
Abstract
Background
To investigate the interfraction displacement and volume variation of primary thoracic esophagus carcinoma with enhanced four-dimensional computed tomography (4DCT) scanning during fractionated radiotherapy.
Methods
4DCT data sets were acquired at the time of treatment simulation and every ten fraction for each of 32 patients throughout treatment. Scans were registered to baseline (simulation) 4DCT scans by using bony landmarks. The gross tumor volumes (GTVs) were delineated on each data set. Coordinates of the GTV centroids were acquired on each respiration phase. Distance between center of the GTV contour on the simulation scan and the centers on subsequent scans were used to assess interfraction displacement between fractions. Volumes were constructed using three approaches: The GTV delineated from the maximum intensity projection (MIP) was defined IGTVMIP, all 10 GTVs were combined to form IGTV10, GTVmean was the average of all 10 phases of each GTV.
Results
Interfraction displacement in left-right (LR), anterior-posterior (AP), superior-inferior (SI) directions and 3D vector were 0.13 ± 0.09 cm, 0.16 ± 0.12 cm, 0.34 ± 0.26 cm and 0.43 ± 0.24 cm, respectively between the tenth fraction and simulation 4DCT scan. 0.14 ± 0.09 cm, 0.19 ± 0.16 cm, 0.45 ± 0.43 cm and 0.56 ± 0.40 cm in LR, AP, SI and 3D vector respectively between the twentieth fraction and simulation 4DCT scan. Displacement in SI direction was larger than LR and AP directions during treatment. For distal esophageal cancer, increased interfraction displacements were observed in SI direction and 3D vector (P = 0.002 and P = 0.001, respectively) during radiotherapy. The volume of GTVmean, IGTVMIP, and IGTV10 decreased significantly at the twentieth fraction for middle (median: 34.01%, 33.09% and 28.71%, respectively) and distal (median: 22.76%, 25.27% and 23.96%, respectively) esophageal cancer, but for the upper third, no significant variation were observed during radiotherapy.
Conclusions
Interfractional displacements in SI direction were larger than LR and AP directions. For distal location, significant changes were observed in SI direction and 3D vector during radiotherapy. For middle and distal locations, the best time to reset position should be selected at the twentieth fraction when the primary tumor target volume changed significantly, and it was preferable to guide target correction and planning modification.
Similar content being viewed by others

Background
Radiotherapy (RT) plays an important role in the treatment of esophageal cancer, the three-dimensional conformal radiotherapy (3D-CRT) and intensity-modulated radiotherapy (IMRT) are the most important delivery platforms [1, 2]. Precise definition of RT fields is crucial for RT planning. Variation of target volume and displacement are the sources for RT fields and plan modification, such changes can be intrafractional or interfractional. Intrafractional esophageal motion can be attributed mostly to respiration, cardiac activity, and esophageal peristalsis [3], which has been well documented [4–8]. But studies about interfractional esophageal motion were limited. As a consequence of radiation treatment, tumor volumes will change during radiotherapy, significant regression in lung tumor volume can occur by 3 weeks after beginning treatment [9–11]. But so far, no conclusive data exist as to the nature of the tumor volume changes during radiotherapy for primary esophageal cancer, or the time at which these changes occur.
Relative to three-dimensional computed tomography (3DCT), four-dimensional computed tomography (4DCT) scan could not only obtain the volume of primary tumor GTV without motion information, for example, the GTV delineated on a single phase; but also obtain internal gross tumor volume (IGTV) volume with entire motion information, for example, the IGTV combined from 10 phases. In addition, we also can obtain IGTVMIP from the maximum intensity projection (MIP). Therefore, based on repeated 4DCT, we can obtain more precise variation of target volume during entire treatment for primary esophageal cancer. In present study, we measured the interfractional displacement of the GTV, and variation of GTV/IGTV in conventional fractioned RT during treatment for primary esophageal cancer using repeated 4DCT.
Methods
Patient characteristics
A total of 32 patients with pathologically confirmed thoracic esophageal cancer were considered eligible for radiotherapy with 3DCRT or IMRT from August 2011 to October 2012. 32 patients completed the simulation 4DCT scan and the tenth fractional scan, 27 patients completed the twentieth fractional scan. Patients with poor pulmonary function or preexisting respiratory problems were excluded. Written informed consent was obtained from all of the patients before the treatment was initiated. The patient characteristics are listed in Table 1.
