
Abstract
Background
Cardiac resynchronisation therapy (CRT) improves mortality and morbidity in heart failure patients with wide QRS. Observational studies suggest that patients having more left ventricular dyssynchrony pre-implantation obtain greater benefit on ventricular function and symptoms with CRT.
Aim
To provide an analysis of the prevalence and type of dyssynchrony in patients included in the CARE-HF trial.
Methods
100 patients 67 (58 to 71) years were examined with echocardiography including tissue doppler imaging before receiving a CRT-pacemaker. Atrio-ventricular dyssynchrony (LVFT/RR) was defined as left ventricular filling time <40% of the RR-interval. Inter-ventricular mechanical delay (IVMD) was measured as the difference in onset of Doppler-flow in the pulmonary and aortic outflow tracts >40 ms. Intra-ventricular (regional) dyssynchrony in a 16-segment model was expressed either as a delayed longitudinal contraction (DLC) during the postsystolic phase or by tissue synchronisation imaging (TSI) with a predefined time-difference in systolic maximal velocities >85 ms.
Results
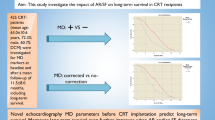
LVFT/RR was present in 34% and IVMD in 60% of patients while intra-ventricular dyssynchrony was present in 85% (DLC) and 86% (TSI) with a high agreement between the measures (Kappascore 0.86–1.00), indicating the methods being interchangeable. Patients with cardiomyopathy (53%) were more likely to have LVFT/RR <40% (45% vs. 21% (p= 0.02)) and more segments affected by intra-ventricular dyssynchrony 4(3, 5) vs. 3(1, 4), p = 0.002, compared to patients with ischemic heart disease.
Conclusion
The prevalence of intra-ventricular dyssynchrony is high in patients with heart failure, wide QRS and depressed systolic function. Most important, TSI appears to be a fast and reliable method to identify patients with intra-ventricular dyssynchrony likely to benefit from CRT.
Similar content being viewed by others

Background
Heart failure (HF) is common and despite recent advances in pharmacological therapy often debilitating [1–4]. Increased QRS duration on the surface electrocardiogram, reflecting regional delays in electrical activation, is present in more than one third of HF patients and has been associated with worse prognosis independent of the level of left ventricular (LV) ejection fraction (EF), rhythm and age [5]. Regional delays in electrical activation may cause regional delays in contraction and relaxation resulting in intra-ventricular dyssynchrony and a decline in ventricular function and efficiency [6]. However, QRS duration is probably only an approximate guide to the presence of dyssynchrony, Dyssynchrony can be classified as atrio-ventricular, inter-ventricular and intra-ventricular. There is some evidence that intra- but not inter-ventricular dyssynchrony predicts deaths or worsening heart failure in patients with idiopathic dilated cardiomyopathy (IDCM) [7, 8]. Assessment of cardiac dyssynchrony by imaging may identify the magnitude of the response to cardiac resynchronization therapy (CRT), in terms of improved cardiac function, symptoms and possibly prognosis, although data from relatively small observational studies must be interpreted with caution [9–12].
The aim of this study is to describe the prevalence of atrio-ventricular, inter-ventricular and intra-ventricular dyssynchrony by different Doppler techniques in patients with and without ischemic heart disease in a subpopulation of the CARE-HF trial.
Methods
Patients
The CARE-HF trial enrolled patients with New York Heart Association (NYHA) class III or IV despite pharmacological treatment, with a QRS duration ≥120 ms, LV ejection fraction (EF) ≤35%, LV end diastolic diameter ≥30 mm/m2 (height in m) and in sinus rhythm. Patients with a QRS duration between 120 ms and 149 ms required at least two of the following dyssynchrony criteria: (1) aortic pre-ejection delay >140 ms; (2) interventricular mechanical delay >40 ms; and (3) delayed activation of the posterolateral wall of the left ventricle as shown by any overlap between time from QRS to peak systolic movement of the posterior wall at m-mode and time from QRS to the beginning of the E-wave at pulsed Doppler transmitral flow. Patients with a QRS duration >150 ms did not require echo confirmation of dyssynchrony.
