
Abstract
Cryptosporidiosis, a protozoal disease which causes significant morbidity in humans, is one of the chief causes of diarrhoea in neonatal ruminants. although the parasite poses a significant threat to public health and animal health in Ireland, its epidemiology on the island is only poorly understood. Environmental studies have shown the waterborne parasite to be widespread in some untreated waterbodies around Ireland. The island's hydrogeological situation, combined with high stocking rates of livestock and the absence of filtration from regular water treatment, render it vulnerable to large-scale outbreaks. This review discusses the parasite in the Irish context and underlines the need for a reference facility to provide active surveillance on the island.
Similar content being viewed by others

Pathology and prevalence of cryptosporidiosis in domestic animals
Cryptosporidiosis in ruminants is said to be on the increase [6] and it is now considered a major disease and one of the main causes of morbidity and mortality in newborn livestock [5, 45, 15]. C. parvum is the predominant parasite in cattle, sheep and goats, while C. andersoni and C. bovis also occur in cattle (one C. bovis infection has also been reported from a two-week-old lamb: Fayer et al., [20]). The latter two are not infective to humans and, apparently, are less pathogenic to cattle than C. parvum [55, 65]. Cryptosporidiosis in calves, lambs and goat kids is characterised by diarrhoea, anorexia, abdominal pain, apathy and depression. It has been suggested that destruction of the intestinal epithelia by the parasite may also increase susceptibility to other enteric pathogens [5, 15, 33] but, so far, synergistic effects have not been reported [2, 45, 46]. Severe cases are characterised by excessive loss of fluid and electrolytes with subsequent metabolic acidosis, which may prove fatal in some circumstances [15, 13]. Generally, the disease lasts between three and 12 days with protracted oocyst shedding well beyond recovery [4]. There are no reports of clinical cryptosporidiosis in adult cattle, sheep or goats, although they may shed oocysts asymptomatically [35, 4, 15, 9, 59].
The parasite is common in ruminants throughout Europe but reported prevalence rates vary widely. Among calves up to 100% of a herd may be affected, especially if the animals are housed communally [4, 15, 32, 59]. In Ireland, two studies have been carried out in commercial beef abattoirs: they reported prevalences between 5.5% (adult cattle only: de Waele et al., in press) and 7.3% (including both adults and calves: Moriarty et al., [44]) with a marked spring peak. In both studies, most infections were due to the non-zoonotic species C. andersoni. Among lambs and goat kids, particularly high prevalences of 40% to 70% have been reported from Spain [45, 4, 6, 9]. In the UK, infection rates appear to be somewhat lower: Sturdee et al. [59] reported an average incidence of 23%. Information is not available about the prevalence of cryptosporidiosis in sheep or goats in Northern Ireland or in the Republic of Ireland. A study of the prevalence of cryptosporidiosis in a commercial deer herd reported widespread asymptomatic infections in both calves and adult deer hinds associated with low levels of oocyst shedding all year around [57]. Among all ruminants, incidence rates usually peak during calving and lambing seasons. This is thought to be due to the presence of large groups of highly susceptible neonates in close proximity to each other and to dams, which may experience a periparturient rise in oocyst shedding [4, 57, 44].
The importance of cryptosporidiosis in horses in unclear. Until recently, clinical disease was thought to be restricted to immunodeficient foals, in which the infection can spread throughout the intestine and bile duct and become life-threatening [1]. Later studies demonstrated cryptosporidiosis in immunocompetent foals and adult horses. In foals, the disease may be asymptomatic [2] or it may cause mild to severe diarrhoea, in which case it may become fatal [25, 10, 11]. There is a single report in the literature of Cryptospordium-associated diarrhoea in a mature horse [38]. Generally, infected mature horses shed small numbers of oocysts without developing clinical signs [40]. With the exception of a novel horse genotype identified in a single Prezwalski's wild horse [52], the only Cryptosporidium species identified in horses is C. parvum. In the UK, reported prevalence rates in foals and horses range between 3% and 20% [46, 59, 10]. A study of 21 normal and 285 diarrhoeic foals from British and Irish stud farms reported prevalences of 27% and 29%, respectively [2].