CT data acquisition
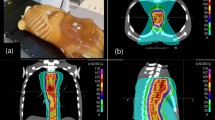
Every patient underwent a 4DCT scan on a 16-slice CT scanner (Philips Brilliance Bores CT, Netherlands). All of the patients were scanned in supine position with arms stretched over the head using the vacuum bag, followed by laser alignment. Metal marks were applied to the laser cross marked points in the bilateral axial midline and the anterior midline. Images were obtained from the neck to the mid-abdomen using the axial CT mode, and all these scans were gathered during free breathing (FB) without any breathing control. During the 4DCT image acquisition, the patient’s respiration was monitored using the Real-Time Position Management (RPM) Respiratory Gating System (Varian Medical Systems, Palo Alto, CA) by tracking the trajectory of the infrared markers placed on the patient’s abdomen. The signal was sent to the scanner to label a time tag on each CT image. GE Advantage 4D software (GE Healthcare, Waukesha, WI) sorts the reconstructed 4DCT images into ten respiratory phases labeled as 0% - 90% on the basis of these tags, with 0% corresponding to end inspiration (EI) and 50% corresponding to end expiration (EE). The 4DCT images were reconstructed using a thickness of 3 mm and then transferred to the Eclipse treatment planning system (TPS) (Eclipse 8.6, Varian Medical Systems, Palo Alto, CA) for structure delineation and treatment planning generation.
GTV delineation, volume and displacement determination
All of the 4DCT data sets of each patient were registered to the reference 4DCT scanning (the first 4DCT scan/simulation) corresponding to the end expiration phase (respiratory phase 50%, GTV50) using software tools in the radiation treatment-planning system on the basis of bony landmarks for comparison. For each 4DCT data set, the primary tumor (was considered as the GTV) was drawn by a single physician with same window level and window widths. The full respiration GTV centroid positions were acquired by the Varian Eclipse 8.6 treatment planning system. Volumes were constructed using three approaches: GTVmean was the average of all 10 phases of each GTV, IGTVMIP was the contour delineated from the MIP, all 10 GTVs were combined to form IGTV10. Displacement in each direction between the center of the GTV50 contour on the simulation scan and the centers on subsequent scans was used to assess interfraction displacement between fractions, which was obtained by coordinates of the GTV50 centroid on the subsequent datasets subtracted that on the reference dataset. In addition, the three dimensional tumor motion vector was obtained using motion data in the different axes.
Statistical analysis
The displacement among three directions and the displacement in the same direction among different locations during the same fraction were used by one-way ANOVA. The displacements on the same direction among all fractions and volumes among all fractions were used by a paired sample T test. Values of P < 0.05 were considered significant. All statistical analyses were performed using the SPSS software package.
Results
Comparison of the interfraction displacement for the tenth fraction 4DCT scan
For all of the patients, slightly larger displacements were observed in the SI direction with mean ± standard deviation (SD) of 0.34 ± 0.26 cm, compared with 0.13 ± 0.09 cm (P = 0.000) and 0.16 ± 0.12 cm (P = 0.001) in the LR and AP directions, respectively. The mean magnitude of the interfractional GTV centroid positional variations for the upper, middle, and distal esophageal cancer were summarized in Table 2. The displacements in the SI direction were also larger than LR and AP directions (P = 0.024, P = 0.028; P = 0.049, 0.047; P = 0.000, P = 0.001; respectively). The displacements in the distal location were larger than in the upper and middle tumor locations in the SI direction and the 3D vector.
Comparison of the interfraction displacement for the twentieth fraction 4DCT scan
For all of the patients, displacement in LR, AP, and SI direction were 0.14 ± 0.09 cm, 0.19 ± 0.16 cm, and 0.45 ± 0.43 cm, respectively. The displacement in SI direction was larger than LR (P = 0.001) and AP (P = 0.007) direction. The mean magnitude of the interfractional GTV centroid positional variations for upper, middle, and distal esophageal cancer were summarized in Table 3. The displacements in SI direction were also larger than in LR and AP directions (P = 0.011, P = 0.028; P = 0.048, 0.045; P = 0.000, P = 0.000; respectively). The displacements in the distal location were larger than in the upper and middle location in the AP, SI direction and the 3D vector.
Changes of interfraction displacement of the GTV centroid during treatment
For the upper and middle tumor locations, no significant differences were found in each direction and the 3D vector. For the distal esophageal cancer, significant differences were observed in SI direction and the 3D vector (P = 0.002 and P = 0.001, respectively) during radiotherapy.
