
Abstract
Background
Target organ damage (mainly cardiac and renal damage) is easy to evaluate in outpatient clinics and offers valuable information about patient's cardiovascular risk. The purpose of this study was to evaluate, using simple methods, the prevalence of cardiac and renal damage and its relationship to the presence of established cardiovascular disease (CVD), in patients with hypertension (HT) and type 2 diabetes mellitus (DM).
Methods
The RICARHD study is a multicentre, cross-sectional study made by 293 investigators in Nephrology and Internal Medicine Spanish outpatient clinics, and included patients aged 55 years or more with HT and type 2 DM with more than six months of diagnosis. Demographic, clinical and biochemical data, and CVD were collected from the clinical records. Cardiac damage was defined by the presence of electrocardiographic left ventricular hypertrophy (ECG-LVH), and renal damage by a calculated glomerular filtration rate (GFR) of <60 ml/min/1.73 m2, and/or the presence of an albumin/creatinine ratio ≥ 30 mg/g; or an urinary albumin excretion (UAE) ≥ 30 mg/24 hours.
Results
2339 patients (mean age 68.9 years, 48.2% females, 51.3% with established CVD) were included. ECG-LVH was present in 22.9% of the sample, GFR <60 ml/min/1.73 m2 in 45.1%, and abnormal UAE in 58.7%. Compared with the reference patients (those without neither cardiac nor renal damage), patients with ECG-LVH alone (OR 2.20, [95%CI 1.43–3.38]), or kidney damage alone (OR 1.41, [1.13–1.75]) showed an increased prevalence of CVD. The presence of both ECG-LVH and renal damage was associated with the higher prevalence (OR 3.12, [2.33–4.19]). After stratifying by gender, this relationship was present for both, men and women.
Conclusion
In patients with HT and type 2 DM, ECG-LVH or renal damage, evaluated using simple methods, are associated with an increased prevalence of established CVD. The simultaneous presence of both cardiac and renal damage was associated to the higher prevalence of CVD, affording complementary information. A systematic assessment of cardiac and renal damage complements the risk assessment of these patients with HT and type 2 DM.
Similar content being viewed by others


Background
The presence of diabetes mellitus (DM) increases the risk of any form of cardiovascular disease (CVD) and of death in hypertensive patients [1]. In the natural course of arterial hypertension (HT) it moreover has been seen that the development of type 2 DM during treatment multiplies the risk of cardiovascular complications over the middle term [2].
In the outpatient setting, the detection of silent cardiac damage (mainly left ventricular hypertrophy [LVH]) [3, 4], or of renal disease (pathological urinary albumin excretion [UAE] [5, 6] or diminished glomerular filtration rate [GFR] [7, 8]) in patients with HT and/or DM, defines a subgroup in whom cardiovascular risk is even greater. The detection of such target organ damage is simple in daily clinical practice, based on the electrocardiogram (ECG) and assessment of kidney function and UAE. Specifically, in patients with HT and DM, this identifies patients at very high cardiovascular risk. In the LIFE study, on patients with HT and electrocardiographic left ventricular hypertrophy (ECG-LVH), mortality during a follow-up period of 5 years was 14% [9], figure that was even greater among patients with elevated UAE [10].
The implication of target organ damage in the appearance of cardiovascular complications, and the possibility of adopting treatments to induce regression of such damage – with improvements in patient prognosis in some cases –, make it necessary to carefully assess silent organ damage. Epidemiological studies conducted in our setting and involving hypertensive subjects have shown a prevalence of ECG-LVH of 10–20% [11–13], with a prevalence of kidney damage of 20–30% [14]. However, no studies to date have evaluated in Spain the prevalence of target organ damage based on simple methods (basically ECG and blood and urine tests), and its impact upon the prevalence of established CVD in patients with HT and type 2 DM. The main objective of the RICARHD study (Cardiovascular risk in patients with arterial hypertension and type 2 diabetes) was to evaluate the prevalence of hypertensive cardiac and renal damage using the methods commonly used in outpatient clinics, and its relationship to the presence of established CVD, in a population of patients with HT and type 2DM.
Patients and methods
The RICARHD study was an epidemiological, multicentre, cross-sectional study conducted by 293 physicians specialized in Internal Medicine or Nephrology, in outpatient consulting offices. The study was approved by an independent Clinical Research Ethics Committee. The data collection period was between October and December 2005. Each investigator recorded information of 10 patients with HT and type 2 DM. In order to reduce selection bias, inclusion was requested of the first two or three programmed patients during 4–5 consecutive days. The study protocol was explained to the patients, and written informed consent was obtained.
