
Abstract
Background and purpose
Surveillance studies evaluating antimicrobial susceptibilities are of great value in preventing the spread of resistant pathogens by elucidating the trend of resistance in commonly used antibiotics and as a consequence providing information for prescribing the most appropriate agent. This study is a longitudinal antimicrobial resistance surveillance study designed to evaluate the trend in antimicrobial resistance to gram negative microorganisms from 2007 to 2010.
Method
During a four-year period (2007–2010) isolates derived from all patients admitted to infectious diseases ward of Imam Khomeini Hospital, the major referral center for infectious disease in Iran with the highest admission rates, were evaluated. Based on disk diffusion method and zone of inhibition size, the microorganism was regarded as to be sensitive, resistant or has intermediate susceptibility to the antimicrobial agents.
Results
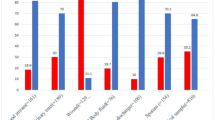
The widest spread Gram-negative microorganism in all of isolates taken together in our study was E.coli (30%) followed by Stenotrophomonas maltophilia in 28.6% and Enterobacter spp. in 11.9%, respectively. The susceptibility to amikacin, imipenem, piperacillin/tazobactam, and nitrofurantoin was equal or above 50% for all microorganisms over four years. However, the susceptibility to ampicillin, ampicillin/sulbactam, cefotaxim, and ceftriaxone was less than 50% in derived isolates during the study period.
Conclusion
In conclusion, the finding of the present study revealed that resistance rate to common antimicrobial agents in Iran is growing and isolates were susceptible mostly to broad-spectrum antibiotics including imipenem and piperacillin/tazobactam.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Antibiotic resistance is a critical challenge for infective diseases management around the word [1–3]. Infection with a resistant strain has been associated to higher rate of morbidity and mortality as well as prolonged length of hospital and intensive care unit stay and increased expenses for the healthcare systems [3, 4].
Surveillance studies evaluating antimicrobial susceptibilities are of great value in providing information for prescribing the most appropriate agent [5]. These studies could be used as a guide in antimicrobial usage policies in order to halt the expansion of microorganism resistance [6–10].
Although there are few reports on the antibiotic resistance in Iran, many of them are simple point-in-time prevalence studies or evaluated pathogens involved in a specific infectious disease [11–14]. Present evaluation is a longitudinal antimicrobial resistance surveillance study designed to evaluate the trend in antimicrobial resistance to nosocomial origin gram negative microorganisms, from 2007 to 2010.
Methods
During a four-year period (2007–2010) isolates biological samples from all patients admitted to Infectious Diseases Ward of Imam Khomeini Hospital Complex, the major referral center for infectious disease in Iran with the highest admission rates, were evaluated. The Institutional Review Board (IRB) and the Medical Ethics Committee of the hospital approved the study.
Isolates were sent to a central laboratory of the hospital for identification and antimicrobial susceptibility testing by Kirby – Bauer disc diffusion method. Based on zone of inhibition size the microorganism was regarded as to be sensitive, resistant or intermediate susceptibility to the antimicrobial agent. Microorganisms’ susceptibilities were investigated against those antimicrobials of clinical utility for the treatment of infections caused by susceptible Gram- negative bacteria available in the hospital. β-lactams such as ampicillin and piperacillin from penicillin class; cephalosporins including cefixime, cefotaxim, ceftazidim, ceftriaxone, cefepime; and the carbapenems such as imipenem were among evaluated antimicrobials. Combinations of penicillins with β-lactamase inhibitors including piperacillin-tazobactam and ampicillin-sulbactam, fluroquinolones such as ciprofloxacin, aminoglycosides including amikacin and gentamicin, nitrofurantoin and cotrimoxazole were those studied for antimicrobial resistance pattern in this surveillance. The trend in this pattern over four years was reviewed and reported.
Results
In a four-year period from 2007 to 2010, 1745 isolates were sent to the central library of the hospital, from those 983 (56.3%) were confirmed to be Gram-negative pathogens. The most frequent specimen sources were blood (46.2%) followed by the urine (27%), and wound (13.7. The most wide spread Gram-negative microorganism in all of isolates taken together in our study was E.coli (30%) followed by Stenotrophomonas maltophilia in 28.6% and Enterobacter spp. in 11.9%, respectively. The frequency of microorganisms in terms of the derived isolates is shown in Table 1.