Three species infect pigs: C. suis (formerly pig genotype I), pig genotype II and, occasionally, C. parvum [53, 54]. Experimental Cryptosporidium infections in piglets may cause moderate illness with anorexia, vomiting and diarrhoea [62, 15]. In contrast, though widespread, natural infections appear to be largely asymptomatic in both piglets and adult pigs [62, 4, 15].
Clinical cryptosporidiosis in dogs and cats (caused by Cryptosporidium canis and Cryptosporidium felis, respectively) has only been reported from animals that are immunosuppressed by concurrent viral infections such as canine distemper, parvoviral gastroenteritis, feline leukaemia or feline immunodeficiency [43, 16, 19]. Furthermore, it has been reported that dogs and cats only rarely act as asymptomatic carriers [4, 19, 12], while PCR screening has shown that many are chronically infected at levels that are too low to be detected microscopically (Professor Una M. Ryan, personal communication, March 2006).
In chickens and other domestic fowl, extra-intestinal infections are much more common than in mammals. The parasite infects the microvillous regions of the digestive tract, the respiratory tract, the bursa of Fabricius and the urinary tract. Mortality rates may be high [15]. It has been suggested that respiratory cryptosporidiosis is due to inhalation of oocysts associated with aerosolised faecal dust. This may be followed by intestinal infections as oocysts are coughed up and swallowed [61]. Respiratory infections are characterised by coughing, sneezing, dyspnea and rales [18]. Chickens with intestinal infections suffer diarrhoea and severe enteritis. Renal cryptosporidiosis is associated with pale and enlarged kidneys, while the ureters may become partially obstructed, resulting in visceral gout [61]. Most infections occur in chickens under 11 weeks of age [24, 18]. The chief avian species are Cryptosporidium baileyi, Cryptosporidium galli and Cryptosporidium meleagridis.
Diagnosis and detection
Most microbiological departments of larger hospitals now test for Cryptosporidium if requested by the clinician or if cryptosporidiodis is indicated by the clinical presentation or the age of the patient. In Northern Ireland, faecal samples from suspected animal cases are tested on request at the laboratories of the Department of Agriculture and Rural Development (Veterinary Sciences Division). In the Republic of Ireland, that service is available at the Regional Veterinary Laboratories, at the Veterinary Hospital, University College Dublin and at the Central Veterinary Research Laboratory, Abbotstown, Dublin. The majority of these laboratories use either modified Ziehl-Neelsen stain or phenol-auramine stain ([47, 63]: http://www.defra.gov.uk/animalh/diseases/vetsurveillance/pdf/nrm-002crypto.pdf), or a combination of both, to detect oocysts (safefood website: http://www.safefoodonline.com/safefood/login_extranet.asp; [36]).
In the UK, the legal limit for the presence of Cryptosporidium is one oocyst/10 litres drinking water (UK Drinking Water Regulations 1999, S.I. No 1527). However, numerous outbreaks have been reported at oocyst concentrations well below this threshold [50]. Current EU legislation does not set limits for Cryptosporidium oocysts in drinking water. Similarly, there are no guidelines for the presence of oocysts in food, even though the number of reported foodborne outbreaks is on the increase. To our knowledge there are currently three laboratories on the island that test environmental samples for the presence of Cryptosporidium oocysts: in Northern Ireland, the Water Service Northern Ireland, Altnagelvin, Derry and, in the Republic of Ireland, the Central Laboratory, Dublin City Council, Dublin 8, and City Analysts Ltd., Ringsend, Dublin 4. Detection of oocysts in water samples and viability testing involves immunomagnetic separation (IMS), immunofluorescence (IFA) and vital dye staining as recommended by the Drinking Water Inspectorate (Regulations 1999, SI No.1524. June 1999) and the EPA (USEPA Methods 1622 and 1623).
Genotyping to species level helped to identify the sources of contamination responsible for the three outbreaks in Northern Ireland during 2000 and 2001 [23] and the 2002 outbreak in Westmeath [31]. However, in the absence of a National Cryptosporidium Reference Laboratory, genotyping is not routinely carried out, although this information would be vital for a better understanding of the chief transmission routes of the parasite on this island.