The study comprised patients aged 55 years or older, with a diagnosis of HT and type 2 DM – both disorders having been present for more than 6 months. The presence of nephropathy not caused by DM or HT, and patient refusal to take part in the study were considered exclusion criteria. The clinical data were obtained from the patient history, while the biochemical parameters were recorded from laboratory testing in the three months prior to consultation (or in the days after consultation if no such prior testing proved available). Blood pressure (BP) recordings were made twice, under baseline conditions, and spaced one minute apart. Patient smoking or the consumption of coffee or other stimulants was not allowed before these measurements were obtained.
Evaluation of the main objective
The main objective of the study was to evaluate the prevalence of cardiac [LVH] and renal damage, based on the ECG and laboratory tests, in patients diagnosed with HT and type 2DM, and its relationship to the presence of established CVD.
ECG-LVH was diagnosed based on the voltage criteria of Cornell [15], and of Sokolow-Lyon [16]. The presence of ECG-LVH was accepted if the patient met: a) the voltage criterion of Cornell (sum of the R-wave on lead aVL + S-wave on V3> 20 mm in women, or >28 mm in males); or b) the voltage criterion of Sokolow-Lyon (sum of the S-wave on V1+ R-wave on leads V5 or V6>38 mm); or c) the patient history specified the presence of ECG-LVH based on any other criterion. Kidney damage was evaluated by conventional laboratory tests. GRF was calculated automatically from serum creatinine using the simplified Modification of Diet in Renal disease (MDRD) equation [17]. Urine testing was also carried out to calculate the UAE, by the albumin/creatinine (A/C) ratio or the 24-hour UAE. Kidney damage was considered if: a) the calculated GFR was <60 ml/min/1.73 m2; or b) the patient presented an A/C ratio of ≥ 3.5 mg/mmol (30 mg/g); or c) the patient presented an UAE ≥ 30 mg/24 hours.
The presence of established CVD was defined according to the patient's clinical records, and included myocardial infarction, angina, heart failure, peripheral vascular disease and stroke.
Statistical analysis
The sample size was calculated according to the main objective of the study and based on the expected prevalence of heart and kidney damage. For an expected prevalence of <10%, a sample size of 2401 hypertensive diabetic patients was estimated for a 95% confidence interval (CI) and an error of 1.2%. The sample was increased 4% to cover data losses, yielding a definitive size of 2500 patients.
Qualitative variables are shown with their frequency distribution. Quantitative variables are summarized by their mean, standard deviation (SD), range and percentiles. Asymmetric variables were described by the median and interquartile range (p25–p75). Association between qualitative variables was evaluated using the chi-square or the Fisher exact tests. The behavior of quantitative variables was analyzed for each of the independent variables using the Mann-Whitney U-test or median test.
A multivariable logistic regression model was made to account for the association of the study variables to the prevalence of established CVD. The odds ratios (OR) and corresponding 95% CI are presented.
Variable distribution was verified in all cases as compared with the theoretical models, and the hypothesis of homogeneity of variances was tested. In all hypothesis testing, the null hypothesis was rejected with a type I error or an alpha error <0.05. The SPSS 11.0 statistical package was used throughout.
Results
Descriptive data
Information was collected on 2466 patients, a total of 127(5.2%) being excluded from the analysis because they failed to meet some inclusion criterion or lacked some essential information. The final sample comprised 2339 patients (mean age 68.9 years [SD 10.8, range 55–98], 48.2% females). The mean body mass index (BMI) was 29.9 kg/m2(SD 7.8). 42.9% had obesity (BMI ≥ 30 kg/m2), and 11.6% were smokers. Some antecedent of CVD was recorded in 51.3% of the patients while 14.6% had a history of atrial fibrillation. The mean BP was 148.3/80.4 mmHg (SD 15.1/11.5), and only 15% showed BP < 130/80 mmHg. The characteristics of males and females are summarized in Table 1.
Target organ damage
ECG-LVH was present in 22.9% of the patients, (22.2% of women and 23.7% of males, p = NS). GFR <60 ml/min/1.73 m2 was documented in 45.1% (52.7% of women and 37.9% of males, p < 0.001). Information on UAE was available in 1887 patients – abnormal values (A/C ratio ≥ 3.5 mg/mmol [30 mg/g], or UAE ≥ 30 mg/24 hours) being recorded in 58.7% of the subjects (52.8% of women and 64.2% of males, p < 0.001).
Cardiac and renal damage, and the prevalence of cardiovascular disease
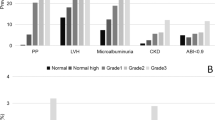
To assess the relationship between the presence of cardiac and/or renal damage and of established CVD, the study population was divided into four groups: patients without cardiac or renal lesions (28.6%); patients with ECG-LVH but no kidney damage (5.4%); patients with kidney damage and no ECG-LVH (48.4%); and patients with both ECG-LVH and renal damage (17.6%). Figure 1 shows the frequency distributions for the global population and by gender.

