
Abstract
Background
To unfold specific-mutational patterns in TP53 gene due to exposures to war environmental hazards and to detect the association of TP53 gene alteration with the depth of bladder cancer.
Methods
Twenty-nine bladder carcinomas were analyzed for TP53 alterations. PCR-single strand conformational polymorphism analysis, DNA sequencing and immunohistochemical analysis using monoclonal mouse anti-human p53 antibody (Clone DO-7) were employed.
Results
TP53 gene mutations occurred in 37.9% of the cases while TP53 overexpression occurred in 58.6%. Both of them were associated with deep invasive-tumors. Single mutations were seen in 63.6%, whereas only 27.3% have shown double mutations. Four mutations were frameshifted (30.8%); two of them showed insertion A after codon 244. There was no significant association between TP53 mutations and protein overexpression (P>0.05), while a significant association was observed between TP53 alterations and tumors progression (P ≤ 0.01).
Conclusion
The infrequent TP53mutations, especially insertion A and 196 hotspot codon, may represent the specific-mutational patterns in bladder carcinoma among the Iraqi patients who were exposed to war environmental hazards. TP53 alteration associated with bladder cancer progression should be analyzed by both mutational and protein expression analysis.
Similar content being viewed by others


Background
Bladder cancer (BC) is the most common malignancy affecting urinary system comprising the seventh most common cancer worldwide with male predominance [1, 2]. In Iraq, the incidence of bladder cancer is the fourth most common type of cancer (in men and eighth most common in women) [3]. The most common type of bladder cancer is transitional cell carcinoma (TCC) accounting for more than 90% of the cases [2]. It represents one of the first tumors that have been associated with environmental risk factors that produce genetic alterations [4, 5].
TP53 gene “the guardian of genome” is the most frequently mutated tumor suppressor gene identified in human cancer. TP53 inactivation led to diminished control cell cycle check points, decreased DNA repair, and increased genomic instability [6–8] . Furthermore, TP53 inactivation has been identified in tumor progression, metastasis, and aggressive phenotype of bladder cancer giving rise to what has been considered as a useful genetic biomarker to predict progression associated with bad prognosis [9–11]. The frequency and the type of mutations vary from one tumor type to another, ranging from 5% to 80% depending on the type, stage and etiology of tumor [12]. Almost all TP53 mutations are point missense mutations leading to a functionally defective protein [13]. Approximately 90% of them are localized in DNA-binding domains encoded by exons 5–8. In total, about 40% of them are localized at the "hotspot" residues R 175, G 245, R 248, R 249, R 273 and R 282 [14]. Indeed, there are considerable numbers of studies on TP53 gene being as a target for carcinogens, with a specific TP53 mutations spectrum, mainly G: C→A: T transitions at CpG and non-CpG sites in bladder cancer [7, 15, 16]. It is well documented that the spectrum of TP53mutations in bladder cancer differs from that of lung cancer, even though cigarette smoking is probably a contributing cause in over one-third of all bladder cancer cases [17]. Specifically, G→T transversions at CpG are relatively uncommon (about 8% in bladder cancer versus 27% in lung cancer) whereas CpG G: C→A: T transition are as twice as common with regard to mutation patterns (22% for bladder cancer versus 11% for lung cancer) [7].
Inactivation of tumor suppresser genes can occur either primarily through mutations, or without any change in the structure of the given genes. Thus, tumor suppressor function should be analyzed at the level of the genes as well as at the level of proteins, and in the context of the pathways in which these genes are involved [18, 19]. The mutated p53 protein has a longer half-life, as compared with normal p53 protein, which can be detected by Immunohistochemistry (IHC) as a surrogate marker for mutation [20]. Immunohistochemical positivity for TP53protein is in general thought to reflect point mutations of TP53 gene in tumor, although it is not always synonymous with TP53 mutation [21]. Accordingly, using both molecular and protein analyses (PCR-based genetic technique and immunohistochemistry respectively) for detection of TP53 alterations have rational efficacy for mutation detection rather than each one alone [20, 22, 23]. The aims of this research were to determine if any specific-mutational pattern in TP53gene may play a possible role in bladder tumorogenesis, which might be resulted from the exposure to the hazardous pollution of the wars in Iraq. An analysis of the alteration of TP53gene using combined PCR-based genetic and IHC analysis to evaluate its association with bladder cancer progression was conducted.
Methods
Ethical approval was obtained from the local medical ethics committee, Faculty of Medicine, University of Kufa. A written informed consent was received from all subjects before proceeding any further. The study was designed and conducted in accordance with the tents of Declaration of Helsinki.
A total of twenty-nine patients (25 males and 4 females) with transitional cell carcinoma (TCC), diagnosed by transurethral resection (TUR-biopsy) at the Department of Pathology of Kufa School of Medicine Teaching Hospital were subjected to the present study. The patients were randomly selected from the Middle Euphrates area and south of Iraq. Both regions were potentially exposed to environmental pollution during the last two decades of wars. The patients ages ranged between 35 and 85 years, with a median age of 69.3 years. Histological examination, grading [24] and staging [25] were performed by two of us independently. Three were classified as grade I, two as grade II, and fifteen classified as grade III. Fourteen cases were superficial TCC [5 as Ta and 9 as T1], while 15 cases were deep invasive TCC (T2). Sixteen of our patients had a history of cigarette smoking for at least 10 years.