Variation of tumor volumes
The tumor volumes variation of the GTVmean, the IGTVMIP and the IGTV10 during radiotherapy are listed in Table 4. The tumor volume showed a trend of decline during the entire treatment, the change trend of GTVmean, IGTVMIP, and IGTV10 are completely consistent. At the tenth fraction, the volume of GTVmean, IGTVMIP, and IGTV10 decreased, but the variations are not significant compared to primary volumes for the upper, middle and distal tumor locations. For the GTVmean, volumes are increased 22.41% in 7 of 32 patients (range, 4.20%-39.42%), differences are statistically significant (P = 0.003). At the twentieth fraction, tumor volumes shrink further more, for all of the tumors, the volume of GTVmean, IGTVMIP, and IGTV10 decreased significantly relative to those of primary volumes (P = 0.000, P = 0.000 and P = 0.000, respectively). For the middle location, the GTVmean volume decreased 34.01% (range, 13.45%-63.28%, P = 0.009), IGTVMIP 33.09% (range, 6.00%-58.00%, P = 0.007), IGTV10 28.71% (range, 2.00%-54.00%, P = 0.012). For the distal esophageal cancer, GTVmean volume decreased 22.76% (range, 14.01%-50.64%, P = 0.047), IGTVMIP 25.27% (range, 9.00%-48.00%, P = 0.024), IGTV10 23.96% (range, 11.00%-51.00%, P = 0.029). But for the upper location, no significant reduction to the volume of GTVmean, IGTVMIP, and IGTV10 (P = 0.079, P = 0.082, and P = 0.164, respectively). Figure 1 showed the absolute volumetric changes of the GTVmean during 3DCRT/IMRT.

Absolute volumetric changes of GTV mean during 3DCRT/IMRT (n = 32).
Discussion
The accurate definition of a target is crucial for the delivery of high-precision radiotherapy in esophageal cancer. The planning target volume (PTV) is defined as the clinical target volume plus an internal margin (IM) that includes the target internal motion and daily setup error (SM) [12]. Some researchers have reported that the tumor position varies intrafractionally, but interfractional displacement and tumor volume variation during radiotherapy were limited. The aim of this study was to introduce interfraction displacement and regression of tumor volume over entire treatment for primary esophageal cancer.
Interfractional displacement is defined as displacement of the tumor position relative to its position at simulation between fractions, reports of which have been limited. In this study, we analyzed interfraction displacement not only in whole esophagus but also in upper, middle, and distal esophagus. In addition, we compared the displacement on same direction among different locations, and the displacement on same direction over entire treatment.
In the present study, interfractional displacement in the SI direction is larger than LR and AP direction whether for whole esophagus or different locations during entire course of treatment (Table 2 and Table 3). These results are consistent with the reported data from Wang et al. [13], who used 4DCT to analyze interfractional displacement for 22 esophageal malignancy patients at the end expiration phase. They demonstrated that the interfractional displacement of the gastroesophageal junction (GEJ) in the SI, AP, and LR directions were 6.77 mm (maximum displacement, 17.6 mm), 2.90 mm and 2.88 mm, respectively. They also confirmed that the interfractional systematic displacement in the SI direction correlated strongly with the interfractional change in tidal volume (r = 0.9635) and vertical diaphragmatic displacement (r =0.9437). Perhaps this is the reason why displacement in the SI direction is larger than in the LR and AP direction. Cohen et al. [14] used CT-on-rails to study 8 patients with esophageal tumors and found a mean absolute esophageal displacement of 3.2 mm below and 4.2 mm above the carina in the LR direction and a mean absolute AP displacement of 2.8 mm posterior below and 3.9 mm posterior above the carina. Another study [15] using cone-beam CT to analyze esophageal shifts in 20 patients with esophageal cancer showed similar 5 mm in the LR direction and 5 mm in the AP direction. However, the two studies above did not address interfractional esophageal motion in the SI direction. The study from Wang et al. [13] did include the SI direction, but they limited their study to the GEJ and did not divide the esophagus into different segments.
