
Abstract
Since the first reports of AIDS, skin involvement has become a burdensome stigma for seropositive patients and a challenging task for dermatologist and infectious disease specialists due to the severe and recalcitrant nature of the conditions. Dermatologic manifestations in AIDS patients act as markers of disease progression, a fact that enhances the importance of understanding their pathogenesis.
Broadly, cutaneous disorders associated with HIV type-1 infection can be classified as primary and secondary. While the pathogenesis of secondary complications, such as opportunistic infections and skin tumours, is directly correlated with a decline in the CD4+ T cell count, the origin of the certain manifestations primarily associated with the retroviral infection itself still remains under investigation.
The focus of this review is to highlight the immunological phenomena that occur in the skin of HIV-1-seropositive patients, which ultimately lead to skin disorders, such as seborrhoeic dermatitis, atopic dermatitis, psoriasis and eosinophilic folliculitis. Furthermore, we compile the latest data on how shifts in the cytokines milieu, impairments of the innate immune compartment, reactions to xenobiotics and autoimmunity are causative agents in HIV-1-driven skin diseases. Additionally, we provide a thorough analysis of the small animal models currently used to study HIV-1-associated skin complications, centering on transgenic rodent models, which unfortunately, have not been able to fully unveil the role of HIV-1 genes in the pathogenesis of their primarily associated dermatological manifestations.
Similar content being viewed by others


Review
More than 25 years have passed since the first reports on AIDS, and we are still unable to fully understand the complexity of this disease. Dermatologic disorders play a unique role in the HIV-1/AIDS spectrum, as almost all seropositive patients suffer from these debilitating and often disfiguring lesions [1]. Cutaneous disorders associated with HIV-1/AIDS undermine self-esteem and induce depression, conditions that put patients at high risk of suicide.
Since the description of Kaposi's sarcoma as an AIDS-related condition, 56 other cutaneous disorders have been linked to HIV-1/AIDS [2]. Although the introduction of highly active antiretroviral therapy (HAART) significantly decreased the prevalence of opportunistic infections and Kaposi's sarcoma, the prevalence of most inflammatory conditions primarily related to HIV-1 remains constant [3, 4]. Nevertheless, while most of these dermatological manifestations directly associated with HIV-1/AIDS are currently considered as markers of disease progression, the pathogenesis of some of them is not completely understood yet [5]. Recent explanations about the pathogenesis of these disorders suggest that not only the decline in CD4+ T cell counts [6], but also the shift into a Th2 cytokine profile [7], the molecular mimicry [8] and the over-expression of superantigens/xenobiotics [9], play a decisive role in the development of dermatological lesions in the context of HIV-1 infection.
Importantly, there is still a lack of conclusive evidence linking HIV-1-associated gene products to the pathogenesis of primary dermatological disorders seen in AIDS patients. This fact derives from multiple factors that include: (1) the shortage on biosafety level 3 (BSL-3) facilities and BSL-3-trained individuals; (2) the expenses associated with non-human primate studies; and (3) the lack of small animal models to study this particular disease. In order to overcome the latter, many groups, including ours, have created transgenic rodent models (rat and mouse) for the study of HIV-1-associated complications; however, none of these has successfully reproduce the data obtained from AIDS patients [10–14]. This report compiles the most recent data on the pathogenesis of inflammatory cutaneous pathology directly associated with HIV-1 infection, and discusses the reasons why transgenic animal models have failed to fully unveil the origin of many complications seen in AIDS patients.
General immunologic cutaneous changes in the patient with HIV-1 infection
The skin is the largest and most visible organ in the body, and consequently presents the most numerous and miscellaneous types of pathological manifestations. The cutaneous immune system is unique in the fact that it contains two types of antigen-presenting cells: the Langerhans cells; and the dermal dendritic cells [15]. Both subsets of cells perform a coordinated series of events upon antigen encounter, resulting in the presentation of processed antigens to naïve T cells in the draining lymph nodes. Once activated, T cells undergo clonal expansion and home to specific sites where their expression of effector soluble factors (cytokines and chemokines) orchestrates a coordinated contention of viral, bacterial, fungal, parasitic or neoplastic invasion [16].
In HIV-1-seropositive patients, the aforementioned process is abrogated in many ways. AIDS patients exhibit a marked decrease in the number and function of Langerhans cells, CD4+, NK cells, macrophages and monocytes [17–20] (Figure 1). While the final outcome of HIV-1 infection is the decrease in these cell types, the mechanisms by which HIV performs such lytic activities still remains controversial. Pope et al [21] showed that physical contact between HIV-1-pulsed dendritic cells and CD4+ T cells in the context of antigen presentation promotes massive replication of the virus with a cytolytic outcome to both cells types. Moreover, the compromise of the skin-associated immune system is so critical that delayed-type hypersensitivity tests now commonly serve as monitors for the progression of the disease [22]. As a consequence of such decline in the number of antigen-presenting and CD4+ T cells, the skin becomes vulnerable to numerous opportunistic infectious agents and neoplastic disorders; however, in this article we are going to focus mainly on describing the pathogenesis of the inflammatory conditions related primarily to HIV-1 infection.

HIV-1-driven immunological changes in the skin. Graphic representation of the immunological processes involved in the pathogenesis of primary HIV-1 related skin disorders, highlighting the presentation of the virus by a dendritic cell to a CD4+ T lymphocyte and the subsequent changes in the cytokine profile that are brought by the death of Th1 cells.
The clinical picture
The description of skin manifestations in HIV-1/AIDS patients is complex and ranges from acne vulgaris to Kaposi's sarcoma. A brief classification of the most common dermatologic disorders in HIV-1/AIDS patients is depicted below and categorizes the spectrum of diseases in two groups: primary HIV-1-related skin disorders; and secondary mucocutaneous signs of HIV-1 infection (Table 1).
Noteworthy, secondary manifestations of HIV-1 infection are more prevalent than primary ones. For example, in Africa, the most prevalent skin disorder in HIV-1/AIDS patients is prurigo nodularis [23–25], a pruritic condition associated with insect bites [26]. In several other countries, mucocutaneous candidiasis and herpes zoster infections are the leading cause of skin disorders in these patients [27, 28].
Nevertheless, a decline of certain skin disorders in HIV-1/AIDS patients has already been observed ever since HAART became more accessible to HIV-1/AIDS patients [29]. Normal CD4+ lymphocyte counts reduce the chances of suffering from co-infectious and neoplastic disorders[3]. Moreover, in developed countries, where most people have access to HAART, dermatologic conditions, such as Kaposi's sarcoma, prurigo nodularis, molluscum, and photodermatitis, are becoming rare [3, 4].
