gratama JW: Treatment of metastatic renal cell carcinoma with CAIX CAR-engineered T cells: clinical evaluation and management of on-target toxicity. Mol Ther. 2013, 21: 904-912.
Morgan RA, Yang JC, Kitano M, Dudley ME, Laurencot CM, Rosenberg SA: Case report of a serious adverse event following the administration of T cells transduced with a chimeric antigen receptor recognizing ERBB2. Mol Ther. 2010, 18: 843-851.
Dao T, Yan S, Veomett N, Pankov D, Zhou L, Korontsvit T, Scott A, Whitten J, Maslak P, Casey E, Tan T, Liu H, Zakhaleva V, Curcio M, Doubrovina E, O'Reilly RJ, Liu C, Scheinberg DA: Targeting the intracellular WT1 oncogene product with a therapeutic human antibody. Sci Transl Med. 2013, 5: 176ra133-
Sergeeva A, Alatrash G, He H, Ruisaard K, Lu S, Wygant J, McIntyre BW, Ma Q, Li D, St John L, Clise-Dwyer K, Molldrem JJ: An anti-PR1/HLA-A2 T-cell receptor-like antibody mediates complement-dependent cytotoxicity against acute myeloid leukemia progenitor cells. Blood. 2011, 117: 4262-4272.
Hinrichs CS, Rosenberg SA: Exploiting the curative potential of adoptive T-cell therapy for cancer. Immunol Rev. 2014, 257: 56-71.
Restifo NP, Dudley ME, Rosenberg SA: Adoptive immunotherapy for cancer: harnessing the T cell response. Nat Rev Immunol. 2012, 12: 269-281.
Barrett DM, Singh N, Porter DL, Grupp SA, June CH: Chimeric antigen receptor therapy for cancer. Annu Rev Med. 2014, 65: 333-347.
Kershaw MH, Wang G, Westwood JA, Pachynski RK, Tiffany HL, Marincola FM, Wang E, Young HA, Murphy PM, Hwu P: Redirecting migration of T cells to chemokine secreted from tumors by genetic modification with CXCR2. Hum Gene Ther. 2002, 13: 1971-1980.
Di Stasi A, De Angelis B, Rooney CM, Zhang L, Mahendravada A, Foster AE, Heslop HE, Brenner MK, Dotti G, Savoldo B: T lymphocytes coexpressing CCR4 and a chimeric antigen receptor targeting CD30 have improved homing and antitumor activity in a Hodgkin tumor model. Blood. 2009, 113: 6392-6402.
Eaton D, Gilham DE, O'Neill A, Hawkins RE: Retroviral transduction of human peripheral blood lymphocytes with Bcl-X(L) promotes in vitro lymphocyte survival in pro-apoptotic conditions. Gene Ther. 2002, 9: 527-535.
Charo J, Finkelstein SE, Grewal N, Restifo NP, Robbins PF, Rosenberg SA: Bcl-2 overexpression enhances tumor-specific T-cell survival. Cancer Res. 2005, 65: 2001-2008.
Bollard CM, Rossig C, Calonge MJ, Huls MH, Wagner HJ, Massague J, Brenner MK, Heslop HE, Rooney CM: Adapting a transforming growth factor beta-related tumor protection strategy to enhance antitumor immunity. Blood. 2002, 99: 3179-3187.
Straathof KC, Pule MA, Yotnda P, Dotti G, Vanin EF, Brenner MK, Heslop HE, Spencer DM, Rooney CM: An inducible caspase 9 safety switch for T-cell therapy. Blood. 2005, 105: 4247-4254.
Wang X, Chang WC, Wong CW, Colcher D, Sherman M, Ostberg JR, Forman SJ, Riddell SR, Jensen MC: A transgene-encoded cell surface polypeptide for selection, in vivo tracking, and ablation of engineered cells. Blood. 2011, 118: 1255-1263.
Pollack SM, O'Connor TP, Hashash J, Tabbara IA: Nonmyeloablative and reduced-intensity conditioning for allogeneic hematopoietic stem cell transplantation: a clinical review. Am J Clin Oncol. 2009, 32: 618-628.
Gooley TA, Chien JW, Pergam SA, Hingorani S, Sorror ML, Boeckh M, Martin PJ, Sandmaier BM, Marr KA, Appelbaum FR, Storb R, McDonald GB: Reduced mortality after allogeneic hematopoietic-cell transplantation. N Engl J Med. 2010, 363: 2091-2101.
Wrzesinski C, Paulos CM, Gattinoni L, Palmer DC, Kaiser A, Yu Z, Rosenberg SA, Restifo NP: Hematopoietic stem cells promote the expansion and function of adoptively transferred antitumor CD8 T cells. J Clin Invest. 2007, 117: 492-501.
