
Abstract
Background
Age-related macular disease is the leading cause of blind registration in the developed world. One aetiological hypothesis involves oxidation, and the intrinsic vulnerability of the retina to damage via this process. This has prompted interest in the role of antioxidants, particularly the carotenoids lutein and zeaxanthin, in the prevention and treatment of this eye disease.
Methods
The aim of this randomised controlled trial is to determine the effect of a nutritional supplement containing lutein, vitamins A, C and E, zinc, and copper on measures of visual function in people with and without age-related macular disease. Outcome measures are distance and near visual acuity, contrast sensitivity, colour vision, macular visual field, glare recovery, and fundus photography. Randomisation is achieved via a random number generator, and masking achieved by third party coding of the active and placebo containers. Data collection will take place at nine and 18 months, and statistical analysis will employ Student's t test.
Discussion
A paucity of treatment modalities for age-related macular disease has prompted research into the development of prevention strategies. A positive effect on normals may be indicative of a role of nutritional supplementation in preventing or delaying onset of the condition. An observed benefit in the age-related macular disease group may indicate a potential role of supplementation in prevention of progression, or even a degree reversal of the visual effects caused by this condition.
Similar content being viewed by others

Background
Epidemiology of age-related macular disease
Age-related macular degeneration is the leading cause of registrable blindness in the developed world [1–3], and its prevalence is expected to increase with the anticipated demographic right-shift [4]. In order to standardise terminology a classification system for age-related macular degeneration has been developed [5]. Early and late stages of the condition are termed age-related maculopathy (ARM) and age-related macular degeneration (AMD) respectively. The term age-related macular disease will be used to encompass ARM and AMD.
ARM is most often clinically apparent over the age of 50 years. The main symptom is increasing difficulty with fine detail discrimination. AMD is categorised further in to 'non-neovascular AMD' (also known as dry AMD or geographic atrophy), and 'neovascular AMD' (also known as wet, exudative, or disciform) [5]. Neovascular AMD refers to the growth of new, weak blood vessels and their subsequent leakage in the macular region of the retina. Non-neovascular AMD is the most common form, and is estimated to be present in 15% of eyes by 80 years of age [6–9]. Progression is slow and legal blindness has been estimated to occur between 5 and 10 years [10]. Neovascular AMD is less common, occurring in 5.2% of the population over 75 years [2], but accounts for 90% of blind registrations [11]. Sufferers experience rapid, significant loss of central vision. Neovascular AMD is generally preceded by the non-neovascular form.
Clinicopathogenesis of age-related macular disease
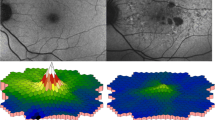
The macula is around 5 mm in diameter and is located centrally in the retina. It has a central depressed area, of approximately 1.5 mm diameter, called the fovea. The fovea is located approximately 4 mm temporal from the optic disc. The central floor of the fovea is called the foveola, which has a diameter of 0.35 mm and is the thinnest part of the retina. It contains only cone photoreceptors and their nuclei [12] (see figure 1).

Human fundus.
Aetiology of AMD
The exact aetiology of AMD is not known, but several hypotheses have been proposed:
Age-related change to Bruch's membrane and the retinal pigment epithelium (RPE)
The RPE lies between Bruch's membrane and the sensory retina. It forms the blood-retina barrier and is involved with vitamin A metabolism, transport of metabolites from the choroid to the retina, manufacture of mucopolysaccharides, and breakdown of damaged photoreceptor outer segments. Bruch's membrane separates the RPE from the choriocapillaris, which serves as the main blood supply to the outer retina [12].
Increasing age promotes an increased lipid content of Bruch's membrane, and the macula is affected by this process to a greater extent than the periphery [13]. Consequential changes to the diffusion characteristics of Bruch's membrane may precipitate AMD [14].
Senescence of RPE cells occurs earlier than in other cell types, such as fibroblasts [15]. Foveal RPE cells decrease in density and selectively lose their hexagonal shape with age [16, 17]. These changes may contribute to the onset of AMD.
Vascular insufficiency
Changes to the choroidal and scleral vasculature, and the resulting increase in haemodynamic resistance have been proposed to cause damage to the RPE [18, 19]. Foveal choriocapillaris blood flow is reduced with age, but has been shown to be further degraded in AMD patients [20, 21]. Laser Doppler flowmetry has been used to establish that choroidal blood volume is reduced via decreased density and diameter of the choriocapillaris [21].
