
Abstract
Objectives
To estimate the health-adjusted life expectancy (HALE) from diabetes mellitus (DM) using a population health survey linked to a population-based DM registry.
Methods
The 1996/97 Ontario Health Survey (N = 35,517) was linked to the Ontario Diabetes Database (N = 487,576). The Health Utilities Index (HUI3) was used to estimate health-related quality of life. HALE was estimated using an adapted Sullivan method.
Results
Life expectancy at birth of people with DM was 64.7 and 70.7 years for men and women – 12.8 and 12.2 years less than for men and women without DM. The HUI3 was lower for physician-diagnosed DM compared to self-reported DM (0.799 versus 0.872). HALE at birth was 58.3 and 62.8 years for men and women – 11.9 and 10.7 years less than that of men and women without DM.
Conclusions
The linked data approach demonstrates that DM is an important cause of disease burden. This approach reduces assumptions when estimating the prevalence and severity of disability from DM compared to methods that rely on self-reported disease status or indirect assessment of disability severity.
Similar content being viewed by others

Background
Summary measures of population health (SMPH) [1], which take into account both mortality and morbidity, fall into two major classes: positive measures of health expectancy [2] such as health-adjusted life expectancy (HALE) [3, 4], and measures of health gaps such as loss of healthy life years [5] or disability-adjusted life years (DALYs) [6]. Health expectancy, which is the focus of this study, represents life expectancy adjusted according to the amount of time spent in less than perfect health or with disability.
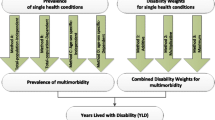
Three data components are needed to estimate all types of SMPH for specific conditions: mortality attributed to the condition; the prevalence or incidence and duration of the condition; and the degree to which health-related quality of life (HRQOL) is affected. While all SMPH commonly use the same source of mortality information, namely vital statistics, there are differences in how other components are measured. Health expectancy measures typically estimate the impact of chronic conditions on HRQOL from population-based health surveys. However, attributing HRQOL to different chronic diseases in population health surveys is difficult since self-reports of chronic disease status often underestimate the prevalence of many chronic conditions [7–11]. The best estimates of disease incidence or prevalence are achieved through population-based epidemiologic studies or disease registries, a method of estimating disease occurrence often used by health gap measures such as DALYs [6]. However, health gap measures also regularly use measures of HRQOL that have disability weights or levels of disabilities that are assigned by informed consumers, expert opinion or other epidemiologic sources that may not reflect the observed impact in specific populations.
In this study, we estimated HALE for people with diabetes mellitus (DM) in Ontario, Canada in 1996 to 1997 using a population health survey that was directly linked to a DM registry. This linkage overcomes the limitations of previous estimates of both health gaps and health expectancy by directly measuring both disease prevalence and HRQOL impact without relying on self-reported disease status or case scenarios of HRQOL that may not reflect the actual HRQOL of people with DM in Ontario.
Methods
Data sources
Cross-sectional data on HRQOL were derived from the 1996/97 Ontario Health Survey (OHS II) [12]. The Ontario Ministry of Health sponsored Statistics Canada to augment the Ontario sample of the 1996/97 National Population Health Survey (NPHS) to be able to produce reliable local-level estimates. 48,770 households were selected through stratified, multi-level cluster sampling of all private dwellings in Ontario, with local planning regions as the primary sampling unit. Residents of Indian reserves, long-term care institutions, prisons, remote areas and Foreign Service personnel were excluded. Respondents were contacted in person at their dwelling or by telephone. The actual survey was a telephone interview with two components, with data collection occurring between October 1996 and August 1997. A general component collected limited information on all members of the household; household response rate was 77.5%, or 37,796 households. The second component, which was the component used in this study, was administered to one randomly selected member from each survey household. The number of respondents who agreed to share their survey information with the provincial Ministry of Health was 37,247, a response rate of 98.5%. A further subgroup of survey respondents agreed to allow their survey responses to be linked to health care data; however, of the 35,517 (96.3%) who agreed to this, only 23,403 (65.6%) were linked to the central health administrative registry (the Registered Persons Database (RPDB), discussed later in this section) due to a technical difficulty resulting in missing OHS II demographic information. This technical problem did not bias the linkage process towards any particular group of respondents [13].
