
Abstract
Background
Acupuncture is used to reduce inflammation and decrease pain in delayed onset muscle soreness (DOMS). This study investigates the efficacy of acupuncture on the symptoms of DOMS.
Methods
Thirty subjects were assigned randomly to there groups, namely the control, non-tender point and tender point groups. Measurement of pain with full elbow flexion was used as indices of efficacy. Measurements were taken before and after exercise, immediately after treatment and seven days after treatment.
Results
Significant differences in visual analog scores for pain were found between the control group and tender point group immediately after treatment and three days after exercise (P < 0.05, Dunnetts multiple test).
Conclusion
The results show that tender point acupuncture relieves muscle pain of DOMS.
Similar content being viewed by others


Background
Delayed onset muscle soreness (DOMS) is a common myogenic condition with main symptoms of pain, tenderness and loss of range of movement that usually occur 24 to 48 hours when unaccustomed. While DOMS is not a serious condition, it may discourage the sufferer's participation in exercise and rehabilitation. Therapy for DOMS currently includes the use of anti-inflammatory analgesics [1], massage [2], transcutaneous electrical nerve stimulation (TENS) [3], ultrasound [4] and laser [5]. DOMS may result from an inflammatory process in muscle after exercise [6–8]. While previous studies show that acupuncture may or may not reduce inflammation and decrease pain in DOMS [9, 10], we believe that response to acupuncture largely depends on the choice and number of acupoints.
Recent clinical investigations on musculoskeletal pain, such as myofascial pain syndrome and fibromyalgesia, focus on tender points and/or trigger points which have already been used for diagnosis and treatment. The present study aims to investigate localized tenderness of experimentally induced DOMS and compare the characteristics of DOMS with those of myofascial pain syndrome [11, 12].
Methods
Subjects
Approved by the Meiji University of Integrative Medicine Ethics Committee this study included healthy student volunteers from the acupuncture school of the University (n = 30, aged 18–22 years). Volunteers were informed of the experimental procedures and agreed to participate in the present study by signing a consent form.
Screening procedure
The exclusion criteria were that the subjects did not have current injury or pain (bone fracture, bruise and/or sprain of upper arm), consumption of any form of drugs, pregnancy, hemophilia, diabetes mellitus, asthma, weight-training, intense fear of needles and participation in a similar experiment within the past year. All subjects were instructed to avoid any form of exercise during the experiment.
Pain induction
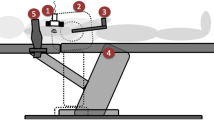
DOMS was induced with standard methods in the non-dominant elbow flexors (biceps brachii) of the subject [13, 14]. Subjects were seated behind an inclined biceps-curl bench so that they could fully flex and extend their elbows. The maximum weight lifted with one voluntary concentric contraction was determined with free weights (a loaded dumbbell) for each subject. This maximum weight was subsequently used to exhaust the elbow flexors. A researcher lifted the weight until the subject's elbow was in a position of full flexion. The subject was instructed to lower the weight as slowly as possible until the elbow reached full extension. The researcher returned the weight to the starting position (full elbow flexion) and the process was repeated for as many times as the subject could control the speed of descent of the weight. The time of exhaustion was taken as the point at which the subject could no longer control the lowering of the weight.
Randomization procedure
A researcher screened and enrolled subjects. After the participants completed a baseline evaluation, another researcher who was not involved with data collection randomly assigned them to one of the three treatment groups using a computer-generated (SAMPSIZE V2.0, Blackwell Science Ltd, UK), blocked random allocation sequence with a block size of three.
Experimental conditions
Control group
Subjects allocated to this group rested supinely on a standard treatment plinth for a period of 10 minutes.
Non tender point group (non-TeP group)
Subjects in this group received needling at four non-tender and non-acupuncture points located on the lateral side of the upper arm in the indentation between the biceps brachii and the brachialis. These points were typically located on the distal third of the belly of the biceps brachii approximately over the musculotendinous junction. Disposable stainless steel needles (0.18 mm × 40 mm, Seirin, Japan) were inserted straight to a depth of 1 to 2 cm and retained in place for 10 minutes.
Tender point group (TeP group)
Subjects in this group received needling at the points identified (by palpation) as the three most tender after exercise. These points were typically located on the distal third of the belly of biceps brachii approximately over the musculotendinous junction. Disposable stainless steel needles (0.18 mm × 40 mm, Seirin, Japan) were inserted straight to a depth of 1 to 2 cm and retained in place for 10 minutes.
Both non-TeP and TeP groups
Ten minutes after exercise, treatments were given to non-TeP and TeP groups simultaneously.