Treatment
In most immunocompetent patients and young animals, the disease is self-limiting and resolves without chemical intervention. For the treatment of more severe cases, over 100 agents have been tested with varying degrees of success [28]. Currently, the only drug approved by the US Food and Drug Administration for treatment of cryptosporidiosis in children is the anti-protozoal agent nitrazoxanidine (Alinia) [3]. Although some studies reported obvious benefits to both immunocompetent and immunocompromised people [3, 58], other workers have questioned its usefulness to HIV-infected patients [66]. Another drug paromomycin, an aminocyclitol antibiotic isolated from Streptomyces, was previously reported to alleviate symptoms and reduce oocyst excretion in human infections. More recently, inconsistent results have raised questions concerning its efficacy against human cryptosporidiosis [27, 56, 66].
To date, no agent has been approved for the prevention or therapy of cryptosporidiosis in calves [30]. Though of questionable efficacy in humans, paromomycin was successfully used as a prophylaxis in dairy calves, where it reduced the duration and severity of diarrhoea [17]. Other studies have shown that the efficiency of paromomycin can be improved by combined use with protease inhibitors [28] or recombinant IL-12 [21]. The antiprotozoal drug halofuginone lactate (Halocur), a synthetic quinazolinone, can delay the establishment of infections in calves and reduce the severity of cryptosporidiosis. During treatment, oocyst excretion is reduced, contributing to decreased contamination of the environment [30]. However, low levels of oocyst shedding may recur following withdrawal of the drug [33, 32]. Unfortunately, both drugs have disadvantages that preclude their widespread use in food animals: both are relatively toxic and require exact doses. Paramomycin is very expensive. Decoquinate, which is highly effective against some other apicomplexans, was found by some to be beneficial in both infected calves and goat kids [49, 39]. Others reported little activity against Cryptosporidium in vitro, or in vivo in calves or suckling mice [34, 42]. The starch-derived excipient beta-cyclodextrin was shown to be highly effective as a prophylactic and therapeutic agent in neonatal lambs [6]. Promising results have also been achieved with a number of other drugs, such as lasalocid, nigericin (two ionophorous antibiotics) and alpha-cyclodextrin in vitro and in the murine model [7, 22, 8], but so far they have not been tried in ruminants.
Since there is no drug that achieves the complete removal of Cryptosporidium from an infected host, and no compound is clearly recognised, widely accepted and immediately available as a prophylactic or therapeutic agent, the preferred treatment in both humans and domestic animals is supportive treatment. Generally, this consists of replacement of fluid and electrolytes, nutritional support and anti-diarrhoeal drugs. Broad-spectrum antibiotics, gastric protectants and anti-ulcer medication may also be beneficial. In humans, the use of antiretroviral agents (HAART), which cause increased CD4+ T-lymphocyte counts in immunocompromised individuals, has dramatically improved recovery and survival rates [29, 3]. The introduction of protease inhibitors (PIs) in HAART has had additional benefits, as PIs appear to directly interfere with the parasite life cycle [28, 58, 66].
Immunity
There is abundant evidence in the literature that adult animals (such as cattle, sheep, poultry, mice) are not usually pathologically affected by cryptosporidiosis [24, 35, 4, 18, 15, 9, 59]. Even though they may become infected and shed oocysts, they show no clinical signs. It has been suggested that this may be due to innate resistance mechanisms, such as maturation of the gut microflora or of the intestinal epithelium, or other age-related changes, which occur in adult animals even if they have not previously been exposed to the pathogen [27]. On the other hand, since oocyst contamination is common in the environment of most calves, and calves are likely to be exposed repeatedly from birth, it is difficult to separate age-related innate resistance from immunity acquired during a previous infection. The only study that investigated innate immunity to cryptosporidiosis found that calves raised in isolation from C. parvum remained susceptible to challenge until at least three months of age [26]. On the other hand, numerous studies confirm that animals (including primates) are fully protected against clinical signs following re-infection although they may shed oocysts asymptomatically [14, 26, 41, 18, 61, 27].