The OHS II, as part of the NPHS, was a two-stage probability sample. The final survey weight represents both the selection probabilities and post-stratification adjustments to match the sample to population characteristics [14]. A new survey weight was calculated specifically for the linkable portion of the survey. All analyses were weighted to represent the Ontario population in 1996–1997. To account for survey design effects, standard errors and coefficients of variation were estimated with the bootstrap technique [15–17].
Although the OHS II contained self-reported DM status, in this study the DM status of survey respondents was established by directly and individually linking them to the Ontario Diabetes Database (ODD) (N = 487,576 in 1997). The ODD is a population-based disease registry that was created through physician payment, hospital discharge data and the RPDB. The ODD has been validated in previous studies and found to be sensitive and specific for identifying persons with physician-diagnosed DM [18]. Approximately 95% of all people in Ontario who have physician-diagnosed DM are identified in the ODD. The algorithm used to create the ODD specified that any patient with two physician service claims bearing a diagnosis of DM within a two-year period, or one hospitalization with a diagnostic code for DM would be identified as having DM [18, 19]. Throughout this study we used this physician-diagnosed definition of DM status, unless otherwise noted, to estimate HRQOL, mortality, life expectancy and health expectancy.
The third linked data source used in the study was the RPDB, which contained basic demographic information on all persons eligible for health insurance coverage in Ontario. The RPDB is linked to vital statistics data collected by the Office of the Registrar General (156,610 deaths among Ontario residents during 1996 and 1997), thereby allowing for mortality estimates for people with and without DM. Approximately 93% of vital statistics deaths were linked to individual RPDP registrants. Age- and sex-specific adjustments were applied to correct for underestimation. Similar to other studies these all-cause deaths were used to estimate life and health expectancy for all Ontarians with and without DM [20–23]. Information on the cause of death from vital statistics is not known for people in RPDB. The death rate from DM as a main underlying cause of death for all Ontarians was obtained from Statistics Canada vital statistics data. The post-censal population estimates for 1996 and 1997 for each age and sex group were from Statistics Canada.
HRQOL Measure – The Health Utilities Index
The HRQOL measure used to calculate HALE in this study was the Health Utilities Index Mark 3 (HUI3) [24]. The HUI3 is a preference-based, multi-attribute health classification system that estimates a summary value of individual health where 0.0 = "dead" and 1.0 = "perfect health" (states worse than death are also possible), based on preference scores for different health states [25]. In many ways, the HUI3 is similar to other generic measures of HRQOL such as the Medical Outcomes Study 36-Item Short Form (SF-36) or the EuroQol Instrument (EQ-5D) [26, 27]. The HUI3 focuses primarily on the "within the skin" attributes of HRQOL, meaning the HUI3 aims to capture physical and mental functioning, as opposed to social participation [25, 28, 29]. Each OHS II respondent answered questions pertaining to eight attributes of functional health: vision, hearing, speech, mobility, dexterity, emotional state, cognition and level of pain and discomfort. Each attribute has from 5 to 6 possible levels ranging from unrestricted to a highly disabled state (see Torrance et al. [30] or the Health Utilities Group website [31] for a description of health states). The eight attributes are assigned utility weights and combined to create a summary value.
The process to establish attribute values and combine these values into a summary score involved a separate study [28]. This study randomly selected respondents from the general public. Respondents were asked to value different health states using a visual analogue scale and the standard gamble technique. The eight attributes were then combined using preference scores from the HUI3 using the following multi-attribute utility function where u is the utility for a chronic health state and b is single-attribute utility score [32] :
u = 1.371 (b 1 × b 2 × b 3 × b 4 × b 5 × b 6 × b 7 × b 8) - 0.371
The scoring system has the potential to create over 972,000 unique health states. 1995 unique health states were reported in respondents of the 1994/95 version of the NPHS [28].