Gattinoni L, Finkelstein SE, Klebanoff CA, Antony PA, Palmer DC, Spiess PJ, Hwang LN, Yu Z, Wrzesinski C, Heimann DM, Surh CD, Rosenberg SA, Restifo NP: Removal of homeostatic cytokine sinks by lymphodepletion enhances the efficacy of adoptively transferred tumor-specific CD8+ T cells. J Exp Med. 2005, 202: 907-912.
Klebanoff CA, Khong HT, Antony PA, Palmer DC, Restifo NP: Sinks, suppressors and antigen presenters: how lymphodepletion enhances T cell-mediated tumor immunotherapy. Trends Immunol. 2005, 26: 111-117.
Dudley ME, Wunderlich JR, Yang JC, Sherry RM, Topalian SL, Restifo NP, Royal RE, Kammula U, White DE, Mavroukakis SA, Rogers LJ, Gracia GJ, Jones SA, Mangiameli DP, Pelletier MM, Gea-Banacloche J, Robinson MR, Berman DM, Filie AC, Abati A, Rosenberg SA: Adoptive cell transfer therapy following non-myeloablative but lymphodepleting chemotherapy for the treatment of patients with refractory metastatic melanoma. J Clin Oncol. 2005, 23: 2346-2357.
Muranski P, Boni A, Wrzesinski C, Citrin DE, Rosenberg SA, Childs R, Restifo NP: Increased intensity lymphodepletion and adoptive immunotherapy–how far can we go?. Nat Clin Pract Oncol. 2006, 3: 668-681.
Kalos M, Levine BL, Porter DL, Katz S, Grupp SA, Bagg A, June CH: T cells with chimeric antigen receptors have potent antitumor effects and can establish memory in patients with advanced leukemia. Sci Transl Med. 2011, 3: 95ra73-
Brentjens RJ, Davila ML, Riviere I, Park J, Wang X, Cowell LG, Bartido S, Stefanski J, Taylor C, Olszewska M, Borquez-Ojeda O, Qu J, Wasielewska T, He Q, Bernal Y, Rijo IV, Hedvat C, Kobos R, Curran K, Steinherz P, Jurcic J, Rosenblat T, Maslak P, Frattini M, Sadelain M: CD19-targeted T cells rapidly induce molecular remissions in adults with chemotherapy-refractory acute lymphoblastic leukemia. Sci Transl Med. 2013, 5: 177ra138-
Torikai H, Reik A, Liu PQ, Zhou Y, Zhang L, Maiti S, Huls H, Miller JC, Kebriaei P, Rabinovitch B, Lee DA, Champlin RE, Bonini C, Naldini L, Rebar EJ, Gregory PD, Holmes MC, Cooper LJ: A foundation for universal T-cell based immunotherapy: T cells engineered to express a CD19-specific chimeric-antigen-receptor and eliminate expression of endogenous TCR. Blood. 2012, 119: 5697-5705.
Sullivan KM, Storb R, Buckner CD, Fefer A, Fisher L, Weiden PL, Witherspoon RP, Appelbaum FR, Banaji M, Hansen J, Martin P, Sanders JE, Singer J, Thomas ED: Graft-versus-host disease as adoptive immunotherapy in patients with advanced hematologic neoplasms. N Engl J Med. 1989, 320: 828-834.
Cruz CR, Micklethwaite KP, Savoldo B, Ramos CA, Lam S, Ku S, Diouf O, Liu E, Barrett AJ, Ito S, Shpall EJ, Krance RA, Kamble RT, Carrum G, Hosing CM, Gee AP, Mei Z, Grilley BJ, Heslop HE, Rooney CM, Brenner MK, Bollard CM, Dotti G: Infusion of donor-derived CD19-redirected virus-specific T cells for B-cell malignancies relapsed after allogeneic stem cell transplant: a phase 1 study. Blood. 2013, 122: 2965-2973.
Terakura S, Yamamoto TN, Gardner RA, Turtle CJ, Jensen MC, Riddell SR: Generation of CD19-chimeric antigen receptor modified CD8+ T cells derived from virus-specific central memory T cells. Blood. 2012, 119: 72-82.
Zhang Y, Joe G, Zhu J, Carroll R, Levine B, Hexner E, June C, Emerson SG: Dendritic cell-activated CD44hiCD8+ T cells are defective in mediating acute graft-versus-host disease but retain graft-versus-leukemia activity. Blood. 2004, 103: 3970-3978.
Dutt S, Tseng D, Ermann J, George TI, Liu YP, Davis CR, Fathman CG, Strober S: Naive and memory T cells induce different types of graft-versus-host disease. J Immunol. 2007, 179: 6547-6554.
Chen BJ, Deoliveira D, Cui X, Le NT, Son J, Whitesides JF, Chao NJ: Inability of memory T cells to induce graft-versus-host disease is a result of an abortive alloresponse. Blood. 2007, 109: 3115-3123.