Distribution of the study population according to cardiac and/or renal damage. ECG-LVH: electrocardiographic left ventricular hypertrophy
The demographic characteristics of the four groups are shown in Table 2. Compared with the patients without ECG-LVH and without kidney damage, those with ECG-LVH showed (p < 0.05) higher mean systolic and diastolic BP values and a greater frequency of established CVD and atrial fibrillation. The patients with kidney damage were older, showed higher systolic BP and had a greater frequency of established CVD and atrial fibrillation (p < 0.05). Finally, those with heart and kidney damage were older, showed higher mean systolic BP and had a greater frequency of established CVD and atrial fibrillation, smoking and alcohol consumption, and hypercholesterolemia (p < 0.05).
The prevalence of the different manifestations of CVD, stratified by the presence of absence of ECG-LVH and/or kidney damage, is reported in Table 3. Compared with the patients with no cardiac or kidney damage, the subjects with kidney or cardiac damage showed a higher prevalence of any type of CVD (p < 0.001). The highest prevalence of any CVD was present in those with both ECG-LVH and kidney damage.
Multivariate analysis
To evaluate the impact of ECG-LVH and kidney damage upon the prevalence of established CVD, a multivariate model was constructed that included age, sex, BMI, moderate-severe alcohol consumption, smoking, hypercholesterolemia and BP.
Compared with the reference patients (no ECG-LVH and no kidney damage), the presence of ECG-LVH was associated with a 2-fold increased prevalence of established CVD (adjusted OR 2.20, 95%CI 1.43–3.38), while the presence of kidney damage alone was associated with a 41% greater prevalence (adjusted OR 1.41, 95%CI 1.13–1.75). The concomitant presence of both, ECG-LVH and renal damage was associated with a 3-fold greater prevalence (adjusted OR 3.12, 95%CI 2.33–4.19) of established CVD. This relationship was shown for the whole population, and also after stratifying by gender (table 4).
Discussion
The main findings of the RICARHD study were the following: 1) The presence of target organ damage (ECG-LVH, renal dysfunction, or abnormal UAE) is frequent in this group of patients with HT and type 2 DM seen in specialized clinics; 2) Such lesions are related to an increased prevalence of established CVD; and 3) The concomitant presence of cardiac and renal damage is associated with an even higher prevalence of cardiovascular complications. Thus, the integral evaluation of both types of lesion affords complementary information. The study was carried out in Internal Medicine and Nephrology outpatient clinics, and the conclusions drawn are applicable to the profile of the patients seen in such settings.
The prevalence of ECG-LVH was nearly 23%, based on simple voltage criteria, and was similar in both males and females. This prevalence may be slightly greater than expected, since the study was conducted in specialized centers. In other study conducted in the out-hospital setting in patients with DM (85% with concomitant HT), the prevalence of ECG-LVH based on the Cornell product was 17.1% [18]. Echocardiographic studies in turn report prevalences between 43% in the study of Sato et al. in patients with normal UAE not taking antihypertensive treatment [19] and 71% in the study of Dawson et al., conducted in the hospital setting [20].
In any case, LVH tends to be more prevalent in hypertensive diabetic patients than in non-diabetics [13], as is the case in patients with the metabolic syndrome [21]. Metabolic anomalies involving insulin resistance and hyperinsulinemia could favor the appearance of LVH independently of HT. At experimental level, insulin exerts trophic effects in animal models [22], while a number of human studies have reported a relationship among high insulin levels, insulin resistance and left ventricle mass [23–25]. In addition, insulin induces sodium retention at kidney level [26], which may also contribute to the development of LVH.
A total of 45.1% of the patients showed GFR <60 ml/min/1.73 m2. GFR was calculated using the simplified MDRD equation [17]. Although this equation may underestimate GFR by up to 29% in healthy subjects, this figure drops to only 6% in patients with genuinely reduced GFR [27], and is moreover the most widely used equation to calculate GRF. GFR decreases with increasing age, and the percentage of patients with diminished GFR recorded in our series is not surprising, moreover considering that HT and DM are independent risk factors for renal derangement. The greater prevalence of impaired kidney function among women has already been reported in other studies in our setting [28] and in other countries [29, 30], and is a consequence of the correction included in the equation for the decrease in muscle mass in women.
The prevalence of pathological UAE was very high in our series (58.7%). This may be conditioned by the fact that some patients were evaluated in Nephrology clinics. Microalbuminuria is predictive of posterior impaired renal function [31], and cross-sectional studies also have revealed an independent relationship between insulin resistance and microalbuminuria [32]. The relationship between diminished GFR and the risk of cardiovascular complications and death has also been observed in different follow-up studies [7, 8].
The most useful finding in our study was the relationship between silent target organ damage and established CVD. The prevalence of established CVD was twice as great in patients with ECG-LVH of either sex, between 30–60% greater in patients with kidney damage versus patients without ECG-LVH or kidney damage, and ever greater (three-fold) in those with both kidney and cardiac damage. This suggests that careful evaluation of these organs can improve patient risk assessment, and that the presence of kidney damage adds information to the presence of ECG-LVH and vice versa.