Analysis methods
Diabetes-deleted mortality rate and HUI3 estimates
DM-deleted mortality rates were calculated by subtracting the mortality rate for people with physician-diagnosed DM from the overall mortality rate for each age-sex group. DM-deleted HUI3 was calculated in a similar manner by removing all people with physician-diagnosed DM from the OHS II sample and recalculating the mean HUI3 for each age-sex group.
Life table analysis
Period life tables for 1996–1997 for men and women were calculated using an adaptation of Chiang's method [33] and 20 standard age-groups (<1 year, 1–4 years, 5–9 years, ..., 90 years and older), except for an adaptation for the final age-group [34]. DM-deleted life expectancy was calculated by substituting the physician-diagnosed DM-deleted mortality rates for the overall mortality rates in the life table [35]. HALE was calculated using a modified Sullivan method [36]. Sullivan used a period life table and the prevalence of disability to estimate the number of life years lived free of disability. After calculating life tables for each group, HALE was estimated by weighting the years of life lived according to the mean HUI3 values by age and sex for each population. The physician-diagnosed DM-deleted mean HUI3 values were used to calculate DM-deleted HALE. Statistical errors for life expectancy and HALE were calculated using the methods of Chiang and Mathers, respectively [37, 38]. See Appendix 1 for Excel life tables used in this study.
Results
Table 1 compares methods for estimating DM status. 53.2% of people in the ODD (who had the disease diagnosed by a physician) reported that they did not have DM [18]. Those in the ODD who also self-reported DM had an HUI score that was lower than those who did not report DM (0.799 versus 0.872), although the age-standardized HUI3 estimates were similar. This suggests that the people with physician-diagnosed DM who did not self-report DM were younger and slightly healthier than people who reported they had DM, possibly because they had the condition for less time than people who reported they had DM. This comparison illustrates how estimating HALE using the HUI3 estimates for DM based on the ODD overcomes the limitations of previous health expectancy estimates that relied on self-reported DM status [23, 39].
Table 2 shows the mean HUI3 score for people with DM and the DM prevalence for different ages and health states. The weights were compared to the World Health Organization Global Burden of Disease (GBD) disability weights [6]. The GBD disability weights are scaled similarly to the HUI3 with death assigned a utility weight of 0 and 1 being perfect health. The GBD project assigned different weights for the complications of diabetic foot and blindness. While this would have been possible in our study for blindness and other complications, we instead estimated the mean HUI3 score for men and women with and without DM at different ages. We then assumed that the impact of DM on HRQOL was the difference between the mean HUI3 score for people with and without DM. The overall HUI3 score for DM (0.896 and 0.886 for men and women, respectively) was lower than the disability weight for uncomplicated DM in the WHO project (0.967). Indeed, the HUI3 score was similar for the WHO weight for diabetic foot (0.871). Since the overall prevalence of blindness in people with DM in this study was 0.1% and other complications such as diabetic foot are uncommon [40], they would have a very small influence in the overall DM HRQOL score in Ontario.
Table 3 shows mortality and HALE estimates for people with and without DM. Almost one quarter of all people who died in Ontario in 1996 and 1997 had DM (18,320 people per year). However, only 12.5% of the people who died in Ontario had DM identified as the underlying cause of death. The age-standardized death rate for people with DM was over twice that of people without DM (1,369 per 100,000 for men with DM versus 588 for men without DM; 1,315 per 100,000 for women with DM versus 533 for women without DM). This increased death rate translates into a life expectancy at birth 12.8 years less than for men without DM and 12.2 years less than women without DM. The estimates of life expectancy at birth combine the experience of people who have diabetes for varying lengths of time from early in life to older years. In addition, these estimates do not distinguish people with type 1 or 2 diabetes. The life expectancy at age 40 years (an age at which type 2 diabetes becomes the more common) for men with DM was 8.9 years less than for men without DM and 10.2 years less than women without DM. Life expectancy and HALE estimates for different age groups are shown in the Appendix (see Additional file 1).
HALE at birth was 58.3 years for men with DM, compared to 70.2 years for those without; and 62.7 years for women with DM compared to 73.5 years for those without DM. Given the present burden of disease, eliminating DM would extend overall life expectancy at birth in Ontario by 2.7 years, and would extend HALE by 3.2 years (Table 4).