Mackinnon S, Papadopoulos EB, Carabasi MH, Reich L, Collins NH, Boulad F, Castro-Malaspina H, Childs BH, Gillio AP, Kernan NA: Adoptive immunotherapy evaluating escalating doses of donor leukocytes for relapse of chronic myeloid leukemia after bone marrow transplantation: separation of graft-versus-leukemia responses from graft-versus-host disease. Blood. 1995, 86: 1261-1268.
Dazzi F, Szydlo RM, Craddock C, Cross NC, Kaeda J, Chase A, Olavarria E, van Rhee F, Kanfer E, Apperley JF, Goldman JM: Comparison of single-dose and escalating-dose regimens of donor lymphocyte infusion for relapse after allografting for chronic myeloid leukemia. Blood. 2000, 95: 67-71.
Grupp SA, Frey N, Aplenc R, Barrett D, Chew A, Kalos M, Levine B, Litchman M, Maude S, Rheingold SR, Shen A, Strait C, Teachey D, Wood PA, Porter DL, June C: T Cells Engineered with a Chimeric Antigen Receptor (CAR) Targeting CD19 (CTL019) Produce Significant In Vivo Proliferation, Complete Responses and Long-Term Persistence Without GvHD In Children and Adults With Relapsed, Refractory ALL. Oral Pres Am Soc Hematol. 2013, 122: 67-
Kochenderfer JN, Dudley ME, Carpenter RO, Kassim SH, Rose JJ, Telford WG, Hakim FT, Halverson DC, Fowler DH, Hardy NM, Mato AR, Hickstein DD, Gea-Banacloche JC, Pavletic SZ, Sportes C, Maric I, Feldman SA, Hansen BG, Wilder JS, Blacklock-Schuver B, Jena B, Bishop MR, Gress RE, Rosenberg SA: Donor-derived CD19-targeted T cells cause regression of malignancy persisting after allogeneic hematopoietic stem cell transplantation. Blood. 2013, 122: 4129-4139.
De Angelis B, Dotti G, Quintarelli C, Huye LE, Zhang L, Zhang M, Pane F, Heslop HE, Brenner MK, Rooney CM, Savoldo B: Generation of Epstein-Barr virus-specific cytotoxic T lymphocytes resistant to the immunosuppressive drug tacrolimus (FK506). Blood. 2009, 114: 4784-4791.
Brewin J, Mancao C, Straathof K, Karlsson H, Samarasinghe S, Amrolia PJ, Pule M: Generation of EBV-specific cytotoxic T cells that are resistant to calcineurin inhibitors for the treatment of posttransplantation lymphoproliferative disease. Blood. 2009, 114: 4792-4803.
Jonnalagadda M, Brown CE, Chang WC, Ostberg JR, Forman SJ, Jensen MC: Efficient selection of genetically modified human T cells using methotrexate-resistant human dihydrofolate reductase. Gene Ther. 2013, 20: 853-860.
Yee C: The use of endogenous T cells for adoptive transfer. Immunol Rev. 2014, 257: 250-263.
Baitsch L, Fuertes-Marraco SA, Legat A, Meyer C, Speiser DE: The three main stumbling blocks for anticancer T cells. Trends Immunol. 2012, 33: 364-372.
Jena B, Dotti G, Cooper LJ: Redirecting T-cell specificity by introducing a tumor-specific chimeric antigen receptor. Blood. 2010, 116: 1035-1044.
Uckun FM, Jaszcz W, Ambrus JL, Fauci AS, Gajl-Peczalska K, Song CW, Wick MR, Myers DE, Waddick K, Ledbetter JA: Detailed studies on expression and function of CD19 surface determinant by using B43 monoclonal antibody and the clinical potential of anti-CD19 immunotoxins. Blood. 1988, 71: 13-29.
Murphy K, Travers P, Walport M, Janeway C: Janeway's immunobiology. 2012, New York: Garland Science, 8
Cooper LJ, Topp MS, Serrano LM, Gonzalez S, Chang WC, Naranjo A, Wright C, Popplewell L, Raubitschek A, Forman SJ, Jensen MC: T-cell clones can be rendered specific for CD19: toward the selective augmentation of the graft-versus-B-lineage leukemia effect. Blood. 2003, 101: 1637-1644.
Brentjens RJ, Latouche JB, Santos E, Marti F, Gong MC, Lyddane C, King PD, Larson S, Weiss M, Riviere I, Sadelain M: Eradication of systemic B-cell tumors by genetically targeted human T lymphocytes co-stimulated by CD80 and interleukin-15. Nat Med. 2003, 9: 279-286.
Kochenderfer JN, Feldman SA, Zhao Y, Xu H, Black MA, Morgan RA, Wilson WH, Rosenberg SA: Construction and preclinical evaluation of an anti-CD19 chimeric antigen receptor. J Immunother. 2009, 32: 689-702.