Genetics
An increased risk of AMD has been demonstrated with a positive family history [22, 23], and this supports the proposed genetic component to development of AMD. It is likely that those with an inherited predisposition for the condition will develop it following exposure to certain risk factors [24].
Free radical/ oxidative stress hypothesis
Reactive oxygen intermediates is an inclusive term used to describe both oxidants and free radical species [25]. A free radical can be described as 'any atom or molecule that has one or more unpaired electrons' [26]. Examples include the superoxide anion (O2-•) and the hydroxyl free radical (OH•). Oxidants such as singlet oxygen (102) and hydrogen peroxide (H202) contain paired electrons, but in a reactive state [27]. It is proposed that many degenerative diseases result from uncontrolled ROI reactions within the body [28]. A free radical will attempt to achieve stability by gaining electrons from other molecules. These molecules become 'reducing agents' by donating electrons and are damaged by this process. In the retina this damage may lead to the development of age-related macular disease. The retina is particularly susceptible to oxidative stress for several reasons:
• The retina is subject to high levels of radiation, particularly blue light.
• Oxygen consumption by the retina is greater than that of other tissues [29].
• Photoreceptor outer segments contain a high proportion of polyunsaturated fatty acids, whose double bonds are a rich source of electrons [30, 31].
• The retina contains photosensitisers, which make cells and tissues sensitive to the influence of irradiation [32–34]
• Phagocytosis by the RPE generates ROI [35].
The body has several defence mechanisms against free radical damage, including antioxidant enzymes such as superoxide dismutase and catalase, antioxidant vitamins such as vitamins C, E and some carotenoids, and other antioxidant compounds such as metallationein, melanin, and glutathione. For a detailed account of the role of oxidation in the pathogenesis of AMD, see Beatty et al. (2000) [36].
Antioxidants and AMD
The lack of treatment options for AMD has prompted a search for possible preventative strategies. The main risk factors for AMD are increasing age [37–41], smoking [42–44], and family history [22, 45–47]. Proposed risk factors include female gender [2, 48], white ethnicity [49–51], sunlight exposure [52, 53], high dietary fat intake [54, 55], hypertension [38, 56–58], and low antioxidant levels [55, 59]. It follows that the risk of developing ARM and AMD may be reduced by lifestyle changes such as cessation of smoking, minimising sunlight exposure, reducing dietary fat intake, and maintaining antioxidant levels. For a review of randomised controlled trials investigating the role of nutritional supplementation in age-related macular disease, see Bartlett and Eperjesi (2003) [60].
The role of lutein and zeaxanthin in prevention and treatment of age-related macular disease
The isometric carotenoids lutein, zeaxanthin, and meso-zeaxanthin make up the macular pigment (MP) [61–63], which appears clinically as a yellow colouration to the macular area. Humans are unable to produce carotenoids but use them in a variety of functions [64]. Carotenoids are synthesised in plants, algae and bacteria [65], and the normal Western diet contains 1.3–3 mg/day of lutein and zeaxanthin combined [66, 67].
Ocular tissues contain several carotenoids, but the retina contains lutein and zeaxanthin exclusively [68]. Lutein and zeaxanthin are present in rod outer segments, where they would be most needed, and concentrations have been shown to be higher in the macular region than the peripheral retina [69]. This evidence supports the selective uptake of lutein in the retina and suggests that it plays important role in maintenance of ocular health.
A 70% reduced risk of AMD has been demonstrated with high (>0.67 μmol/L) versus low (0.25 μmol/L) lutein/zeaxanthin plasma levels [70]. A study of retinal levels of lutein and zeaxanthin in donor eyes found an 82% lower risk of AMD in retinae among the 25% with highest lutein and zeaxanthin levels compared to the 25% with the lowest levels [71]. Measurement of macular pigment optical density (MPOD) in healthy eyes showed an age-related decline, and healthy eyes considered to be at risk for AMD had significantly less MP than healthy eyes not at risk [72]. This evidence suggests that lower plasma and retinal levels of lutein and zeaxanthin present an increased risk of developing AMD.
