
Abstract
Introduction
Carney complex is a multiple neoplasia syndrome involving cardiac, endocrine, neural and cutaneous tumors with a variety of pigmented skin lesions. It has an autosomal dominant mode of inheritance. Approximately 7% of cardiac myxomas are related to the Carney complex. Myxomas that occur as part of the Carney complex affect both sexes with equal frequency. Cardiac myxomas with Carney complex are reported mostly in the left side of the heart and are less common on the right side. As per our review, this is the first reported case of Carney complex with right ventricle cardiac myxoma.
Case presentation
We present a rare case of recurrent cardiac myxoma in a patient later diagnosed to have Carney complex. A 46-year-old Caucasian man with a history of thyroid hyperplasia came to out-patient cardiology department with new onset atrial fibrillation. A transthoracic echocardiogram revealed a right ventricular mass attached to his interventricular septum, which was later seen on a transesophageal echocardiogram and cardiac magnetic resonance imaging. He underwent resection of the ventricular mass which on pathology revealed myxoma. He later developed skin lesions, pituitary adenoma and Sertoli cell tumor suggesting Carney complex. Two years later he developed a new mass within his right atrium which was later resected.
Conclusions
Carney complex is a rare autosomal dominant disease with variable penetrance. Since it involves multiple organs, patients diagnosed with Carney complex should undergo serial endocrine workup, neural assessments, echocardiograms and testicular ultrasounds. Of the total number of cases of Carney complex, 65% are linked to PRKAR1A gene mutation. It is important for clinicians to be cognizant of a link between cardiac myxoma and Carney complex. The use of multi-imaging modalities allows better delineation of the mass before planned resection. Carney complex-related cardiac myxoma comprises 7% of all cardiac myxomas. Right ventricular cardiac myxomas are rare. This case report is the first to describe right ventricular myxoma with Carney complex.
Similar content being viewed by others


Introduction
Carney complex (CNC) is an autosomal dominant multiple neoplasia syndrome involving skin and cardiac myxomas, pigmented skin lesions and endocrine tumors. About 700 patients worldwide have been reported by the National Institutes of Health, Mayo Clinic (USA) and the Institut Cochin (France) by January 2008 [1]. Cardiac myxomas are the second most common manifestations of CNC after skin lentigines [2]. Among all cardiac myxomas, left atrial cardiac myxomas are the most common (75%) [3, 4], followed by right atrial (18%), with left and right ventricular myxomas being the least common (2.5 to 4%) [5–7]. Nearly 7% of all cardiac myxomas are associated with CNC. Various locations of cardiac myxomas associated with CNC have been reported so far but none originating in the right ventricle. We are reporting a case of recurrent cardiac myxoma of the right side of the heart which recurred 2 years after the initial presentation with simultaneous pituitary microadenoma and skin lentigines consistent with the diagnosis of CNC.
Case presentation
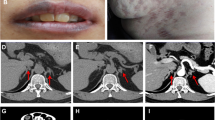
A 46-year-old Caucasian man recently diagnosed with benign thyroid hyperplasia presented to his primary care physician with palpitations, light-headedness, and dizziness and was found to be in atrial fibrillation with rapid heart rate of 140 beats per minute. He denied chest pain, shortness of breath, fevers, night sweats, weight loss, and fatigue. His heart rate was controlled and a transthoracic echocardiogram (TTE) was obtained which showed a right ventricular mass attached to his interventricular septum that was confirmed on a subsequent transesophageal echocardiogram (Figure 1A, 1B, 1C) [Additional file 1: Movies 1 and 2]. Cardiac magnetic resonance imaging (MRI) showed a 2.5cm soft tissue density in his right ventricle attached to the mid-septum (Figure 2A, 2B, 2C).

Transthoracic and transesophageal echocardiograms. (A, B) Parasternal long and short axis views showing right ventricular mass (marked with red arrow). C: Transesophageal echocardiogram: Five chamber view, showing right ventricular mass attached with a stalk to interventricular septum (red arrow).

Magnetic resonance imaging. (A, B) Magnetic resonance imaging perfusion imaging showing right ventricular mass extending from the base of the right ventricle to the apex (red arrow). C: Magnetic resonance imaging pre-scan (pre-perfusion) images showing right ventricular mass (red arrow).
A surface echocardiogram was performed intraoperatively [Additional file 2: Movie 3] and surgical resection of the right ventricular mass was performed followed by the Maze procedure. The resected mass was bilobed measuring at least 7cm×1.5cm (Figure 3A, 3B). Pathology confirmed a myxoma (Figure 4A, 4B, 4C, 4D). Brownish macules were noted on the patient’s lips, conjunctivae and all over his body. Considering his examination findings, cardiac myxoma and history of thyroid neoplasm, concern for a genetic syndrome was raised. He denied any known family history of similar examination findings or known hereditary diseases. At that time he did not pursue genetic screening and was followed regularly with yearly TTE.

