
Abstract
Background
North-West of Pakistan is bestowed with medicinal plant resources due to diverse geographical and habitat conditions. The traditional use of plants for curing various diseases forms an important part of the region’s cultural heritage. The study was carried out to document medicinal plants used in Frontier Region (FR) Bannu, an area affected by the “War on Terror”.
Methods
Fieldwork was carried out in four different seasons (spring, autumn, summer and winter) from March 2012 to February 2013. Data on medicinal plants was collected using structured and semi-structured questionnaires from 250 respondents. The voucher specimens were collected, processed and identified following standard methods.
Results
Of the 107 species of ethnomedicinal plants reported, fifty percent species are herbaceous. The majority of the reported species were wild (55%) but a substantial proportion are cultivated (29%). For most of the plant species (34%), leaves are the most commonly used part in the preparation of ethnomedicines. The most common use of species is for carminative purposes (14 species), with the next most common use being for blood purification (11 species). The main methods used in the preparation of ethnomedicinal recipes involves grinding and boiling, and nearly all the remedies are taken orally along with ingredients such as water, milk or honey for ease of ingestion. Traditional healers prepare plant remedies using one or more plants. There was a significant correlation (r2 = 0.95) between the age of local people and the number of plants known to them, which indicates that in the coming 20 years, an approximate decrease of 75% in the indigenous knowledge may be expected.
Conclusion
Traditional medicines are important to the livelihoods of rural communities in the region affected by the Global war on Terrorism. The medicinal recipes are indigenous; however, there is a threat to their future use on account of rapid modernization and terrorist activities. Documentation of medicinal plants and recipes may help in the conservation of the regional indigenous medicinal knowledge for future generations and to provide a baseline for further studies.
Similar content being viewed by others


Introduction
Plants have been used as folk medicine all over the world for centuries [1] and indigenous communities have developed their own specific knowledge on plant resources, uses, management and conservation [2]. Ethnomedicinal treatment is not merely a medical system but part of a culture [3]. Today, around 25% of all prescribed medicines in the developed world contain ingredients derived from medicinal plants [4]. It has been estimated that herbal medicines are used by more than 80% of the world’s population in developing countries to meet their primary healthcare needs [5]. The traditional use of plants and plant resources is rapidly increasing due to their minimal side-effects and (affordable) accessibility, and because they sometimes represent the only source of healthcare available to poorer communities [6]. However, the key issue in the current era is the loss of indigenous medicinal plant and preparation knowledge, which can serve as a guideline on plant-based therapeutic research for many scientists around the world.
Pakistan has a diverse flora containing a total of 1,572 genera and 5,521 species, most of which are confined to the Hindukush, Himalaya and Karakorum regions [7, 8]. People collect about 600 medicinal plant species as one of the major non-timber forest products (NTFPs) [9]. Of these species, 500 are commonly used in traditional healthcare practices and 350 are traded for millions of US dollars to national and international markets [10]. Twenty-eight leading herbal manufacturing units use medicinal plants for making various preparations, which include 75 crude herbal drugs that are extensively exported. About 60,000 traditional practitioners (Hakeems) in rural and remote areas utilize medicinal plants as household remedies for curing several diseases [11]. Local communities have centuries of traditional knowledge and practice relating to plants of their regions that have been transmitted from generation to generation [12]. About 84% of the country’s population was dependent on traditional medicines in the early 1950’s [13]; however, the practice is now confined to remote areas [14].
This study has been carried out in the Frontier Region (FR) Bannu, which has suffered heavily due following the onset of the Global War on Terrorism. Various ethnomedicinal studies have been carried out [12, 15–18] in other regions of Pakistan; however, the FR has yet to be explored due to limited access. The area represents one of the country’s richest centers of biodiversity and it is a strong source of indigenous knowledge. Most of the population of the area is rural with a low literacy rate; hence they are more dependent upon natural resources, and especially on plants for their healthcare needs and livelihoods. War has crippled modern health facilities in the study area, which in turn has resulted in the spreading of gastrointestinal and skin related diseases among others. However, local people are increasingly using ethnomedicines to treat such diseases at the local level. Shinwari et al. [12] perceived a diminishing of indigenous knowledge due to the ever increasing influence of global commercialization and socio-economic transformation, and a dire need was expressed to preserve such knowledge on medicinal plants before it disappears. Hence, the present study was designed with the following objectives: (i) to identify and explore plant species that are being used locally for the treatment and prevention of various diseases; (ii) to document traditional recipes from medicinal plants including methods of preparation and modes of administration; and (iii) to investigate the current and future status of traditional knowledge among different age groups. The present study may help in the preservation of indigenous knowledge on ethnomedicines and provide baseline data for future studies.