TP53 status
TP53 protein expression
TP53 protein expression was estimated using immunohistochemical techniques [26–28]. Five micron thick sections of formalin-fixed paraffin-embedded tissue (FFPE) were placed on positively charged slides (Fisher scientific Co., Pittsburgh, PA). These sections were then deparaffinized and rehydrated. For staining enhancement, the sections were pre-treated with antigen retrieval solution (0.01 M, citrate buffer, pH6.0, Dako Cytomation/Denmark) in water-bath at 95°C for 40 minutes followed by staining with a monoclonal mouse anti-human TP53 antibody (Clone DO-7, Ready-to-use, DakoCytomation/Denmark). The antigen-antibody complex was visualized using Labeled Streptavidin-Biotin 2 System-Horseradish Peroxidase staining technique (LAB/LSAB2 System-HRP, DakoCytomation/Denmark). The sections were then counterstained with Meyer's haematoxylin.
A breast cancer with high TP53expression detected by immunohistochemical analysis was used as positive external control. Negative controls were obtained by omission of the primary antibody and by a breast cancer with negative TP53 expression detected by immunohistochemical analysis. The non-epithelial cells of samples (lymphocytes, stromal cells and endothelial cells) were used as negative internal control.
All slides were reviewed independently by two investigators without previous knowledge of tumor grade and stage or TP53mutation. TP53 expression (nuclear staining) was evaluated by counting 100 cells/section in five randomly chosen high-power fields (40x) by light microscope. The extent of nuclear reactivity was classified in four categories [9, 20]; no nuclear reactivity (−), few focally positive cells (1 to 10% tumor cells) (+/−), heterogeneous nuclear reactivity (10 to 50% tumor cells) (+) and homogenous intense nuclear reactivity (50 to 100% tumor cells) (++). The samples which demonstrated at least 10% nuclear reactivity were considered to be TP53-positive (have an alteration in TP53) [9, 10, 19, 20].
TP53 mutation
DNA extraction
High-molecular weight DNA was prepared from the fresh tumor specimens by phenol-chloroform-isoamyl alcohol method [20, 29]. DNA which was extracted from whole blood samples of healthy looking individuals was included as normal control with their matched age and sex with Wizard ® Genomic DNA purification kit (Promega Company/USA).
PCR-SSCP and DNA sequencing
The mutational analysis was achieved using PCR-single strand conformation polymorphism (PCR-SSCP) and direct DNA sequencing methods for TP53 gene exons 5–8. Each exon 5–8 was amplified by PCR. The primer sequences used were as follows [15]: (1) exon 5/228 bp, forward: 5′-TTCAACTCTGTCTCCTTCCT-3′ and reverse: 5′–CAGCCCTGTCGTCTCTCCAG-3′; (2) exon 6/159 bp, forward: 5′– GCCTCTGATTCCTCATCGAT-3′ and reverse:5′–TTAACCCCTCCTCCCAGAGA-3′; (3) exon 7/157 bp, forward:5′-AGGCGCACTGGCCTCATCTT-3′ and reverse:5′-TGTGCAGGG TGG CAAGTGGC-3′; and (4) exon 8/214 bp, forward:5′– TTCCTTACTGCCTCTTGCTT-3′and reverse: 5′–AGGCATAACTGCAC CCTTGG-3′. Each PCR reaction was performed in a final volume of 25 μl containing 100 ng DNA, 1X PCR buffer, 1.5 mM MgCL2, 200 μM each dNTP, 0.1 μM of each upstream and downstream primer, and 1.5u of Taq polymerase (CinnaGen Company/Iran). PCR was carried out under the following conditions: an initial denaturation step (95°C for 5 minutes) was followed by 35 cycles consisting of (for exon 5) denaturation at 95°C for 50 seconds, primer annealing at 55°C for 35 seconds and extension at 72°C for 30 seconds; (for exons 6–7) denaturation at 95°C for 50 seconds, primer annealing at 63°C for 25 seconds and extension at 72°C for 15 seconds; or was followed by 30 cycles (for exons 8) consisting of denaturation at 95°C for 50 seconds, primer annealing at 65°C for 25 seconds and extension at 72°C for 15 seconds. The final extension was continued for 10 minutes at 72°C. The PCR products were analyzed on 1.5-2% agarose gel to determine the specific band of each exon product and then analyzed on 12% polyacrylamide gel to another evaluation of specific band purity to ensure the absence of any unwanted products (non-specific bands) which may interfere with SSCP and DNA sequencing analysis.
For non-radioactive SSCP analysis, the SSCP analysis was carried out according to the method of Liechti-Gallati et al., (1999) [30], for both of the tumor and the control samples.