Daily supplementation for 140 days with 30 mg of lutein esters produced a seven fold increase in lutein serum levels and a 20–40% increase in MPOD [73]. A 35% increase in lutein serum levels and a 20% increase in MPOD was demonstrated in a study supplementing 11 subjects daily with 11 mg of lutein from 60 g of spinach and 150 g or corn/maize [74]. Supplementation with 10 mg/day of lutein esters for 12 weeks was shown to increase serum lutein levels by five times and MPOD by approximately 20% [75]. These studies show that lutein supplementation does increase plasma and retinal lutein levels.
Lutein and zeaxanthin are believed to protect the retina in two ways. Firstly, they act as blue-light filters. Action spectrum for blue-light induced damage shows a maximum at 400 nm and 450 nm, and this is consistent with the absorption spectrum of macular pigment [76]. Secondly, they are able to quench free radicals. Energy transfer to them quenches singlet oxygen, and they are also believed to react with peroxy radicals that are involved with lipid peroxidation [77].
Objectives
To determine the effect of 18 months of daily lutein and antioxidant supplementation on measures of visual function in subjects with and without age-related macular disease.
Materials and Methods
Recruitment
The study requires recruitment of people with and without age-related macular disease. Recruitment methods employed include sending information to Birmingham optometrists, ophthalmologists, and a specialist centre for rehabilitation of people with sight loss, an editorial in the Birmingham Evening Mail, recruitment e-mails sent to the Royal National Institute for the Blind (RNIB) and all staff and students at Aston University and Aston Science Park. A project website has also been developed at http://www.aston.ac.uk/lhs/research/nri/opo/amd. Data collection takes place in a standard consulting room at Aston University. Enrolment, randomisation, and data collection are carried out by HB. HB and FE are masked to group assignment. HB is a research optometrist and FE is an optometrist and lecturer at Aston University, Birmingham, UK.
Inclusion/exclusion criteria
For inclusion participants a) have to provide written informed consent, b) have to be available for three visits to Aston University, c) have to present with no ocular pathology in one eye, or no ocular pathology other than dry AMD in one eye. A cataract grading system consisting of grades one, two and three for each of cortical, nuclear, and posterior subcapsular cataracts has been developed. Participants presenting with lens opacities precluding fundus photography are excluded. Throughout the trial period, progression of any type of cataract to the successive grade will require the participant to withdraw.
Exclusion criteria include type I and II diabetes because vitamin E has been shown to affect glucose tolerance [78–82] and diabetic retinopathy may confound the results. Those taking Warfarin medication are excluded as zinc may decrease its absorption and activity [83], as are those who use nutritional supplements that potentially raise vitamin and mineral intake above safe limits. The most recent guidelines for upper limits of nutritional supplementation are set out in the UK Food Standards Agency report [84]. Neovascular AMD and other ocular disease that could potentially interfere with the results are excluded.
Masking
The study formulation and placebo tablets have been produced by Quest Vitamins Ltd, Aston Science Park, Birmingham, B7 4AP, and are identical in external and internal appearance, and taste. The manufacturer has allocated distinguishing symbols, μ and λ. The tablets are packaged in identical, sealed, white containers; the only difference being the symbol on the label. Investigators and participants do not know which symbol represents the placebo tablets, and which represents the active formulation.
Intervention
The study formulation contains the following:
Lutein 6 mg
Vitamin A 750 μg
Vitamin C 250 mg
Vitamin E 34 mg
Zinc 10 mg
Copper 0.5 mg
Participants in both groups are instructed to take one tablet, at the same time every day, with food.
Randomisation
The random number generator function in Microsoft Excel is being used to allocate participants to μ and λ groups. Odd numbers allocate to the μ group.
Baseline data
On application, participants complete a health questionnaire, a food frequency questionnaire, and a food diary. The health questionnaire provides information about general health, medication, nutritional supplementation, smoking history, ocular health, and time spent living abroad. The food questionnaire and diary ask for information about diet for analysis using Foodbase 2000 software (The Institute of Brain Chemistry and Human Nutrition, London N7 8DB).
Outcome measures
The investigation of several measures of visual function is required, as age-related macular disease can produce varying signs and symptoms.
Visual acuity
Distance and near visual acuity (VA) measured using Bailey-Lovie logMAR charts. LogMAR charts have 5 letters and 0.1 log MAR progression per line. The advantage of using these charts is that they provide an equal-interval scale, and there are five letters per line. Standard Snellen charts do not provide a linear scale and have a decreasing number of letters per line as the letter size increases.