The overall susceptibility of the specimens to antimicrobial agents did not remain the same over four years. For some of antimicrobial agents, the percentage of susceptible microorganisms was increased including ciprofloxacin (44.2 to 68.4%), piperacillin(33.3 to 66.7%) and piperacillin/tazobactam (77.8 to 89.5%). In contrast the susceptibility of nosocomial pathogens was reduced against nitrofurantoin (75.9 to 56%) in a four-year period. The susceptibility of microorganisms against all other antimicrobial agents showed non-steady pattern. The susceptibility to amikacin, imipenem, piperacillin/tazobactam, and nitrofurantoin was equal or above 50% for microorganisms all over four years. However, the susceptibility to ampicillin, ampicillin/sulbactam, cefotaxim, and ceftriaxone was less than 50% in derived isolates during the study period. The resistance rate of microorganism to Cefepime was increased in 2007–2008 while the susceptibilities were enhanced in 2009–2010.Comparison of the trend of resistance pattern of isolated bacteria of nosocomial originas well as the rate of frequency of each pathogen was illustrated in Table 2. Regarding the microorganisms, the most frequent resistances were seen in Acientobacter followed by Citrobacter with 50–73.7% and 58.3-65.8% resistant isolates, respectively. In contrast, Enterobcter was the most susceptible microorganism with resistance rate of 25.6-29.5% in the study period. The switches in the percent of resistant microorganism were not the same for all of the pathogens (Table 3). Proteus resistance was decreased in four-year period from 43.9% to 6.7% against all of the antibiotics taken together. Acinetobacter resistance to ciprofloxacin was increased whereas Enterobacter resistance rate to Gentamicin and Ciprofloxacin and E.coli resistance to Ceftazidim was decreased in four-year period. The number of resistant Entrobacter i solates to Cefixim was increased. From 2008 to 2010 the susceptibility rate of Acinetobacter against Ampicillin/sulbactam was reduced.
Discussion
Antimicrobial resistance is a widespread problem that health care providers are encountered with all over the world. Determining the specific pattern of antibiotic resistance especially in infectious diseases wards of main hospitals in every country is of great value for controlling the rate of increasing resistance as well as helping in empirical treatment. Since Imam Khomeini hospital Complex is the main center for infectious diseases in Iran with the highest admission rates, we can say that a serious problem of antimicrobial resistance to commonly used antibiotics exists among different isolates in Iran.
The most frequent isolated pathogen from all specimens taken together was E. coli followed by S. maltophilia and Enterobacter sp. with E. coli being the major derived pathogen from urine and S. maltophilia from bloodstream samples. In a similar Korean study, E. coli had the first rank in terms of the most prevalent organism isolated, Pseudomona sp., and Klebseilla sp. had the next ranks among isolated gram-negative pathogens [15]. During 2000 to 2002, more than 220,000 isolated were collected from intensive care units of five countries including France, Germany, Italy, Canada and United States, in which the most common gram-negative pathogen was E. coli followed by Pseudomona sp.[16]. S. maltophilia which was the most common pathogen for bloodstream samples in the present study, were less common in western countries, however it was also seen frequently in Saudi isolates [17].
Antibiotic resistance among Acinetobacter spp., and Citrobacter spp. were more frequent in comparison with other isolated pathogens, and our susceptibility rates were similar to rates reported from other regions of the world [18, 19]. However, the susceptibility rate of Acinetobacter spp. in our study was less than similar surveillance five-year study in Children Medical Center in Iran [20] and was more consistent with reports of antimicrobial resistance from other parts of the world [19, 21]. Since that Iranian report dated back to approximately a decade ago, this may demonstrate the increase in the rate of Acinetobacter resistance in Iran like other countries over the world. Moreover, the resistance frequency rate of Acinetobacter to Ampicillin/sulbactam had an increasing trend after 2007. This was because the availability of generic Iranian formulation of this specific antibiotic in 2007 as well as the administration of oral dosage forms which was used widespread in that year.