Imai C, Mihara K, Andreansky M, Nicholson IC, Pui CH, Geiger TL, Campana D: Chimeric receptors with 4-1BB signaling capacity provoke potent cytotoxicity against acute lymphoblastic leukemia. Leukemia. 2004, 18: 676-684.
Brentjens RJ, Santos E, Nikhamin Y, Yeh R, Matsushita M, La Perle K, Quintas-Cardama A, Larson SM, Sadelain M: Genetically targeted T cells eradicate systemic acute lymphoblastic leukemia xenografts. Clin Cancer Res. 2007, 13: 5426-5435.
Cheadle EJ, Hawkins RE, Batha H, O'Neill AL, Dovedi SJ, Gilham DE: Natural expression of the CD19 antigen impacts the long-term engraftment but not antitumor activity of CD19-specific engineered T cells. J Immunol. 2010, 184: 1885-1896.
Kochenderfer JN, Yu Z, Frasheri D, Restifo NP, Rosenberg SA: Adoptive transfer of syngeneic T cells transduced with a chimeric antigen receptor that recognizes murine CD19 can eradicate lymphoma and normal B cells. Blood. 2010, 116: 3875-3886.
Milone MC, Fish JD, Carpenito C, Carroll RG, Binder GK, Teachey D, Samanta M, Lakhal M, Gloss B, Danet-Desnoyers G, Campana D, Riley JL, Grupp SA, June CH: Chimeric receptors containing CD137 signal transduction domains mediate enhanced survival of T cells and increased antileukemic efficacy in vivo. Mol Ther. 2009, 17: 1453-1464.
Carpenito C, Milone MC, Hassan R, Simonet JC, Lakhal M, Suhoski MM, Varela-Rohena A, Haines KM, Heitjan DF, Albelda SM, Carroll RG, Riley JL, Pastan I, June CH: Control of large, established tumor xenografts with genetically retargeted human T cells containing CD28 and CD137 domains. Proc Natl Acad Sci U S A. 2009, 106: 3360-3365.
Davila ML, Kloss CC, Gunset G, Sadelain M: CD19 CAR-targeted T cells induce long-term remission and B Cell Aplasia in an immunocompetent mouse model of B cell acute lymphoblastic leukemia. PLoS One. 2013, 8: e61338-
Kochenderfer JN, Wilson WH, Janik JE, Dudley ME, Stetler-Stevenson M, Feldman SA, Maric I, Raffeld M, Nathan DA, Lanier BJ, Morgan RA, Rosenberg SA: Eradication of B-lineage cells and regression of lymphoma in a patient treated with autologous T cells genetically engineered to recognize CD19. Blood. 2010, 116: 4099-4102.
Kochenderfer JN, Dudley ME, Feldman SA, Wilson WH, Spaner DE, Maric I, Stetler-Stevenson M, Phan GQ, Hughes MS, Sherry RM, Yang JC, Kammula US, Devillier L, Carpenter R, Nathan DA, Morgan RA, Laurencot C, Rosenberg SA: B-cell depletion and remissions of malignancy along with cytokine-associated toxicity in a clinical trial of anti-CD19 chimeric-antigen-receptor-transduced T cells. Blood. 2012, 119: 2709-2720.
Porter DL, Kalos M, Frey N, Grupp SA, Loren A, Jemison C, Gilmore J, McConville H, Capobianchi J, Lledo L, Chew A, Zheng Z, Levine B, June C: Chimeric antigen receptor modified T cells directed against CD19 (CTL019 cells) have long-term persistence and induce durable responses in relapsed, refractory CLL. Poster Pres Am Soc Hematol. 2013, 122: 4162-
Cardoso AA, Schultze JL, Boussiotis VA, Freeman GJ, Seamon MJ, Laszlo S, Billet A, Sallan SE, Gribben JG, Nadler LM: Pre-B acute lymphoblastic leukemia cells may induce T-cell anergy to alloantigen. Blood. 1996, 88: 41-48.
Kebelmann-Betzing C, Korner G, Badiali L, Buchwald D, Moricke A, Korte A, Kochling J, Wu S, Kappelmeier D, Oettel K, Henze G, Seeger K: Characterization of cytokine, growth factor receptor, costimulatory and adhesion molecule expression patterns of bone marrow blasts in relapsed childhood B cell precursor all. Cytokine. 2001, 13: 39-50.