However, the prevalence of most cutaneous disorders associated primarily with HIV-1 infection, as well as adverse drug reactions, have not changed in the presence of HAART [4]. This fact enhances the importance of studying the pathogenesis of these disorders in order to develop superior forms for their treatment.
HIV-1-associated primary dermatologic disorders
Seborrheic dermatitis
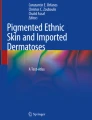
This is an entity characterized by erythema and scaling of the central part of the face, involving nasolabial folds and eyebrows, as well as the scalp [30] (Figure 2A). It is found in up to 40% of seropositive patients [30] and in up to 80% of patients with AIDS compared with 3% of the seronegative population [31, 32]. Berger and Greene in 1991 [33] reported that this condition could be a hypersensitivity reaction to Pityrosporum yeasts, but its association is still doubtful (Figure 1). However, recent studies have failed to demonstrate any fungal overgrowth [34] or a rise in the levels of IgG titers against the yeast in HIV-1-seropositive patients [35, 36].

HIV-1 primary skin disorders. A) Patient with seborrheic dermatitis showing a papulosquamous disorder patterned on the sebum-rich areas of the scalp and face. B) Representative section (H&E 20x) shows focal parakeratosis, moderarte acanthosis, spongiosis related to hair follicles and scarce neutrophils. C) Patient with atopic dermatitis with lesions ranging from weeping crusted areas to lichenified plaques. D) Representative section (H&E 20x) shows acanthosis, mild spongiosis, and dermal infiltrate composed of lymphocytes, monocytes and few eosinophils. E) Patient with psoriasis, characterized by symmetric raised inflamed lesions covered with a silvery white scale in both lower limbs. F) Representative section (H&E 10x) shows hyperkeratosis, parakeratosis, acanthosis, spongiosis, absence of granulosum layer and neutrophil infiltrates (Munro's microabscess). G) Patient with eosinophilic folliculitis featured by follicular pustular papules on the upper part of the chest. H) Representative section (H&E 20x) shows perifollicular and perivascular infiltrate with eosinophils.
Histologically, the lesions of seborrheic dermatitis in patients without HIV-1 show spongiform features, and with time they become less spongiotic and develop follicular plugs of orthokeratotic and parakeratotic cells, and uneven rete ridges [37] (Figure 2B). Skin biopsy specimens taken from lesions of AIDS patients show widespread parakeratosis, keratocytic necrosis, leukoexocytosis and superficial perivascular infiltrate of plasma cells [38]. These sections also show expression of heat-shock proteins (HSP65 and HSP72), a phenomenon that does not occur in HIV-1-negative patients [39]. Seborrheic dermatitis has been linked to depression of T cell function, and in patients with HIV-1 infection, it appears at early stages and worsens as the CD4+ lymphocyte count declines. Thus, it can be used as a marker for disease progression [5, 40].
Xerosis
Dryness of the skin is one of the most common skin manifestations found in patients with HIV-1 infection. This condition is found in more than 20% of people with HIV-1 [41]. It presents mainly on extremities, and it denotes one of the main causes of pruritus in AIDS patients [42]. Its pathogenesis has been suggested to include changes in the microcirculation, the nutrient supply of the skin, and in the production of sweat and oil in the skin [43]. Xerosis has also been related to certain effects on the mast cell population of the skin and to the decreased skin innervation caused by AIDS [43, 44]. Reports show that such substances as calcitonin gene-related peptide and such mediators as substance P are decreased in the skin of these patients [45] (Figure 1). Xerosis has been taken by several authors as a marker for progression as it also correlates with CD4+ T lymphocyte count decline [46].
Atopic dermatitis
This chronic inflammatory skin condition is seen in approximately 30% to 50% of HIV-1/AIDS patients (Figure 2.C) [43, 47] compared with 2% to 20% of the seronegative population [48]. This is a pruritic disorder mediated by Th2 cytokines, whose morphological features include acanthosis and spongiosis, as well as cellular infiltrates composed of lymphocytes, monocytes and eosinophils (Figure 2.D). The pathogenesis of this disorder has been linked to hypereosinophilia and to high levels of IgE secondary to Th1-Th2 imbalance [49]. Changes in cutaneous innervation and peptidergic neurotransmitters have also been related to this disease [50].
A study performed of 74 patients with atopic dermatitis showed that 53% were colonized by toxic-shock-syndrome toxin I produced by S. aureus [9]. These superantigens penetrate the skin and bind to Langerhans cells, thereby stimulating the release of IL-4 and IL-5, which further enhance the production of the allergen-specific IgE response [51]. Broadly, atopic dermatitis is thought to be initiated in predisposed individuals by a Th2 dominant cytokine production that enhances IgE release [52] (Figure 1). This Th1/Th2 cytokine imbalance is practically seen in all AIDS patients, specially in later stages, when this situation predisposes atopic manifestations [53].
Psoriasis
This is a chronic inflammatory skin disorder of presumed autoimmune origin found in 2% of the general population [54]. The cause of psoriasis is still under debate, but it is generally accepted to have a genetic hereditary component, and a hyperproliferative epidermal nature driven by activated lymphocytes [55]. The prevalence of psoriasis in HIV-1-seropositive individuals is similar to that of their seronegative counterparts [56]. However, psoriatic lesions in AIDS patients tend to be more severe, acral, extensive, destructive and recalcitrant [54, 57] (Figures 2E and 2F). Of note, the prevalence of psoriatic arthritis is greatly increased in the HIV-1/AIDS population compared with its immunocompetent counterpart [58].
The pathogenesis of psoriasis in the context of HIV-1 infection has been associated with many immunologic events that include a decrease in the number of Langherhan's cells, but also with a potential epidermal proliferative effect of HIV-1 itself, an altered CD8:CD4 ratio and high synthesis of nitric oxide driven by HIV-1 in macrophages [56]. This association has actually led to an obscure hypothesis involving psoriasis and psoriatic arthritis with a retroviral background [59, 60].
In fact, in patients with known risk for HIV-1 exposure, new onset of psoriasis may sometimes be a marker of HIV-1 infection [61]. A full comparative analysis between HIV-1-related and HIV-1-negative psoriasis is depicted in Table 2.