Contrast sensitivity
Contrast sensitivity (CS) is measured using a Pelli-Robson chart (Clement Clarke International, Edinburgh Way, Harlow, Essex, CM20 2TT, UK) and provides additional information about vision. The Pelli-Robson chart determines the contrast required to read large letters and is designed to test mid- to low-spatial frequencies. Some people may have normal visual acuity, but reduced contrast sensitivity at low spatial frequencies, particularly if they suffer from ocular pathologies such as age-related macular disease.
Colour vision
Colour vision measured using the PV-16 quantitative colour vision test (Precision Vision Inc, 944 First Street, La Salle, IL, 61301, USA). Macular disease can cause a deficiency in blue-yellow colour vision as the short-wavelength photoreceptors are concentrated around the fovea.
Macular Mapping Test
Macular Mapping (MM) test (The Smith-Kettlewell Research Institute, 2318 Fillmore Street, San Francisco, CA, 94115, USA) was developed to map visual defects caused by macular disease. It was developed by MacKeben and Colenbrander [85] and differs from conventional field analysis in that the stimuli are single letters rather than spots of light. This is a novel piece of equipment and each participant is given a practice run to eliminate learning effects. At the end of the test a single figure score is presented.
Glare recovery
Eger Macular Stressometer (EMS) (Gulden Ophthalmics, Elkins Park, PA 19027) is used to assess glare recovery, also known as photostress recovery time (PSRT). This is the time taken for the regeneration of photopigments in bleached photoreceptors to a level that allows resolution of, for example, a letter at near. Resynthesis of the photopigments is dependent upon the integrity of the photoreceptors and RPE [86]; it follows that the PSRT may be extended in those with diseases affecting these structures. This is a novel piece of equipment and each participant is given a practice run to eliminate learning effects.
Fundus photography
Fundus photographs of the macular will be assessed using colour and edge analysis software.
Follow up
Data collection will take place at baseline, nine, and 18 months.
Analyses
For each outcome measure the change between baseline, nine month, and 18 month values will be calculated. A Student's t test will be used to determine whether the means of these values differ at the 5% significance level between the placebo and active formulation results for age-related macular disease participants, and normal participants, after differences in age, gender and diet have been taken into account.
Power
From initial data collection we have calculated the treatment group sizes required in order to have 80% power at the 5% significance level for VA, CS, MM test, and the EMS. These values suggest that a total of 63 normal, and 96 age-related macular disease participants are required.
Ethical approval
The study has been approved by the Aston University Human Sciences Ethical Committee. The tenets of the Declaration of Helsinki are being followed [87].
Discussion
Randomised masked trials differ from observational studies in that they have the ability to demonstrate causality. The influence of confounding variables is reduced by random assignment of participants to intervention groups, and masking reduces the influence of investigator bias. There is evidence for selective deposition of lutein in the retina, increase of retinal and serum levels of lutein with supplementation, and an increased risk of age-related macular disease with reduced retinal lutein levels. This randomised controlled trial will provide further information regarding the effect of lutein and antioxidant supplementation on specific measures of visual function in people with and without age-related macular disease. The current paucity of treatment modalities for this condition has prompted research into the development of prevention strategies. A positive effect of the supplementation on normals may be indicative of its potential role in prevention or delaying the onset of age-related macular disease. This may be of particular importance for those with a positive family history, or exposure to other risk factors. A positive effect in age-related macular disease affected eyes may suggest a role of nutritional supplementation in prevention of progression of the disease, or even in reversal of symptoms.
References
Evans JR: Causes of blindness and partial sight in England and Wales 1990-1991. Studies on medical and population subjects. 1995, London, HMSO, 57:
Klein R, Klein BEK, Linton KLP: Prevalence of Age-Related Maculopathy - the Beaver Dam Eye Study. Ophthalmology. 1992, 99: 933-943.
Mitchell P, Smith W, Attebo K, Wang JJ: Prevalence of Age-Related Maculopathy in Australia - the Blue Mountains Eye Study. Ophthalmology. 1995, 102: 1450-1460.
United Nations: The world population prospects: the 2002 revision. www.un.org/esa/population/publications/wpp2000/highlights.pdf. 2002
Bird AEC, Bressler NM, Bressler SB, Chisholm IH, Coscas G, Davis MD, Dejong Ptvm, Klaver CCW, Klein BEK, Klein R, Mitchell P, Sarks JP, Sarks SH, Sourbane G, Taylor HR, Vingerling JR: An International Classification and Grading System for Age- Related Maculopathy and Age-Related Macular Degeneration. Survey of Ophthalmology. 1995, 39: 367-374.