Materials and methods
Study area
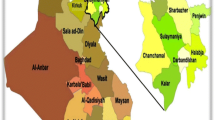
The present study was carried out in the Frontier Region (FR) Bannu located in the south of Khyber Pakhtunkhwa (KPK) Province, Pakistan (Figure 1). FR-Bannu consists of a total area of 877 square kilometers with a population of 19,593. The area lies within the Karakoram mountain range [19] between 32°-43 to 33°-06 N latitude and 73°-20 to 70°-07 E longitude. The total cultivated area is about 33,000 acres, with wheat, maize and sugarcane being the main cultivated crops [20]. About 25% of the inhabitants of the area as well as Afghan refugees are engaged in the collection and marketing of medicinal plants [20]. The area consists of alluvial plain with an annual rainfall of 111.36 mm [21]. The dominant plant species are Acacia modesta, Acacia nilotica, Calotropis procera, Dodonaea viscosa and Withania somnifera.

Map of the study area.
Sampling
Ethnomedicinal data was collected in four field visits per season in spring, autumn, summer and winter from March 2012 to February 2013. The methods for the collection of data and voucher specimens during the field study followed that described by Martin [22]. Initially, local administrative officers and representatives (Malik) of the study area were visited, who provided information on key resource persons in the field of medicinal plants. The key persons then suggested 269 potential respondents (local healers, rural herbalists and elders), all of whom were known in the community for their knowledge on medicinal plants and ethnomedicines. Prior to data collection, a brief group discussion was held with the respondents in order to gain their consent, to explain objectives of the research study and to assure them protection of their traditional knowledge. This was done to clarify the purpose of the research and to build confidence among respondents so that they would provide reliable information without holding any suspicion. Among the respondents, 19 were reluctant to provide any information leaving a total of 250 respondents being selected for data collection.
The biographic characteristics of the respondents in this study include age, gender and ethnic group. Of the 250 respondents, 201 were male and 49 female, and all belonged to one of three ethnic groups (Wazir, Banuchi or Afghan refugees). Due to customary restrictions in the study area, it was difficult to identify and gain access to a large number of females with knowledge on medicinal plants. The majority of the respondents were aged between 35 and 90 years and most (133) were Waziri, the largest ethnic group of the study area (Table 1). All the respondents and focal persons of the study area provided permission to publish and protect the data on traditional medicines provided by them.
Identification of medicinal plants used as ethnomedicines
Structured and semi-structured questionnaires were designed for data collection. For this purpose, individual interviews were held with each respondent in the local language of Pashto, which is spoken by all ethnic groups in the study area. More structured questionnaires were used to obtain specific information about medicinal plants of the study area, and informants were asked about the number of plants known to them, their local names, life-form, medicinal uses, occurrence, plant status and the most preferred part used for treatment [23]. Plant life-form implied herb, shrub or tree. Plant use referred to the use of either part of the plant or several parts and were categorized accordingly as whole plant, leaves, roots, bark, flowers, seeds, shoots, rhizomes and fruits. Plant status referred to the classification of plants across three categories, i.e. wild or cultivated or both.
Specimens of recorded medicinal plants were collected in their flowering and fruiting seasons during field visits and were processed in the laboratory using normal methods [22, 24]. Specimens were identified with the help of a plant taxonomist in the Department of Botany, Kohat University of Science and Technology (KUST). Following plant identification, specimens were pressed and dried in blotting sheets. Before mounting on the herbarium sheets, the plants were treated either with formaldehyde or mercuric chloride solution (0.5%) in order to protect plant material from insect or fungal damage. The scientific names, family names and names of publication authors were corrected according to the flora of Pakistan and software index kewensis [8, 25]. Identified plant specimens on herbarium sheets were placed in the herbarium at KUST.