Expanding on the pathogenesis of psoriasis, the causative trigger of the lymphocytic activation remains unknown; however, self-antigens may play a significant role in breaking the peripheral tolerance [69]. Recently, there is growing evidence that links certain conditions of autoimmune origin to human endogenous retroviruses (HERVs) [8, 70]. HERVs are genomic sequences that use reverse transcriptase and that can move from one chromosomal site to another, belonging to a class of parasitic elements that represent as much as 40% of the mammalian genome [71].
These elements were integrated into our genome million of years ago, when exogenous retroviruses infected germ cells; once integrated, these sequences were transmitted vertically as mutations of essential genes in a mendelian fashion [70]. Retrovirologists often refer to HERVs as defective proviruses with accumulated deletions, frame shift mutations, or with stop codons in gag, pol or env open reading frames, that limit their infectious capacity [8]. The activation of these dormant sequences of the genome has been linked to the pathogenesis of several autoimmune diseases, including most of the chronic arthropathies and systemic lupus erythematosus [72, 73]. Several HERVs are expressed in normal peripheral blood lymphocytes [74], keratinocytes [75] and many other tissues [76].
Notably, the hypothesis associating HERVs with psoriasis resulted from the detection of viral-like particles resembling murine C-type retrovirus in psoriatic plaques in 1983 [77]. The microscopic findings were further supported by the detection of p27, a retrovirus-like particle in skin and lymphocytes from psoriatic patients [78, 79], and more recently, by the detection of an increased titers of IgG anti-murine leukaemia virus antibodies in serum from patients with psoriasis when compared with a healthy control [80].
A reasonable explanation of this association involves molecular mimicry as the main phenomenon [70]. In the context of viral infection, similarities between viral amino acids and those found in host proteins lead to an autoimmune reaction mediated either by T lymphocytes or auto-antibodies that may last even after resolution of the viral infection (Figure 3) [81]. Activation of HERVs not only depend on retroviral infection, but they can also by activated in the presence of ultraviolet light or certain chemicals [69].

Human endogenous retroviruses and their hypothetical role in psoriasis. During HIV-1 infection, HIV-1 tat protein acts as a trans-acting factor activating HERV's long terminal repeat (LTR). Stimulation of the trans-activation region (TAR) by its interaction with the HIV-1 tat protein activates transcription. Subsequently, exogenous retroviruses trigger an immune response, and HERV-encoded proteins are recognized as self-antigens (molecular mimicry) awakening a cellular-based autoimmune phenomenon.
Recently, sequences of three different families of HERVs have been identified in psoriatic lesions [69]. Sequences of families W,E,K, and a new sequence of the ERV-9/HERV-W family were identified by the use of reverse transcriptase-polymerase chain reaction. This sequence contains at least two open reading frames that could encode for a gag protein and a retroviral protease. The expression of this sequence was detected in 29 of 43 lesional psoriasis skin samples, and in only two of 21 of normal skin samples [69]. Supporters of this theory consider Koebner's phenomenon as the result from the damage of keratinocytes that expose viral proteins to the immune system [70].
In addition, Mallon et al have suggested HIV-1-associated immune dysregulation as a possible trigger of psoriasis in those patients carrying the HLA-Cw0602 alele [62]. The HLA-Cw0602 alele might be a target for CD8 lymphocytes responding to processed peptides presented in the context of major histocompatibility complex-1, strengthening the argument for an important role for CD8 T lymphocytes in the immunopathogenesis of psoriasis.
Eosinophilic folliculitis
This is a cutaneous manifestation almost exclusively related to HIV-1 infection, particularly in late stages of AIDS. It was first described in 1986 [82] as a different entity from Ofuji's disease (pruritic follicular papules and pustules that involve palms and soles). Eosinophilic folliculitis (EF) presents with increased serum IgE levels, eosinophlia and peripheral leukocytosis; palms and soles are spared [83]. The most common presentation of EF is an erythematous urticarial papular rash with some pinpoint vesicles or pustules on the face, neck, and upper chest and back, almost exclusively above the nipple line [46] (Figure 2G).
Histology of the lesions shows follicular spongiosis and folliculocentric mixed inflammatory infiltrate of eosinophils, lymphocytes, hystiocytes, mast cells and neutrophils around the outer root sheaths of hair follicles [84] (Figure 2H).
EF is typically seen when CD4+ cell count drops below 300 cells/mm3 [85]. The suggested pathogenesis involves a Th2 cytokine response to an unknown antigen (Pityrosporum ovale or Demodex folliculorum) [86], with elevation of interleukin-4, interleukin-5 and the chemokines RANTES (chemokine that mediates chemotaxis, recruits eosinophils in the allergic late phase reaction) and Eotaxin ( a chemoattractant for eosinophils, basophils, mast cells and Th-2 lymphocytes) [7] (Figure 1). Additionally, EF has also been described as an autoimmune reaction to the sebocyte [87].
A clinical entity, called necrotizing eosinophilic folliculitis, describes the spectrum of the disease in AIDS patients who are atopic and develop ulceration, nodules and dermal follicular necrosis [88]. Its pathogenesis suggests an unrepressed Th2-type response to epicutaneous stimuli in atopic individuals [88]. EF has been interpreted as a marker of HIV-1 infection for subjects who have a high risk of developing opportunistic infections [89], but it is also part of the immune reconstitution syndrome when antiretroviral therapy is started [90].
Miscellaneous disorders
Other dermatologic manifestations have been associated primarily with HIV-1 infection. Photodermatitis [91], vitiligo and other pigmentary alterations of the skin [92], porphyria cutanea tarda (PCT) [93], granuloma anulare [94], pityriasis rubra pilaris [95], pemphigus vulgaris and many other autoimmune reactions [96] have been reported, but a clear association between the pathogenesis of each of these disorders and the retrovirus has not yet been established.
In the case of PCT, the presence of this disorder in HIV-1/AIDS patients is thought to be secondary to a defect in the hepatic cytochrome oxidase system [97]. This impairment could lead to an aberration in porphyrin metabolism and subsequently cause porphyria [97]. Predisposing factors for the development of PCT in HIV-1/AIDS patients are co-infection with hepatitis C, alcohol abuse and hepatotoxic drug consumption [93]. Major precautions have to be taken by caregivers of these individuals as HIV-1 virions have been isolated from blister fluid of PCT/HIV-1 patients [98].
Cutaneous drug reactions (CDRs) are often reported in AIDS patients as directly related to HIV-1 infection [99]. CDRs include a wide spectrum of disorders that range from mild morbilliform reactions (~70%) to Stevens-Johnson syndrome/toxic epidermal necrolysis (7.3%) [99]. Their direct connection with HIV-1 is based on two major changes associated with the infection: the induction of defective metabolic pathways; and the modification in the immune function. HIV-1 infection induces the production of interferons [99]. Subsequently, interferons increase the production of xanthine oxidase, a superoxide that destroys the hepatic cytochrome, P-450. Modifications on this drug-metabolizing system enhance the toxic potential of many drugs [100]. Moreover, CDRs may also be stimulated by the T cell imbalance produced by HIV-1 depletion of CD4+ cells [99, 101].