Of the 813 patients enrolled in the trial, 735 had an analysable echocardiographic examination. [13] including 92 patients with a QRS duration of between 120 ms and 149 ms. One-hundred patients aged 67.1 ± 10,4 years and randomized to the CARE-HF trial in five TDI interested and geographically close participating centers in Denmark, Germany and Sweden were eligible to the current sub study. The study was approved by the local ethics committees and all patients gave written informed consent.
Tissue Doppler echocardiography
Patients were examined in the left lateral position and tissue Doppler echocardiography was acquired in the apical 4 -chamber, 2-chamber and long-axis views using a VIVID-5 system with a 2,5 MHz transducer (GE-Vingmed Ultrasound, Horten, Norway). An average of 2–4 RR-intervals were stored as a cine loop (from p-wave to p-wave) on an optical disc for later off-line analysis (Echo-Pac Software, GE-Vingmed Ultrasound, Horten, Norway). Systole was defined as the ejection time from opening until closure of the aortic valves as measured by tissue velocity imaging (TVI) in the apical long-axis view [14]. The time from onset of the QRS-complex until opening of the aortic and pulmonary valves were defined as the pre-ejection periods. From the TVI loops colour Doppler TVI analysis was performed in each of the apical views. The 16 segment LV-model of the American Society of Echocardiography was used for regional analysis of the extent of dyssynchrony [15]. The extent of dyssynchrony during systole was evaluated regionally by tissue synchronisation imaging (TSI) (Figure 1). The TSI-start was set to the aortic valve opening and the TSI-end to the aortic valve closure and the TSI cut-off value was preset to 85 ms. This cut-off value, assumed to indicate important intra-ventricular dyssynchrony, was chosen based on the application of the method in previous patients in our echo-laboratory, and now tested in a prospective trial.

TVI-, DLC-curves and TSI illustrating dyssynchrony. TVI curves (left) showing late systolic peak velocity in the posterior segments (yellow and blue). TSI (right), is a signal-processing algorithm of the tissue Doppler data to automatically detect peak positive velocity and then colour-code the time to peak velocities in green for normal timing, yellow-orange for moderate delay, and red for severe delay, in peak velocity showing dyssynchrony (orange) in the corresponding posterior segments and SR curves showing delayed longitudinal contraction (DLC, yellow) in the same segment after aortic valve closure (AVC).
Presence or absence of delayed longitudinal contraction (DLC), i.e. motion towards the apex following closure of the aortic valve was recorded by strain rate (SR) technique in each of the 16 LV segments [16]. Motion toward the apex after closure of the aortic valve was only registered as DLC if negative SR documented that the motion reflected true shortening (Figure 1). All the TVI analyses were performed twice by the same investigator and the mean of the two measurements was used. Intra- and inter-variability was fairly low. The coefficient of variation for TSI and DLC analysis was 3 and 5%, and 4,5 and 9%, respectively.
Atrio-ventricular and Inter-ventricular dyssynchrony
Atrio-ventricular dyssynchrony (LVFT/RR) was considered present if the left ventricular filling time (LVFT) measured from the mitral valve Doppler in-flow signal was <40% of the cardiac interval (R-R). The inter-ventricular mechanical delay (IVMD), was defined as the time difference between the onset of forward flow in the LV outflow tract and RV outflow tract and >40 ms was considered indicative IVMD [17]
Other methods
Other aspects of the study methods such as assays for NT-proBNP have been published in detail [17].
Statistical analysis
Descriptive statistics were used to analyse the study population and median (interquartile range) are given unless otherwise stated. Difference in proportions was assessed using Fisher's exact test, and the Kruskal Wallis test was used to compare non normally distributed continuous data. Different variables all known to be risk-factors in the heart failure syndrome were tested by univariate analysis for relations with intra-ventricular dyssynchrony measured by TSI and DLC separately. All tested risk-factors with a p-value < 0.10 were also tested in a multiple regression analyses in order to find out which variables that might be independently most important for intra-ventricular dyssynchrony. Tested variables were examined through developing generalised linear models, with log link functions and Poisson error structure. Thus, the statistical analysis attempts to predict the presence and severity of dyssynchrony in a subject. Multivariate models used forward stepwise selection, with a P value of 0.10 for entry to the model, and p = 0.05 to stay in the model. All analyses were conducted using SAS 9.1 (SAS Institute, Cary, NC).