The to controls were analyzed. PCR products were denaturated at 96°C for 10 min at 3:2 dilution of formamide loading dye (SSCP denaturing solution) containing 95% formamide, 100 mM NaOH, 0.25% bromophenol blue, 0.25% xylene cyanol and thereafter placed immediately on ice to prevent re-annealing of the single-stranded product. The denaturized samples, the controls and the normal PCR product of controls were loaded quickly into wells of the 12% polyacrylamide gel and run at 4–10°C/80 V for overnight. The gel was stained with Sliver Staining and alterations of bands relative
All the samples that revealed mobility shift in their migration during SSCP screening mutation analysis were sent to the direct DNA sequencing in both directions: forward sequencing 5′→3′and reverse sequencing 3′→5′using the same primer sequences and dideoxy chain termination method. The DNA sequencing was achieved by Gen Fanavaran Company/Iran. The DNA sequencing chromatogram was interpreted using Chromagen 2.3 version software that allows comparison of a newly generated sequence of DNA sample with free DNA sequence. Viewers (available from National Center for Biotechnology Information (NCBI) website) were used as reference sequence of gene of interest for comparison.
Statistical analysis
The Fisher’s exact probability test and Odds ratios (ORs), using contingency tables, were applied to analyze the data using the program statistical package for the Social Science (SPSS for windows, version 10.0). The relationships between the variables were assessed using non-parametric Fisher’s exact probability test. A P-value ≤0.05 was considered as statistically significant at a level of 5%. The strength of the associations between the variables was measured by calculating Odds ratios (ORs) and confidence intervals (95% CI). Possible categories for OR are greater than 1and less than 1. A value greater than 1 indicates positive association and a value less than 1 indicates negative association.
Results
Mutational analysis of the TP53 gene in relation to clinicopathological features
Characteristic of TP53 gene mutation
The PCR-SSCP analysis showed that 12 out of 29 cases of bladder cancer patients had aberrantly migrating bands or extra bands that were further analyzed by DNA sequencing to represent the mutations of TP53 gene (Figure 1). All controls used in this study revealed normal migration of SSCP bands and normal sequencing of all studied exons (Figure 1a,c,e).

Example of PCR-SSCP/HD and DNA sequencing analysis of p53 gene in transitional cell carcinoma. (a) PCR-SSCP/HD analysis of exon 5 shows extra bands and bands with mobility shift indicated by arrows (−ve: undenaturated DNA control; +ve: denaturated DNA control, and T: tumors). DNA sequencing reveals transition CGC → CAC at codon 175 in exon 5 (b) and insertion A after codon 244 (GGC) in exon in exon 7 (d) in compared to wild types (c) and (e) respectively (arrows).
The sequencing results confirmed that 10 cases harbored one or more TP53 mutations within identical or separated samples, one case had silent mutation and one case had bad sequencing. Eleven (37.9%) cases were classified as TP53-positive [10 cases with detected mutation and 1 case without DNA sequencing] and 18 (62.1%) cases as p53-negative [17 cases without detected mutation and 1 case with silent mutation: case 5, codon 244; GGC (Gly) to GGA (Gly)] (Table 1).
Among TP53-positive cases; seven patients (63.6%) showed single mutation, three patients (27.3%) had double mutations and one patient (9.1%) with mutation detected only by SSCP analysis. A total of 13 mutations determined in ten cases; 9 mutations (69.2%) were single-base pair substitutions and 4 mutations (30.8%) were with frameshift mutations.
The patterns of TP53 base-pair mutations showed that five mutations (38.4%) were of transitions including G: C → A: T, three of them (23.8%) occurred at CpG dinucleotide in the codons (175 and 196) that were reported as hotspot for TP53 mutations. The other two (15.4%) mutations occurred at non-CpG sites. The four (30.8%) transversions detected were two (15.4%) G → C, one (7.7%) T → G, and one (7.7%) C → A. Two of the base-pair substitutions were silent mutations found in double mutations [case 12, codon 154; GGC (Gly) to GGA (Gly) and case 25, codon 294; GAG (Glu) to GAA (Glu)], and seven were missense resulted in amino acid changes.
Of the observed frameshift mutations (30.8%) three (23.1%) were in the exon7 [two (15.4%) with insertion A after the codon 244 (GGC/Gly) and one (7.7%) with deletion A at the codon 230(ACC/Thr)]. The remaining one was deletion G (7.7%) at codon 293 (GGG/Gly) in exon 8. The double mutations were found in case 12 in exon 5 [codon 154; Gly → Gly (silent)] and in exon 6 [codon 192; Glu → His (missense)], case 20 in exon 6 [codon 196; Arg → Glu (missense)] and exon 8 [codon 283; Arg → pro (missense)], and case 25 in exon 8 [codon 293, del G and codon 294, Glu → Glu (silent)] (Table 1) (Figure 1b and d). The TP53 mutations were higher in deep invasive-tumors (high grade and stage T2) (40%) than in superficially invasive tumors (low grade and stage Ta-T1) (35.7%) (OR, 1.2; CI, 0.26-5.4) (Table 2).