Stevens-Johnson syndrome (SJS), a cell-mediated immune reaction, is more prevalent in HIV-1-positive individuals than in their seronegative counterparts [99]. SJS is commonly seen as the consequence of a multi-drug regimen that includes sulfa-drugs and antiretroviral agents (e.g., nevirapine) [101, 102]. Nevertheless, there are a number of case reports that support the concept of erythema multiforme as the presenting manifestation of HIV-1 seroconversion [103–105]. Yet there is not enough data to support a cause-effect relationship.
Small animal models for the study of HIV-1-related primary cutaneous complications
Due to the high costs of non-human primate research, transgenic rodent models represent the best approach to reproduce pathologies seen in HIV-1 infection. In the late 1990s, a couple of rodent models seemed to be promising tools to study the pathogenesis of HIV-1-associated complications. These models transgenically expressed the human marker, CD4 (hCD4), and the co-receptor, hCXCR4, or the chemokine receptor, hCCR5, respectively [106, 107]. As promising as they could be, numerous drawbacks were observed in these mice, which included a lack of CD4+ T cells binding to HIV-1 protein gp120, and subsequent lack of infectivity and replication in the target cells [108].
From that experience, some non-infectious transgenic murine models of HIV-1 with deleted gag and pol genes were created. These HIV-1 Tg mice developed pathologic conditions similar to their human counterparts with HIV-1 infection; including the development of skin disorders [109, 110]. Such lesions were reported as proliferative epidermal lesions accompanied by progressive ulceration of the epidermis, or described as benign lesions resembling papillomas, Kaposi's sarcoma-like lesions [14] or B cell lymphomas [111].
However, the data generated from these models evidenced several failures, including numerous post-entry blocks due to inefficient tat transactivation. The deficiency in Tat function was further correlated with its lack of interaction with a gene product encoded on human chromosome 12, named cyclin T [108]. Mice's cyclin T does not interact functionally with tat, a fact that makes it a non-functional viral promoter [112] and consequently an unreliable model.
In 2001, we developed an HIV-1 Tg rat that showed similar pathology to that expressed in HIV-1/AIDS patients, and that overcame some of the problems encountered in the Tg mouse [109].
Unlike mice carrying the same transgene, efficient viral gene expression occurred in lymph nodes, spleen, thymus and blood, suggesting a functional tat [109]. Additionally, the generation of an HIV-1 transgenic rat appears to be a much better model both from the standpoint of size and that rat-derived cells are permissive for post-entry steps in the HIV-1 replication cycle. As recently reported, the HIV-1 Tg rat developed skin lesions in about 30% of the littermates [10]. Histologically, these lesions exhibited epidermal hyperplasia and hyperkeratosis, with an intense lymphocytic infiltrate and epidermal necrosis. Additionally, while the Tg rat showed the same pattern of serum cytokines seen in HIV-1/AIDS patients with a shift from Th1 to Th2 cytokines [113], analysis of the lesional skin showed a mixed cytokine profile [10]. In fact, none of the HIV-1 Tg rodent models currently available resembles precisely the pathology observed in AIDS patients.
However, while the non-infectious HIV-1 rodent models did not reproduce similar skin pathology to that observed in AIDS patients, a recently reported humanized murine model might recapitulate the immunological phenomena seen in the skin of HIV-1-infected individuals. In this model, non-obese diabetic mice with severe combined immunodeficiency are implanted with human fethal thymic and liver organoids, followed by sub-lethal irradiation, and then transplanted with human CD34+ stem cells derived from fetal livers [114]. These chimeric humanized mice show infiltration of stem cell-derived leukocytes (T and B lymphocytes) in different organs, including the liver, lung, gastrointestinal tract and grafted human skin [115]. Lately, this model has become a valuable tool to evaluate intra-rectal HIV-1 primary infection and anti-retroviral drug efficacy [114, 116].
Moreover, there is another animal model that might be promising for the study of the pathogenesis of psoriasis and HERVs [117]. This mouse strain was originally reported to have a natural mutation known as flaky skin (fsn) mutation, localized in chromosome 17. This mutation induces a pathologic conditions that resembles psoriasiform dermatitis, accompanied by anaemia, hyper-IgE and anti-dsDNA autoantibodies similar to those detected in systemic lupus erythematosus [117]. The cause of this mutation is due to the insertion of an endogenous retrovirus (early transposon class) into intron 14 of the Tetratricopeptide repeat domain 7 gene. Further studies on this animal might confirm a definite role of HERVs in the pathogenesis of psoriasis.
Conclusions
The pathogenesis of most HIV-1-related complications is not completely understood due to the complexity of this novel virus and to the drawbacks associated with their reproduction in controlled settings. Skin disorders are not the exception; the high prevalence of cutaneous manifestations related to this disease encourages us to search for more reliable explanations of the pathogenesis of these disorders.
Secondary complications related to HIV-1 are becoming less prevalent as HAART is more widely available [29]. However, no change in prevalence is seen in the primary complications. Moreover, such disorders as acne, staphylococcal infections, and erythema nodosum are being seen more frequently as part of the immune reconstitution syndrome [4].
All of the primary dermatologic complications in HIV-1-infected patients are also seen in immunocompetent patients. Such conditions as atopic dermatitis, psoriasis, and seborrheic dermatitis are extremely common dermatologic problems expressed in the general population; however, the direct role of the virus in the pathogenesis of these manifestations is still to be discovered. Noteworthy, the use of infectious and non-infectious HIV-1 Tg rodent models has failed to reproduce immunological phenomena and similar morphological skin disorders observed in AIDS patients. Better animal models, which may include humanized rodents, might represent a more suitable approach for the study of the pathogenesis of HIV-1-related disorders and the development of more effective forms of treatment.
Consent
Written consent for publication was obtained from the patients or their relatives.
References
Zalla MJ, Su WP, Fransway AF: Dermatologic manifestations of human immunodeficiency virus infection. Mayo Clin Proc 1992, 67:1089–1108.
Munoz-Perez MA, Rodriguez-Pichardo A, Camacho F, Colmenero MA: Dermatological findings correlated with CD4 lymphocyte counts in a prospective 3 year study of 1161 patients with human immunodeficiency virus disease predominantly acquired through intravenous drug abuse. Br J Dermatol 1998, 139:33–39.