Documentation of ethnomedicinal recipes
Semi-structured questionnaires were used to gather information on the mode of preparation and administration as well as information on typical compliments used with the ethnomedicines. The ailments treated were grouped into 21 types including febrifuge, carminative, stomach problems and chest infections among others. Questions on ethnomedicines inquired on modes of preparation (powder, boiled etc.), administration (oral or dermal), use of single or mixture of plants, ease of intake and other ingredients used such as water, sugar, milk and others. All the data collected through structured and semi-structured questionnaires were organized using Microsoft Excel.
Traditional knowledge and associated threats
Correlation between the age of the respondents and the number of medicinal plants known to them was analyzed using Pearson Correlation in SPSS [26]. Moreover, a conceptual diagram was developed in which the age groups in possession of indigenous knowledge were categorized and displayed showing current numbers (2013) and predicted numbers for 2023 and 2033. Data on the current status of indigenous knowledge was gathered during the present study while data for the next 10 and 20 years were predicted on the basis of a study by Shinwari [12], who predicted a 50% decline in indigenous medicinal plant knowledge among rural people for every 10 years due to modernization.
Results and discussion
The present study has recorded valuable ethnomedicinal knowledge from an area almost inaccessible due to the current armed conflict. Indigenous people from different localities have their own specific knowledge on the traditional utilization of medicinal plants [2] and our study highlights certain threats related to the disappearance of such knowledge. Medicinal plants represent a significant contribution to human health and it has been suggested that their use is one of the most significant ways in which humans directly reap the benefits provided from biodiversity [27].
Medicinal plants of the study area
In the war affected region of Pakistan, the use of folk remedies is a common practice and locals are highly dependent on the native flora for their healthcare needs. The inhabitants of the region use 107 plant species distributed across 90 genera and 56 families for the treatment of various ailments (Table 2). Such widespread use of medicinal plants for primary healthcare needs in the study area might be due to the lack of health facilities as a result of both increased armed conflict as well as cultural beliefs of the people who use ethnomedicines in the rural areas.
Figure 2 shows that herbs (53) and trees (32) are the most common life-form of the plants described by healers as having medicinal properties. The higher use of herbs for medicinal purposes in the study area may be due to their ease of collection, higher abundance and high effectiveness in the treatment of ailments in comparison to other life-forms [9], while in other regions it may also be due to seasonal variability or differences in socio-cultural beliefs and practices of healers. With regard to trees, their extensive use in the preparation of ethnomedicines might be linked to their ability to withstand long dry seasons, thus resulting in their availability throughout the year in arid and semi-arid areas [28].

Life form distribution of ethnomedicinal plants.
Results indicate that most of the study plants (55%) are collected from the wild to treat different diseases (Table 2). The basic reason behind using wild plants may be due to three reasons: i) The inhabitants of the region are not very well off; ii) In the current situation of war they are heavily dependent on medicinal plants; or iii) Such species are readily available at minimum cost near households as compared to cultivated plants. Giday and Tilahun [29] also found that in Ethiopia the use of wild plants is more common than the use of cultivated plants, and people also use wild medicinal plants for economic purposes. As a result, in our study area, economically valuable species such as Caralluma tuberculata and Nannorrhops ritchiana[30] which have the potential to be cultivated [20] for ecological restoration and rural livelihood are under threat due to over-collection.
Ethnomedicinal uses
The majority of plant species reported in the study area were used for carminative (14), blood purifying (11) or febrifuge (9) purposes, and each of the 8 species were used to treat stomach or chest problems (Figure 3). These findings are in line with other ethnobotanical studies [9, 31], where most plant species were reported to be used for the treatment of chest, fever or gastro-intestinal related diseases. Such diseases may have been recently exacerbated due to the increasing armed conflict and lack of security in the area, a lack of proper sanitation, or because of wood-fuel smoke inside houses. Moreover, the majority of people in the study have little or no access to safe drinking water, which may have increased the prevalence of waterborne diseases [32]. Gastrointestinal problems are not only common in the study area but are a common issue for the whole country. According to Ribeiro et al. [33], such diseases can result in higher mortality rates if not treated promptly. Results of the field surveys indicate that Acacia nilotica, Caralluma tuberculata, Convolvulus arvensis, Nannorrhops ritchiana, Withania somnifera and some other species are used for the treatment of more than one type of ailment. Our findings are in line with the ethnobotanical studies carried out by Badshah and Hussain [34] and Khan [35], who also reported various medicinal uses for the aforementioned plants. The multiple uses for each plant serve as a strong indicator of the natural availability of a variety of therapeutic phytochemicals within the plants, and such findings may prompt further research into their medicinal application.