Bressler NM, Bressler SB, Fine SL: Age-related macular degeneration. Survey of Ophthalmology. 1988, 32: 375-413.
Bressler NM, Bressler SB, Fine SL: Subfoveal neovascular membranes in senile macular degeneration: relationship between membrane size and visual prognosis. Retina. 1983, 3: 7-11.
Murphy RP: Age-related macular degeneration. Ophthalmology. 1986, 93: 969-971.
Tso MOM: Pathogenic factors of aging macular degeneration. Ophthalmology. 1985, 92: 628-636.
Arnold JJ, Sarks SH: Extracts from "Clinical evidence" - Age related macular degeneration. Br. Med. J. 2000, 321: 741-744. 10.1136/bmj.321.7263.741.
Chopdar A, Chakravarthy U, Verma D: Age-related macular degeneration. British Medical Journal. 2003, 326: 485-488. 10.1136/bmj.326.7387.485.
Kanski JJ: Clinical Ophthalmology. 1994, Oxford, Butterworth-Heineman, Third
Holz FG.et.al: Analysis of lipid deposits extracted from human macular and peripheral Bruch's membrane. Archives of Ophthalmology. 1994, 112: 402-406.
Ambati J, Ambati BK, Yoo SH, Ianchulev S, Adamis AP: Age-Related Macular Degeneration: Etiology,Pathogenesis, and Therapeutic Strategies. Survey of Ophthalmology. 2003, 48: 257-293. 10.1016/S0039-6257(03)00030-4.
Rawes V, Kipling D, Kill IR, Faragher RG: The kinetics of senescence in retinal pigment epithelial cells: a test for the telomere hypothesis of ageing?. Biochemistry. 1997, 62: 1291-1295.
Dorey CK, Wu G, Ebenstein D: Cell loss in the aging retina. Relationship to lipofuscin accumulation and macular degeneration. Invest Ophthalmol Vis Sci. 1989, 30: 1691-1699.
Watzke RC, Soldevilla JD, Trune DR: Morphometric analysis of human retinal pigment epithelium: correlation with age and location. Current Eye Research. 1993, 12: 133-142.
Friedman E: A hemodynamic model of the pathogenesis of age-related macular degeneration. American Journal of Ophthalmology. 1997, 124: 677-682.
Friedman E: The role of the atherosclerotic process in the pathogenesis of age-related macular degeneration. American Journal of Ophthalmology. 2000, 130: 658-663. 10.1016/S0002-9394(00)00643-7.
Grunwald JE, Hariprasad SM, DuPont J: Effect of aging on foveolar choroidal circulation. Archives of Ophthalmology. 1998, 116: 150-154.
Grunwald JE, Hariprasad SM, DuPont J: Foveolar choroidal blood flow in age-related macular degeneration. Investigative Ophthalmological Vision Science. 1998, 39: 385-390.
Hyman LG, Lilienfeld AM, Ferris FL, Fine SL: Senile Macular Degeneration - a Case-Control Study. Am. J. Epidemiol. 1983, 118: 213-227.
Smith W, Mitchell P: Family history and age-related maculopathy: the Blue Mountains Eye Study. Archives of Ophthalmology. 1998, 26: 203-206.
Bird A: Age-related macular disease. Br. J. Ophthalmol. 1996, 80: 2-3.
Rose RC, Richer SP, Bode AM: Ocular Oxidants and Antioxidant Protection. Proceedings of the Society for Experimental Biology and Medicine. 1998, 217: 397-407.
Southorn PA, Powis G: Free radicals in medicine I. Chemical nature and biological reactions. Mayo Clinical Procedures. 1988, 63: 381-389.
Halliwell B: Reactive oxygen species in living systems: source, biochemistry and role in human disease. Am J Med. 1991, 91 (Supp): 14-22.
Florence TM: Ther role of free radicals in disease (review). Australian and New Zealand Journal of Ophthalmology. 1995, 23: 3-7.
Sickel W: Retinal metabolism in dark and light. Handbook of sensory physiology. Edited by: FuortesMGF. 1972, Berlin, Springer-Verlag, 667-727.