In our study, we found displacement in the SI direction and 3D vector in the distal location were larger than upper and middle third esophagus during radiotherapy. This finding suggests that displacement in the distal esophagus is large, especially in the SI direction. Wang’s study [13] also found large interfractional SI displacements. We also analyzed displacement variation on the same direction over entire treatment. For the upper and middle locations, no significant differences were found in each direction and 3D vector. For the distal esophageal cancer, significant differences were observed in the SI direction and 3D vector (P = 0.002 and P = 0.001, respectively) during radiotherapy. Along with treatment, the displacement in SI direction (0.86 ± 0.39 cm vs 0.51 ± 0.25 cm) and 3D vector (0.96 ± 0.36 cm vs 0.59 ± 0.22 cm) for distal patients increased. Suggesting that expanding margin reasonably in SI direction is needed for the distal patients at the twentieth fraction. Wang et al. [13] analyzed one patient who had the largest inferior systematic displacement; the CTV was underdosed, which resulted in higher-than-expected doses to the GEJ, and these hot spots also affected exposure to the normal stomach and lung. Their findings thus justified at least a 10 mm inferior PTV margin. This reminds us that we must pay great attention to interfractional displacement at the twentieth fraction, particularly for distal patients, to prevent a high radiation dose to the normal tissues and an insufficient dose to the target.
Monitoring the regression and deformation for tumor volume could help revise the target and treatment plan in time. In this study, we found the majority of the tumor volumes were decreased with increasing fractions during radiotherapy based on repeated 4DCT scanning. However, at the tenth fraction, the volume of the GTVmean increased 22.41% in 7 of 32 patients (range, 4.20%-39.42%). Similar to our study, Britton et al. [10] used 4DCT to assess GTV regression during radiotherapy for non-small-cell lung cancer; they showed a transient increased in the GTV volume for 5 patients during the first or second week of treatment. The case was also observed in intracranial lesions [16–22]. In the process of sketch, we found that the tumor and esophageal mucosa nearby thickened locally, but by only relying on CT imaging, we cannot judge whether the increase is caused by oedema or infiltration. Therefore, according to the studies above, clinicians should pay attention to tumor volume change at the initial treatment, because target mispositioning will result in a high radiation dose to the normal tissues and an insufficient dose to the target.
Along with the progress of radiotherapy treatment, the tumor size decreased significantly. In our study, except for upper third esophagus, the GTVmean, IGTVMIP, and IGTV10 of middle and distal esophageal cancer decreased significantly at the twentieth fraction. Studies on lung cancer concluded that significant changes in the target volume occurred after 2 weeks. For example, A study from Underberg et al. [23], who identify potential time trends in target volumes and tumor mobility after stereotactic radiotherapy (SRT) for Stage I non–small-cell lung cancer in 40 tumors, showed that GTV and ITV decreased significantly at the fourth week after the start of treatment (P < 0.015). In our study, we found the larger the absolute initial tumor volume, the greater the absolute tumor volume shrinking. In the present study, the tumor volume in the upper third is smaller than that of mid- and distal segment (P = 0.003), perhaps this is the reason to the differentiation of volume change in different locations. Our study showed that the tumor volume in 2 patients increased continuously over entire course of treatment. We analyzed the probable causes may be related to image artifacts affecting the numbers of slices contoured. We could not rule out the cause of the tumor growth.
In addition, a similar time trend as for the GTVmean was observed for the IGTV10 and IGTVMIP, with an overall decrease during radiotherapy. Just as the GTVmean, the volumes also decreased significantly at the twentieth fraction. IGTV10 was fused by GTVs on ten phases, contained mobility information of entire respiratory cycle [24, 25]. Our results show that the GTV or IGTV volume changes significantly at the twentieth fraction of treatment, suggesting the need for reimaging and potential replanning for some patients.
Conclusions
We investigated the interfraction displacement and tumor volume variation during radiotherapy for primary esophageal cancer. Larger displacement in SI direction was observed, significant variation were exist in SI direction and 3D vector for distal esophageal cancer during radiotherapy. Tumor volume decreased significantly at the twentieth fraction. Therefore, for primary middle and distal esophageal cancer, the best time to reset the position may be at the twentieth fraction when the primary tumor target volume changed significantly. Resetting the position is recommended to guide the target correction and treatment planning modification.
Abbreviations
- 4DCT:
-
Four-dimensional computed tomography
- IGTV:
-
Internal gross tumor volume
- MIP:
-
Maximum intensity projection
- LR:
-
Left-right
- AP:
-
Anterior-posterior
- SI:
-
Superior-inferior
- PTV:
-
Planning target volume
- RPM:
-
Real time positioning management
- TPS:
-
Treatment planning system
- SD:
-
Standard deviation
- 3D-CRT:
-
Three-dimensional conformal radiotherapy
- IMRT:
-
Intensity-modulated radiotherapy.