Results
Baseline characteristics of the patients
Eight hundred and thirteen patients were recruited to the CARE-HF trial of which 100 participated in the tissue Doppler sub study. Only nine patients in the sub study had QRS below 150 ms. The characteristics of the patients in the sub study were similar to those in the main-study, except for evidence for more intense pharmacological management (Table 1 and Table 2). Echocardiographic measures of dimensions and LV EF were however similar and there was only a trend to higher (N.S.) NT-proBNP.
Atrio-ventricular and Inter-ventricular dyssynchrony
Thirty-four patients (34%) had a LVFT/RR <40%, 60 (60%) had inter-ventricular dyssynchrony and the median IVMD was 47.9 ms (Table 3).
Intra-ventricular dyssynchrony
Eighty-six patients (86%) had intra-ventricular dyssynchrony on TSI. The distribution of TSI-measured dyssynchrony is shown in figure 2. The median number of affected segments was four and all showed dyssynchrony in one or more basal segment. Mid-segments were affected in 69 patients, with a median of two affected segments, but none had apical dyssynchrony. Eighty-five patients (85%) had intra-ventricular dyssynchrony measured by the SR technique, all 85 patients having affected basal segments, with a median two out of six segments, 70 having mid-segments affected but none having apical dyssynchrony (Table 3).

Distribution of intra-ventricular dyssynchrony in affected segments in the heart failure population, n = 100.
On univariate analysis, patients with dyssynchrony measured by TSI were more likely to be women p = 0.001, have IDCM p = 0.002 and have greater QRS duration p = 0.03. Findings were similar for intra-ventricular dyssynchrony by DLC (Table 4).
On multi-variate analysis woman, patients with IDCM and measures of ventricular dilatation and dysfunction, but not QRS duration, predicted the presence of dyssynchrony by TSI and DLC.
Inter-relationship between TSI and DLC
Most patients had intra-ventricular dyssynchrony using both methods but measurements of TSI are substantially faster. Accordingly, we investigated the agreement between the methods analysing every segment separately in the 16-segment model [15] to determine wheather their results were interchangeable. Within the six basal segments, three had a perfect match and the Kappa coefficient was 0.86–1.0. The agreement within the mid-segments was even better with three segments showing perfect match and the Kappa coefficient being 0.92–1.0. These findings suggests that TSI and DLC are interchangeable methods with which to assess dyssynchrony.
Presence of different types of dyssynchrony in patients with and without intra-ventricular dyssynchrony
LVFT/RR <40% was present in 33% and IVMD in 51% of patients with intra-ventricular dyssynchrony (TSI or DLC). Conversely, 85% of the patients with IVMD >40 ms had intra-ventricular dyssynchrony.
All three types of dyssynchrony co-existed in only 23% of the patients (Table 5).
The impact of aetiology – cardiomyopathy or ischemic heart disease on LV dyssynchrony
Patients with cardiomyopathy had shorter LVFT and more LVFT/RR than those with ischemic heart disease, 45,3% vs. 21,3%, p = 0.02. IVMD was present in 69% of patients with IDCM and 48,9% of those with IHD, p = 0.09. Similar numbers of patients with IDCM and IHD had intra-ventricular dyssynchrony, with the basal lateral and posterior segments most commonly affected (Figure 3), but patients with IDCM had more affected segments, with a median of 4(3, 5) vs. 3(1, 4), p = 0.027 (Table 3 and 5).

Distribution of intra-ventricular dyssynchrony in affected segments in patients with cardiomyopathy n = 53 (left) and ischemic heart disease n = 47 (right).