Discussion
This study used linked databases containing population-based mortality, morbidity and DM prevalence to estimate life expectancy and HALE of people with and without DM. People with DM have a much lower life expectancy and HALE than people without DM. Furthermore, the life expectancy and HALE of the entire population would be substantially higher if DM were eliminated, demonstrating that DM is an important burden of disease in the Ontario population.
It is important not only to add "years to life", but also to add "life to years", meaning improvements in life expectancy should ideally be accompanied by improvements in HRQOL [41]. Efforts to prevent diseases that are fatal will add "years to life"; while reducing the prevalence of diseases that affect HRQOLwill add "life to years". DM has about the same impact on HRQOL as mortality in men and a larger HRQOL impact in women, suggesting that reducing or eliminating the disease has the potential to "compress morbidity" – meaning extra years of life would be lived in a state of improved HRQOL. This is in contrast to the impact of a reduction in the incidence of conditions that have a higher mortality burden than HRQOL burden, such as cancer, which has been predicted to cause an "expansion of morbidity", since people would live longer but in poorer health due to the onset of other conditions such arthritis [39, 42].
It is worth highlighting a few of the advantages of using linked databases when estimating SMPH. Disease registries that are linked to a current population health survey are well suited to measure morbidity from different conditions, as health surveys directly estimate the health status of a population at a defined time period. Health surveys that are repeated over time can monitor the progress of reducing morbidity in populations. These prevalence-based estimates of HRQOL for specific conditions yield the combined effect of duration and severity of disease along with the impact of health interventions or other health improvements. As the typical estimation of SMPH in the GBD usually uses different sources of information for each of these disease properties, their methods may have difficulty reflecting differences in the HRQOL impact of diseases in different populations and time periods. For an example of these differences, consider what would happen to HRQOL if a new DM medication was introduced that dramatically improved HRQOL. A population-based health survey would capture the current improvement. GBD DALYs, as commonly derived, would require further epidemiologic studies and expert opinion to readjust disability weights for treated people with DM and estimate the proportion of people treated with the new intervention. As there are many factors affecting disease morbidity in different populations that are constantly changing over time – such as socioeconomic conditions, physical and social environment, medical therapies, and health risk behaviour – it would seem unlikely that the current GBD approach could reflect the actual disease morbidity burden in any specific population.
Furthermore, since our linked databases include health administrative information about people who receive different health interventions (drug prescribing, physician consultations, hospital admissions, etc.), it may be possible to assess the health impact of specific interventions on the people who received those interventions [43, 44], or the total population [45].
An important limitation of this study is the omission of residents of long-term care facilities in the morbidity data used in the calculation of HRQOL impact. Berthelot and colleagues have shown that including these people would reduce population HRQOL utility estimates by up to 30% for women in the oldest age groups [46]. On the basis of their findings, the overall HALE estimates would be about 0.6 to 0.8 years lower if institutionalised people were included (calculations not shown). The bias resulting from excluding this population may be higher for conditions such as DM, which may be over-represented in institutions.
Health expectancy measures have been criticized because they are prevalence-based, which makes them less suited to monitoring trends in disease occurrence and the impact of disease prevention on future health [47, 48]. Because the DM registry used in this study contains information on disease incidence, prevalence and duration of disease, and age of death, it is possible to estimate the changing HRQOL impact over time and age based on either disease incidence or prevalence, thereby opening novel opportunities to improve estimates of summary measures (including health gap, health expectancy or hybrid measures) by considering the effect of changing disease incidence on future HRQOL [48].
An additional benefit of using linked data and population health surveys is the ability to adjust summary measure estimates for comorbidity (defined as the effect of a person's HRQOL being influenced by other chronic conditions) by various methods [39]. In this study, we adjusted for comorbidity by assuming the HRQOL burden of DM is equal to the difference in HRQOL between people with and without DM at the same age and sex. This method assumes that if DM were eliminated, the HRQOL would improve to the level of the remaining population, many of whom have other conditions. Although DALYs have been estimated considering co-morbidity, this is not usually done [37]. In the usual GBD approach, it is assumed that if DM were eliminated, people would have no disability at all – a situation that is particularly unlikely in older ages.