Ethnomedicinal uses in the study area.
All parts of medicinal plants - including the leaves, stem, flower, bark, roots, fruits and seeds are used by traditional healers and local people, but the part of the plant collected for each specific purpose depends on the requirements of the user and type of plant. Figure 4 shows that 34% of plants were used for their leaves in the making of various medicinal preparations, which is easy to process into a digestible paste and have less conservational issues than the collection of roots, bark, stem or the whole plant [36]. The predominance of leaf use in the preparation of remedies has also been reported by Muthu et al. [37] and Kala et al. [38] and similar results have been reported from other areas of Pakistan [35, 39, 40].

Parts of the plants (%) used in the preparation of ethnomedicines.
Drying and pulverizing into powder, boiling for tea, juicing and pounding into a paste are the common preparation methods observed for our study area (Table 2). According to Deeba [41], grinding or crushing and boiling are the most common and effective methods of active ingredient extraction. While the majority of preparations of remedies in our study area involved the use of single plant, some of the remedies were prepared by combining different plants, for example, the powder of Acacia nilotica is mixed with the flowers of Punica granatum to be used for carminative purposes. Similarly, a mixture of leaves of Aloe barbadensis with the powder form of Curcuma longa is used to treat wounds, while the whole plant of Cynodon dactylon is mixed with leaves of Cannabis sativa and ground to powder for use against bleeding piles. According to traditional healers, complex medicines of two or more plant species are more potent than those prepared with a single species. The use of multiple therapies in traditional medicine based on combining plants has recently been shown to increase the efficacy of some herbal medicines [42]. According to Bussmann and Sharon [43], the use of more than one plant species to prepare a remedy for ailments is attributed to the additive or synergistic effects that they could have during ailment treatment. The method of drug preparation in many cases varies from individual to individual, while the same plant material for the same ailment may be prepared in different ways by different traditional healers. For example, in the present study the leaves and roots of Oxalis corniculata are used for stomach problems in powder form, but according to Murad et al. [44], the same plant is used for the same ailment in juice form in the Malakand district of Pakistan. Similarly, leaves of Cannabis sativa in boiled form are therapeutically very active against relieving pain in the study area, but the same plant is prepared in powder form to treat the same in the Swat region of Pakistan [5]. Such similarities in the cross-cultural usage of the traditional plant remedies are a strong indication of the bioactivity potential of the documented plant species. Table 2 shows that nearly all plant remedies are ingested orally in combination with other ingredients (vehicles) such as water, sugar, lime, wheat flour, mustard oil, honey, butter and milk to minimize the effect of the remedy’s astringent taste. It has been suggested that the use of such vehicles may dilute or reduce the relative potency of the drug [45]. However, there is no consensus on the dosage and frequency of the medication among healers because the dosage varies according to the type and severity of the illness or injury being treated.
Traditional knowledge and age of the respondents
Data analysis showed that there is a strong positive correlation (r2 = 0.95) between the respondent’s age and the number of medicinal plants known to them (Figure 5). In our study younger people up to 25 years old knew of approximately 15 medicinal plant species, which is far fewer than that of older people. Hussain et al. [46] in the South Waziristan and Parveen et al. [47] in the Thar Desert of India reported that people older than 30 years of age are more knowledgeable than younger ones in terms of medicinal plants and their uses. Ethnomedicinal recipes made by the local elders (collectors, traditional practitioners) are more effective than those made by young people [37, 47]. This may be partly explained by recent trends of modernization that have caused the level of information being directly transmitted between generations to be greatly reduced [9], and which may lead to the eventual disappearance of such knowledge and the weakening of the relationship between people and plants. Figure 6 represents a conceptual diagram that projects a decline in indigenous medicinal plant knowledge of around 75% in the coming 20 years. Another cause of such a decline may be related to the influence of increased armed conflict in the region. A large proportion of the inhabitants of the investigated area have recently migrated to urban areas, which may exacerbate any decline in indigenous knowledge as modernization and disinterest among youth in the urban areas has rendered traditional knowledge almost extinct [12]. Traditional knowledge is now confined to the remote areas of Pakistan [14], but various remote regions are vulnerable to annual climate-change-induced water scarcity and flooding and others problems such as financial crises, high transportation costs, increased prices of consumer goods, shortages of clean water, poor social networks and terrorism, all of which encourage the migration of a large proportion of the population toward urban areas. A study conducted by Cheikhyousaf et al. [48] showed that most of the healers in the region gained their knowledge from their grandparents. Considering the current high levels of youth migration from rural areas, such relationships are less likely to be formed across generations, resulting in the loss of medicinal plant knowledge when traditional healers pass away. As such, the documentation of traditional knowledge on ethnomedicinal uses is regarded as a necessity to safeguard future generations and encourage further research studies.