The data afforded by follow-up surveys and by cross-sectional studies thus support the need for correct assessment of damage to both target organs in patients with HT and DM, in order to define the cardiovascular risk and management strategy. The 2003 European Society of Cardiology/European Society of Hypertension Guidelines for the Management of Arterial Hypertension consider both, diabetes mellitus and target organ damage, as situations associated to a high 10-year cardiovascular risk (20–30%) even in subjects with high-normal BP [33]. This and other studies as the LIFE diabetes substudy address the question of if these diabetic hypertensive patients with target organ damage should fall into the very-high risk category (estimated ten-year risk of CVD over 30%). In the LIFE study, the mortality rate after 4.8 years of follow-up (half the follow-up that that used for the estimation in the Guidelines) was 14% for the subgroup of diabetic patients with HT and ECG-LVH [9], and 20,3% suffered a cardiovascular complication (cardiovascular death, myocardial infarction or stroke). Moreover, the higher risk was for those with UAE >16.9 mg/mmol (approximately equivalent to 150 mg/g), in whom mortality after 4.8 years was nearly 20%, and the incidence of cardiovascular complications was 26.4% [10].
In diabetic patients a BP control target of under 130/80 mmHg is accepted [33–35], and blocking of the rennin-angiotensin system is recommendable when kidney damage or ECG-LVH is detected. Different studies have shown that not only is such organ damage predictive of cardiovascular complications, but – more importantly – the regression of such lesions reduces the incidence of cardiovascular complications over the middle term. In the 1195 patients with HT, DM and ECG-LVH of the LIFE DM substudy [9], treatment with losartan (plus hydrochlorothiazide in most cases) reduced mortality by 40% versus treatment with atenolol (plus hydrochlorothiazide in most cases) and the greater reduction of microalbuminuria after one year of treatment was related to posterior reduction of the cardiovascular complications and in mortality [36]. A number of studies have also shown that in patients with HT and LVH, hypertrophy regression as demonstrated by both ECG [37, 38] and echocardiography [39, 40] is associated with an improved cardiovascular prognosis and that, moreover, the regression of both disorders (microalbuminuria and LVH) may improve the prognosis even more than regression of only one of the lesions [41]. Therefore, therapy in these patients should aim not only to control BP but also to induce regression of LVH and to reduce UAE.
Our study presents two major limitations: its cross-sectional nature and the setting in which it was carried out. The cross-sectional design only allows us to establish associations, without reliably defining the underlying cause-effect relationship. The important of some cardiovascular diseases involving high mortality, such as stroke, may be underestimated. The selection of Internal Medicine and Nephrology clinics for conducting the study means that the observed prevalences do not reflect the global population of hypertensive patients with type 2 DM. In fact, the prevalences of established CVD in this sample, as well as of renal damage, were extremely high. These high prevalences may be due not only to the setting in which the study was conducted but also because the selection of patients was not done at random: they were consecutively included, and this could have favored the inclusion of more sick patients (patients with established CVD), because they are usually more closely followed-up and attend the outpatient clinics more frequently. In this sense, the results of our study should apply only to this population and not to the universe of hypertensive type 2 diabetic patients. Nevertheless, the conclusions drawn in terms of the relationship between target organ damage and CVD are valid, and the size of the sample and the multicenter nature of the study offer a very reliable assessment of the population seen by such specialists.
Conclusion
In conclusion, the prevalence ECG-LVH and of renal damage, diagnosed by simple methods, in this population of hypertensive patients with type 2 DM, is high, and is associated with an increased prevalence of established CVD. Moreover, each lesion is independently related to CVD – the simultaneous presence of both lesions affording complementary information. The methods used to evaluate these lesions are very simple and inexpensive, and their careful application may help to improve the evaluation and to establish therapeutic objectives and strategies in these patients with such important cardiovascular risk.
Abbreviations
- CVD:
-
cardiovascular disease
- HT:
-
hypertension
- DM:
-
diabetes mellitus
- LVH:
-
left ventricular hypertrophy
- ECG:
-
electrocardiogram
- ECG-LVH:
-
electrocardiographic left ventricular hypertrophy
- GFR:
-
glomerular filtration rate
- UAE:
-
urinary albumin excretion
- OR:
-
odds ratio
- CI:
-
confidence interval
- SD:
-
standard deviation
- BP:
-
Blood pressure
- MDRD:
-
Modification of Diet in Renal disease
- BMI:
-
body mass index
- A/C ratio:
-
albumin/creatinine ratio
References
Kannel WB, D'Agostino RB, Wilson PW, Belanger AJ, Gagnon DR: Diabetes, fibrinogen, and risk of cardiovascular disease: the Framingham experience. Am Heart J. 1990, 120: 672-6. 10.1016/0002-8703(90)90026-T.