In humans, separation of innate and acquired immunity to cryptosporidiosis is even more problematic and may depend on the species of Cryptosporidium or, indeed, the strain. Incidence data indicate that children are more severely affected, however, it has been argued that this bias may be due to a greater likelihood that parents seek medical attention for a child with diarrhoea and that stool samples are collected for laboratory analysis. Statistics from the largest cryptosporidiosis outbreak ever recorded (in 1993, in Milwaukee, Wisconsin, which affected approximately 403,000 people) showed that the group aged 30 to 39 years was most severely affected [37]. It was discovered later that this outbreak had been due to C. hominis [60]. Human infectivity studies carried out with seronegative volunteers found previous infections with C. parvum conferred only partial resistance to re-infection. Challenge with the same isolate one year after the first infection resulted in less severe symptomatic infections and lower levels of oocyst excretion [48]. Similarly, Xiao et al. [64] detected repeat infections (with homologous and heterologous genotypes of C. parvum, C. hominis and C. meleagridis) in HIV-negative children in Peru and concluded that acquired immunity against Cryptosporidium was only partial or short-lived. Innate and acquired immunity are primarily dependent on gamma-interferon and CD4 T-lymphocytes [29]. Serum antibodies, although commonly observed in recovering and immune animals [35], seem to be of minor importance [51].
Conclusion
Cryptosporidium causes serious recurrent disease in humans and is one of the major enteropathogens affecting neonatal ruminants. The Waterborne Cryptosporidiosis Subcommittee, set up by the Department of Health and Children in 2000, found that the pathogen posed a significant threat to both public health and animal health. Recognising the potential for large-scale waterborne outbreaks in Ireland, the body called for a National Cryptosporidium Reference Laboratory responsible for typing of isolates and provision of expert advice [50]. In 2004, a cross-border Cryptosporidium Research Network was set up to promote and facilitate interdisciplinary research and the transfer of information about cryptosporidiosis on the island of Ireland. In addition, facilities for genotyping Cryptosporidium to species and strain level has been set up in the Central Veterinary Laboratory and at University College Dublin. More such measures and collaborations between medical, veterinary and environmental scientists and health care professionals will be necessary to enhance our knowledge of cryptosporidiosis on the island and to avert or minimise future outbreaks.
Cryptosporidiumin Ireland: recent initiatives
In 2004, Professor Grace Mulcahy, School of Agriculture, Food Science and Veterinary Medicine, University College Dublin (UCD) set up the cross-border Cryptosporidium Research Network. Funded by 'safefood', the Food Safety Promotion Board, the network sets out to promote and facilitate interdisciplinary research and the transfer of information about cryptosporidiosis on the island of Ireland.
Genotyping of cattleisolates has been carried out under Dr Tom Murphy at the Central Veterinary Laboratory since 2002. Professors Grace Mulcahy and Seamus Fanning have set up a facility for genotyping Cryptosporidium to species and strain level at the UCD School of Agriculture, Food Science and Veterinary Medicine. Dr Nicholas Holden, School Of Agriculture, Food Science and Veterinary Medicine, UCD and Dr Tom Murphy, Central Veterinary Laboratory, are currently setting up a project which will use a microbial risk assessment model to identify catchments where potable water is at high risk of being contaminated.
Clarification
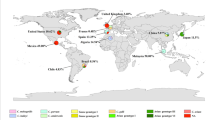
Part one of this scientific paper appeared in the previous edition of the Irish Veterinary Journal [59 (8) pp 442-447]. It has been noted that, within that article, the content of Figure 4 was not made immediately clear. Thus, for purposes of clarification, Figure 4 is repeated here, with highlighting (smaller box) of the relevant area.

(which was figure 4 in part one of this article, Irish Veterinary Journal [59 (8) pp442-447]) Identification of C. hominis (lanes 2, 3 and 5, 6) and C. parvum (lanes 4 and 7) by PCR-RFLP. Digestion with the endonuclease Sspl results in products of approx 500 and 250 bp in both spp. Digestion with the endonuclease Vspl renders products of approx 590 (C. hominis) and 610 bp (C. parvum). Lanes 1 and 8 are molecular weight markers.
Note
* This paper is the second part to "An Irish perspective on Cryptosporidium," published in the previous issue of the Irish Veterinary Journal [59 (9) pp 442-447)]
References
Bjorneby JM, Leach DR, Perryman LE: Persistent cryptosporidiosis in horses with severe combined immunodeficiency. Infection and Immunity. 1991, 59: 3823-3826.
Browning GF, Chalmers RM, Snodgrass DR, Batt RM, Hart CA, Ormarod SE, Leadon D, Stoneham SJ, Rossdale PD: The prevalence of enteric pathogens in diarrhoeic Thoroughbred foals in Britain and Ireland. Equine Veterinary Journal. 1991, 23: 405-409. 10.1111/j.2042-3306.1991.tb03751.x.