Bernstein WB, Little RF, Wilson WH, Yarchoan R: Acquired immunodeficiency syndrome-related malignancies in the era of highly active antiretroviral therapy. Int J Hematol 2006, 84:3–11.
Maurer TA: Dermatologic manifestations of HIV infection. Top HIV Med 2005, 13:149–154.
Uthayakumar S, Nandwani R, Drinkwater T, Nayagam AT, Darley CR: The prevalence of skin disease in HIV infection and its relationship to the degree of immunosuppression. Br J Dermatol 1997, 137:595–598.
Tschachler E, Bergstresser PR, Stingl G: HIV-related skin diseases. Lancet 1996, 348:659–663.
Amerio P, Verdolini R, Proietto G, Feliciani C, Toto P, Shivji G, Loconsole F, Cassano N, Amerio P, Vena G, Sauder DN: Role of Th2 cytokines, RANTES and eotaxin in AIDS-associated eosinophilic folliculitis. Acta Derm Venereol 2001, 81:92–95.
Perl A: Role of endogenous retroviruses in autoimmune diseases. Rheum Dis Clin North Am 2003, 29:123–143. vii
Yarwood JM, Leung DY, Schlievert PM: Evidence for the involvement of bacterial superantigens in psoriasis, atopic dermatitis, and Kawasaki syndrome. FEMS Microbiol Lett 2000, 192:1–7.
Cedeno-Laurent F, Bryant J, Fishelevich R, Jones OD, Deng A, Eng ML, Gaspari AA, Trujillo JR: Inflammatory papillomatous hyperplasia and epidermal necrosis in a transgenic rat for HIV-1. J Dermatol Sci 2009, 53:112–119.
Klotman PE, Rappaport J, Ray P, Kopp JB, Franks R, Bruggeman LA, Notkins AL: Transgenic models of HIV-1. AIDS 1995, 9:313–324.
Dickie P, Ramsdell F, Notkins AL, Venkatesan S: Spontaneous and inducible epidermal hyperplasia in transgenic mice expressing HIV-1 Nef. Virology 1993, 197:431–438.
Corallini A, Altavilla G, Pozzi L, Bignozzi F, Negrini M, Rimessi P, Gualandi F, Barbanti-Brodano G: Systemic expression of HIV-1 tat gene in transgenic mice induces endothelial proliferation and tumors of different histotypes. Cancer Res 1993, 53:5569–5575.
Vogel J, Hinrichs SH, Reynolds RK, Luciw PA, Jay G: The HIV tat gene induces dermal lesions resembling Kaposi's sarcoma in transgenic mice. Nature 1988, 335:606–611.
Langhoff E, Terwilliger EF, Bos HJ, Kalland KH, Poznansky MC, Bacon OM, Haseltine WA: Replication of human immunodeficiency virus type 1 in primary dendritic cell cultures. Proc Natl Acad Sci USA 1991, 88:7998–8002.
Tindall B, Cooper DA: Primary HIV infection: host responses and intervention strategies. AIDS 1991, 5:1–14.
Belsito DV, Sanchez MR, Baer RL, Valentine F, Thorbecke GJ: Reduced Langerhans' cell Ia antigen and ATPase activity in patients with the acquired immunodeficiency syndrome. N Engl J Med 1984, 310:1279–1282.
Tschachler E, Groh V, Popovic M, Mann DL, Konrad K, Safai B, Eron L, diMarzo Veronese F, Wolff K, Stingl G: Epidermal Langerhans cells--a target for HTLV-III/LAV infection. J Invest Dermatol 1987, 88:233–237.
Ward J, Davis Z, DeHart J, Zimmerman E, Bosque A, Brunetta E, Mavilio D, Planelles V, Barker E: HIV-1 Vpr triggers natural killer cell-mediated lysis of infected cells through activation of the ATR-mediated DNA damage response. PLoS Pathog 2009, 5:e1000613.
Mantegani P, Tambussi G, Galli L, Din CT, Lazzarin A, Fortis C: Perturbation of the natural killer cell compartment during primary human immunodeficiency virus 1 infection primarily involving the CD56 bright subset. Immunology 129:220–233.
Pope M, Betjes MG, Romani N, Hirmand H, Cameron PU, Hoffman L, Gezelter S, Schuler G, Steinman RM: Conjugates of dendritic cells and memory T lymphocytes from skin facilitate productive infection with HIV-1. Cell 1994, 78:389–398.
Gordin FM, Hartigan PM, Klimas NG, Zolla-Pazner SB, Simberkoff MS, Hamilton JD: Delayed-type hypersensitivity skin tests are an independent predictor of human immunodeficiency virus disease progression. Department of Veterans Affairs Cooperative Study Group. J Infect Dis 1994, 169:893–897.
Hira SK, Wadhawan D, Kamanga J, Kavindele D, Macuacua R, Patil PS, Ansary MA, Macher AM, Perine PL: Cutaneous manifestations of human immunodeficiency virus in Lusaka, Zambia. J Am Acad Dermatol 1988, 19:451–457.
Josephine M, Issac E, George A, Ngole M, Albert SE: Patterns of skin manifestations and their relationships with CD4 counts among HIV/AIDS patients in Cameroon. Int J Dermatol 2006, 45:280–284.
Kumarasamy N, Solomon S, Jayaker Paul SA, Venilla R, Amalraj RE: Spectrum of opportunistic infections among AIDS patients in Tamil Nadu, India. Int J STD AIDS 1995, 6:447–449.
Resneck JS Jr, Van Beek M, Furmanski L, Oyugi J, LeBoit PE, Katabira E, Kambugu F, Maurer T, Berger T, Pletcher MJ, Machtinger EL: Etiology of pruritic papular eruption with HIV infection in Uganda. JAMA 2004, 292:2614–2621.
Spira R, Mignard M, Doutre MS, Morlat P, Dabis F: Prevalence of cutaneous disorders in a population of HIV-infected patients. Southwestern France, 1996. Groupe d'Epidemiologie Clinique du SIDA en Aquitaine. Arch Dermatol 1998, 134:1208–1212.
Jing W, Ismail R: Mucocutaneous manifestations of HIV infection: a retrospective analysis of 145 cases in a Chinese population in Malaysia. Int J Dermatol 1999, 38:457–463.