The most commonly administered antibiotics in different countries all over the world are β-lactams, and decreased susceptibility of nosocomial pathogens to this therapeutic class of antibiotics has resulted in a major clinical disaster [22]. Iran is not an exception for this statement, and cephalosporines are commonly used in the country because of their availability as well as low rate of adverse events [12]. With respect to antibiotics, the most frequent resistance to antibiotics was observed in ampicillin (66.7-100%) and third generation cephalosporines consisting of cefotaxime (57.2-100%), ceftazidim (42.1-86.4%), cefixime (45-75%) and ceftriaxone (65.7-74.8%). To elucidate the importance of increasing resistance, it is worth mentioning that even the resistant rate of Enterobacter as the most susceptible microorganism to cefixime was increased in a four-year period. In contrast, the lowest resistant rates were seen with imipenem (4.5-26.5%),piperacillin/tazobactam (7.9-22.2%), and amikacin (21.3-33.3%). Resistance to third generation cephalosporines in this study was higher than similar studies evaluating the susceptibility rates of gram-negative pathogens [23–25]. This higher resistance can be attributed to the frequent use of third generation cephalosporines in the empirical management of infectious in Iran as the resistance rate of E.coli to ceftazidim was reduced after its administration was reduced and it was omitted from local protocols of empiric treatment for a period of time. Resistance of microorganisms to Cefepime, as a fourth generation cephalosporine, had an increasing trend in 2007–2008 but with restrictions in its usage the susceptibility rates were improved in 2009–2010.In contrast to previous studies that reported an increase in the resistance rate to fluoroquinolones [26, 27], we found an improving susceptibility to ciprofloxacin in our study in a four-year period with Acinetobacter as an exception. This can be partly explained by the fact that fluoroquinolones are not routinely used as an empirical antibiotic for infectious diseases in Imam Hospital. In the present study, resistance to ciprofloxacin was 31.6-54.5% that was less than similar previous evaluation in Argentina with resistance rate of more than 80% [28]. On the other hand, the majority of the nosocomial pathogens from various specimen resources in the present study were susceptible to imipenem and this was consistent through the assessment period. As there was a correlation between previous use of fluoroquinolones and imipenem resistance [29, 30], the low administration rate of ciprofloxacin and as a consequence improved sensitivity of organisms to this agent can be the reason behind the susceptibility of most of the organisms to imipenem. The low resistance rate of isolates to imipenem was also reported in previous Belgian and Polish studies with 13% and 8% resistant isolated, respectively [23, 25]. In contrast, in Turkish patients resistance to imipenem was slightly more prevalent than that of our study [31]. Amikacin was among the most active antimicrobial agents against isolates with the low resistant rate of 21.3-33.3%. Studies performed over a long time period revealed that the increase in resistance to aminoglycosides is milder than for any other antimicrobial agent even with continued administration [32, 33].
In conclusion, the finding of the present study revealed that resistance rate to common antimicrobial agents in Iran is growing and isolates were susceptible mostly to broad-spectrum antibiotics including imipenem and piperacillin/tazobactam. As the antibiotic resources of developing countries including Iran are limited, periodic surveillances of antimicrobial resistance patterns play a vital role in controlling the spread of resistant strains as well as implementing protocols for halting the process. Moreover, it is rational to establish a committee for appropriate antibiotic administration to control the use of antimicrobial agents at the same time of performing surveillance studies for the aim of effective infection management. Such surveillance studies could help in limiting the rate of antimicrobial resistance all over the world.
References
Masterton RG: Surveillance studies: how can they help in the management of infection?. J Antimicrob Chemother. 2000, 46: 53-58.
Masterton R, Drusano G, Paterson DL, Park G: Appropriate antimicrobial treatment in nosocomial infections—the clinical challenges. J Hosp Infect. 2003, 55: 1-12.
Kollef MH, Fraser VJ: Antibiotic resistance in the intensive care unit. Ann Intern Med. 2001, 134: 298-314.
Kollef M: Appropriate empirical antibacterial therapy for nosocomial infections: getting it right the first time. Drug. 2003, 63: 2157-2168. 10.2165/00003495-200363200-00001.
Turner PJ: Trends in antimicrobial susceptibilities among bacterial pathogens isolated from patients hospitalized in European medical centers: 6-year report of the MYSTIC Surveillance Study (1997–2002). Diagn Microbiol Infect Dis. 2005, 51: 281-289. 10.1016/j.diagmicrobio.2004.11.013.
Morris AK, Masterton RG: Antibiotic resistance surveillance: action for international studies. J Antimicrob Chemother. 2002, 49: 7-10.
Lewis D: Antimicrobial resistance surveillance: methods will depend on objectives. J Antimicrob Chemother. 2002, 49: 3-5.
Fontana R, Lo CG, Giacobone E, Romero E, Cipriani P, Sessa R, Franchino L: Resistance surveillance in Italy: four-year results from the MYSTIC Program. J Chemother. 2002, 14: 323-331.