The acupuncture was performed by three acupuncturists with three years of acupuncture training and one or ten years of clinical experience.
Measurement
Pain measurement
Intensity of muscle pain of the arm muscle at full flexion was estimated before and immediately after exercise, immediately after treatment and one, two, three and seven days after exercise. Subjects were asked to rate their current level of pain by marking a visual analog scale (VAS). A 10 cm line appeared with 'no pain' marked at one end and 'maximum pain' marked at the other. Subjects were asked to indicate their current level of pain with full elbow flexion.
Experimental schedule
Thirty subjects were allocated randomly to one of the three groups. In treatment groups one and two, the VAS of the exercised muscle was measured before and immediately after exercise, immediately after and one, two, three, four and seven days after treatment. No treatment was performed in the control group, but the VAS was measured on the same schedule as the other groups. This study is an observer-blinded, randomized controlled clinical trial.
Blinding
The measurements were performed by an independent investigator who was not informed of the treatment allocation.
Statistical analysis
The data are reported as means ± standard deviation (means ± SD). Repeated measures analysis of variance (ANOVA) was used for the primary measure, an inter-group of VAS scores. Repeated measures ANOVA were performed in each group for intra-group differences, followed by pair wise comparisons with Sidak correction to maintain experiment error rate below 5%. Differences between the groups at each time period were analysed with the unpaired t test and Dunnett's test, by which each test performed was judged against a corrected significance level as α/c, where α is significance level (0.05) and c is the number of paired comparisons. SYSTAT 11 was used for the analysis of a between-group (repeated measures ANOVA) and StatView for Windows (version 5.0) was used for the analysis of between the groups (Dunnett's test). P < 0.05 was considered to be statistically significant.
Results
Subjects
Thirty subjects (13 women, 17 men; aged 18–22 years) were randomly assigned to the groups. No differences were found among the groups in terms of baseline variables and age.
Three subjects in the control group and one subject in the non-TeP group dropped out. The reason for dropout was that they received other treatments (e.g. massage, anti-inflammatory poultice). The analyses were conducted with the data from the 26 patients who completed the study (Figure 1).

Subject participation flow in the study.
VAS score
Immediately after exercise, subjects in all groups felt warmth and tenderness in the working muscle of the upper arm. The region of tenderness was gradually restricted to the musculotendinous junction, and a rope-like taut band was observed in the tender area after exercise on the first day of the study.
As shown in Table 1, the mean VAS scores tended to decrease from immediately after treatment, although the time courses were different for each group. There were statistically significant differences between the VAS scores of the control group and TeP group immediately (4.2 ± 2.7 vs 0.6 ± 0.9) and three days (2.4 ± 2.3 vs 0.4 ± 0.5) after treatment (P < 0.005 in both cases). There were no significant differences between VAS scores of the control group and non-TeP group. While the non-TeP group and TeP group reported relatively lower pain intensity than the control group, the differences were not statistically significant in ANOVA.
Discussion
A statistically significant difference was found only between the tender point acupuncture and control groups, immediately and three days after treatment. The results suggest that tender point acupuncture treatment may be effective for DOMS.
Clinical trials
Available experimental evidence does not consistently support acupuncture as a method for pain relief [15, 16]. Past studies were flawed in experimental design, sample size or control. In some randomized controlled trials of acupuncture, control groups were defined as no-treatment controls [17], pricking (without penetration) [18], minimal acupuncture (shallow and weak needling) [19] and mock TENS (without pulse) [20, 21]. Moreover, negative results tended to come from studies using non-tender point acupuncture [10] and positive results from studies using non-acupuncture control groups [9]. We used no-treatment controls and non-tender point acupuncture in this study. Non-tender point acupuncture has been proposed as a sham technique [22, 23], which is problematic due to the existence of diffuse noxious inhibitory controls (DNIC) phenomena. Painful stimulation inhibits pain, and DNIC has been proposed as a physiological basis of acupuncture analgesia [24, 25]. In fact, six subjects complained of dull sensation (known as deqi) during non-tender acupuncture treatment. Therefore, we used non-tender point acupuncture as treatment group in this study.
Previous experience with acupuncture and confidence in acupuncture may influence the measurement of efficacy [24, 26]. Therefore, the limitations of the present study is that the subjects were students of an acupuncture school, who had considerable knowledge of acupuncture and the special sensation of deqi, and who had confidence in acupuncture.
Effects of tender point acupuncture on DOMS
Our results show that tender point acupuncture has analgesic effects. The strength of stimulation may depend on various parameters such as manipulating procedure, size of needle and site of insertion. Tender point insertion of the needle affects sensitized nociceptors, whereas non-tender point insertion does not [27, 28]. Tender points are sites where nociceptors, such as polymodal-type receptors, have been sensitized by various factors [29, 30]. Our data suggest that acupuncture stimulation of tender points may activate sensitized polymodal-type receptors thereby relieving pain. In clinical practice, acupuncture treatment may be effective on myofascial pain syndromes.