Immunhistochemical analysis of TP53 gene in relation to clinicopathological features
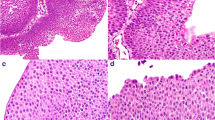
Immunohistochemical analysis showed that TP53 immunoreactivty was restricted to the nuclei of tumor cells. Four patterns of immunohistochemical nuclear staining was observed (Figure 2) including: no detectable immunoreactivty (−) in 20.7% (Figure 2,a), few focal reactivity in less than 10% of tumor cells (+/−) in 20.7% (Figure 2,b), heterogeneous nuclear reactivity in 10 -50% of tumor cells (+) in 10.3% (Figure 2,c), and intense homogenous nuclear reactivity was greater than 50% of tumor cells (++) in 48.3% (Figure 2,d). The level of TP53 nuclear reactivity was classified into two categories: wild-type TP53including score (−) and (+/−), and altered TP53 includes score (+) and (++). While, negative internal control of samples (non-epithelial cells) showed absence of TP53 nuclear staining that was consistent with wild-type expression of TP53 gene (Figure 2, D). The TP53 overexpression was identified in 17 cases (58.6%) out of 29 TCC cases. The altered expression of TP53 was more frequent in high grade tumor than low grade (66.7% vs. 28.6% respectively) and in T2 stage than Ta and T1 (66.7% vs. 28.6% respectively), giving rise to a statistically significant difference (p ≤ 0.05) (Table 2).

Immunohistochemical detection of p53 nuclear reactivity in transitional cell carcinoma (a) Invasive transitional cell carcinoma, poorly differentiated (Grade III) showing no detectible nuclear p53 immunostaining (Score (−), (10X)). (b) Papillary transitional cell carcinoma, well differentiated (Grade I) showing a few p53 immunoreactivty of tumor nuclei (Score (+/−), arrowed, (10X and 40X)). (c) Invasive transitional cell carcinoma, poorly differentiated (Grade II) showing heterogeneous p53 nuclear immunostaining (Score (+); arrowed,(40X)). (d) Papillary transitional cell carcinoma, well differentiated (Grade I) showing homogenous intense p53 nuclear immunostaining (Score (++); yellow arrow, (10X and 40X), (Red arrow indicates surrounding stromal and infiltrative lymphocytes with no detectible nuclear p53 immunostaining)).
Correlation of p53 mutation with nuclear reactivity
The present data shows no significant association between TP53 mutations and the immunohistochemical detection of TP53 protein (p>0.05) (Table 3). Seven tumors which had TP53 mutation [six of them with point mutation (missense), and one case with SSCP mobility shift] were positive for TP53protein overexpression. Four tumor cases with frameshift mutations of TP53had no detectable TP53 nuclear accumulation. Ten tumor cases without detected mutation had TP53overexpression. Accordingly, the TP53 alteration (TP53 status) defined by either presence of mutations or TP53 immunoreactivty, or both was demonstrated (Table 1) [23]. Our data showed that the TP53 alteration (TP53 status) was strongly associated with high grade and stage (p≤ 0.01) (Table 2).
Discussion
In Iraq, the incidence of most types of cancer (including bladder cancer) has increased sharply in the last few years due to exposure to wars pollution [31–33]. Mutational analysis of the TP53 gene provides a unique opportunity to investigate the etiology, epidemiology, and pathogenesis of human cancer [34, 35]. Few studies have been conducted on the Iraqi population following the conflicts that led to hazardous environmental pollution. The effects of exposure to such pollutants is hard to ascertain as it is not possible to compare to data pre-conflict, which are not available either because they were not measured or, because they were destroyed. There is also the difficulty in finding a cohort of unexposed individuals: the conflicts were country wide and the shifting sands spread chemical pollutants over great distances. A definitive geographical location of where the greatest chemical pollution exists could not be determined [31, 32]. However, it is not implausible to suggest that almost all Iraqis have had some exposure to hazardous and/or toxic substances. To the best of our knowledge, the present study is the first molecular analysis of TCC in Iraq to determine the pattern of TP53 mutations. The results were compared with other areas polluted with radioactive substances [15, 35] and with reported specific TP53 mutations that were known to be associated with smoking, as smoking is a major risk factors for bladder cancer [5].
The present investigation revealed that the frequency of TP53 mutations was higher in deep invasive-tumors (high grade and stage T2) than superficially invasive tumors (low grade and stage Ta-T1) (37.9% Vs 35.7%) (OR, 1.2; CI, 0.26-5.4) (Table 2). These observations provide further support for the proposed association between TP53 alteration and bladder cancer progression [5, 20, 36]. In these results, a history of smoking was not associated with a high frequency of TP53 mutation, nor with the pattern of mutation in patients with TCC.
Although the number of our patients is rather small, many interesting observations are apparent. Our results showed that the TP53 double mutations constituted 27.3% of all mutations detected, which is consistent with values reported by Yamamoto et al., (1999) [15] who found double mutations in their cases of dysplasia and CIS in radio-contaminated areas. The possible explanation for the occurrence of double mutations found in our study is most likely because of the presence of a strong carcinogenic insult from war pollution that may have resulted in multiple transformation events [15, 37].
It has been indicated that G → A transitions were the most prevalent type of TP53 mutation in bladder cancer; about half of these transitions occurred at CpG sites [38]. There is increasing evidence to indicate that CpG bases might be more susceptible than other sites to attack by environmental mutagens [39]. Studies conducted in radio-contaminated regions in Ukraine found a high frequency of CpG/G → A mutations (73%) that were significantly different from those reported by IARC [17]. In the present study, the frequency of all G → A transitions was 38.4% and those that occurred at CpG sites were 23.8% with predominant hotspots (2 out of 3 cases) at codon 196. This is considered to be infrequent in bladder tumors [40] and may reflect the effect of certain exogenous carcinogens, such as depleted uranium, on the frequency of mutation (Table 1).