Pearson correlation between age of the respondents and the number of medicinal plants known to them.

A conceptual diagram on the current and future status of indegnous knowledge.
Conclusion
Traditional medicines serve as an integral source of rural livelihood in the study region in northwestern Pakistan, which is severely affected by armed conflict in the so-called War on Terror. The study area has plenty of medicinal plants to treat a wide spectrum of human ailments and local healers, although in decline, can be experts in the preparation of various ethnomedicinal remedies. Moreover, the use of specific plant parts, similar uses of same plants in different regions and multiple uses of single plants for the preparation of medicinal remedies suggest the prevalence of biologically active compounds across a range of medicinal plant species. Further phytochemical analysis, pharmaceutical application and clinical trials are therefore recommended in order to evaluate the authenticity of ethnomedicines to scientific standards. Indigenous knowledge on ethnomedicinal preparations persist more among older traditional healers, however, such knowledge is being lost to younger generations and continuing armed conflict in the region may further inhibit the transition of such knowledge. As such, studies on the documentation of ethnomedicines may be extended to other war-affected areas for the protection of traditional knowledge.
References
Smitherman LC, Janisse J, Mathur A: The use of folk remedies among children in an urban black community: remedies for fever, colic, and teething. Pediatrics. 2005, 3: 297-304.
Cotton CM: Ethnobotany: Principles and Applications. 1996, New York: John Wiley and Sons, 412-
Thomas H: Indigenous knowledge, emanicipation and alination. J Knowledge Transfer Util. 1998, 1: 63-73.
Rao MR, Palada MC, Becker BN: Medicinal and aromatic plants in agro-forestry systems. Agroforestory Syst. 2004, 61: 107-122.
Akhtar N, Rashid A, Murad W, Bergmeier E: Diversity and use of ethno-medicinal plants in the region of Swat, North Pakistan. J Ethnobiol Ethnomed. 2013, 9: 25-10.1186/1746-4269-9-25.
Acharya KP, Acharya R: Ethnobotanical study of medicinal plants used by Tharu Community of Parroha VDC, Rupandehi District, Nepal. Scientific World. 2009, 7: 80-84.
Sheikh K, Ahmad T, Khan MA: Use, exploitation and prospects for conservation: people and plant biodiversity of Naltar Valley, northwestern Karakorums, Pakistan. Biodivers Conserv. 2002, 11: 715-742. 10.1023/A:1015584202121.
Ali SI, Qaiser M: Flora of Pakistan. No 1–215 (1972–2010), Pakistan, http://www.efloras.org/flora_page.aspx?flora_id=5, accessed on 9 November, 2010
Adnan M, Begum S, Latif A, Tareen AM, Lee LJ: Medicinal plants and their uses in selected temperate zones of Pakistani Hindukush- Himalaya. J Med Plants Res. 2012, 6: 4113-4127.
Ahmad H: Capacity building for cultivation and sustainable harvesting of medicinal and aromatic plants. Proceeding of international workshop on conservation and sustainable uses of medicinal and aromatic plants in Pakistan, WWF Pakistan. Edited by: Ahmad H, Khan AA. 2003, 31-36.
Hamayun M: Studies on Ethnobotany, conservation and plant diversity of Utror and Gabral valleys, district Swat, Pakistan. 2004, Pakistan: Quaid-i-Azam University Islamabad, PhD thesis
Shinwari ZK: Medicinal plants research in Pakistan. J Med Plants Res. 2010, 4: 161-176.
Hocking GM: Pakistan medicinal plants. Qualitas Plantarium Ethnobotanical Material Vegetablies. 1958, 5: 145-153. 10.1007/BF01099867.
Ibrar M, Hussain F, Sultan A: Ethnobotanical studies on plant resources of Ranyal Hills, District Shangla, Pakistan. Pak J Bot. 2007, 2: 329-337.