References
Wu VW, Sham JS, Kwong DL: Inverse planning in three-dimensional conformal and intensity-modulated radiotherapy of mid-thoracic esophageal cancer. Br J Radiol 2004, 77: 568-572. 10.1259/bjr/19972578
Chandra A, Guerrero TM, Liu HH, Tucker SL, Liao Z, Wang X, Murshed H, Bonnen MD, Garg AK, Stevens CW, Chang JY, Jeter MD, Mohan R, Cox JD, Komaki R: Feasibility of using intensity-modulated radiotherapy to improve lung sparing in treatment planning for distal esophageal cancer. Radiother Oncol 2005, 77: 247-253. 10.1016/j.radonc.2005.10.017
Hashimoto T, Shirato H, Kato M, Yamazaki K, Kurauchi N, Morikawa T, Shimizu S, Ahn TC, Akine Y, Miyasaka K: Real-time monitoring of a digestive tract marker to reduce adverse effects of moving organs at risk (OAR) in radiotherapy for thoracic and abdominal tumors. Int J Radiat Oncol Biol Phys 2005, 61: 1559-1564. 10.1016/j.ijrobp.2005.01.006
Lorchel F, Dumas J, Noel A, Wolf D, Bosset JF, Aletti P: Esophageal cancer: determination of internal target volume for conformal radiotherapy. Radiother Oncol 2006, 80: 327-332. 10.1016/j.radonc.2006.08.003
Zhao KL, Liao Z, Bucci MK, Komaki R, Cox JD, Yu ZH, Zhang L, Mohan R, Dong L: Evaluation of respiratory-induced target motion for esophageal tumors at the gastro-esophageal junction. Radiother Oncol 2007, 84: 283-289. 10.1016/j.radonc.2007.07.008
Yaremko BP, Guerrero TM, McAleer MF, Bucci MK, Noyola-Martinez J, Nguyen LT, Balter PA, Guerra R, Komaki R, Liao Z: Determination of respiratory motion for distal esophagus cancer using four-dimensional computed tomography. Int J Radiat Oncol Biol Phys 2008, 70: 145-153. 10.1016/j.ijrobp.2007.05.031
Patel AA, Wolfgang JA, Niemierko A, Hong TS, Yock T, Choi NC: Implications of respiratory motion as measured by four-dimensional computed tomography for radiation treatment planning of esophageal cancer. Int J Radiat Oncol Biol Phys 2009, 74: 290-296. 10.1016/j.ijrobp.2008.12.060
Yamashita H, Kida S, Sakumi A, Haga A, Ito S, Onoe T, Okuma K, Akahane M, Nakagawa K: Four-dimensional measurement of the displacement of internal fiducial markers during 320-multislice computed tomography scanning of thoracic esophageal cancer. Int J Radiat Oncol Biol Phys 2011, 79: 588-595. 10.1016/j.ijrobp.2010.03.045
Bosmans G, Baardwijk A, Dekker A, Dekker A, Ollers M, Boersma L, Minken A, Lambin P, De Ruysscher D: Intra-patient variability of tumor volume and tumor motion during conventionally fractionated radiotherapy for locally advanced non–small-cell lung cancer: a prospective clinical study. Int J Radiat Oncol Biol Phys 2006, 66: 748-753. 10.1016/j.ijrobp.2006.05.022
Britton KR, Starkschall G, Tucker SL, Pan T, Nelson C, Chang JY, Cox JD, Mohan R, Komaki R: Assessment of gross tumor volume regression and motion changes during radiotherapy for non–small-cell-lung cancer as measured by four-dimensional computed tomography. Int J Radiat Oncol Biol Phys 2007, 68: 1036-1046. 10.1016/j.ijrobp.2007.01.021
Juhler-Nøttrup T, Korreman SS, Pedersen AN, Persson GF, Aarup LR, Nystrom H, Olsen M, Tarnavski N, Specht L: Inter-fractional changes in tumour volume and position during entire radiotherapy courses for lung cancer with respiratory gating and image guidance. Acta Oncol 2008, 47: 1406-1413. 10.1080/02841860802258778
International Commission on Radiation Units and Measurements: ICRT report 62, prescribing, recording and reporting photon bream therapy (supplement to ICRU report 50). Bethesda: ICRU; 1999.