Conversely, the transversion type of mutation that was shown in this study (30.8%) was similar to a previously reported finding which confirmed that TP53 mutation in bladder cancer patients who smoked consisted of G:C → C:G transversions [41, 42]. In our study, most TP53 mutations occurred in both smokers and non-smokers (such as G → C transversions), or occurred in non-smokers only (such as C → A and T → G transversions). This observation unveils new evidence for the presence of risk factors for cancer, other than cigarette smoking, that may underlie this type of mutation.
Another important observation was the frameshift mutations which were found to be higher (30.8%) in frequency than what has been reported previously [5, 43], and was found preferentially to occur in exon-7 . Two the frameshift mutation having the same mutation (insertion A after codon 244) that cannot be excluded as a relative hotspot (Table 1). In fact, the most common mutations observed in TP53 DNA binding (exons 5–8) were missense mutations while frameshift types were found to be less frequent [43]. Most studies concerning the mutational signature of p53 in relation to the history of smoking revealed that the frameshift mutation in the DNA binding either have not been observed [44] or occurred less frequently than point mutation (7% and 7.1%) with different types of deletions and insertions [7, 40]. In radio-contaminated regions in Ukraine, all TP53 mutations determined were single-bp substitutions; no base deletions or insertions were found [15, 45]. This indicated a possible distinct molecular carcinogenesis pathway for bladder cancer after the Chernobyl disaster, based on a different incidence of p53 gene mutations compared with tumors found in the same population before the accident [45].
Accordingly, frameshift mutations (especially insertion A) of TP53 may reflect the effect of certain exogenous environmental contamination and may be considered as a useful predictor marker for bladder cancer. No reports on the levels of environmental pollution from toxic chemicals or radiation exist as no studies have been conducted to measure and specify these effects with accuracy. This study and future studies on the health of the Iraqi populace are needed to stimulate investigations on the extent and localization of environmental pollution caused by the recent conflicts.
In fact, the occurrence of TP53mutations leads to conformational changes of the protein, resulting in a prolonged half-life and subsequent accumulation of mutations in the nuclei. The extended half-life of the protein is the basis for immunohistochemical detection of TP53 [20, 22, 44]. Whilst immunohistochemical positivity for TP53 protein generally reflects point mutations of TP53 genes in tumor cells, it is not always synonymous with mutations [20, 22]. The present study revealed that the TP53 overexpression (58.6%) was observed more frequently in high grade and in T2 stage than in low grade and Ta and T1 tumors (p ≤ 0.05) (Table 2). This is consistent with other findings which reported that the TP53 overexpression was associated with high grade and stage of bladder cancer [20, 46].
It has been reported that there is a good concordance between overexpression and mutation of TP53 gene [20, 22], however, other studies have shown a considerable discrepancy between them [47, 48]. Analysis of the data in this study showed no significant association between TP53 mutations and the immunohistochemical detection of TP53 protein (p>0.05) (Table 3). This is largely because of the four tumors with frameshift mutations that had no detectable TP53 protein. These mutations encoded deleted or truncated proteins that are very unstable in the cell and usually not detectable by IHC method even when using an antibody containing the corresponding N-terminal epitope [49, 50]. The tumors with missense mutations were positive for TP53 protein overexpression (Table 3); missense mutations resulting in amino acid change render the TP53 protein a more stable compound with a longer half-life that can be detected by standard immunhistochemical methods [20, 44].
On the other hand, the presence of other tumors that demonstrated TP53 overexpression without mutations might be due to mutations in the TP53 that occurred outside exons 5–8 [49], or to the overexpression of TP53 caused not only by TP53 mutations but also by other factors (such as MDM2) which bind to TP53 protein, thus increasing its half-life and allowing it to accumulate in the nucleus. This observation may reflect alterations in the TP53 pathway rather than in the TP53 gene itself [6, 51]. However, the antibody used in our study recognises both the wild-type and the mutant forms of TP53 protein at the same time. Hence, it is possible that the IHC assay detects accumulation of the wild-type in some cases. The level of wild-type TP53 protein can be increased in response to DNA damage, hypoxia, oncogene activation and changes in the nucleotide pool, which are commonly observed in primary tumors [51, 52]. Furthermore, up-regulation of wild-type TP53 protein in tumors may indicate the last step of defence before metastasis [53]. Therefore, the TP53 alteration (TP53status) that is used as a prognostic marker of bladder tumorigenesis should be determined by combination of mutational and IHC analysis. Accordingly, the present investigation of TP53 status has shown a strong association with deep invasive tumors (p≤ 0.01) (Table 2). The altered expression of TP53 tumor suppressor gene is an independent predictor of bladder cancer progression when examined as an individual determinant [10, 20].
Conclusions
The TP53 frameshift mutations (especially insertion A) and 196 hotspot codon may represent a possible specific-mutational patterns associated with bladder tumorigenesis, and reflect a preferential target for exogenous carcinogens. Furthermore, the difference in incidence and type of TP53 mutations among the Iraqi TCC patients may explicitly indicate a distinct molecular pathway responsible for the development of bladder cancer due to exposure to environmental hazards (e.g. depleted uranium). The unusual mutation patterns of TP53 necessitates a complete molecular epidemiological study for further clarification of distinct molecular pathways for bladder cancer pathogenesis among Iraqi patients. The current study confirmed that the combination of molecular analysis and protein expression of TP53 tumor suppressor gene is highly recommended for studying gene alterations in bladder cancer rather than the application of a single approach.