Intra- operative pictures. A: A right ventricular myxoma seen through the tricuspid valve intraoperatively. B: Right ventricular mass attached to the base of the right ventricle. C: Small resected mass at the apex of right atrium.

Histopathology. A: Hematoxylin and eosin stain showing scattered single myxoma cells, stellate and plump, in a background of amorphous; basophilic material admixed with fibrillary pink stroma. B: Hematoxylin and eosin stain showing myxoma cells forming rings, cords and nests. C: Hematoxylin and eosin stain showing heterologous bone within tumor. D: Hematoxylin and eosin stain showing heterologous smooth muscle elements within the tumor.
Additional file 2: Movie 3. Surface echocardiogram in the operating room reveals bilobed right ventricular mass. (WMV 238 KB)
Screening with TTE 2 years later revealed a new mass in his right atrium measuring 1.8cm×1.4cm on resection and it was a myxoma (Figure 3C). He underwent rigorous workup for CNC which revealed elevated insulin-like growth factor 1 (IGF-1) levels, and positive oral glucose tolerance test with pituitary microadenoma on MRI consistent with acromegaly. He was also diagnosed with bilateral multiple large-cell calcifying Sertoli cell tumor (LCCSCT) of the testes. He was treated for acromegaly and was also recommended to follow up with repeat pituitary MRI in 6 months and an annual testicular ultrasonography. His children were sent for genetic studies.
Discussion
The CNC was first described in 1985 by J. Aidan Carney, as the combination of myxomas, spotty pigmentation and endocrine overactivity [8]. CNC is defined as an autosomal dominant, multiple neoplasia syndrome involving skin and cardiac myxomas, pigmented skin lesions and endocrine tumors.
The most recent diagnostic criteria include clinical findings such as spotty skin pigmentation, cutaneous and cardiac myxomas, breast myxomatosis, acromegaly, primary pigmented nodular adrenocortical disease, blue nevus, epithelioid blue nevus, osteochondromyxoma, thyroid carcinoma, LCCSCT in males, ovarian cyst in females and mutation of the PRKAR1A gene. At least two of these manifestations must be present to confirm the diagnosis of CNC. With PRKAR1A mutation and/or a first-degree relative affected by CNC, a single manifestation is sufficient for the diagnosis [8–11].
Cardiac myxomas are rare benign tumors accounting for 45% of primary cardiac tumors in adults [12] and among cardiac myxomas, left atrial cardiac myxomas are the most common (75%) followed by right atrial (18%), followed by left and right ventricular myxomas being the least common (2.5 to 4%). Up to 7% of all the cardiac myxomas are associated with CNC and are notorious for recurrence [13] when compared to sporadic cardiac myxomas. CNC cardiac myxomas are known to have a left heart origin and are unlikely to be right sided as in our patient. Patients with CNC who have cardiac tumors may be totally asymptomatic but have an increased risk of sudden death, which makes it clinically important.
CNC is associated with at least two genetic loci including the PRKAR1A gene located on chromosome 17 and the CNC2 locus mapped to chromosome 2 [14] and a possible third loci. Clinical suspicion of CNC should be followed by thorough evaluation. This includes biochemical and imaging modalities for endocrine, cardiac and skin tumors. A preoperative coronary angiograph is advised if coronary artery disease is suspected or if the patient is above the age of 40 years [15]. Surgical excision of the tumors is the primary management of most tumors [16].
Due to its high association with morbidity and mortality, surveillance is key. For pre-pubertal, post-pubertal children and adults with excised myxoma, an echocardiogram is performed every 6 months or yearly. For children with LCCSCT, close monitoring of growth rate, pubertal status and testicular ultrasonography are essential. Every patient diagnosed with CNC should have a yearly testicular ultrasound, and serum IGF-1 levels and urinary free cortisol levels should be monitored. Thyroid ultrasound and ovarian ultrasound should be repeated as needed [17]. Approximately 70% of individuals diagnosed with CNC have an affected parent; approximately 30% have a de novo mutation [1]; first degree relatives should be screened when PRKAR1A mutations are identified.
Conclusions
Our patient initially had multiple myxomas in his right ventricle, the least common location of cardiac myxomas, which aroused the suspicion of CNC and reevaluation confirmed the diagnosis. This is the first case of right ventricular cardiac myxoma in association with CNC.
Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Abbreviations
- CNC:
-
Carney complex
- IGF-1:
-
Insulin-like growth factor 1
- LCCSCT:
-
Large-cell calcifying Sertoli cell tumor
- MRI:
-
Magnetic resonance imaging
- TTE:
-
Transthoracic echocardiogram.
References
Stratakis CA, Horvath A: Carney Complex [Updated 2012 Sep 20]. GeneReviews™ [Internet]. Edited by: Pagon RA, Adam MP, Bird TD. 2003, Seattle: University of Washington, 1993-2014.
Stratakis CA, Kirschner LS, Carney JA: Clinical and molecular features of the Carney complex: diagnostic criteria and recommendations for patient evaluation. J Clin Endocrinol Metab. 2001, 86 (9): 4041-4046. 10.1210/jcem.86.9.7903.
Pinede L, Duhaut P, Loire R: Clinical presentation of left atrial cardiac myxoma. A series of 112 consecutive cases. Medicine (Baltimore). 2001, 3: 159-172.
Peachell JL, Mullen JC, Bentley MJ, Taylor DA: Biatrial myxoma: a rare cardiac tumor. Ann Thorac Surg. 1998, 6: 1768-1769.
Chen M, Wang JH, Chao SF, Hsu YH, Wu DC, Lai CP: Cardiac myxoma originating from the anterior mitral leaflet. Jpn Heart J. 2003, 44: 429-434. 10.1536/jhj.44.429.
Grebenc ML, Rosado-de-Christenson ML, Green CE, Burke AP, Galvin JR: Cardiac myxoma: Imaging features in 83 patients. Radio Graphics. 2002, 22 (3): 673-689.
Sa MI, Abreu A, Cabral S, Reis AH, Torres S, de Oliveira F, Oliveira R, Branco L, Galrinho A, Abreu A, Abreu J, Fiarresga A, Mamede A, Ramos R, Leal A, Pinto E, Fragata J, Ferreira R: Myxoma in the right ventricular outflow tract. Rev Port Cardiol. 2007, 26 (4): 377-381.
Carney JA, Gordon H, Carpenter PC, Shenoy BV, Go VL: The complex of myxomas, spotty pigmentation, and endocrine overactivity. Medicine (Baltimore). 1985, 64: 270-283.
Kirschner LS, Sandrini F, Monbo J, Lin JP, Carney JA, Stratakis CA: Genetic heterogeneity and spectrum of mutations of the PRKAR1A gene in patients with the Carney complex. Hum Mol Genet. 2000, 9: 3037-3046. 10.1093/hmg/9.20.3037.
Groussin L, Kirschner L, Vincent-Dejean C, Perlemoine K, Jullian E, Delemer B, Zacharieva S, Pignatelli D, Carney JA, Luton JP, Bertagna X, Stratakis CA, Bertherat J: Molecular analysis of the cyclic AMP-dependent protein kinase A (PKA) regulatory subunit 1A (PRKAR1A) gene in patients with Carney complex and primary pigmented nodular adrenocortical disease (PPNAD) reveals novel mutations and clues for pathophysiology: augmented PKA signaling is associated with adrenal tumorigenesis in PPNAD. Am J Hum Genet. 2002, 71: 1433-1442. 10.1086/344579.
Carney JA, Young WF: Primary pigmented nodular adrenocortical disease and its associated conditions. Endocrinologist. 1992, 2: 6-10.1097/00019616-199201000-00003.
MacGowan SW, Sidhu P, Aherne T, Luke D, Wood AE, Neligan MC: Atrial myxoma: National incidence, diagnosis and surgical management. Ir J Med Sci. 1993, 162: 223-226. 10.1007/BF02945200.
Carney JA: Carney complex: the complex of myxoma, spotty, pigmentation, endocrine overactivity and schwannomas. Semin Dermotal AM J Cardiol. 1989, 63: 1006-1008. 10.1016/0002-9149(89)90162-8.
Kacerovská D, Michal M, Síma R, Grossmann P, Kazakov DV: Carney complex. Cesk Patol. 2011, 47 (4): 192-197.
Obeid AI, Marvasti M, Parker F, Rosenberg J: Comparison of transthoracic and transesophageal echocardiography in diagnosis of left atrial myxoma. Am J Cardiol. 1989, 63: 1006-1008. 10.1016/0002-9149(89)90162-8.
Wr C: Cardiac neoplasms: Current diagnosis, pathology and therapy. J Card Surg. 1988, 3: 119-154. 10.1111/j.1540-8191.1988.tb00232.x.
Jérôme B: Carney Complex. Orphanet J Rare Dis. 2006, 1: 21-10.1186/1750-1172-1-21.
Acknowledgement
We would like to specially thank our patient who wanted the world to know more about this particular disease.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
AL, WS and KM carried out manuscript writing. AK and WS carried out editing of manuscript and images. JER, FCM and HGZ carried out proofreading of the manuscript. MRS carried out manuscript design, conceptualization, manuscript writing, editing and final proofread. All authors read and approved the final manuscript.
Electronic supplementary material
13256_2013_2780_MOESM1_ESM.zip
Additional file 1: Movie 1 and 2. Transthoracic echocardiogram and transesophageal echocardiogram showing right ventricle mass. (ZIP 608 KB)
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Sardar, M.R., Lahoti, A., Khaji, A. et al. Recurrent right ventricular cardiac myxoma in a patient with Carney complex: a case report. J Med Case Reports 8, 134 (2014). https://doi.org/10.1186/1752-1947-8-134
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1752-1947-8-134