Discussion
In this cohort of 100 patients with moderate to severe heart failure, reduced systolic LV function and prolonged QRS duration we found a high prevalence and severity of each type of dyssynchrony. Intra-ventricular dyssynchrony was present in the great majority of patients measured by either tissue Doppler imaging method both of which appear to identify patients who respond better to CRT in observational trials. Reports of the prevalence of intra-ventricular dyssynchrony vary depending on the method used. Previous reports have suggested a prevalence of 72–80% in patients with heart failure and QRS duration >120 ms [18–20] which is similar to the rate reported in his study.
IVMD, one of the potential entry criteria for CARE-HF tended to be less prevalent but occurred in 60% of the patients in this sub study, a similar proportion (62%) to that observed in the overall study [10] and in previous reports [18, 19]. The rates they report are entirely consistent with these data. Intra-ventricular dyssynchrony was equally common in patients with and without IVMD. It would appear that inter- and intra-ventricular dyssynchrony are both common but one does not appear to influence the prevalence of the other. Why are IVMD and intra-ventricular dyssynchrony not linked (0.86 multiplied by 0.6 = 0.51 i.e. 51% is a simple proportion which it should not be if they were linked). This is somewhat surprising since greater intra-ventricular dyssynchrony should allow the intra-ventricular septum to contract earlier leading to a shorter pre-ejection period and impaired LV function leading to longer aortic pre-ejection time. However, the most likely explanation to this is that IVMD reflects a global dyssynchrony but intra-ventricular dyssynchrony a more heterogeneous regional dyssynchrony as described in figure 2. The agreement between inter-and intra -ventricular dyssynchrony has been reported low [18].
Inter-ventricular and intra-ventricular dyssynchrony
Many studies show that QRS duration predicts mortality in patients with heart failure. It is assumed by many that this reflects more severe dyssynchrony. However, QRS also reflects LVEF [21]. There are few data that show whether dyssynchrony by imaging is prognostically important. In the CARE-HF study, IVMD was associated with a better prognosis in the control group. One small observational study [8] with an unusually high mortality found that intra -ventricular dyssynchrony but not IVMD or QRS predicted mortality.
The QRS width has been shown to be related to both inter- and intra-ventricular dyssynchrony but during long-term follow up of patients with dilated cardiomyopathy only intra-ventricular dyssynchrony was related to cardiac events [7, 8]. Another important issue is the capability to predict LV reverse remodelling after CRT and even if IVMD has been shown to predict response to CRT [22] most investigators consider intra-ventricular dyssynchrony to select responders to CRT [23, 24]. On the other hand, IVMD is easy to measure and in this study 85% of the patients with IVMD >40 ms also had intra-ventricular dyssynchrony which could make it reasonable to include IVMD in clinical routine.
Tissue synchronisation imaging and strain rate
In this study, we found a high prevalence of intra-ventricular dyssynchrony with a high agreement between the two methods suggesting that they are inter-changeable in terms of evaluating intra-ventricular dyssynchrony. Thus a postsystolic DLC is associated with a delayed maximal velocity in the same region during systole.
Since the TSI analyse is substantially faster to perform, TSI may be used in clinical routine. In a previous report by Gorscan et al a cut-off value of >65 ms had a sensitivity and specificity of 87% and 100%, respectively, to predict the initial response to CRT [25]. LV reverse remodelling after three months of CRT may also be predicted by TSI with a sensitivity of 87% and specificity of 81% [26]. Van de Veire et al found there was an excellent correlation between LV dyssynchrony measured manually by color-coded TDI and automatically using TSI [27]. The recently published PROSPECT trial, an observational study, tested twelve different techniques to describe dyssynchrony and many of those turned out to be difficult, due to high variability, to use in a multicenter study [28]. As a mater of fact, those techniques which could be said are easiest to use i.e. lateral- septum maximal velocity difference (TS -lateral- septum), LVFT/RR, APE and IVMD turned out to be the most useful. This further support the use of the fast and simple TSI technique (Fig 4, 5). In our preliminary analysis of outcome data at least two TSI positive segments are needed to predict a responder to CRT.