Barlas et al. concluded that acupuncture had little effect on the cardinal signs and symptoms of DOMS. We find the claim problematic. Deep pain sensation, such as muscle pain, is very complex [31]. A previous study found that the intensity of muscle pain at full flexion and full extension were different [32]. Moreover, pressure algometry used in studying muscle pain excites cutaneous receptors and may induce pain sensation in the skin [33]. In the present study, we estimated the intensity of muscle pain of the arm at full flexion.
Conclusion
The present study shows that tender point acupuncture relieves the symptoms of DOMS. Large scale clinical trials are warranted to confirm this finding.
Abbreviations
- DOMS:
-
delayed onset muscle soreness
- TENS:
-
transcutaneous electrical nerve stimulation
- Non-TeP:
-
non-tender point
- TeP:
-
tender point
- VAS:
-
visual analog scale
- ANOVA:
-
analysis of variance
References
Barlas P, Craig JA, Robinson J, Walsh DM, Baxter GD, Allen JM: Managing delayed-onset muscle soreness: Lack of effect selected oral systemic analgesics. Arch Phys Med Rehabil. 2000, 81: 966-72. 10.1053/apmr.2000.6277.
Smith LL, Keating MN, Holbert D, Spratt DJ, McCammon MR, Smith SS, Israel RG: The effects of athletic massage on delayed onset muscle soreness, creatine kinase, and neutrophil count: A preliminary report. JOSPT. 1994, 19 (2): 93-9.
Craig JA, Cunningham MB, Walsh DM, Baxter GD, Allen JM: Lack of effect of transcutaneous electrical nerve stimulation upon experimentally induced delayed onset muscle soreness in humans. Pain. 1996, 67 (2–3): 285-9. 10.1016/0304-3959(96)03124-7.
Ciccone CD, Leggin BG, Callamaro JJ: Effects of ultrasound and trolamine salicylate phonophoresis on delayed-onset muscle soreness. Phys Ther. 1991, 71 (9): 666-75.
Craig JA, Barlas P, Baxter GD, Walsh DM, Allen JM: Delayed-onset muscle soreness: lack of effect of combined phototherapy/low-intensity laser therapy at low pulse repetition rates. J Clin Laser Med Surg. 1996, 14 (6): 375-80.
Armstrong RB, Warren GL, Warren JA: Mechanisms of exercise-induced muscle fibre injury. Sports Med. 1991, 12 (3): 184-207.
Smith LL: Acute inflammation: the underlying mechanism in delayed onset muscle soreness?. Med Sci Sports Exerc. 1991, 23: 542-551.
Ebbeling CB, Clarkson PM: Exercise-induced muscle damage and adaptation. Sport Med. 1989, 7: 207-234. 10.2165/00007256-198907040-00001.
Lin JG, Yang SH: Effects of acupuncture on exercise-induced muscle soreness and serum creatine kinase activity. Am J Chin Med. 1999, 27 (3–4): 299-305.
Barlas P, Robinson J, Allen J, Baxter GD: Lack of effect of acupuncture upon signs and symptoms of delayed onset muscle soreness. Clinical Physiology. 2000, 20 (6): 449-456. 10.1046/j.1365-2281.2000.00280.x.
Itoh K, Okada K, Kawakita K: A proposed experimental model of myofascial trigger points in human muscle after slow eccentric exercise. Acupunct Med. 2004, 22: 2-12.
Itoh K, Kawakita K: Effect of indomethacin on the development of eccrntric exercise-induced localized sensitive region in the fascia of the rabbit. Jap J Physiol. 2002, 52: 173-180. 10.2170/jjphysiol.52.173.
Craig JA, Cunningham MB, Walsh DM, Baxter GD, Allen JM: Lack of effect of transcutaneous electrical nerve stimulation upon experimentally induced delayed onset muscle soreness in humans. Pain. 1996, 67 (2–3): 285-9. 10.1016/0304-3959(96)03124-7.
Craig JA, Bradley J, Walsh DM, Baxter GD, Allen JM: Delayed onset muscle soreness: lack of effect of therapeutic ultrasound in humans. Arch Phys Med Rehabil. 1999, 80 (3): 318-23. 10.1016/S0003-9993(99)90144-2.
Chapman CR, Colpitts YH, Benedetti C, Kitaeff R, Gehrig JD: Evoked potential assessment of acupuncture analgesia: attempted reversal with noloxone. Pain. 1980, 9: 183-197. 10.1016/0304-3959(80)90006-8.