Verdecchia P, Reboldi G, Angeli F, Borgioni C, Gattobigio R, Filippucci L, Norgiolini S, Bracco C, Porcellati C: Adverse prognostic significance of new diabetes in treated hypertensive subjects. Hypertension. 2004, 43: 963-9. 10.1161/01.HYP.0000125726.92964.ab.
Kannel WB, Gordon T, Offutt D: Left ventricular hypertrophy by electrocardiogram. Prevalence, incidence, and mortality in the Framingham study. Ann Intern Med. 1969, 71: 89-105.
Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP: Prognostic implications of echocardiographically determined left ventricular mass in the Framingham Heart Study. N Engl J Med. 1990, 322: 1561-6.
Agewall S, Wikstrand J, Ljungman S, Fagerberg B: Usefulness of microalbuminuria in predicting cardiovascular mortality in treated hypertensive men with and without diabetes mellitus. Risk Factor Intervention Study Group. Am J Cardiol. 1997, 80: 164-9. 10.1016/S0002-9149(97)00312-3.
Jensen JS, Feldt-Rasmussen B, Strandgaard S, Schroll M, Borch-Johnsen K: Arterial hypertension, microalbuminuria, and risk of ischemic heart disease. Hypertension. 2000, 35: 898-903. [http://hyper.ahajournals.org/cgi/content/full/35/4/898]
Manjunath G, Tighiouart H, Coresh J, Macleod B, Salem DN, Griffith JL, Levey AS, Sarnak MJ: Level of kidney function as a risk factor for cardiovascular outcomes in the elderly. Kidney Int. 2003, 63: 1121-9. 10.1046/j.1523-1755.2003.00838.x.
Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY: Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004, 351: 1296-305. 10.1056/NEJMoa041031.
Lindholm LH, Ibsen H, Dahlof B, Devereux RB, Beevers G, de Faire U, Fyhrquist F, Julius S, Kjeldsen SE, Kristiansson K: Cardiovascular morbidity and mortality in patients with diabetes in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenolol. Lancet. 2002, 359: 1004-10. 10.1016/S0140-6736(02)08090-X.
Wachtell K, Ibsen H, Olsen MH, Borch-Johnsen K, Lindholm LH, Mogensen CE, Dahlof B, Devereux RB, Beevers G, de Faire U: Albuminuria and cardiovascular risk in hypertensive patients with left ventricular hypertrophy: the LIFE study. Ann Intern Med. 2003, 139: 901-6. [http://www.annals.org/cgi/reprint/139/11/901.pdf]
Llisterri Caro JL, Rodriguez Roca GC, Alonso Moreno FJ, Lou Arnal S, Divison Garrote JA, Santos Rodriguez JA, Raber Bejar A, de Castellar Sanso R, Ruilope Urioste LM, Banegas Banegas JR: Blood pressure control in Spanish hypertensive patients in Primary Health Care Centres. PRESCAP 2002 Study. Med Clin (Barc). 2004, 122: 165-71. 10.1157/13057821.
Barrios V, Campuzano R, Peña G, Guzman G, Ruilope LM: Estratificación del riesgo cardiovascular en hipertensión en Atención Primaria e impacto sobre el tratamiento antihipertensivo. Estudio DIORISC. Hipertensión. 2002, 19: 114-20.
Lozano JV, Redon J, Cea-Calvo L, Fernandez-Perez C, Navarro J, Bonet A, Gonzalez-Esteban J: Left ventricular hypertrophy in the Spanish hypertensive population. The ERIC-HTA study. Rev Esp Cardiol. 2006, 59: 136-42. 10.1157/13084641.
Pedrinelli R, Dell'Omo G, Di Bello V, Pontremoli R, Mariani M: Microalbuminuria, an integrated marker of cardiovascular risk in essential hypertension. J Hum Hypertens. 2002, 16: 79-89. 10.1038/sj.jhh.1001316.
Casale PN, Devereux RB, Kligfield P, Eisenberg RR, Miller DH, Chaudhary BS, Phillips MC: Electrocardiographic detection of left ventricular hypertrophy: development and prospective validation of improved criteria. J Am Coll Cardiol. 1985, 6: 572-80.
Sokolow M, Lyon T: Ventricular complex in left ventricular hypertrophy as obtained by unipolar precordial and limb leads. Am Heart J. 1949, 37: 161-186. 10.1016/0002-8703(49)90562-1.
Levey AS, Coresh J, Balk E, Kausz AT, Levin A, Steffes MW, Hogg RJ, Perrone RD, Lau J, Eknoyan G, National Kidney Foundation: National Kidney Foundation practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Ann Intern Med. 2003, 139: 137-47. [http://www.annals.org/cgi/reprint/139/2/137.pdf]
Bruno G, Giunti S, Bargero G, Ferrero S, Pagano G, Perin PC: Sex-differences in prevalence of electrocardiographic left ventricular hypertrophy in Type 2 diabetes: the Casale Monferrato Study. Diabet Med. 2004, 21: 823-8. 10.1111/j.1464-5491.2004.01246.x.