Maurer T, Rodrigues LK, Ameli N, Phanuphak N, Gange SJ, DeHovitz J, French AL, Glesby M, Jordan C, Khalsa A, Hessol NA: The effect of highly active antiretroviral therapy on dermatologic disease in a longitudinal study of HIV type 1-infected women. Clin Infect Dis 2004, 38:579–584.
Mathes BM, Douglass MC: Seborrheic dermatitis in patients with acquired immunodeficiency syndrome. J Am Acad Dermatol 1985, 13:947–951.
Froschl M, Land HG, Landthaler M: Seborrheic dermatitis and atopic eczema in human immunodeficiency virus infection. Semin Dermatol 1990, 9:230–232.
Valia RG: Etiopathogenesis of seborrheic dermatitis. Indian J Dermatol Venereol Leprol 2006, 72:253–255.
Berger TG, Greene I: Bacterial, viral, fungal, and parasitic infections in HIV disease and AIDS. Dermatol Clin 1991, 9:465–492.
Wikler JR, Nieboer C, Willemze R: Quantitative skin cultures of Pityrosporum yeasts in patients seropositive for the human immunodeficiency virus with and without seborrheic dermatitis. J Am Acad Dermatol 1992, 27:37–39.
Bergbrant IM, Andersson B, Faergemann J: Cell-mediated immunity to Malassezia furfur in patients with seborrhoeic dermatitis and pityriasis versicolor. Clin Exp Dermatol 1999, 24:402–406.
Faergemann J, Bergbrant IM, Dohse M, Scott A, Westgate G: Seborrhoeic dermatitis and Pityrosporum (Malassezia) folliculitis: characterization of inflammatory cells and mediators in the skin by immunohistochemistry. Br J Dermatol 2001, 144:549–556.
Ackerman AB: Histopathologic differentiation of eczematous dermatitides from psoriasis and seborrheic dermatitis. Cutis 1977, 20:619–623.
Eisenstat BA, Wormser GP: Seborrheic dermatitis and butterfly rash in AIDS. N Engl J Med 1984, 311:189.
Puig L, Fernandez-Figueras MT, Ferrandiz C, Ribera M, de Moragas JM: Epidermal expression of 65 and 72 kd heat shock proteins in psoriasis and AIDS-associated psoriasiform dermatitis. J Am Acad Dermatol 1995, 33:985–989.
Ippolito F, Passi S, Di Carlo A: Is seborrhoeic dermatitis a clinical marker of HIV disease? Minerva Ginecol 2000, 52:54–58.
Coldiron BM, Bergstresser PR: Prevalence and clinical spectrum of skin disease in patients infected with human immunodeficiency virus. Arch Dermatol 1989, 125:357–361.
Singh F, Rudikoff D: HIV-associated pruritus: etiology and management. Am J Clin Dermatol 2003, 4:177–188.
Lin RY, Lazarus TS: Asthma and related atopic disorders in outpatients attending an urban HIV clinic. Ann Allergy Asthma Immunol 1995, 74:510–515.
Yoshioka M, Bradley WG, Shapshak P, Nagano I, Stewart RV, Xin KQ, Srivastava AK, Nakamura S: Role of immune activation and cytokine expression in HIV-1-associated neurologic diseases. Adv Neuroimmunol 1995, 5:335–358.
Rowe A, Mallon E, Rosenberger P, Barrett M, Walsh J, Bunker CB: Depletion of cutaneous peptidergic innervation in HIV-associated xerosis. J Invest Dermatol 1999, 112:284–289.
Gelfand JM, Rudikoff D: Evaluation and treatment of itching in HIV-infected patients. Mt Sinai J Med 2001, 68:298–308.
Scott GB, Buck BE, Leterman JG, Bloom FL, Parks WP: Acquired immunodeficiency syndrome in infants. N Engl J Med 1984, 310:76–81.
Ong PY, Leung DY: Immune dysregulation in atopic dermatitis. Curr Allergy Asthma Rep 2006, 6:384–389.
Majors MJ, Berger TG, Blauvelt A, Smith KJ, Turner ML, Cruz PD Jr: HIV-related eosinophilic folliculitis: a panel discussion. Semin Cutan Med Surg 1997, 16:219–223.
Anand P, Springall DR, Blank MA, Sellu D, Polak JM, Bloom SR: Neuropeptides in skin disease: increased VIP in eczema and psoriasis but not axillary hyperhidrosis. Br J Dermatol 1991, 124:547–549.
Jappe U: Superantigens and their association with dermatological inflammatory diseases: facts and hypotheses. Acta Derm Venereol 2000, 80:321–328.
Leung DY: Atopic dermatitis and the immune system: the role of superantigens and bacteria. J Am Acad Dermatol 2001, 45:S13–16.
Lin RY: Chronic diffuse dermatitis and hyper-IgE in HIV infection. Acta Derm Venereol 1988, 68:486–491.
Duvic M, Johnson TM, Rapini RP, Freese T, Brewton G, Rios A: Acquired immunodeficiency syndrome-associated psoriasis and Reiter's syndrome. Arch Dermatol 1987, 123:1622–1632.
Schon MP, Boehncke WH: Psoriasis. N Engl J Med 2005, 352:1899–1912.
Namazi MR: Paradoxical exacerbation of psoriasis in AIDS: proposed explanations including the potential roles of substance P and gram-negative bacteria. Autoimmunity 2004, 37:67–71.
Johnson TM, Duvic M, Rapini RP, Rios A: AIDS exacerbates psoriasis. N Engl J Med 1985, 313:1415.
Dover JS, Johnson RA: Cutaneous manifestations of human immunodeficiency virus infection. Part II. Arch Dermatol 1991, 127:1549–1558.
Arnett FC, Reveille JD, Duvic M: Psoriasis and psoriatic arthritis associated with human immunodeficiency virus infection. Rheum Dis Clin North Am 1991, 17:59–78.
Bartke U, Venten I, Kreuter A, Gubbay S, Altmeyer P, Brockmeyer NH: Human immunodeficiency virus-associated psoriasis and psoriatic arthritis treated with infliximab. Br J Dermatol 2004, 150:784–786.
Duvic M: Immunology of AIDS related to psoriasis. J Invest Dermatol 1990, 95:38S-40S.
Mallon E, Bunker CB: HIV-associated psoriasis. AIDS Patient Care STDS 2000, 14:239–246.
Obuch ML, Maurer TA, Becker B, Berger TG: Psoriasis and human immunodeficiency virus infection. J Am Acad Dermatol 1992, 27:667–673.
Mallon E, Young D, Bunce M, Gotch FM, Easterbrook PJ, Newson R, Bunker CB: HLA-Cw*0602 and HIV-associated psoriasis. Br J Dermatol 1998, 139:527–533.