Finally, our method creates a tight association between the measurement of disease, HRQOL and mortality. The typical GBD method often defines different disability weights for different severities of disease, but these severity groups may not be congruent with the measurement of disease incidence. For example, if the definition of disease used to measure disease incidence is broad, thereby capturing people with mild disease, but the disability weight used is based on more severe disease, then the burden of disease will be overestimated. Such definitional differences have been reduced in our study because HRQOL is measured for people within the same disease registry used to estimate disease incidence and prevalence [42].
The increased mortality ratio in this study was similar to that observed in other populations [49]. Consequently, we observed a life expectancy difference between people with and without DM that was similar to other studies [20–22]. Care should be taken when making inferences from life expectancy estimates. Period life table estimates are summary descriptive measures created from cross-sectional data of open populations with a main assumption a stationary or steady-state population. This means that life expectancy for people with DM is estimated using people with varying time lengths of exposure to diabetes – in the same way that life expectancy of a country includes immigrants to that country, with a differing length of exposure to that county's health risks. In practical terms, estimates in this study should not be used to "predict" life expectancy, but instead to describe the mortality and health experience of people with and without DM. Similarly, a limitation of this study was the inability to differentiate type 1 and type 2 DM. The onset of illness is earlier for type 1 DM, therefore, the cumulative impact of type 1 DM on individual health is likely greater than for type 2 DM. However, the impact of DM on population health is strongly influenced by type 2 DM because it is much more prevalent than type 1 DM.
The cause-deleted life table approach assumes that if DM were eliminated the mortality rate and HRQOL burden for people who had DM would be the same as those without DM. It is possible that people with DM have a higher mortality rate or HRQOL burden from causes that are not directly related to DM – i.e. health behaviour such as hypertension and obesity – thereby resulting in our study overestimating of the population impact of DM. However, it should be noted that reduction in illness from these non-DM-related conditions may also be achieved if the prevalence of DM is reduced through health promotion or disease prevention that targets common risk factors for other disease. Therefore, reducing DM through these methods would potentially exceed the gains in life expectancy and HALE that we report. Vital statistics have been found to be a challenging data source to use for DM mortality studies since many DM deaths are identified as other conditions as the "underlying cause of death" [49]. Similar to other jurisdictions, Canada has begun systematically recording multiple causes of death, which will open opportunities to adjust for co-morbid conditions for mortality estimates in future studies.
There are limitations when estimating SMPH using information from population health surveys. Although there are at least 50 countries that have now conducted population health surveys, they are neither routinely repeated over time, nor easily comparable between populations and seldom have provisions for linkages to other data sources [50]. The latter omission makes it particularly difficult to apply the methods presented in this study in other jurisdictions. However, population health surveys linked to administrative data or disease registries can be an accurate method of ascertaining disease status and therefore provide a useful method of estimating population-based HRQOL for persons with chronic conditions such as DM. As such, they could be used to enhance and improve the estimates of the more subjective disability assignment and incidence or prevalence estimation exercises. The disability weights project in the Netherlands used health surveys and other sources to improve disability weights for their country and those improved disability weights have been used in other countries [51]. The approach used in this study is not well suited for acute conditions or other chronic conditions that cannot be accurately identified in population health surveys or linked registries and health care data.
This study has demonstrated that linked databases containing HRQOL and prevalence information can be used to estimate the large combined mortality and morbidity burden of diabetes. This is important, since there is a commitment in Ontario for regular routine large population health surveys (every two years with a sample size >40,000 respondents), so it will be possible to monitor progress in reducing the burden of diabetes and other diseases. With the approach of this study we can potentially measure the progress of reducing the large burden of disease from DM.