Carey CM, Lee H, Trevors JT: Biology, persistence and detection of Cryptosporidium parvum and Cryptosporidium hominis oocyst. Water Research. 2004, 38: 818-862. 10.1016/j.watres.2003.10.012.
Casemore DP, Wright SE, Coop RL: Cryptosporidiosis-human and animal epidemiology. Cryptosporidium and Cryptosporidiosis. Edited by: Fayer R. 1997, Boca Raton, Florida: CRC Press, 65-92.
Casey MJ: Cryptosporidium and bovine cryptosporidiosis: A review. Irish Veterinary Journal. 1991, 44: 2-7.
Castro-Hermida JA, Gonzalez-Losada Y, Freire-Santos F, Gonzalez-Warleta M, Mezo-Menendez M, Ares-Mazas ME: Efficacy of beta-cyclodextrin against experimental cryptosporidiosis in neonatal lambs. Journal of Parasitology. 2002, 88: 185-187. 10.1645/0022-3395(2002)088[0185:EOCAEC]2.0.CO;2.
Castro-Hermida JA, Freire-Santos F, Oteiza López AM, Vergara Castiblanco CA, Ares-Mazás ME: In vitro and in vivo efficacy of lasalocid for treatment of experimental cryptosporidiosis. Veterinary Parasitology. 2000, 90: 265-270. 10.1016/S0304-4017(00)00243-0.
Castro-Hermida JA, Ares-Mazas ME: In vitro and in vivo efficacy of alpha-cyclodextrin for treatment of experimental cryptosporidiosis. Veterinary Parasitology. 2003, 114: 237-245. 10.1016/S0304-4017(03)00156-0.
Causapé AC, Quílez J, Sánchez-Acedo C, del Cacho E, López-Bernad F: Prevalence and analysis of potential risk factors for Cryptosporidium parvum infection in lambs in Zaragoza (northeastern Spain). Veterinary Parasitology. 2002, 104: 287-298.
Chalmers RM, Thomas AL, Butler BA, Davies Morel CG: Identification of Cryptosporidium parvum genotype 2 in domestic horses. Veterinary Record. 2005, 156: 49-50.
Chalmers RM, Grinberg A: Significance of Cryptosporidium in horses. Veterinary Record. 2005, 156: 688-
Cirak VY, Bauer C: Comparison of conventional coproscopical methods and commercial coproantigen ELISA kits for the detection of Giardia and Cryptosporidium infections in dogs and cats. Berliner und Munchener Tierarztliche Wochenschrift (Berlin). 2004, 117: 410-413.
Constable PD: The treatment of the diarrheic calf: An update. Recent developments and perspectives in bovine medicine. 2002, 132-143. (Proceedings of XXII World Buiatrics Congress, Hanover, Germany)
Current WL, Snyder DB: Development of and serologic evaluation of acquired immunity to Cryptosporidium baileyi by broiler chickens. Poultry Science. 1988, 67: 720-729.
De Graaf DC, Vanopdenbosch E, Ortega-Mora LM, Abbassi H, Peeters V: A review of the importance of cryptosporidiosis in farm animals. International Journal for Parasitology. 1999, 29: 1269-1287. 10.1016/S0020-7519(99)00076-4.
Denholm KM, Haitjema H, Gwynne BJ, Morgan UM, Irwin PJ: Concurrent Cryptosporidium and parvovirus infections in a puppy. Australian Veterinary Journal. 2001, 79: 98-101. 10.1111/j.1751-0813.2001.tb10708.x.
Fayer R, Ellis W: Paromomycin is effective as prophylaxis for cryptosporidiosis in dairy calves. Journal of Parasitology. 1993, 79: 771-774. 10.2307/3283619.
Fayer R, Speer CA, Dubey JP: General biology of Cryptosporidium. Cryptosporidium and Cryptosporidiosis. Edited by: Fayer R. 1997, Boca Raton, Florida: CRC Press, 1-42.
Fayer R, Trout JM, Xiao L, Morgan UM, Lal AA, Dubey JP: Cryptosporidium canis n. sp. from domestic dogs. Journal of Parasitology. 2001, 87: 1415-1422. 10.1645/0022-3395(2001)087[1415:CCNSFD]2.0.CO;2.