Davila ML, Riviere I, Wang X, Bartido S, Park J, Curran K, Chung SS, Stefanski J, Borquez-Ojeda O, Olszewska M, Qu J, Wasielewska T, He Q, Fink M, Shinglot H, Youssif M, Satter M, Wang Y, Hosey J, Quintanilla H, Halton E, Bernal Y, Bouhassira DC, Arcila ME, Gonen M, Roboz GJ, Maslak P, Douer D, Frattini MG, Giralt S: Efficacy and Toxicity Management of 19-28z CAR T Cell Therapy in B Cell Acute Lymphoblastic Leukemia. Science translational medicine. 2014, 6: 224ra225-
Frey NV, Porter DL: Graft-versus-host disease after donor leukocyte infusions: presentation and management. Best Pract Res Clin Haematol. 2008, 21: 205-222.
Hosen N, Sonoda Y, Oji Y, Kimura T, Minamiguchi H, Tamaki H, Kawakami M, Asada M, Kanato K, Motomura M, Murakami M, Fujioka T, Masuda T, Kim EH, Tsuboi A, Oka Y, Soma T, Ogawa H, Sugiyama H: Very low frequencies of human normal CD34+ haematopoietic progenitor cells express the Wilms' tumour gene WT1 at levels similar to those in leukaemia cells. Br J Haematol. 2002, 116: 409-420.
Scharnhorst V, van der Eb AJ, Jochemsen AG: WT1 proteins: functions in growth and differentiation. Gene. 2001, 273: 141-161.
Yang L, Han Y, Suarez Saiz F, Minden MD: A tumor suppressor and oncogene: the WT1 story. Leukemia. 2007, 21: 868-876.
Miwa H, Beran M, Saunders GF: Expression of the Wilms' tumor gene (WT1) in human leukemias. Leukemia. 1992, 6: 405-409.
Miyoshi Y, Ando A, Egawa C, Taguchi T, Tamaki Y, Tamaki H, Sugiyama H, Noguchi S: High expression of Wilms' tumor suppressor gene predicts poor prognosis in breast cancer patients. Clin Cancer Res. 2002, 8: 1167-1171.
Dupont J, Wang X, Marshall DS, Leitao M, Hedvat CV, Hummer A, Thaler H, O'Reilly RJ, Soslow RA: Wilms Tumor Gene (WT1) and p53 expression in endometrial carcinomas: a study of 130 cases using a tissue microarray. Gynecol Oncol. 2004, 94: 449-455.
Oji Y, Miyoshi S, Maeda H, Hayashi S, Tamaki H, Nakatsuka S, Yao M, Takahashi E, Nakano Y, Hirabayashi H, Shintani Y, Oka Y, Tsuboi A, Hosen N, Asada M, Fujioka T, Murakami M, Kanato K, Motomura M, Kim EH, Kawakami M, Ikegame K, Ogawa H, Aozasa K, Kawase I, Sugiyama H: Overexpression of the Wilms' tumor gene WT1 in de novo lung cancers. Int J Cancer. 2002, 100: 297-303.
Campbell CE, Kuriyan NP, Rackley RR, Caulfield MJ, Tubbs R, Finke J, Williams BR: Constitutive expression of the Wilms tumor suppressor gene (WT1) in renal cell carcinoma. Int J Cancer. 1998, 78: 182-188.
Bergmann L, Miething C, Maurer U, Brieger J, Karakas T, Weidmann E, Hoelzer D: High levels of Wilms' tumor gene (wt1) mRNA in acute myeloid leukemias are associated with a worse long-term outcome. Blood. 1997, 90: 1217-1225.
Ostergaard M, Olesen LH, Hasle H, Kjeldsen E, Hokland P: WT1 gene expression: an excellent tool for monitoring minimal residual disease in 70% of acute myeloid leukaemia patients - results from a single-centre study. Br J Haematol. 2004, 125: 590-600.
Ogawa H, Tamaki H, Ikegame K, Soma T, Kawakami M, Tsuboi A, Kim EH, Hosen N, Murakami M, Fujioka T, Masuda T, Taniguchi Y, Nishida S, Oji Y, Oka Y, Sugiyama H: The usefulness of monitoring WT1 gene transcripts for the prediction and management of relapse following allogeneic stem cell transplantation in acute type leukemia. Blood. 2003, 101: 1698-1704.
Hamalainen MM, Kairisto V, Juvonen V, Johansson J, Auren J, Kohonen K, Remes K, Salmi TT, Helenius H, Pelliniemi TT: Wilms tumour gene 1 overexpression in bone marrow as a marker for minimal residual disease in acute myeloid leukaemia. Eur J Haematol. 2008, 80: 201-207.
Yamagami T, Sugiyama H, Inoue K, Ogawa H, Tatekawa T, Hirata M, Kudoh T, Akiyama T, Murakami A, Maekawa T: Growth inhibition of human leukemic cells by WT1 (Wilms tumor gene) antisense oligodeoxynucleotides: implications for the involvement of WT1 in leukemogenesis. Blood. 1996, 87: 2878-2884.
O'Reilly RJ, Dao T, Koehne G, Scheinberg D, Doubrovina E: Adoptive transfer of unselected or leukemia-reactive T-cells in the treatment of relapse following allogeneic hematopoietic cell transplantation. Semin Immunol. 2010, 22: 162-172.