Morar N, Dlova N, Gupta AK, Naidoo DK, Aboobaker J, Ramdial PK: Erythroderma: a comparison between HIV positive and negative patients. Int J Dermatol 1999, 38:895–900.
Mallon E: Retroviruses and psoriasis. Curr Opin Infect Dis 2000, 13:103–107.
Townsend BL, Cohen PR, Duvic M: Zidovudine for the treatment of HIV-negative patients with psoriasis: a pilot study. J Am Acad Dermatol 1995, 32:994–999.
Fischer T, Schworer H, Vente C, Reich K, Ramadori G: Clinical improvement of HIV-associated psoriasis parallels a reduction of HIV viral load induced by effective antiretroviral therapy. AIDS 1999, 13:628–629.
Moles JP, Tesniere A, Guilhou JJ: A new endogenous retroviral sequence is expressed in skin of patients with psoriasis. Br J Dermatol 2005, 153:83–89.
Rebora A: Human endogenous retroviruses and their possible impact on dermatology. J Am Acad Dermatol 2005, 52:E7.
Kazazian HH Jr: Genetics. L1 retrotransposons shape the mammalian genome. Science 2000, 289:1152–1153.
Krieg AM, Gourley MF, Perl A: Endogenous retroviruses: potential etiologic agents in autoimmunity. Faseb J 1992, 6:2537–2544.
Griffiths DJ, Cooke SP, Herve C, Rigby SP, Mallon E, Hajeer A, Lock M, Emery V, Taylor P, Pantelidis P, Bunker CB, du Bois R, Weiss RA, Venables PJ: Detection of human retrovirus 5 in patients with arthritis and systemic lupus erythematosus. Arthritis Rheum 1999, 42:448–454.
Krieg AM, Gourley MF, Klinman DM, Perl A, Steinberg AD: Heterogeneous expression and coordinate regulation of endogenous retroviral sequences in human peripheral blood mononuclear cells. AIDS Res Hum Retroviruses 1992, 8:1991–1998.
Hohenadl C, Germaier H, Walchner M, Hagenhofer M, Herrmann M, Sturzl M, Kind P, Hehlmann R, Erfle V, Leib-Mosch C: Transcriptional activation of endogenous retroviral sequences in human epidermal keratinocytes by UVB irradiation. J Invest Dermatol 1999, 113:587–594.
Leib-Mosch C, Bachmann M, Brack-Werner R, Werner T, Erfle V, Hehlmann R: Expression and biological significance of human endogenous retroviral sequences. Leukemia 1992,6(Suppl 3):72S-75S.
Dalen AB, Hellgren L, Iversen OJ, Vincent J: A virus-like particle associated with psoriasis. Acta Pathol Microbiol Immunol Scand [B] 1983, 91:221–229.
Iversen OJ, Nissen-Meyer J, Dalen AB: Characterization of virus-like particles from a psoriatic patient with respect to the possible presence of particle-associated RNA and RNA-directed DNA polymerase. Acta Pathol Microbiol Immunol Scand [B] 1983, 91:413–417.
Iversen OJ, Dalen AB: The major internal protein, p27, of a retrovirus-like particle is expressed in blood lymphocytes from psoriatic patients. Arch Virol 1985, 85:197–207.
Moles JP, Hadi JC, Guilhou JJ: High prevalence of an IgG response against murine leukemia virus (MLV) in patients with psoriasis. Virus Res 2003, 94:97–101.
Oldstone MB: Molecular mimicry and autoimmune disease. Cell 1987, 50:819–820.
Soeprono FF, Schinella RA: Eosinophilic pustular folliculitis in patients with acquired immunodeficiency syndrome. Report of three cases. J Am Acad Dermatol 1986, 14:1020–1022.
Colton AS, Schachner L, Kowalczyk AP: Eosinophilic pustular folliculitis. J Am Acad Dermatol 1986, 14:469–474.
McCalmont TH, Altemus D, Maurer T, Berger TG: Eosinophilic folliculitis. The histologic spectrum. Am J Dermatopathol 1995, 17:439–446.
Rajendran PM, Dolev JC, Heaphy MR Jr, Maurer T: Eosinophilic folliculitis: before and after the introduction of antiretroviral therapy. Arch Dermatol 2005, 141:1227–1231.
Brenner S, Wolf R, Ophir J: Eosinophilic pustular folliculitis: a sterile folliculitis of unknown cause? J Am Acad Dermatol 1994, 31:210–212.
Fearfield LA, Rowe A, Francis N, Bunker CB, Staughton RC: Itchy folliculitis and human immunodeficiency virus infection: clinicopathological and immunological features, pathogenesis and treatment. Br J Dermatol 1999, 141:3–11.
Magro CM, Crowson AN: Necrotizing eosinophilic folliculitis as a manifestation of the atopic diathesis. Int J Dermatol 2000, 39:672–677.
Rosenthal D, LeBoit PE, Klumpp L, Berger TG: Human immunodeficiency virus-associated eosinophilic folliculitis. A unique dermatosis associated with advanced human immunodeficiency virus infection. Arch Dermatol 1991, 127:206–209.
French MA, Price P, Stone SF: Immune restoration disease after antiretroviral therapy. AIDS 2004, 18:1615–1627.
Smith KJ, Skelton HG, Tuur S, Yeager J, Decker C, Wagner KF: Increased cutaneous toxicity to ionizing radiation in HIV-positive patients. Military Medical Consortium for the Advancement of Retroviral Research (MMCARR). Int J Dermatol 1997, 36:779–782.
Antony FC, Marsden RA: Vitiligo in association with human immunodeficiency virus infection. J Eur Acad Dermatol Venereol 2003, 17:456–458.
Drobacheff C, Derancourt C, Van Landuyt H, Devred D, de Wazieres B, Cribier B, Rey D, Lang JM, Grosieux C, Kalis B, Laurent R: Porphyria cutanea tarda associated with human immunodeficiency virus infection. Eur J Dermatol 1998, 8:492–496.
Toro JR, Chu P, Yen TS, LeBoit PE: Granuloma annulare and human immunodeficiency virus infection. Arch Dermatol 1999, 135:1341–1346.
Bonomo RA, Korman N, Nagashima-Whalen L, Briggs J, Graham R, Salata RA: Pityriasis rubra pilaris: an unusual cutaneous complication of AIDS. Am J Med Sci 1997, 314:118–121.
Bull RH, Fallowfield ME, Marsden RA: Autoimmune blistering diseases associated with HIV infection. Clin Exp Dermatol 1994, 19:47–50.