Garcia-Rodriguez JA, Jones RN, The MYSTIC Programme Study Group: Antimicrobial resistance in Gram-negative isolates from European intensive care units: data from the Meropenem Yearly Susceptibility Test Information Collection (MYSTIC) Programme. J Chemother. 2002, 14: 25-32.
Masterton RG, Kuti JL, Turner PJ, Nicolau DP: The OPTAMA Programme: utilizing MYSTIC (2002) to predict critical pharmacody- namic target attainment against nosocomial pathogens in Europe. J Antimicrob Chemother. 2005, 55: 71-77.
Aslani MM, Alikhani MY, Zavari A, Yousefi R, Zamani AR: Characterization of enteroaggregative Escherichia coli (EAEC) clinical isolates and their antibiotic resistance pattern. Int J Infect Dis. 2011, 15: e136-e139. 10.1016/j.ijid.2010.10.002.
Hadadi A, Rasoulinejad M, Maleki Z, Yonesian M, Shirani A, Kourorian Z: Antimicrobial resistance pattern of Gram-negative bacilli of nosocomial origin at 2 university hospitals in Iran. Diagn Microbiol Infec Dis. 2008, 60: 301-305. 10.1016/j.diagmicrobio.2007.10.010.
Vessal G, Afhami S, Gholami K, Shafaghi B, Yazdi SH: Evaluation of antimicrobial resistance among gram-negative isolates collected from intensive care units and reliability of routine disc susceptibility tests at a teaching hospital in tehran. Iranian Journal of Pharmaceutical Research. 2006, 2: 89-100.
Bush K: Bench-to-bedside review: The role of β-lactamases in antibiotic-resistant Gram-negative infections. Crit Care. 2010, 14: 224-10.1186/cc8892.
Lee K, Lee MA, Lee CH, Lee J, Roh KH, Kim S, Kim JJ, Koh E, Yong D, Chong Y: KONSAR Group. Increase of ceftazidime- and fluoroquinolone-resistant Klebsiellapneumoniae and imipenem-resistant Acinetobacter spp. in Korea: analysis of KONSAR study data from 2005 and 2007. Yonsei Med J. 2010, 51: 901-911. 10.3349/ymj.2010.51.6.901.
Jones ME, Darghi DC, Thornsberry C, Karlowsky JA, Sahm DF, Wenzel RB: Emerging resistance among bacterial pathogens in the intensive care unit: A European and North American Surveillance study 2000–2002. Ann Clin Microbiol Antimicrob. 2004, 3: 14-10.1186/1476-0711-3-14.
Al-Johani SM, Akhter J, Balkhy H, El-Saed A, Younan M, Memish Z: Prevalence of antimicrobial resistance among gram-negative isolates in an adult intensive care unit at a tertiary care center in Saudi Arabia. Ann Saudi Med. 2010, 30: 364-369.
Winokur PL, Canton R, Casellas JM, Legakis N: Variations in the prevalence of strains expressing an extended spectrum β-lactamase phenotype and characterization of isolates from Europe, the Americas, and the Western Pacific region. Clin Infect Dis. 2001, 32: S94-S103. 10.1086/320182.
Gales AC, Jones RN, Forward KR, Linares J, Sader HS, Verhoef J: Emerging importance of multi-drug resistant Acinetobacter species and Stenotrophomonas maltophiliaas pathogens in seriously ill patients: geographic patterns, epidemiological features, and trends in the SENTRY Antimicrobial Surveillance Program (1997–1999). Clin Infect Dis. 2001, 32: S104-S113. 10.1086/320183.
Mamishi S, Pourakbari B, Ashtiani MH, Hashemi FB: Frequency of isolation and antimicrobial susceptibility of bacteria isolated from bloodstream infections at Children’s Medical Center, Tehran, Iran, 1996–2000. Int J Antimicrob Agents. 2005, 26: 373-379. 10.1016/j.ijantimicag.2005.08.004.
Fluit AC, Jones ME, Schmitz FJ, Acar J, Gupta R, Verhoef J: Antimicrobial susceptibility and frequency of occurrence of clinical blood isolates in Europe from the SENTRY antimicrobial surveillance pro- gram, 1997 and 1998. Clin Infect Dis. 2000, 30: 454-460. 10.1086/313710.