Abbreviations
- LSAB+:
-
Labeled Streptavidin-biotin
- BC:
-
Bladder Cancer
- TCC:
-
Transitional Cell Carcinoma
- FFPE:
-
Formalin-Fixed Paraffin-Embedded Tissue
- DU:
-
Depleted Uranium
- IHC:
-
Immunohistochemistry
- PCR:
-
Polymerase chain reaction
- TUR:
-
Transurethral
- SSCP:
-
Single strand conformation polymorphism.
References
Bray F, Sanklla R, Ferlay J, Parkin DM: Estimates of cancer incidence and mortality in Europe in 1995. Eur J Cancer. 2002, 38: 99-166. 10.1016/S0959-8049(01)00350-1.
Heijden A, Hulsbergen-Van de kaa CA, Witjes JA: The influence of thermo-chemotherapy on bladder tumors: an immunohistochemical analysis. World J Uorl. 2007, 25 (3): 303-308. 10.1007/s00345-007-0143-1.
Al-Foudi A, Parkin DM: Seven years data from the Baghdad tumor registry. Int. J. Cancer. 2006, 34 (2): -10.1002/ijc.2910340211.
Zeegers M, Swaen G, Kant I, Goldbohm R, van den Brandt P: Occupational risk factors for male bladder cancer: results from a population based case cohort study in the Netherlands. Occup Environ Med. 2010, 58: 590-596.
Wallerand H, Bakkar AA, de Medina SG, Pairon JC, Yang YC, Vordos D, Bittard H, Fauconnet S, Kouyoumdjian JC, Jaurand MC, Zhang ZF, Radvanyi F, Thiery JP, Chopin DK: Mutations in TP53, but not FGFR3, in urothelail cell carcinoma of the bladder are influenced by smoking: contribution of exogenous versus endogenous carcinogens. Carcinogenesis. 2005, 26 (1): 177-184.
Vogelstein B, Lane D, Levine AJ: Surfing the p53 network. Nature. 2000, 408: 307-310. 10.1038/35042675.
Olivier M, Eeles R, Hollstein M, Khan MA, Harris CC, Hainaut P: The IARC TP53 database: new online analysis and recommendations to users. Hum Mutat. 2002, 19: 607-614. 10.1002/humu.10081.
Chen D, Yu Z, Zhu Z, Lopez C: The p53 pathway promotes efficient mitochondrial DNA base excision repair in colorectal cancer cells. Cancer Res. 2006, 66 (7): 3485-3494. 10.1158/0008-5472.CAN-05-4103.
Esriq D, Elmajian D, Groshen S, Freeman JA, Stein JP, Chen SC, Nichols PW, Skinner DG, Jones PA, Cote RJ: Accumulation of Nuclear p53 and Tumor Progression in Bladder Cancer. New Eng J Med. 1994, 331 (19): 1259-1264. 10.1056/NEJM199411103311903.
Chatterjee S, Datar R, Youssefzadeh D, George B, Goebell P, Stein J, Young L, Shi SR, Gee C, Groshen S, Skinner DG, Cote RJ: Combined effects of P53, P21, and PRb expression in the progression of bladder transitional cell carcinoma. J Clin Oncol. 2004, 22 (6): 1007-1013. 10.1200/JCO.2004.05.174.
Mitra AP, Datar RH, Cote RJ: Molecular staging of bladder cancer. BJU Int. 2005, 96 (1): 7-12. 10.1111/j.1464-410X.2005.05557.x.
Crow JF: How much do you know about spontaneous mutation rates. Environ Mol Mutagenesis. 1993, 21: 122-129. 10.1002/em.2850210205.
Hollstein M, Rice K, Greenbelt MS, Soussi T, Fuchs R, Sorlie T, Hoviq E, Smith-Sorensen B, Montesano R, Harris CC: Database of p53 gene somatic mutations in human tumors and cell lines. Nucleic Acids Res. 1994, 22 (17): 3351-3355.
Cho Y, Gorina S, Jeffrey PD, Pavletich NP: Crystal structure of a p53 tumor suppressor-DNA complex: understanding tumorigenic mutations. Science. 1994, 265 (5170): 346-355. 10.1126/science.8023157.
Yamamoto S, Romanenko A, Wei M, Masuda C, Zaparin W, Vinnichenko W, Vozianov A, Lee CC, Morimura K, Wanibuchi H, Tada M, Fukushima S: Specific p53 gene Mutations in Urinary Bladder Epithelium after the Chernobyl Accident. Cancer Res. 1999, 59 (15): 3606-3609.
Vahakangas K: Molecular epidemiology of human cancer risk. Gene-enviroment interactions and P53 mutation spectrum in human ling cancer. Methods Mol Med. 2003, 74: 43-59.
Silverman DT, Mooison AS, Deveas SS: Bladder cancer. Cancer epidemiology and prevention. Edited by: Schottenfold D, Fraumeni JF. 1996, Oxford University Press , New York, 1156-1179.