Bazan NG: The metabolism of omega-3 polyunsaturated fatty acids in the eye: the possible role of docosahexaenoic acid and docosanoids in retinal physiology and ocular pathology. Progress in Clinical and Biological Research. 1989, 312: 95-112.
Stone WL, Farnsworth CC, Dratz EA: A reinvestigation of the fatty acid content of bovine, rat and frog retinal rod outer segments. Experimental Eye Research. 1979, 28: 387-397.
Delmelle M: Retinal sensitized photodynamic damage to liposomes. Photochemistry and Photobiology. 1978, 28: 357-360.
Gaillard ER, Atherton SJ, Eldred G, Dillon J: Photophysical studies on human retinal lipofuscin. Photochemistry and Photobiology. 1995, 61: 448-453.
Rozanowska M, Jarvis-Evans J, Korytowski W: Blue light-induced reactivity of retinal pigment. In vitro generation of oxygen-reactive species. Journal of Biological Chemistry. 1995, 270: 18825-18830. 10.1074/jbc.270.32.18825.
Tate DJ Jr, Miceli MV, Newsome DA: Phagocytosis and H202 induce catalase and metallothionein gene expression in human retinal pigment epithelial cells. Invest Ophthalmol Vis Sci. 1995, 36: 1271-1279.
Beatty S, Koh HH, Henson D, Boulton M: The role of oxidative stress in the pathogenesis of age-related macular degeneration. Surv. Ophthalmol. 2000, 45: 115-134. 10.1016/S0039-6257(00)00140-5.
Kahn HA, Moorhead HB: Statistics on blindness in the Model Reporting Area 1969-1970. 1973, Washington. DC, US DHEW
Goldberg J, Flowerdew G, Smith E, Brody JA, Tso MOM: Factors Associated with Age-Related Macular Degeneration - an Analysis of Data from the 1st National-Health and Nutrition Examination Survey. Am. J. Epidemiol. 1988, 128: 700-710.
Hawkins BS, Bird A, Klein R, West SK: Epidemiology of age-related macular degeneration. Mol. Vis. 1999, 5: U7-U10.
Klein R: Epidemiology. Age-Related Macular Degeneration. Edited by: Berger JW; Fine SL; Maguire MG. 1999, Philadelphia, Mosby, 31-55.
Smith W, Assink J, Klein R, Mitchell P, Klaver CCW, Klein BEK, Hofman A, Jensen S, Wang JJ, de Jong Ptvm: Risk factors for age related macular degeneration - Pooled findings from three continents. Ophthalmology. 2001, 108: 697-704. 10.1016/S0161-6420(00)00580-7.
Tamakoshi, Akiko, Yuzawa, Mitsuko, Matsui, Mizuo: Smoking and neovascular form of age-related macular degeneration in late middle aged males: findings from a case-control study in Japan. British Journal of Ophthalmology. 1997, 81: 901-904.
Seddon JM, Willett WC, Speizer FE, Hankinson SE: A prospective study of cigarette smoking and age-related macular degeneration in women. JAMA. 1996, 276:
Hawkins RL: Smoking, platelets and thrombosis. Nature. 1972, 236: 450-452.
Heiba IM,et.al: Sibling correlations and segregation analysis of age-related maculopathy: the Beaver Dam Eye Study. Genetic Epidemiology. 1994, 11: 51-67.
Klaver CCW, Smith, Smith: Familial aggregation of age-related macular degeneration in the Rotterdam Study (abstract). Investigative Opthalmological Visual Science. 1997, 38: S967-
Klaver CCW, Wolfs RCW, Assink JJM: Genetic Risk of Age-Related Maculopathy. Population-Based Familial Aggregation Study. Archives of Ophthalmology. 1998, 116: 1646-1651.
Kahn HA, smith, jones.: The Framingon Eye Study. 1. Outline and major prevalence findings. American Journal of Epidemiology. 1977, 106: 17-32.
Schachat AP, Hyman L, Leske MC, Connell AMS, Wu SY: Features of Age-Related Macular Degeneration in a Black- Population. Arch. Ophthalmol. 1995, 113: 728-735.
Friedman DS, Katz J, Bressler NM, Rahmani B, Tielsch JM: Racial differences in the prevalence of age-related macular degeneration - The Baltimore eye survey. Ophthalmology. 1999, 106: 1049-1055. 10.1016/S0161-6420(99)90267-1.