Tissue synchronization imaging (TSI) showing delayed lateral systolic contraction in red colour with corresponding TVI-curves. AVO and AVC = aortic valve opening and closure.

Tissue synchronization imaging (TSI) showing inferior delayed systolic contraction in red colour with corresponding TVI-curves. The TSI-technique is timesaving and makes it easy to find intra ventricular regions with dyssynchrony. Abbreviations see fig 4.
However, analysis of CARE-HF suggests that the initial response of LV function to CRT is a poor predictor of the effect of intervention on long-term mortality. Strain rate analyses of delayed longitudinal contraction (DLC) often require an off-line approach and are therefore more time-consuming. The main advantage with strain rate is its ability to differentiate between active systolic contraction and passive motion. The number of segments with DLC is related to the improvement in LV systolic function by biventricular pacing during long-term follow-up [11]. Thus, both methods might be useful to select patients who get greater benefit from CRT. However, randomized controlled trials (RCTs) that might be difficult to design will be required to test this hypothesis.
Cardiomyopathy or ischemic heart disease
We found patients with cardiomyopathy to have shorter LVFT than those with ischemic ethiology and more patients had LVFT/RR <40% of the R-R interval. There was a tendency to more patients having intra-ventricular dyssynchrony in the CMP group compared to IHD, and there was a difference in the number of affected segments 4(3, 5) vs. 3(1, 4), p = 0.027. Thus, two types of dyssynchrony and combinations of dyssynchrony were more common in patients with dilated cardiomyopathy. Similar findings with signs of less dyssynchrony in patients with ischemic heart failure were shown in a study by Zwanenburg et al using Magnetic resonance imaging [29]. Thus, CRT might be less effective in ischemic patients compared with patients with cardiomyopathy (but CARE-HF shows ischemic patients to have smaller effect on LV function but similar effect on long-term mortality). This has been observed in i.e. the MIRACLE trial in which both non-ischemic and ischemic patients improved regarding reverse remodelling and enhanced EF but the changes was statistically significantly smaller in the ischemic group [30]. This difference has also been observed in other studies [31, 32] and could thus be explained by less dyssynchrony in the ischemic patients but perhaps also by the ischemic patients having more scar tissue.
Limitations of the study
The PROSPECT (Predictors of response to cardiac resynchronization therapy) study was recently reported at the hotline session during the ESC meeting 2007 and commented on by E. S Zegers and F.W.A Verheugt in the Euro Heart J [33]. This is a multicentre study including 426 patients with standard indication for CRT. The aim was to identify echocardiographic and tissue Doppler measures of dyssynchrony and their ability to predict response to CRT. It was found that presence of signs of dyssynchrony was linked to 11–13% additional clinical response to CRT and 13–23% additional response for reverse remodelling compared to absence of measures of dyssynchrony. One limitation of our study is we do not report on outcome of the patients, however, that was not the aim of this study but obviously it is important to identify signs of dyssynchrony. Another finding in the PROSPECT study was a high inter-variability measuring signs of dyssynchrony and therefore a need for simplification of methodology. However, it is important to remember this was not a RCT but an observational study which means that the importance of dyssynchrony can not be fully estimated. TSI might be such a simple method as described in this paper. It is also easy to measure LVFT/RR and IVMD and using these three signs of dyssynchrony in clinical routine might be sufficient to identify potential responders to CRT.
Other examinations
It appears important to assess the amount of scars, especially if the patient has IHD, and LV cardiac reserve which can be done by i.e. magnetic resonance imaging (MRI) or dobutamine stress echocardiography (DSE). Da Costa et al found a 25% increase of LVEF during low-dose DSE and IVMD>50 ms to have independent predictive value to predict response to CRT [34]. There is also an on-going multicenter study, LODO-CRT, testing the value of low-dose DSE before implanting biventricular pacemaker in heart failure patients with standard indication for CRT [35]. Other potentially valuable examinations might be i.e. 3D- echocardiography and speckle tracking echocardiography.