Abbreviations
- DALY:
-
DALY Disability-adjusted life year
- DM:
-
DM Diabetes mellitus
- GBD:
-
GBD Global Burden of Disease
- HALE:
-
HALE Health adjusted life expectancy
- HRQOL:
-
HRQOL Health-related quality of life
- HUI3:
-
HUI3 Health Utilities Index Mark III
- NPHS National Population Health Survey:
-
1996/97
- ODD:
-
ODD Ontario Diabetes Database
- OHS II Ontario Health Survey:
-
1996/97
- RPDB:
-
RPDB Registered Persons Database
- SMPH:
-
SMPH Summary measures of population health
References
Summary measures of population health: concepts, ethics, measurement and applications (Edited by: Murray CJL, Salomon J, Mathers CD and Lopez AD). Geneva, World Health Organization 2002.
Determining Health Expectancies (Edited by: Robine J-M, Jagger C, Mathers CD, Crimmins EM and Suzman RM). Chichester, UK, John Wiley & Sons Ltd. 2003.
Manuel DG, Goel V, Williams JI, Corey P: Health-adjusted Life Expectancy at the Local Level in Ontario. Chronic Dis Can 2000, 21: 73-80.
Wolfson MC: Health-adjusted life expectancy. Health Rep 1996, 8: 41-46.
Hyder AA, Rotllant G, Morrow RH: Measuring the burden of disease: healthy life-years. Am J Public Health 1998, 88: 196-202.
The Global Burden of Disease: a comprehensive assessment of mortality and disability from diseases, injuries, and risk factors in 1990 and projected to 2020 (Edited by: Murray CJ and Lopez AD). Washington, Harvard School of Public Health on behalf of the World Health Organization and the World Bank 1996.
Heliovaara M, Aromaa A, Klaukka T, Knekt P, Joukamaa M, Impivaara O: Reliability and validity of interview data on chronic diseases. The Mini-Finland Health Survey. J Clin Epidemiol 1993, 46: 181-191.
Beckett M, Weinstein M, Goldman N, Yu-Hsuan L: Do health interview surveys yield reliable data on chronic illness among older respondents? Am J Epidemiol 2000, 151: 315-23.
Gross R, Bentur N, Elhayany A, Sherf M, Epstein L: The validity of self-reports on chronic disease: Characteristics of underreporters and implications for the planning of services. Public Health Rev 1996, 24: 167-182.
Jabine TB: Reporting chronic conditions in the National Health Interview Survey. A review of findings from evaluation studies and methodological test. Vital Health Stat 2 1987, 1-45.
Moesgaard-Iburg K, Salomon J, Tandon A: Cross population comparability of self-reported and physician-assessed mobility levels: Evidence from the Third National Health and Nutrition Exam Survey. GPE Discussion Paper. Geneva, World Health Organization 2001., Evidence and Information for Policy Discussion Paper No. 14:
Canada Statistics: 1996-97 NPHS Public Use Microdata Documentation. Ottawa 1999.
Diabetes Health Status and Risk Factors Diabetes in Ontario: An ICES Practice Atlas (Edited by: Hux JE, Booth G, Slaughter PM and Laupacis A). Toronto, Institute for Clinical Evaluative Sciences 2003, 4.77-4.94.
Swain L, Catlin G, Beaudet MP: The National Population Health Survey--its longitudinal nature. Health Rep 1999, 10: 69-82.
Rao JNK, Wu CFJ, Yue K: Some recent work on resampling methods for complex surveys. Survey Methodology Ottawa, Statistics Canada 1992, 18: 209-217.
Rust KF, Rao JN: Variance estimation for complex surveys using replication techniques. Stat Methods Med Res 1996, 5: 283-310.
Yeo D, Mantel H, Liu TP: Bootstrap variance estimation for the National Population Health Survey. American Statistical Association: Proceedings of the Survey Research Methods Section. Baltimore, American Statistical Association 1999, 778-783.
Hux JE, Ivis F, Flintoft V, Bica A: Diabetes in Ontario: determination of prevalence and incidence using a validated administrative data algorithm. Diabetes Care 2002, 25: 512-516.
Blanchard JF, Ludwig S, Wajda A, Dean H, Anderson K, Kendall O, Depew N: Incidence and prevalence of diabetes in Manitoba, 1986-1991. Diabetes Care 1996, 19: 807-11.
Baan CA, Nusselder WJ, Barendregt JJ, Ruwaard D, Bonneux L, Feskens EJ: The burden of mortality of diabetes mellitus in The Netherlands. Epidemiology 1999, 10: 184-187.