Wang J, Lin SH, Dong L, Balter P, Mohan R, Komaki R, Cox JD, Starkschall G: Quantifying the interfractional displacement of the gastroesophageal junction during radiation therapy for esophageal cancer. Int J Radiat Oncol Biol Phys 2012, 83: e273-e280.
Cohen RJ, Paskalev K, Litwin S, Price RA Jr, Feigenberg SJ, Konski AA: Esophageal motion during radiotherapy: quantification and margin implications. Dis Esophagus 2010, 23: 473-479. 10.1111/j.1442-2050.2009.01037.x
Yamashita H, Haga A, Hayakawa Y, Okuma K, Yoda K, Okano Y, Tanaka K, Imae T, Ohtomo K, Nakagawa K: Patient setup error and day-to-day esophageal motion error analyzed by cone-beam computed tomography in radiation therapy. Acta Oncol 2010, 49: 485-490. 10.3109/02841861003652574
Peterson AM, Meltzer CC, Evanson EJ, Flickinger JC, Kondziolka D: MR imaging response of brain metastases after gamma knife stereotactic radiosurgery. Radiology 1999, 211: 807-814. 10.1148/radiology.211.3.r99jn48807
Huber PE, Hawighorst H, Fuss M, van Kaick G, Wannenmacher MF, Debus J: Transient enlargement of contrast uptake on MRI after linear accelerator (linac) stereotactic radiosurgery for brain metastases. Int J Radiat Oncol Biol Phys 2001, 49: 1339-1349. 10.1016/S0360-3016(00)01511-X
Szeifert GT, Massager N, DeVriendt D, David P, De Smedt F, Rorive S, Salmon I, Brotchi J, Levivier M: Observations of intracranial neoplasms treated with gamma knife radiosurgery. J Neurosurg 2002,97(Suppl 5):623-626.
Nakamura H, Jokura H, Takahashi K, Boku N, Akabane A, Yoshimoto T: Serial follow-up MR imaging after gamma knife radiosurgery for vestibular schwannoma. Am J Neuroradiol 2000, 21: 1540-1546.
Chung WY, Pan DH, Shiau CY, Guo WY, Wang LW: Gamma knife radiosurgery for craniopharyngiomas. J Neurosurg 2000,93(Suppl. 3):47-56.
Bakardjiev AI, Barnes PD, Goumnerova LC, Black PM, Scott RM, Pomeroy SL, Billett A, Loeffler JS, Tarbell NJ: Magnetic resonance imaging changes after stereotactic radiation therapy for childhood low grade astrocytoma. Cancer 1996, 78: 864-873. 10.1002/(SICI)1097-0142(19960815)78:4<864::AID-CNCR25>3.0.CO;2-S
Tung GA, Noren G, Rogg JM, Jackson IM: MR imaging of pituitary adenomas after gamma knife stereotactic radiosurgery. Am J Roentgenol 2001, 177: 919-924. 10.2214/ajr.177.4.1770919
Underberg RW, Lagerwaard FJ, van Tinteren H, Cuijpers JP, Slotman BJ, Senan S: Time trends in target volumes for stage I non-small-cell lung cancer after stereotactic radiotherapy. Int J Radiat Oncol Biol Phys 2006, 64: 1221-1228. 10.1016/j.ijrobp.2005.09.045
Ezhil M, Vedam S, Balter P, Choi B, Mirkovic D, Starkschall G, Chang JY: Determination of patient-specific internal gross tumor volumes for lung cancer using four dimensional computed tomography. Radiat Oncol 2009, 4: l-14.
Kang Y, Zhang X, Chang JY, Wang H, Wei X, Liao Z, Komaki R, Cox JD, Balter PA, Liu H, Zhu XR, Mohan R, Dong L: 4D Proton treatment planning strategy for mobile lung tumors. Int J Radiat Oncol Biol Phys 2007, 67: 906-914. 10.1016/j.ijrobp.2006.10.045
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
JZW, JBL participated in the study design, contributed to the data collection, and draft the manuscript. WW, HPQ, ZFM and YJZ made important contributions in the design of the study and in revising the content. TYF, QS and MX contributed in collecting and analyzing data. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Wang, J.Z., Li, J.B., Wang, W. et al. Detection of interfraction displacement and volume variance during radiotherapy of primary thoracic esophageal cancer based on repeated four-dimensional CT scans. Radiat Oncol 8, 224 (2013). https://doi.org/10.1186/1748-717X-8-224
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1748-717X-8-224