Jampol LM, Tielsch JM: Race, Macular Degeneration, and the Macular Photocoagulation Study. Archives of Ophthalmology. 1992, 110: 1699-1700.
Cruickshanks KJ, Klein R, Klein BEK, Nondahl DM: Sunlight and the 5-year incidence of early age-related maculopathy - The Beaver Dam Eye Study. Arch. Ophthalmol. 2001, 119: 246-250.
Delcourt C, Carriere I, Ponton-Sanchez A: Light Exposure and the Risk of Age-Related Macular Degeneration: The POLA Study. Archives of Ophthalmology. 2001, 119: 1463-1468.
Mares-Perlman JA.et.al: Dietary fat and age-related maculopathy. Archives of Ophthalmology. 1995, 113: 743-748.
Yannuzzi LA, Sorenson JA, Sobel RS, Daly JR, Derosa JT, Seddon JM, Gragoudas ES, Puliafito CA, Gelles E, Gonet R, Burton TC, Culver J, Metzger K, Kalbfleisch N, Zarling D, Farber MD, Blair N, Stelmack T, Axelrod A, Waitr SE, Cross A, Rolnick C, Flom T, Haller J, Pusin S, Cassel G, Applegate CA, Seigel D, Sperduto RD, Hiller R, Mowery R, Chew E, Tamboli A, Miller DT, Sowell AL, Gunter EW, Dunn M, Shamban K, Lento D, Alexander JA, Phillips DA: Risk-Factors for Neovascular Age-Related Macular Degeneration. Arch. Ophthalmol. 1992, 110: 1701-1708.
Hyman L, Smith, Smith: Risk factors for age-related maculopathy. Investigative Ophthalmological Vision Science. 1992, 33: 801-
Smith W, Mitchell P, Leeder SR.et.al: Plasma Fibrinogen Levels, Other Cardiovascular Risk Factors, and Age-Related Maculopathy. Archives of Ophthalmology. 1998, 116: 583-587.
The Age-Related Eye Disease Study Research Group: Risk factors associated with age-related macular degeneration - A case-control study in the Age-Related Eye Disease Study: Age- Related Eye Disease Study report number 3. Ophthalmology. 2000, 107: 2224-2232. 10.1016/S0161-6420(00)00409-7.
Richer S: Multicenter ophthalmic and nutritional age-related macular degeneration study part 2: antioxidant intervention and conclusions. J Am Optom Assoc. 1996, 67: 30-49.
Bartlett H, Eperjesi F: Age-related macular degeneration and nutritional supplementation: a review of randomised controlled trials. Ophthalmic and Physiological Optics. 2003, 23: 383-399. 10.1046/j.1475-1313.2003.00130.x.
Handelman GJ, Dratz EA, Reay CC: Carotenoids in the human macula and the whole retina. Invest Ophthalmol Vis Sci. 1988, 29: 850-855.
Bone RA;, Landrum JT;, Tarsis SL;: Preliminary identification of the human macular pigment. Vision Res. 1985, 25: 1531-1535. 10.1016/0042-6989(85)90123-3.
Khachik F, Bernstein PS, Garland DL: Identification of lutein and zeaxanthin oxidation products in human and monkey retinas. Invest Ophthalmol Vis Sci. 1997, 38: 1802-1811.
Isler O: Carotenoids. Edited by: Basel. 1971, Birkhauser-Verlag
Goodwin TW: . Methods in Enzymology. Edited by: PackerL. 1992, New York, Academic Press, 213: 167-172.
Nebeling LC, Forman MR, Graubard BI, Snyder RA: Changes in carotenoid intake in the United States. The 1987 and 1992 National Health Interview Surveys. Journal of the American Dietetic Association. 1997, 97: 991-996. 10.1016/S0002-8223(97)00239-3.
Nebeling LC, Forman MR;, Graubard BI, Snyder RA: The Impact of Lifestyle Characterisitcs on Carotenoid Intake in the United States: The 1987 National Health Interview Survey. American Journal of Public Health. 1997, 87: 268-271.
Bernstein PS, Khachik F, Carvalho LS, Muir GJ, Zhao DY, Katz NB: Identification and quantitation of carotenoids and their metabolites in the tissues of the human eye. Experimental Eye Research. 2001, 72: 215-223. 10.1006/exer.2000.0954.