Conclusion
The prevalence of intra-ventricular dyssynchrony is high in patients with heart failure, wide QRS and severely depressed systolic function. Patients with cardiomyopathy were more likely to have dyssynchrony compared to ischemic patients. We recommend using TSI to identify patients with intra-ventricular dyssynchrony since TSI is an easy method to use and appears to be a reliable and time-efficient method to identify patients likely to benefit from biventricular pacing.
References
Mostered A, Hoes AW, de Bruyne MC, Deckers JW, Linkerr DT, Hofman A, et al.: Prevalence of heart failure and left ventricular dysfunction in the general population. The Rotterdam study. Eur Heart J. 1999, 20: 447-55. 10.1053/euhj.1998.1239
Mejhert M, Persson H, Edner M, Kahan T: Epidemiology of heart failure in Sweden – a national survey. Eur J Heart Fail. 2001, 3: 97-103. 10.1016/S1388-9842(00)00115-X
Stewart S, MacIntyre K, MacLeod MMC, Bailey AEM, Capewell S, MacMurray JJV: Trends in hospitalisation for heart failure in Scotland, 1990–1996. Eur Heart J. 2001, 22: 209-17. 10.1053/euhj.2000.2291
Cleland JGF, Gemmell I, Khand A, Boddy A: Is the prognosis of heart failure improving?. Eur J Heart Fail. 1999, 1: 229-41. 10.1016/S1388-9842(99)00032-X
Silvet H, Amin J, Padmanabhan S, Pai RG: Prognostic implications of increased QRS duration in patients with moderate and severe left ventricular systolic dysfunction. Am J Cardiol. 2001, 88: 182-5. 10.1016/S0002-9149(01)01619-8
Murkofsky RL, Dangas G, Diamond JA, Metha D, Schaffer A, Ambrose JA: A prolonged QRS duration on surface electrocardiogram is a specific indicator of left ventricular dysfunction. J Am Coll Cardiol. 1998, 32: 476-82. 10.1016/S0735-1097(98)00242-3
Fauchier L, Marie O, Casset-Senon D, Babuty D, Cosnay P, Fauchier JP: Interventricular and intraventricular dyssynchrony in idiopathic dilated cardiomyopathy. J Am Coll Cardiol. 2002, 40: 2022-30. 10.1016/S0735-1097(02)02569-X
Bader H, Garrigue S, Lafitte S, Reuter S, Jais P, Haissaguerre M, et al.: Intra- left ventricular electromechanical asynchrony. A new independent predictor of severe cardiac events in heart failure patients. J Am. Coll Cardiol. 2004, 43: 248-56. 10.1016/j.jacc.2003.08.038
Kerwin WF, Botvinick EH, O'Connell JW, Merrick SH, DeMarco T, Chatterjee K, et al.: Ventricular contraction abnormalities in dilated cardiomyopathy: effect of biventricular pacing to correct interventricular dyssynchrony. J Am Coll Cardiol. 2000, 35: 1221-7. 10.1016/S0735-1097(00)00555-6
Cleland JGF, Daubert JC, Erdman E, Freemantle N, Gras D, Kappenberger L, et al.: The effect of cardiac resynchronization on morbidity and mortality in heart failure. New Eng J Med. 2005, 352: 1539-49. 10.1056/NEJMoa050496
Sogaard P, Egeblad H, Kim WY, Jensen HK, Pedersen AK, Kristensen BO, et al.: Tissue Doppler imaging predicts improved systolic performance and reversed left ventricular remodeling during long-term cardiac resynchronization therapy. J Am Coll Cardiol. 2002, 40: 723-30. 10.1016/S0735-1097(02)02010-7
Yu C-M, Fung W-H, Lin H, Zhang Q, Sanderson JE, Lau C-P: Predictors of left ventricular reverse remodelling after cardiac resynchronization therapy for heart failure secondary to idiopathic dilated or ischemic cardiomyopathy. Am J Cardiol. 2003, 91: 684-8. 10.1016/S0002-9149(02)03404-5
Cleand JGF, Daubert JC, Erdman E, Freemantle N, Gras D, Kappenberger L, et al.: Baseline characteristics of patients recruited into the CARE-HF study. Eur J Heart Fail. 2005, 7 (2): 205-14. 10.1016/j.ejheart.2005.01.010
Kjaergaard J, Hassager C, Oh JK, Kristensen JH, Berning J, Sogaard P: Measurement of cardiac time intervals by Doppler tissue m-mode imaging of the anterior mitral leaflet. J Am Soc Echocardiogr. 2005, 18: 1058-65. 10.1016/j.echo.2005.03.043
, Schiller NB, Shah PM, Crawford M, DeMaria A, Devereux R, Feigenbaum H, et al.: Recommendations for quantitation of the left ventricle by two-Dimensional Echocardiography. J Am Soc Echocardiogr. 1989, 2: 358-67.