Sato A, Tarnow L, Nielsen FS, Knudsen E, Parving HH: Left ventricular hypertrophy in normoalbuminuric type 2 diabetic patients not taking antihypertensive treatment. QJM. 2005, 98: 879-84. 10.1093/qjmed/hci137.
Dawson A, Morris AD, Struthers AD: The epidemiology of left ventricular hypertrophy in type 2 diabetes mellitus. Diabetologia. 2005, 48: 1971-9. 10.1007/s00125-005-1896-y.
Mule G, Nardi E, Cottone S, Cusimano P, Volpe V, Piazza G, Mongiovi R, Mezzatesta G, Andronico G, Cerasola G: Influence of metabolic syndrome on hypertension-related target organ damage. J Intern Med. 2005, 257: 503-13. 10.1111/j.1365-2796.2005.01493.x.
Holmang A, Yoshida N, Jennische E, Waldenstrom A, Bjorntorp P: The effects of hyperinsulinaemia on myocardial mass, blood pressure regulation and central haemodynamics in rats. Eur J Clin Invest. 1996, 26: 973-8. 10.1046/j.1365-2362.1996.2880577.x.
Verdecchia P, Reboldi G, Schillaci G, Borgioni C, Ciucci A, Telera MP, Santeusanio F, Porcellati C, Brunetti P: Circulating insulin and insulin growth factor-1 are independent determinants of left ventricular mass and geometry in essential hypertension. Circulation. 1999, 100: 1802-7. [http://circ.ahajournals.org/cgi/content/full/100/17/1802]
Lind L, Andersson PE, Andren B, Hanni A, Lithell HO: Left ventricular hypertrophy in hypertension is associated with the insulin resistance metabolic syndrome. J Hypertens. 1995, 13: 433-8. 10.1097/00004872-199512000-00012.
Rutter MK, Parise H, Benjamin EJ, Levy D, Larson MG, Meigs JB, Nesto RW, Wilson PW, Vasan RS: Impact of glucose intolerance and insulin resistance on cardiac structure and function: sex-related differences in the Framingham Heart Study. Circulation. 2003, 107: 448-54. 10.1161/01.CIR.0000045671.62860.98.
DeFronzo RA, Cooke CR, Andres R, Faloona GR, Davis PJ: The effect of insulin on renal handling of sodium, potassium, calcium, and phosphate in man. J Clin Invest. 1975, 55: 845-55.
Rule AR, Larson TS, Bergstralh EJ, Slezak JM, Jacobsen SJ, Cosio FG: Using serum creatinine to estimate glomerular filtration rate: Accuracy in good health and in chronic kidney disease. Ann Intern Med. 2004, 141: 929-937. [http://www.annals.org/cgi/reprint/141/12/929.pdf]
Redon J, Cea-Calvo L, Lozano JV, Fernandez-Perez C, Navarro J, Bonet A, Gonzalez-Esteban J, ERIC-HTA 2003 Study Investigators: Kidney function and cardiovascular disease in the hypertensive population: the ERIC-HTA study. J Hypertens. 2006, 24: 663-9. 10.1097/01.hjh.0000209979.36359.70.
Clase CM, Garg AX, Kiberd B: Estimating the prevalence of low glomerular filtration rate requires attention to the creatinine assay calibration. J Am Soc Nephrol. 2002, 13: 2812-2816. 10.1097/01.ASN.0000013291.78621.26. [http://jasn.asnjournals.org/cgi/content/full/13/11/2811]
Viktorsdottir O, Palsson R, Andresdottir MB, Aspeland T, Gudnason V, Indridason OS: Prevalence of chronic kidney disease based on estimated glomerular filtration rate and proteinuria in Icelandic adults. Nephrol Dial Transplant. 2005, 20: 1799-1807. 10.1093/ndt/gfh914.
Schmieder RE, Messerli FH, Garavaglia G, Nunez B: Glomerular hyperfiltration indicates early target organ damage in essential hypertension. JAMA. 1990, 264: 2775-80. 10.1001/jama.264.21.2775.
Parvanova AI, Trevisan R, Iliev IP, Dimitrov BD, Vedovato M, Tiengo A, Remuzzi G, Ruggenenti P: Insulin resistance and microalbuminuria: a cross-sectional, case-control study of 158 patients with type 2 diabetes and different degrees of urinary albumin excretion. Diabetes. 2006, 55: 1456-62. 10.2337/db05-1484.
2003 European Society of Hypertension – European Society of Cardiology guidelines for management of arterial hypertension. J Hypertens. 2003, 21: 1011-1053. 10.1097/00004872-200306000-00001.