Hamayun M, Khan SA, Kim HY, Leechae IJ: Traditional knowledge and ex-situ conservation of some threatened medicinal Plants of Swat Kohistan. Pak J Bot. 2006, 2: 205-209.
Jabeen A, Khan AM, Ahmad M, Zafar M, Ahmad F: Indigenous uses of economically important flora of Margallah hills national park, Islamabad, Pakistan. Afr J Biotechnol. 2009, 5: 763-784.
Gilani SS, Shinwari ZK: Sustainable harvest of medicinal plants at Bulashbar Nullah, Astore (Northern Pakistan). J Ethnopharmacol. 2003, 84: 289-298. 10.1016/S0378-8741(02)00333-1.
Haq F, Ahmad H, Alam M: Traditional uses of medicinal plants of Nandiar Khuwarr catchment (District Battagram), Pakistan. J Med Plants Res. 2011, 1: 39-48.
Haq F, Ahmad H, Alam M, Ahmad IB: Species diversity of vascular plants of Nandiar valley western Himalaya, Pakistan. Pak J Bot. 2010, 42: 213-229.
Samreen : Some of the ethnomedicinaly important plants of FR-Bannu region, KPK, Pakistan. Master Thesis. 2009, Pakistan: Bannu University
Jehanzeb K, Rooman K, Rizwana Aleem Q: Ethnobotanical Study of Commonly Used Weeds of District Bannu, Khyber Pakhtunkhwa (Pakistan). J Med Plant Stud. 2013, 2: 1-6.
Martin GJ: Ethnobotany: A methods manual. 1995, London: Chapman and Hall
Waller DP: Methods in ethnopharmacology. J Ethnopharmacol. 1993, 38: 189-195. 10.1016/0378-8741(93)90016-X.
Kim H, Song MJ: Ethnobotany. 2008, World Science Com: In Seoul
Index Kewensis 2.0: On compact disc version 2.0 for the IBM PC. 1997, United Kingdom: Oxford University Press
Maroyi A, SPSS Inc: SPSS Version 16.0 for Windows. SPSS, Chicago IL 2007: Traditional use of medicinal plants in south-central Zimbabwe: review and perspectives. J Ethnobiol Ethnomed. 2011, 9: 31-
Bannister K, Prophet River Ethnobotany: A report on traditional plant knowledge and contemporary concerns of the Prophet River First Nation. 2006, Northeastern British Colombia: Prophet River First Nation and Prophet River Contracting Ltd, 1-53.
Maroyi A: Traditional use of medicinal plants in south-central Zimbabwe: review and perspectives. J Ethnobiol Ethnomed. 2011, 9: 31-
Giday M, Teklehaymanot T: Ethnobotanical study of plant used in management of livestock health problems by Afar people of Adaar District, Afar Regional State, Ethiopia. J Ethnobiol Ethnomed. 2013, 9: 18-10.1186/1746-4269-9-18.
Sher Z, Khan DUZ, Hussain F: Ethnobotanical studies of some plants of Chagharzai valley, district Buner, Pakistan. Pak J Bot. 2011, 3: 1445-1452.
Khan AA: Role of conservation of medicinal and aromatic plants in the socioeconomic development of rural poor’s. International workshop on conservation and sustainable uses of medicinal and aromatic plants in Pakistan. Joint venture by WWF-Pakistan, MINFAL and Qarshi Industries Pvt. Ltd. 2003, Lahore, Pakistan: Ihsan Printers
Azizullah A, Khattak MNK, Richter P, Häder PD: Water pollution in Pakistan and its impact on public health. Environ Int. 2011, 37: 479-497. 10.1016/j.envint.2010.10.007.
Ribeiro A, Romeiras MM, Tavares J, Faria MT: Ethnobotanical survey in Canhane village, district of Massingir, Mozambique: medicinal plants and traditional knowledge. J Ethnobiol Ethnomed. 2010, 6: 33-10.1186/1746-4269-6-33.
Badshah L, Hussain F: People preferences and use of local medicinal flora in District Tank, Pakistan. Med Plants Res Pakistan. 2011, 1: 22-29.
Khan N, Ahmed M, Ahmed A, Shaukat SS, Wahab M, Ajaib M, Siddiqui MF, Nasir M: Important medicinal plants of Chitral Gol National Park (Cgnp) Pakistan. Pak J Bot. 2011, 2: 797-809.