Jagger C, Goyder E, Clarke M, Brouard N, Arthur A: Active life expectancy in people with and without diabetes. J Public Health Med 2003, 25: 42-46. 10.1093/pubmed/fdg009
Gu K, Cowie CC, Harris MI: Mortality in adults with and without diabetes in a national cohort of the U.S. population, 1971-1993. Diabetes Care 1998, 21: 1138-1145.
Narayan KM, Boyle JP, Thompson TJ, Sorensen SW, Williamson DF: Lifetime risk for diabetes mellitus in the United States. JAMA 2003, 290: 1884-1890. 10.1001/jama.290.14.1884
Feeny DH, Torrance GW, Furlong WJ: Health Utilities Index - Chapter 26. Quality of Life and Pharmacoeconomics in Clinical Trials Second Edition (Edited by: Spilder B). Philadelphia, Lippincott-Raven 1996.
Feeny D, Furlong W, Boyle M, Torrance GW: Multi-attribute health status classification systems. Health Utilities Index. Pharmacoeconomics 1995, 7: 490-502.
Coons SJ, Rao S, Keininger DL, Hays RD: A comparative review of generic quality-of-life instruments. Pharmacoeconomics 2000, 17: 13-35.
Hawthorne G, Richardson J, Day NA: A comparison of the Assessment of Quality of Life (AQoL) with four other generic utility instruments. Ann Med 2001, 33: 358-70.
Feeny D, Furlong W, Torrance GW, Goldsmith CH, Zhu Z, DePauw S, Denton M, Boyle M: Multiattribute and single-attribute utility functions for the health utilities index mark 3 system. Med Care 2002, 40: 113-128. 10.1097/00005650-200202000-00006
Organization World Health: International Classification of Function, Disability and Health: ICF Geneva, World Health Organization 2001, -299.
Torrance GW, Furlong W, Feeny D, Boyle M: Multi-attribute Preference Functions - Health Utilities Index. Pharmacoeconomics 1995, 7: 503-520.
Health Utilities Group /Health Utilities Index and Quality-of-Life http://www fhs mcmaster ca/hug/ 2004.
Furlong W, Feeny D, Torrance G, Barr R: The Health Utilities Index (HUI3) System for Assessing Health-Related Quality of Life in Clinical Studies. Health Economics and Policy Analysis Research Working Paper.
Chiang CL: The Life Table and Its Applications Malabar, Florida, Robert E. Krieger Publ. Co. 1984, 1-316.
Hsieh JJ: A general theory of life table construction and a precise abridged life table method. Biom J 1991, 33: 143-162.
Newman SC: Formulae for cause-deleted life tables. Stat Med 1987, 6: 527-8.
Sullivan DF: A single index of mortality and morbidity. HSMHA Health Reports 1971, 86: 347-54.
Mathers C, Vos T, Stevenson C: The burden of disease and injury in Australia. Canaberra, Australian Institute of Health and Welfare 1999., PHE17:
MP Fay, ER Feuer: Confidence intervals for directly standardized rates: A method based on the gamma distribution. Stat Med 1997, 16: 791-801. 10.1002/(SICI)1097-0258(19970415)16:7<791::AID-SIM500>3.3.CO;2-R
Manuel DG, Schultz SE, Kopec JA: Measuring the health burden of chronic disease and injury using health adjusted life expectancy and the Health Utilities Index. J Epidemiol Community Health 2002, 56: 843-850. 10.1136/jech.56.11.843
Hux JE, Jacka R, Fuug K, Rothwell D: Diabetes and Peripheral Vascular Diseases. An ICES Practical Atlas. Institute for Clinical Evaluative Sciences (Edited by: Hux JE, Booth G, Slaughter PM, Laupacis A. Toronto). 2003, 6:-.
Manuel DG, Schultz SE: Adding Life to Years and Years to Life: Life and Health Expectancy in Ontario. An ICES Atlas Report Toronto, Institute for Clinical Evaluative Sciences 2001.