May RJ, Dao T, Pinilla-Ibarz J, Korontsvit T, Zakhaleva V, Zhang RH, Maslak P, Scheinberg DA: Peptide epitopes from the Wilms' tumor 1 oncoprotein stimulate CD4+ and CD8+ T cells that recognize and kill human malignant mesothelioma tumor cells. Clin Cancer Res. 2007, 13: 4547-4555.
Oka Y, Elisseeva OA, Tsuboi A, Ogawa H, Tamaki H, Li H, Oji Y, Kim EH, Soma T, Asada M, Ueda K, Maruya E, Saji H, Kishimoto T, Udaka K, Sugiyama H: Human cytotoxic T-lymphocyte responses specific for peptides of the wild-type Wilms’ tumor gene (WT1) product. Immunogenetics. 2000, 51: 99-107.
Weber G, Karbach J, Kuci S, Kreyenberg H, Willasch A, Koscielniak E, Tonn T, Klingebiel T, Wels WS, Jager E, Bader P: WT1 peptide-specific T cells generated from peripheral blood of healthy donors: possible implications for adoptive immunotherapy after allogeneic stem cell transplantation. Leukemia. 2009, 23: 1634-1642.
Ohminami H, Yasukawa M, Fujita S: HLA class I-restricted lysis of leukemia cells by a CD8(+) cytotoxic T-lymphocyte clone specific for WT1 peptide. Blood. 2000, 95: 286-293.
Doubrovina ES, Doubrovin MM, Lee S, Shieh JH, Heller G, Pamer E, O'Reilly RJ: In vitro stimulation with WT1 peptide-loaded Epstein-Barr virus-positive B cells elicits high frequencies of WT1 peptide-specific T cells with in vitro and in vivo tumoricidal activity. Clin Cancer Res. 2004, 10: 7207-7219.
Scheibenbogen C, Letsch A, Thiel E, Schmittel A, Mailaender V, Baerwolf S, Nagorsen D, Keilholz U: CD8 T-cell responses to Wilms tumor gene product WT1 and proteinase 3 in patients with acute myeloid leukemia. Blood. 2002, 100: 2132-2137.
Rezvani K, Brenchley JM, Price DA, Kilical Y, Gostick E, Sewell AK, Li J, Mielke S, Douek DC, Barrett AJ: T-cell responses directed against multiple HLA-A*0201-restricted epitopes derived from Wilms' tumor 1 protein in patients with leukemia and healthy donors: identification, quantification, and characterization. Clin Cancer Res. 2005, 11: 8799-8807.
Gao L, Bellantuono I, Elsasser A, Marley SB, Gordon MY, Goldman JM, Stauss HJ: Selective elimination of leukemic CD34(+) progenitor cells by cytotoxic T lymphocytes specific for WT1. Blood. 2000, 95: 2198-2203.
Doubrovina E, Carpenter T, Pankov D, Selvakumar A, Hasan A, O'Reilly RJ: Mapping of novel peptides of WT-1 and presenting HLA alleles that induce epitope-specific HLA-restricted T cells with cytotoxic activity against WT-1(+) leukemias. Blood. 2012, 120: 1633-1646.
Kim YS, Yuan M, Itzkowitz SH, Sun QB, Kaizu T, Palekar A, Trump BF, Hakomori S: Expression of LeY and extended LeY blood group-related antigens in human malignant, premalignant, and nonmalignant colonic tissues. Cancer Res. 1986, 46: 5985-5992.
Kobayashi K, Sakamoto J, Kito T, Yamamura Y, Koshikawa T, Fujita M, Watanabe T, Nakazato H: Lewis blood group-related antigen expression in normal gastric epithelium, intestinal metaplasia, gastric adenoma, and gastric carcinoma. Am J Gastroenterol. 1993, 88: 919-924.
Dettke M, Loibner H: Different types of FCgamma-receptors are involved in anti-Lewis Y antibody induced effector functions in vitro. Br J Cancer. 2000, 82: 441-445.
Westwood JA, Smyth MJ, Teng MW, Moeller M, Trapani JA, Scott AM, Smyth FE, Cartwright GA, Power BE, Honemann D, Prince HM, Darcy PK, Kershaw MH: Adoptive transfer of T cells modified with a humanized chimeric receptor gene inhibits growth of Lewis-Y-expressing tumors in mice. Proc Natl Acad Sci U S A. 2005, 102: 19051-19056.
Sakamoto J, Furukawa K, Cordon-Cardo C, Yin BW, Rettig WJ, Oettgen HF, Old LJ, Lloyd KO: Expression of Lewisa, Lewisb, X, and Y blood group antigens in human colonic tumors and normal tissue and in human tumor-derived cell lines. Cancer Res. 1986, 46: 1553-1561.