Almehmi A, Deliri H, Szego GG, Teague AC, Pfister AK, Martin SA: Porphyria cutanea tarda in a patient with HIV-infection. W V Med J 2005, 101:19–21.
O'Connor WJ: Porphyria cutanea tarda and HIV: two cases associated with hepatitis C. AIDS Patient Care STDS 1998, 12:341–346.
Todd G: Adverse cutaneous drug eruptions and HIV: a clinician's global perspective. Dermatol Clin 2006, 24:459–472. vi
Mannering GJ, Deloria LB, Abbott V: Role of xanthine oxidase in the interferon-mediated depression of the hepatic cytochrome P-450 system in mice. Cancer Res 1988, 48:2107–2112.
Lehmann DF, Liu A, Newman N, Blair DC: The association of opportunistic infections with the occurrence of trimethoprim/sulfamethoxazole hypersensitivity in patients infected with human immunodeficiency virus. J Clin Pharmacol 1999, 39:533–537.
Rotunda A, Hirsch RJ, Scheinfeld N, Weinberg JM: Severe cutaneous reactions associated with the use of human immunodeficiency virus medications. Acta Derm Venereol 2003, 83:1–9.
Lewis DA, Brook MG: Erythema multiforme as a presentation of human immunodeficiency virus seroconversion illness. Int J STD AIDS 1992, 3:56–57.
Mortier E, Zahar JR, Gros I, Vignali JP, Simonpoli AM, Pouchot J, Vinceneux P: Primary infection with human immunodeficiency virus that presented as Stevens-Johnson syndrome. Clin Infect Dis 1994, 19:798.
Schechner AJ, Pinson AG: Acute human immunodeficiency virus infection presenting with erythema multiforme. Am J Emerg Med 2004, 22:330–331.
Sawada S, Gowrishankar K, Kitamura R, Suzuki M, Suzuki G, Tahara S, Koito A: Disturbed CD4+ T cell homeostasis and in vitro HIV-1 susceptibility in transgenic mice expressing T cell line-tropic HIV-1 receptors. J Exp Med 1998, 187:1439–1449.
Keppler OT, Welte FJ, Ngo TA, Chin PS, Patton KS, Tsou CL, Abbey NW, Sharkey ME, Grant RM, You Y, Scarborough JD, Ellmeier W, Littman DR, Stevenson M, Charo IF, Herndier BG, Speck RF, Goldsmith MA: Progress toward a human CD4/CCR5 transgenic rat model for de novo infection by human immunodeficiency virus type 1. J Exp Med 2002, 195:719–736.
van Maanen M, Sutton RE: Rodent models for HIV-1 infection and disease. Curr HIV Res 2003, 1:121–130.
Reid W, Sadowska M, Denaro F, Rao S, Foulke J Jr, Hayes N, Jones O, Doodnauth D, Davis H, Sill A, O'Driscoll P, Huso D, Fouts T, Lewis G, Hill M, Kamin-Lewis R, Wei C, Ray P, Gallo RC, Reitz M, Bryant J: An HIV-1 transgenic rat that develops HIV-related pathology and immunologic dysfunction. Proc Natl Acad Sci USA 2001, 98:9271–9276.
Kopp JB, Rooney JF, Wohlenberg C, Dorfman N, Marinos NJ, Bryant JL, Katz SI, Notkins AL, Klotman PE: Cutaneous disorders and viral gene expression in HIV-1 transgenic mice. AIDS Res Hum Retroviruses 1993, 9:267–275.
Vellutini C, Horschowski N, Philippon V, Gambarelli D, Nave KA, Filippi P: Development of lymphoid hyperplasia in transgenic mice expressing the HIV tat gene. AIDS Res Hum Retroviruses 1995, 11:21–29.
Wei P, Garber ME, Fang SM, Fischer WH, Jones KA: A novel CDK9-associated C-type cyclin interacts directly with HIV-1 Tat and mediates its high-affinity, loop-specific binding to TAR RNA. Cell 1998, 92:451–462.
Reid W, Abdelwahab S, Sadowska M, Huso D, Neal A, Ahearn A, Bryant J, Gallo RC, Lewis GK, Reitz M: HIV-1 transgenic rats develop T cell abnormalities. Virology 2004, 321:111–119.
Sun Z, Denton PW, Estes JD, Othieno FA, Wei BL, Wege AK, Melkus MW, Padgett-Thomas A, Zupancic M, Haase AT, Garcia JV: Intrarectal transmission, systemic infection, and CD4+ T cell depletion in humanized mice infected with HIV-1. J Exp Med 2007, 204:705–714.
Delhem N, Hadida F, Gorochov G, Carpentier F, de Cavel JP, Andreani JF, Autran B, Cesbron JY: Primary Th1 cell immunization against HIVgp160 in SCID-hu mice coengrafted with peripheral blood lymphocytes and skin. J Immunol 1998, 161:2060–2069.
Stoddart CA, Bales CA, Bare JC, Chkhenkeli G, Galkina SA, Kinkade AN, Moreno ME, Rivera JM, Ronquillo RE, Sloan B, Black PL: Validation of the SCID-hu Thy/Liv mouse model with four classes of licensed antiretrovirals. PLoS One 2007, 2:e655.
Helms C, Pelsue S, Cao L, Lamb E, Loffredo B, Taillon-Miller P, Herrin B, Burzenski LM, Gott B, Lyons BL, Keppler D, Shultz LD, Bowcock AM: The Tetratricopeptide repeat domain 7 gene is mutated in flaky skin mice: a model for psoriasis, autoimmunity, and anemia. Exp Biol Med (Maywood) 2005, 230:659–667.
Acknowledgements
We thank Dr Catherine S. Wade for her insightful comments. Dr Trujillo is supported by NIH RO1 supplement A01A06048-1-01A2.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
All authors declare that they have no competing interests.
Authors' contributions
FCL drafted the manuscript and conceived the outline. MGF, NM and JAR provided patient samples, photographs, helped to draft the manuscript and gave insightful comments. AAG helped to draft the manuscript and participated in its design coordination. JRT conceived the outline, helped draft the manuscript and coordinated its design. All authors read and approved the final manuscript.
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License ( https://creativecommons.org/licenses/by-nc/2.0 ), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Cedeno-Laurent, F., Gómez-Flores, M., Mendez, N. et al. New insights into HIV-1-primary skin disorders. JIAS 14, 5 (2011). https://doi.org/10.1186/1758-2652-14-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1758-2652-14-5