Ticktin T: The ecological implications of harvesting non-timber forest products. J Appl Ecol. 2004, 41: 11-21. 10.1111/j.1365-2664.2004.00859.x.
Muthu C, Ayyanar M, Raja N, Ignacimuthu S: Medicinal plants used by traditional healers in Kancheepuram District of Tamil Nadu, India. J Ethnobiol Ethnomed. 2006, 2: 43-10.1186/1746-4269-2-43.
Kala CP: Ethnomedicinal botany of the Apatani in the eastern Himalayan region of India. J Ethnobiol Ethnomed. 2005, 1: 11-18. 10.1186/1746-4269-1-11.
Murad W, Azizullah A, Adnan M, Tariq A, Khan KU, Waheed S, Ahmad A: Ethnobotanical assessment of plant resources of Banda Daud Shah, District Karak, Pakistan. J Ethnobiol Ethnomed. 2013, 9: 77-10.1186/1746-4269-9-77.
Shinwari ZK, Rehman M, Watanabe T, Yoshikawa Y: Medicinal and Aromatic Plants of Pakistan. 2006, A Pictorial Guide: Kohat University of Science and Technology, Kohat, Pakistan
Deeba F: Documentation of ethnoveterinary practices in urban and peri-urban areas of Faisalabad, Pakistan. 2009, Faisalabad Pakistan: University of Agriculture, PhD Thesis
Zonyane S, Van Vuuren SF, Makunga NP: In Paper presented at South Africa Association of Botanist 38th Annual Conference, 15–18 January 2012. Pharmacological and phyto-chemical analysis of a medicinal plant mixture that is used as traditional medicine in Western Cape. 2012, Pretoria: University of Pretoria, 124-
Bussmann RW, Sharon D: Traditional medicinal plant use in Northern Peru: tracking two thousand years of healing culture. J Ethnobiol Ethnomed. 2006, 2: 47-10.1186/1746-4269-2-47.
Murad W, Ahmad A, Gilani SA, Khan MA: Indigenous knowledge and folk use of medicinal plants by the tribal communities of Hazar Nao Forest, Malakand District, North Pakistan. J Med Plants Res. 2011, 7: 1072-1086.
Jabbar A, Raza MA, Iqbal Z, Khan N: An inventory of the ethnobotanicals used as anthelmintics in the southern Punjab (Pakistan). J Ethnopharmacol. 2006, 108: 152-154. 10.1016/j.jep.2006.04.015.
Hussain M, Shah GM, Khan MA: Traditional medicinal and economic uses of Gymnosperms of Kaghan valley, Pakistan. Ethnobotany leaflets. 2006, 10: 72-81.
Parveen , Upadhyaya B, Shikha R, Ashwani K: Traditional uses of medicinal plants among the rural communities of Churu district in the Thar Desert, India. J Ethnopharmacol. 2007, 113 (3): 387-399. 10.1016/j.jep.2007.06.010.
Cheikhyousaf A, Shapi M, Matengu K, Ashekele HM: Ethnobotanical study of indigenous knowledge on medicinal plant use by traditional healers in Oshikoto region, Namibia. J Ethnobiol Ethnomed. 2011, 7: 10-10.1186/1746-4269-7-10.
Acknowledgment
Staff at the Department of Botany, Kohat University of Science & Technology is highly acknowledged for their help and support. We also thank the local respondents for sharing their indigenous knowledge with us. Authors are thankful to Mouhammad Sherin Zaman and Prof. Hashim Khan (community representatives) for giving permission to collect data. The authors owe thanks to Dr. Muhammad Naeem Butt and Dr. Syed Shujaat Ali, Kohat University of Science & Technology for language correction and academic support.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
MA designed the research project, conducted statistical analysis and provided comments on the draft manuscript. IU conducted the field work, wrote the draft manuscript and has equally contributed as first author with MA. AT analyzed the data and helped in writing the draft of the manuscript. AU, WM, NA and ALK provided comments and suggestions on the draft manuscript. All authors have read and approved the final manuscript.
Muhammad Adnan, Ihsan Ullah, Akash Tariq contributed equally to this work.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an open access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Adnan, M., Ullah, I., Tariq, A. et al. Ethnomedicine use in the war affected region of northwest Pakistan. J Ethnobiology Ethnomedicine 10, 16 (2014). https://doi.org/10.1186/1746-4269-10-16
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1746-4269-10-16