Brockhaus A, Elger CE: Hypoalgesic efficacy of acupuncture on experimental pain in man. Comparison of needle acupuncture and laser acupuncture. Pain. 1990, 43: 181-185. 10.1016/0304-3959(90)91071-P.
Coan RM, Wong G, Coan PL: The acupuncture treatment of neck pain: a randomized controlled study. Am J Chin Med. 1982, 9 (4): 326-32.
Johansson A, Wenneberg B, Wagersten C, Haraldson T: Acupuncture in treatment of facial muscular pain. Acta Odontol Scand. 1991, 49: 153-8. 10.3109/00016359109005900.
Vincent CA: A controlled trial of the treatment of migraine by acupuncture. Clin J Pain. 1989, 5: 305-12.
Petrie JP, hazleman BL: A controlled study of acupuncture in back pain. Br J Reumatol. 1986, 25: 271-5. 10.1093/rheumatology/25.3.271.
Streitberger K, Kleinhenz J: Introducing a sham needle into acupuncture research. Lancet. 1998, 352: 364-5. 10.1016/S0140-6736(97)10471-8.
Vincent C, Lewith G: Placebo controls for acupuncture studies. J R Soc Med. 1995, 88: 199-202.
Richardson PH, Vincent CA: Acupuncture for the treatment of pain: a review of evaluative research. Pain. 1986, 24: 15-40. 10.1016/0304-3959(86)90023-0.
Nabeta T, Kawakita K: Relief of chronic neck and shoulder pain by manual acupuncture to tender point – a sham-controlled randomized trial. Complement Ther Med. 2002, 10: 217-22. 10.1016/S0965-2299(02)00082-1.
Bing Z, Villanueva L, Le Bars D: Acupuncture and diffuse noxious inhibitory controls: naloxone-reversible depression of activities of trigeminal convergent neurons. Neuroscience. 1990, 37: 809-818. 10.1016/0306-4522(90)90110-P.
Birch S, Jamison RN: Controlled trial of Japanese acupuncture for chronic myofascial neck pain: assessment of specific and nonspecific effects of treatment. Clin J Pain. 1998, 14: 248-255. 10.1097/00002508-199809000-00012.
Ceccherelli F, Rigoni MT, Gagliardi G, Ruzzante L: Comparison of superficial and deep acupuncture in the treatment of lumbar myofascial pain: a double-blind randomised controlled study. Clin J Pain. 2002, 18 (3): 149-53. 10.1097/00002508-200205000-00003.
Ishimaru K, Kawakita K, Sakita M: Analgesic effects by TENS and electroacupuncture with different types of stimulating electrodes on deep tissues in human subjects. Pain. 1995, 63 (1): 181-7. 10.1016/0304-3959(95)00030-V.
Kawakita K: Polymodal receptor hypothesis on the peripheral mechanisms of acupuncture and moxibustion. Am J Acupunct. 1993, 21 (4): 331-338.
Kumazawa T: Nociceptors and autonomic nervous control. Asian Med J. 1981, 24: 632-56.
Kawakita K, Miura T, Iwase Y: Deep pain measurement at the tender point by pulse algometry with insulated needle electrodes. Pain. 1991, 44: 235-239. 10.1016/0304-3959(91)90091-B.
Itoh K, Kawamoto S, Fujiwara H, Nakano Y, Yamaguchi M, Nanba T, Nishida A, Ochi H, Kitakoji H: [Effects of acupuncture on Delayed Onset Muscle Soreness. -Clinical trial of tender point acupuncture treatment-]. Bull Meiji Univ Orient Med. 2005, 25: 11-17.
Takahashi K, Taguchi T, Itoh K, Okada K, Kawakita K, Mizumura K: Influence of surface anesthesia on the pressure pain threshold measured with different-sized probes. Somatosens Mot Res. 2005, 22 (4): 299-305. 10.1080/08990220500420475.
Acknowledgements
The authors wish to thank S Itoh for his comments on the manuscript, and S Kawamoto, H Fujiwara, A Nishida, T Nakano, Y Nanba and M Yamaguchi for their assistance in this study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
KI did the study design, acupuncture treatment and manuscript preparation. HO performed statistical analysis. HK did the study design, critical review of the manuscript and recruitment of subjects. All authors read and approved the final version of the manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Itoh, K., Ochi, H. & Kitakoji, H. Effects of tender point acupuncture on delayed onset muscle soreness (DOMS) – a pragmatic trial. Chin Med 3, 14 (2008). https://doi.org/10.1186/1749-8546-3-14
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1749-8546-3-14