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jones DW, Materson BJ, Oparil S, Wright JT, Roccella EJ, National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure, National High Blood Pressure Education Program Coordinating Committee: The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. The JNC 7 report. JAMA. 2003, 289: 2560-2572. 10.1001/jama.289.19.2560.
American Diabetes Association: Standards of Medical Care in Diabetes-2006. Diabetes Care. 2006, 29 (Suppl 1): S4-S42. [http://care.diabetesjournals.org/cgi/content/full/29/suppl_1/s4]
Ibsen H, Olsen MH, Wachtell K, Borch-Johnsen K, Lindholm LH, Mogensen CE, Dahlof B, Snapinn SM, Wan Y, Lyle PA: Does albuminuria predict cardiovascular outcomes on treatment with losartan versus atenolol in patients with diabetes, hypertension, and left ventricular hypertrophy? The LIFE study. Diabetes Care. 2006, 29: 595-600. 10.2337/diacare.29.03.06.dc05-1724.
Levy D, Salomon M, D'Agostino RB, Belanger AJ, Kannel WB: Prognostic implications of baseline electrocardiographic features and their serial changes in subjects with left ventricular hypertrophy. Circulation. 1994, 90: 1786-93.
Okin PM, Devereux RB, Jern S, Kjeldsen SE, Julius S, Nieminen MS, Snapinn S, Harris KE, Aurup P, Edelman JM: Regression of electrocardiographic left ventricular hypertrophy during antihypertensive treatment and the prediction of mayor cardiovascular events. JAMA. 2004, 292: 2343-2349. 10.1001/jama.292.19.2343.
Verdecchia P, Schillaci G, Borgioni C, Ciucci A, Gattobigio R, Zampi I, Reboldi G, Porcellati C: Prognostic significance of serial changes in left ventricular mass in essential hypertension. Circulation. 1998, 97: 48-54. [http://circ.ahajournals.org/cgi/content/full/97/1/48]
Devereux RB, Wachtell K, Gerdts E, Boman K, Nieminen MS, Papademetriou V, Rokkedal J, Harris K, Aurup P, Dahlof B: Prognostic significance of left ventricular mass change during treatment of hypertension. JAMA. 2004, 292: 2350-2356. 10.1001/jama.292.19.2350.
Olsen MH, Wachtell K, Ibsen H, Lindholm LH, Dahlof B, Devereux RB, Kjeldsen SE, Oikarinen L, Okin PM, LIFE Study Investigators: Reductions in albuminuria and in electrocardiographic left ventricular hypertrophy independently improve prognosis in hypertension: the LIFE study. J Hypertens. 2006, 24: 775-81.
Acknowledgements
We are in debt with all the Physicians that have participated collecting data for the RICARHD study. This study was conducted with the scientific support of the Spanish Society of Internal Medicine (SEMI), the Spanish Society of Hypertension (SEH-LELHA), and the Spanish Society of Nephrology (SEN), and was funded by a research grant from Merck Sharp Dohme of Spain.
RICARHD (Riesgo Cardiovascular en el Paciente Hipertenso con Diabetes Tipo 2) Investigators (in alphabetical order): Acha Pérez, Francisco Javier (Hospital Miguel Servet); Afonso Suárez, Octavio (Hospital Universitario Gran Canaria Dr Negrín); Aguilar Cortés, Eduardo (Hospital C. de Alcañiz); Aguilar Soler, Gerardo (Hospital Germans Trias I Pujol); Alonso Gómez, Juan Carlos (Hospital Lluis Alcanyis); Alonso Ortiz, Belén (Hospital Universitario Gran Canaria Dr. Negrín); Alonso Pardo, José María (Asociación Investigación y desarrollo FRCV Hosp); Álvarez Chiva, Vicente (CE Hospital la Princesa); Amores Arriaga, Beatriz (Hospital Clínico Universitario Lozano Blesa); Andía Melero, Víctor Manuel (Hospital Ntra. Sra. de Sonsoles); Aomar Millán, Ismael (Cons. Hernández Torres); Aranda Lara, Pedro (Hospital Carlos Haya); Arias Zambrano, Andrés (Hospital Universitario Virgen del Rocio); Arroyo Díaz, Juan Antonio (Hospital de la Sta. Cruz y S. Pablo); Arteaga Coloma, Jesus (Hospital de Navarra); Asín Marcotegui, José Luis (Cons. Ext. del Hospital); Aznar Ondoño, Itziar (Hospital Universitario de Canarias); Barril Cuadrado, Guillermina (Hospital de la