Nusselder WJ, van der Velden K, van Sonsbeek JL, Lenior ME, van den Bos GA: The elimination of selected chronic diseases in a population: the compression and expansion of morbidity. Am J Public Health 1996, 86: 187-94.
Alter DA, Naylor CD, Austin P, Tu JV: Effects of socioeconomic status on access to invasive cardiac procedures and on mortality after acute myocardial infarction. N Engl J Med 1999, 341: 1359-67. 10.1056/NEJM199910283411806
Rochon PA, Tu JV, Anderson GM, Gurwitz JH, Clark JP, Lau P, Szalai JP, Sykora K, Naylor CD: Rate of heart failure and 1-year survival for older people receiving low-dose beta-blocker therapy after myocardial infarction. Lancet 2000, 356: 639-644. 10.1016/S0140-6736(00)02606-4
Heller RF, Dobson AJ: Disease impact number and population impact number: population perspectives to measures of risk and benefit. BMJ 2000, 321: 950-953. 10.1136/bmj.321.7266.950
Berthelot J-M, Roberge R, Wolfson MC: The calculation of health-adjusted life expectancy for a Canadian province using a multi-attribute utility function: a first attempt. Calculation of health expectancies: harmonization, consensus achieved and future perspectives (Edited by: Robine J-M, Mathers CD, Bone I and Romieu I). London, John Libbey and Company Ltd. 1993.
Barendregt JJ: Incidence- and Prevalence-based SMPH: Making the Twain Meet. Summary measures of population health: concepts, ethics, measurement and applications (Edited by: MurrayCJL, SalomonJ, MathersCD and LopezAD). Geneva, World Health Organization 2002, 221-222.
Murray CJ, Salomon JA, Mathers C: A critical examination of summary measures of population health. Bull World Health Organ 2000, 78: 981-994.
Chapter 11: Mortality in Non-Insulin-Dependant Diabetes Diabetes in America 2nd Edition Edition (Edited by: Harris MI, Cowie CC, Stern MP, Boyko EJ, Reiber GE and Bennet PH). Washington, DC, Government Printing Office; NIH Publication 95-1468 1995, 11: 233-257.
Sadana R, Mathers CD, Lopez AD, Murray CJL, Iburg K: Comparative Analyses of More Than 50 Household Surveys on Health Status. GPE Discussion Paper. Geneva, World Health Organization 2000, Evidence and Information for Policy Discussion Paper No. 15: 1-77.
Stouthard MEA, Essink-Bot M-L, Bonsel GJ, Barendregt JJ, Kramer PGN, van de Water HPA, van der Maas PJ, Gunning-Schepers LJ: Disability Weights for Diseases in The Netherlands. Rotterdam, Department of Public Health, Erasmus University Rotterdam 1997.
Acknowledgements
The authors would like to thank Jan Hux and Gillian Booth for comments on an earlier draft and assistance using the Ontario Diabetes Database, and the reviewers and editors for helpful suggestions.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
None declared.
Authors' contributions
Both authors contributed to all stages of the study including the conception, design, analysis and manuscript preparation. DM had major responsibly for the overall conception and completion of the study. Both authors read and approved the final manuscript.
Electronic supplementary material
12963_2003_16_MOESM1_ESM.xls
Additional File 1: This appendix contains the life tables that were used to calculate life expectancy and HALE for people with and without DM and for the Ontario population with and without DM eliminated. The life tables include estimates of statistical variation. These life tables can be used for several purposes such as: estimating life expectancy and HALE for different age-groups; estimating different life table functions such as probability of developing DM or surviving with DM for different age-periods; and as a spreadsheet template for the estimation of life and health expectancy for different populations, conditions or planning scenarios. To use the spreadsheet as a template for estimating life expectancy and HALE in different populations, the mortality and/or HRQOL estimates for the Ontario population can be substituted with age- and sex-specific mortality and/or HRQOL estimates of alternative populations. (XLS 262 KB)
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Manuel, D.G., Schultz, S.E. Using linked data to calculate summary measures of population health: Health-adjusted life expectancy of people with Diabetes Mellitus. Popul Health Metrics 2, 4 (2004). https://doi.org/10.1186/1478-7954-2-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1478-7954-2-4