Sogaard P, Kim WY, Jensen HK, Mortensen P, Pedersen AK, Ostergaard Kristensen B, et al.: Impact of acute biventricular pacing on left ventricular performance and volumes in patients with severe heart failure. Cardiology. 2001, 95: 173-82. 10.1159/000047369
Cleand JGF, Daubert J-C, Erdman E, Freemantle N, Gras D, Kappenberger L, et al.: Design and methodology of the CARE-HF trial a randomized trial of cardiac resynchronisation in patients with heart failure and ventricular dyssynchrony. Eur J Heart Fail. 2001, 3: 481-9. 10.1016/S1388-9842(01)00176-3
Ghio S, Constantin C, Klersy C, Serio A, Fontana A, Campana C, et al.: Interventricular and intraventricular dyssynchrony are common in heart failure patients, regardless of QRS duration. Eur Heart J. 2004, 25: 571-8. 10.1016/j.ehj.2003.09.030
Perez de Isla L, Florit J, Garcia-Fernandez MA, Evangelista A, Zamorano J: Prevalence of echocardiographically detected ventricular asynchrony in patients with left ventricular systolic dysfunction. J Am Soc Echocardiogr. 2005, 18: 850-9. 10.1016/j.echo.2004.09.012
Yu CM, Lin H, Zhang Q, Sanderson JE: High prevalence of left ventricular systolic and diastolic asynchrony in patients with congestive heart failure and normal QRS duration. Heart. 2003, 89: 54-60. 10.1136/heart.89.1.54
Lainsack M, Cleland JGF, Lenzen MJ, Follath F, Komajda M, Swedberg K: International variations in the treatment and in co-morbidity of left ventricular systolic dysfunction: Data from EuroHeart Failure Survey. Eur J Heart Fail. 2007, 9: 292-9. 10.1016/j.ejheart.2006.07.007
Penika M, Bartunek J, De Bruyne B, Vanderheyden M, Goethals M, De Zutter M, et al.: Improvement of left ventricular function after cardiac resynchronization therapy is predicted by tissue Doppler imaging echocardiography. Circ. 2004, 109: 978-83. 10.1161/01.CIR.0000116765.43251.D7.
Bordacher P, Lafitte S, Reuter S, Sanders P, Jais P, Haissaguerre M, et al.: Echocardiographic parameters of ventricular dyssynchrony validation in patients with heart failure using sequential biventricular pacing. J Am Coll Cardiol. 2004, 44: 2157-65. 10.1016/j.jacc.2004.08.065
Yu CM, Fung WH, Zhang Q, Chan CK, Chan YS, Lin H, et al.: Tissue Doppler imaging is superior to strain rate imaging and post systolic shortening on the prediction of reverse remodelling in both ischemic and no ischemic heart failure after cardiac resynchronization therapy. Circ. 2004, 110: 66-73. 10.1161/01.CIR.0000133276.45198.A5.