Rapp LM, Maple SS, Choi JH: Lutein and zeaxanthin concentrations in rod outer segment membranes from perifoveal and peripheral human retina. Investigative Ophthalmology & Visual Science. 2000, 41: 1200-1209.
EDCCS Group: Antioxidant status and neovascular age-related macular degeneration. The Eye Disease Case Control Study Group. Archives of Ophthalmology. 1993, 111: 104-109.
Bone RA, Landrum JT, Mayne ST, Gomez CM, Tibor SE, Twaroska EE: Macular pigment in donor eyes with and without AMD: A case-control study. Invest Ophthalmol Vis Sci. 2001, 42: 235-240.
Beatty S, Murray IJ, Henson DB, Carden D, Koh H, Boulton ME: Macular pigment and risk for age-related macular degeneration in subjects from a Northern European population. Investigative Ophthalmology & Visual Science. 2001, 42: 439-446.
Landrum JT, Bone RA, Joa H, Kilburn MD, Moore LL, Sprague KE: A one year study of the macular pigment: the effect of 140 days of a lutein supplement. Experimental Eye Research. 1997, 65: 57-62. 10.1006/exer.1997.0309.
Hammond B R, Jr, Johnson EJ, Russell RM, Krinsky NI, Yeum KJ, Edwards RB, Snodderly DM: Dietary modification of human macular pigment density. Investigative Ophthalmology & Visual Science. 1997, 38: 1795-1801.
Berendschot Ttjm, Goldbohm RA, Klopping WAA, van de Kraats J, van Norel J, van Norren D: Influence of lutein supplementation on macular pigment, assessed with two objective techniques. Invest. Ophthalmol. Vis. Sci. 2000, 41: 3322-3326.
Ham WT Jr, Mueller HA, Ruffolo JJ Jr: Basic mechanisms underlying the production of photochemical lesions in the mammalian retina. Curr Eye Res. 1984, 3: 165-174.
Landrum JT, Bone RA: Lutein, zeaxanthin, and the macular pigment. Archives of Biochemistry and Biophysics. 2001, 385: 28-40. 10.1006/abbi.2000.2171.
Bierenbaum ML, Noonan FJ, Machlin LJ: The effect of supplemental vitamin E on serum parameters in diabetics, post coronary and normal subjects. Nutr Rep Int. 1985, 31: 1171-1180.
Paolisso G, D’Amore A, Giugliano D: Pharmacologic doses of vitamin E improve insulin action in healthy subjects and non-insulin dependent diabetic patients. Am J Clin Nutr. 1993, 57: 650-656.
Paolisso G, D’Amore A, Galzerano D: Daily vitamin E supplements improve metabolic control but not insulin secretion in elderly type II diabetic patients. Diabetes Care. 1993, 16: 1433-1437.
Tütüncü NB, Bayraktar M, Varli K: Reversal of defective nerve condition with vitamin E supplementation in type 2 diabetes. Diabetes Care. 1998, 21: 1915-1918.
Skrha J, Sindelka G, Kvasnicka J, Hilgertova J: Insulin action and fibrinolysis influenced by vitamin E in obese type 2 diabetes mellitus. Diabetes Res Clin Pract. 1999, 44: 27-33. 10.1016/S0168-8227(99)00010-8.
Pinto JT: The pharmacokinetic and pharmacodynamic interactions of foods and drugs. Topics in Clinical Nutrition. 1991, 6: 14-33.
Minerals Expert Group on Vitamins and: Safe Upper Limits for Vitamins and Minerals. 2003, www.foodstandards.gov.uk/multimedia/pdfs/vitamins2003.pdf, Food Standard Agency
MacKeben M, Colenbrander A: The assessment of residual vision in patients with maculopathies. Non-invasive assessment of the visual system. Technical Digest. 1993, 3: 274-277.
Brindley GS: Physiology of the retina and visual pathways. 1970, Baltimore, Williams and Wilkins
World Medical Association: Declaration of Helsinki. Journal of the Americal Medical Society. 1997, 277: 925-926.
Acknowledgments
This research is funded by the College of Optometrists, UK.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
None declared.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Bartlett, H., Eperjesi, F. A randomised controlled trial investigating the effect of nutritional supplementation on visual function in normal, and age-related macular disease affected eyes: design and methodology [ISRCTN78467674]. Nutr J 2, 12 (2003). https://doi.org/10.1186/1475-2891-2-12
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1475-2891-2-12