Fayer R, Santin M, Xiao L: Cryptosporidium bovis n. sp. (Apicomplexa: Cryptosporidiidae) in cattle (Bos taurus). Journal of Parasitology. 2005, 91: 624-9. 10.1645/GE-3435.
Gamra MM, el-Hosseiny LM: Comparative study of the prophylactic and therapeutic effects of paromomycin, recombinant IL-12 alone or in combination against Cryptosporidium parvum infection in immunosuppressed mice. Journal of the Egyptian Society for Parasitology. 2003, 33: 109-122.
Giacometti A, Cirioni O, Del Prete MS, Barchiesi F, Scalise G: Short-term exposure to membrane-active antibiotics inhibits Cryptosporidium parvum infection in cell culture. Antimicrobial Agents and Chemotherapy. 2000, 44: 3473-3475. 10.1128/AAC.44.12.3473-3475.2000.
Glaberman S, Moore JE, Lowery CJ, Chalmers RM, Sulaiman I, Elwin K, Rooney PJ, Millar BC, Dooley JSG, Lal AA, Xiao L: Three drinking-water-associated cryptosporidiosis outbreaks, Northern Ireland. Emerging Infectious Diseases. 2002, 8: 631-633.
Goodwin MA, Brown J: Effect of Cryptosporidium baileyi on broilers infected at 26 days of age. Avian Diseases. 1990, 34: 458-462. 10.2307/1591436.
Grinberg A, Oliver L, Learmonth JJ, Leyland M, Roe W, Pomroy WE: Identification of Cryptosporidium parvum 'cattle' genotype from a severe outbreak of neonatal foal diarrhoea. Veterinary Record. 2003, 153: 628-631. 10.1136/vr.153.20.628.
Harp JA, Woodmansee DB, Moon HW: Resistance of calves to Cryptosporidium parvum: effects of age and previous exposure. Infection and Immunity. 1990, 58: 2237-2240.
Harp JA: Cryptosporidium and host resistance: historical perspective and some novel approaches. Animal Health Research Reviews. 2003, 4: 53-62. 10.1079/AHRR200352.
Hommer V, Eichholz J, Petry F: Effect of antiretroviral protease inhibitors alone, and in combination with paromomycin, on the excystation, invasion and in vitro development of Cryptosporidium parvum. Journal of Antimicrobial Chemotherapy. 2003, 52: 359-364. 10.1093/jac/dkg357.
Hunter PR, Nichols G: Epidemiology and clinical features of Cryptosporidium infection in immunocompromised patients. Clinical Microbiology Reviews. 2002, 15: 145-154. 10.1128/CMR.15.1.145-154.2002.
Jarvie BD, Trotz-Williams LA, D R, Leslie KE, Wallace MM, Todd CG, Sharpe PH, Peregrine AS: Effect of halofuginone lactate on the occurrence of Cryptosporidium parvum and growth of neonatal dairy calves. Journal of Dairy Science. 2005, 88: 1801-1806. 10.3168/jds.S0022-0302(05)72854-X.
Jennings P, Rhatigan A: Cryptosporidiosis outbreak in Ireland linked to public water supply. Eurosurveillance Weekly. 2002, 6: 1-4.
Joachim A, Krull T, Schwarzkopf J, Daugschies A: Prevalence and control of bovine cryptosporidiosis in German dairy herds. Veterinary Parasitology. 2003, 112: 277-288. 10.1016/S0304-4017(03)00006-2.
Lefay D, Naciri M, Poirier P, Chermette R: Efficacy of halofuginone lactate in the prevention of cryptosporidiosis in suckling calves. Veterinary Record. 2001, 148: 108-112. 10.1136/vr.148.4.108.
Lindsay DS, Woods KM, Upton SJ, Blagburn BL: Activity of decoquinate against Cryptosporidium parvum in cell cultures and neonatal mice. Veterinary Parasitology. 2000, 89: 307-311. 10.1016/S0304-4017(00)00209-0.
Lorenzo-Lorenzo MJ, Ares-Mazas E, Villacorta Martinez de Maturana I: Detection of oocysts and IgG antibodies to Cryptosporidium parvum in asymptomatic adult cattle. Veterinary Parasitology. 1993, 47: 9-15. 10.1016/0304-4017(93)90171-I.