Gorscan J, Kanzaki H, Bazaz R, Dohi K, Schwartzman D: Usefulness of echocardiographic tissue synchronization imaging to predict acute response to cardiac resynchronization therapy. Am J Cardiol. 2004, 93: 1178-81. 10.1016/j.amjcard.2004.01.054
Yu CM, Zhang Q, Fung JWH, Chan HCK, Chan YS, Yip GWK, et al.: A novel tool to assess systolic asynchrony and identify responders of cardiac resynchronization therapy by tissue synchronization imaging. J Am Coll Cardiol. 2005, 45: 677-84. 10.1016/j.jacc.2004.12.003
Veire van de N, Bleeker G, De Sutter J, Ypenburg C, Holman E, Wall van der E, et al.: Tissue synchronization imaging accurately measures left ventricular dyssynchrony and predicts response to cardiac resynchronization therapy. Heart. 2007, doi:10.1136/hrt.2006.099424
Chung ES, Leon AR, Tavazzi L, Sun J-P, et al.: Results of the Predictors of Response to CRT (PROSPECT) Trial. Circ. 2008, 117: 2608-16. 10.1161/CIRCULATIONAHA.107.743120.
Zwanenburg JJM, Gotte MJW, Marcus JT, Kuijer JPA, Knaapen P, Heethaar RM, et al.: Propagation of onset and peak time of myocardial shortening in ischemic versus no ischemic cardiomyopathy. J Am Coll Cardiol. 2005, 46: 2215-22. 10.1016/j.jacc.2005.08.047
St John Sutton MG, Plappert T, Abraham WT, Smith AL, DeLurgio DB, Leon AR, et al.: Effect of cardiac resynchronization therapy on left ventricular size and function in chronic heart failure. Circ. 2003, 107: 1985-90. 10.1161/01.CIR.0000065226.24159.E9.
Reuter S, Garrigue S, Barold SS, Jais P, Hocini M, Haissaguerre M, et al.: Comparison of characteristics in responders versus nonresponders with biventricular pacing for drug-resistant congestive heart failure. Am J Cardiol. 2002, 89: 346-9. 10.1016/S0002-9149(01)02240-8
Lindner O, Vogt J, Kammeier A, Wielepp P, Holzinger J, Baller D, et al.: Effect of cardiac resynchronization therapy on global and regional oxygen consumption and myocardial blood flow in patients with non-ischemic and ischemic cardiomyopathy. Eur Heart J. 2005, 26: 70-6. 10.1093/eurheartj/ehi046
Zegers ES, Verheught FWA: Hotline sessions of the 29th European Congress of Cardiology. Eur Heart J. 2007, 28: 2799-2802. 10.1093/eurheartj/ehm495.
Da Costa A, Thevenin J, Roche F, Faure E, et al.: Prospective validation of stress echocardiography as an identifier of CRT responders. Heart Rhythm. 2006, 3: 406-13. 10.1016/j.hrthm.2005.12.017
Muto C, Gasparini M, Iacopino S, Peraldo C, et al.: Efficacy of LOw-dose DObutamine stress echocardiography to predict CRT response (LODO-CRT) multicenter prospective study-Design and rationale. Am Heart J. 2008, 156: 656-61. 10.1016/j.ahj.2008.06.011
Acknowledgements
The authors would like to acknowledge the CARE-HF Study Management Team at Medtronic.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
ME: Made substantial contributions to conception and design, acquisition, analysis and interpretation of data, mainly responsible for drafting the manuscript. YK: acquisition, analysis and interpretation of data and drafting the manuscript. KNK: acquisition, analysis and interpretation of data. GE: acquisition, analysis and interpretation of data. KLR: acquisition, analysis and interpretation of data. FM: acquisition, analysis and interpretation of data. NF: statistical analysis and interpretation of data. JGFC: analysis and interpretation of data, drafting the manuscript. PS: acquisition, analysis and interpretation of data, drafting the manuscript. All authors approved the final version.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Edner, M., Kim, Y., Hansen, K.N. et al. Prevalence and inter-relationship of different Doppler measures of dyssynchrony in patients with heart failure and prolonged QRS: a report from CARE-HF. Cardiovasc Ultrasound 7, 1 (2009). https://doi.org/10.1186/1476-7120-7-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1476-7120-7-1