Peinert S, Prince HM, Guru PM, Kershaw MH, Smyth MJ, Trapani JA, Gambell P, Harrison S, Scott AM, Smyth FE, Darcy PK, Tainton K, Neeson P, Ritchie DS, Honemann D: Gene-modified T cells as immunotherapy for multiple myeloma and acute myeloid leukemia expressing the Lewis Y antigen. Gene Ther. 2010, 17: 678-686.
Miyake M, Taki T, Hitomi S, Hakomori S: Correlation of expression of H/Le(y)/Le(b) antigens with survival in patients with carcinoma of the lung. N Engl J Med. 1992, 327: 14-18.
Kitamura K, Stockert E, Garin-Chesa P, Welt S, Lloyd KO, Armour KL, Wallace TP, Harris WJ, Carr FJ, Old LJ: Specificity analysis of blood group Lewis-y (Le(y)) antibodies generatedagainst synthetic and natural Le(y) determinants. Proc Natl Acad Sci U S A. 1994, 91: 12957-12961.
Scott AM, Tebbutt N, Lee FT, Cavicchiolo T, Liu Z, Gill S, Poon AM, Hopkins W, Smyth FE, Murone C, MacGregor D, Papenfuss AT, Chappell B, Saunder TH, Brechbiel MW, Davis ID, Murphy R, Chong G, Hoffman EW, Old LJ: A phase I biodistribution and pharmacokinetic trial of humanized monoclonal antibody Hu3s193 in patients with advanced epithelial cancers that express the Lewis-Y antigen. Clin Cancer Res. 2007, 13: 3286-3292.
Saleh MN, Sugarman S, Murray J, Ostroff JB, Healey D, Jones D, Daniel CR, LeBherz D, Brewer H, Onetto N, LoBuglio AF: Phase I trial of the anti-Lewis Y drug immunoconjugate BR96-doxorubicin in patients with lewis Y-expressing epithelial tumors. J Clin Oncol. 2000, 18: 2282-2292.
Herbertson RA, Tebbutt NC, Lee FT, MacFarlane DJ, Chappell B, Micallef N, Lee ST, Saunder T, Hopkins W, Smyth FE, Wyld DK, Bellen J, Sonnichsen DS, Brechbiel MW, Murone C, Scott AM: Phase I biodistribution and pharmacokinetic study of Lewis Y-targeting immunoconjugate CMD-193 in patients with advanced epithelial cancers. Clin Cancer Res. 2009, 15: 6709-6715.
Vera J, Savoldo B, Vigouroux S, Biagi E, Pule M, Rossig C, Wu J, Heslop HE, Rooney CM, Brenner MK, Dotti G: T lymphocytes redirected against the kappa light chain of human immunoglobulin efficiently kill mature B lymphocyte-derived malignant cells. Blood. 2006, 108: 3890-3897.
Pricop L, Hatakeyama A, Isobe H, Bona C: Analysis of lambda repertoire in kappa-deficient mice. Clin Immunol Immunopathol. 1995, 76: S179-S187.
Zegers BJ, Maertzdorf WJ, Van Loghem E, Mul NA, Stoop JW, Van Der Laag J, Vossen JJ, Ballieux RE: Kappa-chain deficiency. An immunoglobulin disorder. N Engl J Med. 1976, 294: 1026-1030.
Pule MA, Straathof KC, Dotti G, Heslop HE, Rooney CM, Brenner MK: A chimeric T cell antigen receptor that augments cytokine release and supports clonal expansion of primary human T cells. Mol Ther. 2005, 12: 933-941.
Ocqueteau M, San Miguel JF, Gonzalez M, Almeida J, Orfao A: Do myelomatous plasma cells really express surface immunoglobulins?. Haematologica. 1996, 81: 460-463.
Matutes E, Owusu-Ankomah K, Morilla R, Garcia Marco J, Houlihan A, Que TH, Catovsky D: The immunological profile of B-cell disorders and proposal of a scoring system for the diagnosis of CLL. Leukemia. 1994, 8: 1640-1645.
Matsushita H, Nakamura N, Tanaka Y, Ohgiya D, Tanaka Y, Damdinsuren A, Asai S, Yabe M, Kawada H, Ogawa Y, Ando K, Miyachi H: Clinical and pathological features of B-cell non-Hodgkin lymphomas lacking the surface expression of immunoglobulin light chains. Clin Chem Lab Med. 2012, 50: 1665-1670.
Warren EH, Zhang XC, Li S, Fan W, Storer BE, Chien JW, Boeckh MJ, Zhao LP, Martin PJ, Hansen JA: Effect of MHC and non-MHC donor/recipient genetic disparity on the outcome of allogeneic HCT. Blood. 2012, 120: 2796-2806.