Loda M, Cukor B, Tam SW, Lavin P, Fiorentino M, Draetta GF, Jessup JM, Pagano M: Increased proteasome-dependent degradation of the cyclin-dependent kinase inhibitor P27 in aggressive colorectal carcinomas. Nature Med. 1997, 3 (2): 231-234. 10.1038/nm0297-231.
Chatterjee SJ, George B, Goebell P, Alavi-Tafreshi M, Shi SR, Fung YK, Jones PJ, Cordon-Cardo C, Datar RH, Cote RJ: Hyperphosphorylation of pRb: a mechanism for RB tumor suppressor pathway inactivation in bladder cancer. J Pathol. 2004, 203 (3): 762-770. 10.1002/path.1567.
Esriq D, Spruck C, Nichols PW, Chaiwun B, Steven K, Groshen S, Chen SC, Skinner DG, Jones PA, Cote RJ: P53 nuclear protein accumulation correlates with mutations in the P53 gene, tumor grade, and stage in bladder cancer. Am J Pathol. 1993, 143 (5): 1389-1397.
Mizobuchi S, Furihata M, Sonobe H, Ohtsuki Y, Ishikawa T, Murakami H, Kurabayashi A, Ogoshi S, Sasaguri S: Association between p53 immunostaining and cigarette smoking in squamous cell carcinoma of the esophagus. Japn J Clin Oncol. 2000, 30 (10): 423-428. 10.1093/jjco/hyd114.
Vet JA, Brinquier PP, Schaafsma HE, Witjes JA, Debruyne FM, Schalken JA: Comparison of p53 protein overexpression with p53 mutation in bladder cancer: Clinical and biological aspects. Lab Invest. 1995, 73 (6): 837-843.
Xing EP, Yang GY, Wang LD, Shi ST, Yang CS: Loss of heterozygosity of the Rb gene correlates with pRb protein expression and associates with p53 alteration in human esophageal cancer. Clin Cancer Res. 1999, 5 (5): 1231-1240.
Epstein JI, Amin MB, Reuter VR, Mostofi FK: The World Health Organization/International Society of Urological Pathology consensus classification of urothelial (transitional cell) neoplasms of the urinary bladder. Bladder Consensus Conference Committee. Am J Surg Pathol. 1998, 22 (12): 1435-1448. 10.1097/00000478-199812000-00001.
AJCC Cancer Staging Manual. Edited by: Green F, Page D, Fleming I, Fritz A, Balch C, Haller D, Morrow M. 2002, Springer, New York, NY, 6
Al-Dujaily EA, Al-Janabi AA, Pierscioniek T, Yasseen AA: High prevalence of HER-2/neu overexpression in female breast cancer among an Iraqi population exposed to depleted Uranium. Journal of Carcinogenesis. 2008, 7: 1-5. 10.1186/1477-3163-7-1.
Al-Abbassi DS, Al-Janabi AA, Al-Toriahi KM, Jabor TH, Yasseen AA: Expresssion of VEGF in urinary bladder transitional cell carcinoma in an Iraqi population subjected to depleted Uranium. Applied immunohistochemistry and molecular morphology. 2009, 17 (4): 307-311. 10.1097/PAI.0b013e3181941794.
Al-Mumen MM, Al-Janabi AA, Jumaa AS, Al-Toriahi KM, Yasseen AA: Exposure to depleted Uranium does nor alter the co-expression of HER-2/neu and P53 in breast cancer patients. BMC Research Notes. 2011, 4: 87-10.1186/1756-0500-4-87.
Sato T, Tanigami A, Yamakawa K, Akiyama F, Kasumi F, Sakamoto G, Nakamura Y: Allelotype of breast cancer: cumulative allele losses promote tumor progression in primary breast cancer. Cancer Res. 1990, 50: 7184-7189.
Liechti-Gallati S, Schneider V, Neeser D, Kraemer : Two buffer page system-based SSCP/HD analysis of DNA and RNA: a general protocol for rapid and sensitive mutation screening in cystic fibrosis and any other human genetic disease. Eur J Hum Genet. 1999, 7: 590-598. 10.1038/sj.ejhg.5200338.
Khudair A, Abdul Kader K and Al-Taha T: Study of the radiological pollution level in pastures of Basrah in: The conference on the effects of the use of DU weaponry on human and environment in Iraq: 26-27March 2002. 2000, Baghdad, Iraq
Tawfiq NF, Al-Jobori SM, Al-Saji AW, Itawi RK: Determination of Alpha-emitters in Iraqi soil samples using solid state nuclear track detectors CR-39 and CN-85. The Conference on the Effects of DU Weaponry on Human and Environment in Iraq. 2002, The Iraqi Ministry of Higher Education and Scientific Research, Baghdad, Iraq
Al-Azzawi S: Depleted Uranium radioactive contamination in Iraq: An overview. Global Res. 2006, Center for Research on Globalization, ,www.globalresearch.ca,
Denissenko MF, Chen JX, Tang M-S, Pfeifer GP: Cytosine methylation determines hot spots of DNA damage in the human p53 gene. Proc Natl Acad Sci USA. 1997, 94: 3893-3898. 10.1073/pnas.94.8.3893.