Jean SS, Teng LJ, Hsueh PR, Ho SW, Luh KT: Antimicrobial susceptibilities among clinical isolates of extended-spectrum cephalosporin-resistant Gram-negative bacteria in a Taiwanese University Hospital. J Antimicrobiol Chemother. 2002, 49: 69-76.
Glupczynski Y, Delmee M, Goossens H, Struelens M: Belgian Multicenter ICU Study Group. Distribution and prevalence of antimicrobial resistance among gram-negative isolates in intensive care units (ICU) in Belgian hospitals between 1996 and 1999. Acta Clin Belg. 2001, 56: 297-306.
Ishii Y, Alba J, Kimura S, Yamaguchi K: Evaluation of antimicrobialactivity of betalactam antibiotics by E-test against clinical isolates from100 medical centers in Japan. Diagn Microbiol Infect Dis. 2006, 55: 143-148. 10.1016/j.diagmicrobio.2006.01.001.
Patzer J, Dzierzanowska D, Turner P: Susceptibility patterns of Gram- negative bacteria from a Polish intensive care unit, 1997–2000. Int J Antimicrob Agents. 2002, 9: 431-434.
Ko WC, Hsueh PR: Increasing extended-spectrum b-lactamase production and quinolone resistance among Gram-negative bacilli causing intra-abdominal infections in the Asia/Pacific region: Data from the Smart Study 2002–2006. J Infect. 2009, 59: 95-103. 10.1016/j.jinf.2009.06.003.
Karlowsky JA, Jones ME, Draghi DC, Thornsberry C, Sahm DF, Volturo GA: Prevalence and antimicrobial susceptibilities of bacteria isolated from blood cultures of hospitalized patients in the United States in 2002. Ann Clin Microbiol Antimicrob. 2004, 3: 7-14. 10.1186/1476-0711-3-7.
Rodriguez CH, Juarez J, de Mier C, Pugliese L, Blanco G, Vay C: Bacterial resistance to antibiotics in gram-negative rods isolated from intensive care units. Comparative analysis between two periods (1998 and 2001). Medicina. 2003, 63: 21-27.
Lautenbach E, Weiner MG, Nachamkin I, Bilker WB, Sheridan A, Fishman NO: Imipenem resistance among Pseudomonas aerugi- nosa isolates: risk factors for infection and impact of resis- tance on clinical and economic outcomes. Infect Control Hosp Epidemiol. 2006, 27: 893-900. 10.1086/507274.
Tanimoto K, Tomita H, Fujimoto S, Okuzumi K, Ike Y: Fluoroquinolone enhances the mutation frequency for meropenem-selected carbapenem resistance in Pseudomonas aeruginosa, but use of the high-potency drug doripenem inhibits mutant formation. Antimicrob Agents Chemother. 2008, 52: 3795-3800. 10.1128/AAC.00464-08.
Kucukates E: Antimicrobial resistance among Gram-negative bacteria isolated from intensive care units in a Cardiology Institute in Istanbul Turkey. Jpn J Infect Dis. 2005, 58: 228-231.
Gerding DN, Larson TA, Hughes RA: Aminoglycoside resistance and aminoglycoside usage: ten years of experience in one hospital. Antimicrob Agents Chemother. 1991, 35: 1284-1290. 10.1128/AAC.35.7.1284.
Hsueh PR, Chen WH, Luh KT: Relationships between antimicrobial use and antimicrobial resistance in Gram-negative bacteria causing nosocomial infections from 1991–2003 at a university hospital in Taiwan. Int J Antimicrob Agents. 2005, 26: 463-472. 10.1016/j.ijantimicag.2005.08.016.
Acknowledgement
We must appreciate the staffs of Valiasr Laboratory Department for their supports.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors have not any conflict of interest about this work and have not any financial support.
Authors’ contributions
MRS collected the culture and anti-biogram results of the patients from the microbiology laboratory. HK is main supervisor of the study and organized the data, SJ was responsible for clinical interpretation of the results, AA was responsible for the laboratory data analysis, Statistical analysis was done by ZJR and SDK and AH-T prepared the manuscript. All authors read and approved the final manuscript.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Khalili, H., Dashti-Khavidaki, S., Shahidi, MR. et al. Changes in gram negative microorganisms’ resistance pattern during 4 years period in a referral teaching hospital; a surveillance study. DARU J Pharm Sci 20, 28 (2012). https://doi.org/10.1186/2008-2231-20-28
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/2008-2231-20-28