Fontaine P, Roy-Proulx G, Knafo L, Baron C, Roy DC, Perreault C: Adoptive transfer of minor histocompatibility antigen-specific T lymphocytes eradicates leukemia cells without causing graft-versus-host disease. Nat Med. 2001, 7: 789-794.
Warren EH, Fujii N, Akatsuka Y, Chaney CN, Mito JK, Loeb KR, Gooley TA, Brown ML, Koo KK, Rosinski KV, Ogawa S, Matsubara A, Appelbaum FR, Riddell SR: Therapy of relapsed leukemia after allogeneic hematopoietic cell transplantation with T cells specific for minor histocompatibility antigens. Blood. 2010, 115: 3869-3878.
Nilsson K, Klein G, Henle W, Henle G: The establishment of lymphoblastoid lines from adult and fetal human lymphoid tissue and its dependence on EBV. Int J Cancer. 1971, 8: 443-450.
Fisher B, Packard BS, Read EJ, Carrasquillo JA, Carter CS, Topalian SL, Yang JC, Yolles P, Larson SM, Rosenberg SA: Tumor localization of adoptively transferred indium-111 labeled tumor infiltrating lymphocytes in patients with metastatic melanoma. J Clin Oncol. 1989, 7: 250-261.
Kamei M, Nannya Y, Torikai H, Kawase T, Taura K, Inamoto Y, Takahashi T, Yazaki M, Morishima S, Tsujimura K, Miyamura K, Ito T, Togari H, Riddell SR, Kodera Y, Morishima Y, Takahashi T, Kuzushima K, Ogawa S, Akatsuka Y: HapMap scanning of novel human minor histocompatibility antigens. Blood. 2009, 113: 5041-5048.
den Haan JM, Meadows LM, Wang W, Pool J, Blokland E, Bishop TL, Reinhardus C, Shabanowitz J, Offringa R, Hunt DF, Engelhard VH, Goulmy E: The minor histocompatibility antigen HA-1: a diallelic gene with a single amino acid polymorphism. Science. 1998, 279: 1054-1057.
Bocchia M, Gentili S, Abruzzese E, Fanelli A, Iuliano F, Tabilio A, Amabile M, Forconi F, Gozzetti A, Raspadori D, Amadori S, Lauria F: Effect of a p210 multipeptide vaccine associated with imatinib or interferon in patients with chronic myeloid leukaemia and persistent residual disease: a multicentre observational trial. Lancet. 2005, 365: 657-662.
Falkenburg JH, Wafelman AR, Joosten P, Smit WM, van Bergen CA, Bongaerts R, Lurvink E, van der Hoorn M, Kluck P, Landegent JE, Kluin-Nelemans HC, Fibbe WE, Willemze R: Complete remission of accelerated phase chronic myeloid leukemia by treatment with leukemia-reactive cytotoxic T lymphocytes. Blood. 1999, 94: 1201-1208.
Dubrovsky L, Pankov D, Brea EJ, Dao T, Scott A, Yan S, O’Reilly RJ, Liu C, Scheinberg DA: A TCR-mimic antibody to WT1 bypasses tyrosine kinase inhibitor resistance in human BCR-ABL+ leukemias. Blood. 2014, 123: 3296-3304.
Giordano Attianese GM, Marin V, Hoyos V, Savoldo B, Pizzitola I, Tettamanti S, Agostoni V, Parma M, Ponzoni M, Bertilaccio MT, Ghia P, Biondi A, Dotti G, Biagi E: In vitro and in vivo model of a novel immunotherapy approach for chronic lymphocytic leukemia by anti-CD23 chimeric antigen receptor. Blood. 2011, 117: 4736-4745.
Mardiros A, Dos Santos C, McDonald T, Brown CE, Wang X, Budde LE, Hoffman L, Aguilar B, Chang WC, Bretzlaff W, Chang B, Jonnalagadda M, Starr R, Ostberg JR, Jensen MC, Bhatia R, Forman SJ: T cells expressing CD123-specific chimeric antigen receptors exhibit specific cytolytic effector functions and antitumor effects against human acute myeloid leukemia. Blood. 2013, 122: 3138-3148.
Nagai K, Ochi T, Fujiwara H, An J, Shirakata T, Mineno J, Kuzushima K, Shiku H, Melenhorst JJ, Gostick E, Price DA, Ishii E, Yasukawa M: Aurora kinase A-specific T-cell receptor gene transfer redirects T lymphocytes to display effective antileukemia reactivity. Blood. 2012, 119: 368-376.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
HG wrote the manuscript with assistance from AM. EM and GA outlined and revised the manuscript. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Garber, H.R., Mirza, A., Mittendorf, E.A. et al. Adoptive T-cell therapy for Leukemia. Mol and Cell Ther 2, 25 (2014). https://doi.org/10.1186/2052-8426-2-25
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/2052-8426-2-25