Little JB: Radiation Carcinogenesis. Carcinogenesis. 2000, 21 (3): 347-404.
Lipponen PK: Overexpression of p53 nuclear oncoprotein in transitional cell bladder cancer and its prognostic value. Int J Cancer. 1993, 53 (3): 365-376. 10.1002/ijc.2910530304.
Yamamoto S, Tatematsu M, Yamamoto M, Fukami H, Fukushima S: Clonal analysis of urothelial carcinomas in C3H/HeN ↔BALB/c chimeric mice treated with N-butyl-N-(4-hydroxybutyl) nitrosamine. Carcinogenesis. 1998, 19 (5): 855-860. 10.1093/carcin/19.5.855.
Williamson MP, Elder PA, Knowles MA: The spectrum of Tp53 mutations in bladder carcinoma. Genes chromosome Cancer. 1994, 9 (2): 108-118. 10.1002/gcc.2870090206.
Pfeifer GP: P53 mutational spectra and the role of methylated CpG sequences. Mutat Res. 2000, 450 (1–2): 155-166.
Schroeder JC, Conway K, Li Y, Mistry K, Bell DA, Taylor JA: p53 Mutations in bladder cancer: evidence for exogenous versus endogenous risk factors. Cancer Res. 2003, 63 (21): 7530-7538.
Jung I, Messing E: Molecular mechanism and pathways in bladder cancer development and progression. Cancer control. 2000, 7 (4): 325-334.
Habuchi T, Takahashi R, Yamada H, Ogawa O, Kakehi Y, Ogura K, Hamazaki S, Toguchida J, Ishizaki K, Fujita J: Influence of cigarette smoking and schistosomiasis on p53 gene mutation in urothelial cancer. Cancer Res. 1993, 53 (16): 3795-3799.
Harris CC: Structure and function of the p53 tumor suppressor gene: clues for rational cancer therapeutic strategies. J Natl Cancer Inst. 1996, 88 (20): 1442-1455. 10.1093/jnci/88.20.1442.
Moore LE, Smith AH, Eng C, DeVries SD, Kalman D, Bhargava V, Chew S, Ferreccio C, Rey OA, Hopenhayn C, Biggs ML, Bates MN, Waldman FM: P53 alterations in bladder tumors from arsenic and tobacco exposed patients. Carcinogenesis. 2003, 24 (11): 1785-1791. 10.1093/carcin/bgg136.
Morimura K, Romanenko A, Min W, Salim E, Kinoshita A, Wanibuchi H, Vozianov A, Fukushima S: Possible disitinct molecular carcinogenic pathways for bladder cancer in Ukraine, before and after the Chernobyl disaster. Oncol Rep. 2004, 11: 881-886.
Shariat SF, Tokunaga H, Zhou J, Kim J, Ayala GE, Benedict WF, Lerner SP: P53, P21, PRB, and P16 expression predict clinical outcome in cystectomy with bladder cancer. J Clin Oncol. 2004, l22 (6): 1014-1024.
Matsushima AY, Cesarman E, Chadburn A, Knowles D: Post thymic T cell lymphomas frequently overexpress p53 protein but infrequently exhibit p53 gene mutation. Am J Pathol. 1994, 144 (3): 573-584.
Hall PA, Lane DP: P53 in tumor pathology: can we trust immunohistochemistry?—Revisited. J Pathol. 1994, 172 (1): 1-4. 10.1002/path.1711720103.
Greenblatt MS, Bennett WP, Hollstein M, Harris CC: Mutations in p53 tumor suppresser gene: clues to cancer etiology and molecular pathogenesis. Cancer Res. 1994, 54: 4855-4878.
Knowles MA: Molecular subtypes of bladder cancer: Jekyll and Hyde or chalk and chees?. Carcinogenesis. 2006, 27 (3): 361-373.
Vazquez A, Bond E, Levine A, Bond G: The genetics of the p53 pathway, apoptosis and cancer therapy. Nat Rev Drug Discovery. 2008, 7: 979-987. 10.1038/nrd2656.
Shiao YH, Palli D, Caporaso NE, Alvord WG, Amorosi A, Nesi G, Saieva C, Masala G, Fraumeni JF, Rice JM: Genetic and immunohistochemical analyses of p53 independently predict regional metastasis of gastric cancers. Cancer Epidemiol Biomarkers Prev. 2000, 9 (6): 631-633.
Jen K-Y, Cheung VG: Identification of novel p53 target genes in ionizing radiation response. Cancer Res. 2005, 65: 7666-7673.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
ThAA and MH carried out the molecular genetic studies. THAA performed the statistical analysis. AA and AKM initiated the project at the University of Kufa . DA and AA carried out the immunohistochemical analysis and histopathological examination. MR participated in the molecular genetic studies. MNA provided the surgical specimens. AAY and AA conceived of the study, participated in its design and drafted the manuscript. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Al-Kashwan, T.A., Houshmand, M., Al-Janabi, A. et al. Specific-mutational patterns of p53 gene in bladder transitional cell carcinoma among a group of Iraqi patients exposed to war environmental hazards. BMC Res Notes 5, 466 (2012). https://doi.org/10.1186/1756-0500-5-466
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1756-0500-5-466