Lowery CJ, Millar BC, Moore JE, Xu J, Xiao L, Rooney PJ, Crothers L, Dooley JSG: Molecular genotyping of human cryptosporidiosis in Northern Ireland: epidemiological aspects and review. Irish Journal of Medical Science. 2001, 170: 246-250. 10.1007/BF03167789.
MacKenzie WR, Hoxie NJ, Proctor ME, Gradus MS, Blair KA, Peterson DE, Kazmierczak JJ, Addiss DG, Fox KR, Rose JB, Davis JP: A massive outbreak in Milwaukee of Cryptosporidium infection transmitted through the public water supply. New England Journal of Medicine. 1994, 331: 161-167. 10.1056/NEJM199407213310304.
McKenzie DM, Diffay BC: Diarrhoea associated with cryptosporidial oocyst shedding in a quarterhorse stallion. Australian Veterinary Journal. 2000, 78: 27-28. 10.1111/j.1751-0813.2000.tb10351.x.
Mancassola R, Richard A, Naciri M: Evaluation of decoquinate to treat experimental cryptosporidiosis in kids. Veterinary Parasitology. 1997, 69: 31-37. 10.1016/S0304-4017(96)01094-1.
Majewska AC, Solarczyk P, Tamang L, Graczyk TK: Equine Cryptosporidium parvum infections in western Poland. Parasitology Research. 2004, 93: 274-278. 10.1007/s00436-004-1111-y.
Miller RA, Bronsdon MA, Morton WR: Experimental cryptosporidiosis in a primate model. Journal of Infectious Diseases. 1990, 161: 312-315. 10.1093/infdis/161.2.312.
Moore DA, Atwill ER, Kirk JH, Brahmbhatt D, Herrera Alonso L, Hou L, Singer MD, Miller TD: Prophylactic use of decoquinate for infections with Cryptosporidium parvum in experimentally challenged neonatal calves. Journal of the American Veterinary Medical Association. 2003, 223: 839-845. 10.2460/javma.2003.223.839.
Morgan UM, Sargent KD, Elliot A, Thompson RCA: Cryptosporidium in cats - additional evidence for C. felis. Veterinary Journal. 1998, 156: 159-161. 10.1016/S1090-0233(05)80047-4.
Moriarty EM, McEvoy JM, Lowery CJ, Thompson HP, Finn M, Sheridan JJ, Blair IS, Mcdowell DA, Duff G: Prevalence and characterisation of Cryptosporidium species in cattle faeces and on beef carcasses at slaughter. Veterinary Record. 2005, 156: 165-168.
Munoz M, Alvarez M, Lanza I, Carmenes P: Role of enteric pathogens in the aetiology of neonatal diarrhoea in lambs and goat kids in Spain. Epidemiology and Infection. 1996, 117: 203-211. 10.1017/S0950268800001321.
Netherwood T, Wood JLN, Townsend HGG, Mumford JA, Chanter N: Foal diarrhoea between 1991 and 1994 in the United Kingdom associated with Clostridium perfringens, rotavirus, Strongyloides westeri and Cryptosporidium spp. Epidemiology and Infection. 1996, 117: 375-383. 10.1017/S0950268800001564.
OIE (Office International des Epizooties): Cryptosporidiosis. Manual of Standards for Laboratory Tests and Vaccines. Paris. 2004, [http://www.oie.int/eng/normes/en_mmanual.htm]Fifth
Okhuysen PC, Chappell CL, Sterling CR, Jakubowski W, DuPont HL: Susceptibility and serologic response of healthy adults to reinfection with C. parvum. Infection and Immunity. 1998, 66: 441-443.
Redman DR, Fox JE: The effect of varying levels DECCOX on experimental Cryptosporidia infections in Holstein bull calves. Proceedings of the 26th Annual Convention of the American Association of Bovine Practitioners. 1993, 157-159.
Report of Waterborne Cryptosporidiosis Subcommittee of the Scientific Advisory Committee: Health Protection Surveillance Centre, 25-27 Middle Gardiner Street, Dublin 1, Ireland. 2004
Riggs MW: Recent advances in cryptosporidiosis: the immune response. Microbes and Infection. 2002, 4: 1067-1080. 10.1016/S1286-4579(02)01631-3.
Ryan U, Xiao L, Read C, Zhou L, Lal AA, Pavlasek I: Identification of novel Cryptosporidium genotypes from the Czech Republic. Applied and Environmental Microbiology. 2003, 69: 4302-4307. 10.1128/AEM.69.7.4302-4307.2003.
Ryan UM, Samarasinghe B, Read C, Buddle JR, Robertson ID, Thompson RC: Identification of a novel Cryptosporidium genotype in pigs. Applied and Environmental Microbiology. 2003, 69: 3970-3974. 10.1128/AEM.69.7.3970-3974.2003.
Ryan UM, Monis P, Enemark HL, Sulaiman I, Samarasinghe B, Read C, Buddle R, Robertson I, Zhou L, Thompson RCA, Xiao L: Cryptosporidium suis n. sp. (Apicomplexa: Cryptosporidiidae) in pigs (Suis scrofa). Journal for Parasitology. 2004, 90: 769-773. 10.1645/GE-202R1.
Santin M, Trout JM, Xiao L, Zhou L, Greiner E, Fayer R: Prevalence and age related variation of Cryptosporidium species and genotypes in dairy calves. Veterinary Parasitology. 2004, 122: 103-117. 10.1016/j.vetpar.2004.03.020.
Siripanth C, Punpoowong B, Amarapal P, Thima N, Eampokalap B, Kaewkungwal J: Comparison of Cryptosporidium parvum development in various cell lines for screening in vitro drug testing. Southeast Asian Journal of Tropical Medicine and Public Health. 2004, 35: 540-546.
Skerrett HE, Holland CV: Asymptomatic shedding of Cryptosporidium oocysts by red deer hinds and calves. Veterinary Parasitology. 2001, 94: 239-246. 10.1016/S0304-4017(00)00405-2.
Smith HV, Corcoran GD: New drugs and treatment for cryptosporidiosis. Current Opinion in Infectious Diseases. 2004, 17: 557-564. 10.1097/00001432-200412000-00008.
Sturdee AP, Bodley-Tickell AT, Archer A, Chalmers RM: Long-term study of Cryptosporidium prevalence on a lowland farm in the United Kingdom. Veterinary Parasitology. 2003, 116: 97-113. 10.1016/S0304-4017(03)00261-9.
Sulaiman IM, Lal AA, Xiao L: A population genetic study of the Cryptosporidium parvum human genotype parasites. Journal of Eukaryotic Microbiology Suppl. 2001, 24S-27S. 10.1111/j.1550-7408.2001.tb00441.x.
Trampel DW, Pepper TM, Blagburn BL: Urinary tract cryptosporidiosis in commercial laying hens. Avian Diseases. 2000, 44: 479-484. 10.2307/1592566.
Tzipori S, Mccartney E, Lawson GHK, Rowland AC, Campbell I: Experimental infection of piglets with Cryptosporidium. Research in Veterinary Science. 1981, 31: 358-368.
UK National Reference Method 002, issued by the Veterinary and Public Health Test Standardisation Group: Standard Operating Procedure for the examination of faeces for Cryptosporidium. Ref no: NRM002-cryptosporidiosis[FEB05].doc. 2003, [http://www.defra.gov.uk/animalh/diseases/vetsurveillance/pdf/nrm-002crypto.pdf]
Xiao L, Bern C, Limor J, Sulaiman I, Roberts J, Checkley W, Cabrera L, Gilman RH, Lal AA: Identification of five types of Cryptosporidium parasites in children in Lima, Peru. Journal of Infectious Diseases. 2001, 183: 492-497. 10.1086/318090.
Xiao L, Fayer R, Ryan U, Upton SJ: Cryptosporidium taxonomy: Recent advances and implications for public health. Clinical Microbiology Reviews. 2004, 17: 72-97. 10.1128/CMR.17.1.72-97.2004.
Zardi EM, Picardi A, Afeltra A: Treatment of cryptosporidiosis in immunocompromised hosts. Chemotherapy. 2005, 51: 193-196. 10.1159/000086920.
Author information
Authors and Affiliations
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution 2.0 International License (https://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Zintl, A., Mulcahy, G., de Waal, T. et al. An Irish perspective on Cryptosporidium. Part 2. Ir Vet J 59, 495 (2006). https://doi.org/10.1186/2046-0481-59-9-495
Published:
DOI: https://doi.org/10.1186/2046-0481-59-9-495