Princesa); Basterrechea Sanz, Ma Ángeles (Hospital G. Docente Guadalajara); Becerra Fernández, Antonio (Hospital Ramón y Cajal); Benet Gusta, Teresa (Hospital de la Sta. Cruz y S. Pablo); Benítez Bermejo, Rosa Isabel (Hospital G. Universitario Valencia); Bernardino de la Serna, José Ignacio (Hospital la Paz); Bianchi Llave, José Luis (Hospital C. Punta Europa); Bilbao Garay, Javier (Hospital Puerta de Hierro); Blancas Altabella, David (Hospital Res. San Camilo); Blázquez Encinar, Julio Cesar (Hospital de San Vicente); Boldova Gil, Ignacio (Hospital Miguel Servet); Borrego Hinojosa, Josefa (Hospital Universitario MQ. Jaen); Bravo Blanco, Ana (Hospital Ntra. Sra. del Cristal); Brito Sanfiel, Miguel Ángel (Hospital Puerta de Hierro); Bromsoms Artero, Josep (Hospital de Gerona Dr. J. Trueta); Burillo Fuertes, Maria Pilar (Hospital C. de Alcañiz); Caballero Granado, Francisco Javier (Hospital C. Punta Europa); Camba Caride, Maria Jesús (Hospital Ntra. Sra. del Cristal); Campayo Ibáñez, Antonio (HospitalbG. de Ontinyent); Campos Gutiérrez, Belén (Hospital C. de Alcañiz); Cano Leal, Antonio (Hospital Clínico Universitario Puerto Real); Cantero Sánchez, Natalia (CS. la Fe); Carraro Casieri, Raffaele (CE. Hospital la Princesa); Carreño Hernández, María Cruz (CE. Hospital Puerta de Hierro); Carreño Parrilla, Agustín (Hospital G. de Ciudad Real Sescam); Carrillo Linares, Juan Luis (Hospital Costa del Sol); Casal Álvarez, Florentino (Hospital de Cabueñes); Castellanos Guerrero, Victoriano (Hospital de la Serranía); Castillo Palma, Maria Jesús del (Hospital de Valme); Cazo Cativiela, F. Javier del (Hospital García Orcoyen); Cebollada del Hoyo, Jesús (Hospital G. San Jorge); Cepero García, Daniel (Hospital Torrecárdenas); Ceresuela Eito, Luis Miguel (CE. Hospital G. de L'hospitalet); Climent Codina, Celia (Hospital G. Universitario Alicante); Collado Nieto, Silvia (CE. Hospital Clínic Prov. Barcelona); Cortés Rodríguez, Begoña (Hospital Universitario Reina Sofía Córdoba); Costa Ferrer, Natalia (Hospital Can Misses); Costero Fernández, Olga (Hospital la Paz); Cruz de Frutos, Elena de la (Hospital G. Universitario Alicante); Cuadrado Gómez, Luis Miguel (Hospital Príncipe de Asturias); Chabrera Gaya, Vicente (Hospital de la Plana); Chimeno Viñas, Montserrat (Hospital Prov. Rodríguez Chamorro); Díaz Alcázar, Fernando (Hospital de Galdakano); Díaz Molina, Hugo (CE. Hospital G. Virgen de la Concha); Díaz Torres, Miguel Ángel (Hospital Duques del Infantado); Drusetta Llahues, Antonio (Clínica Juaneda); Dueñas Gutiérrez, Carlos (Hospital General Yagüe); Durán Castellón, Maria del Carmen (Hospital Universitario de Canarias); Elizaga Corrales, Jorge (CE. Hospital G. de Segovia); Escalera Morón, Berta (Hospital Universitario Virgen Macarena); Espino Montoro, Antonio (Hospital Ntra. Sra. de la Merced); Espinosa Garriga, Gerard (Hospital Clínic Prov. Barcelona); Estefan Kasabji, Jorge (Hospital Virgen Monte Toro); Estepa Marín, Araceli (CE. Hosp. Sant Camil); Estévez Domínguez, Rafael (Clínica San Roque); Ezquerra Larreina, Rafael (Hospital G. Santiago Apóstol); Fernández de Almeida, Alejandro (Hospital General Yagüe); Fernández Galante, Inmaculada (Hospital Clínico Universitario Valladolid); Fernández Martín, Julián (Hospital Meixoeiro); Fernández Molle, José Enrique (Hospital Juan Grande); Fernández Pérez, Esther (Comp. Hospital Virgen Blanca); Fernández Torres, Celia (Hospital Res. Ruiz de Alda Clínico MQ.); Ferré Vallés, Raimón (CE. Hospital S. Juan de Reus); Filgueira Rubio, José Santiago (CE. Clinica N. Sra. América); Flores Cid, Juan (Hospital Arnau de Vilanova); Fontanals Allue, Carlos (Centro Médico Teknon); Fort Ros, Juan (Hospital G. Vall Hebrón); Galindo Andugar, Ma Ángeles (Hospital G. Mancha Centro); García Donaire, José Antonio (Hospital 12 de Octubre); García Aparicio, Carlos (Hospital de la Marina Baja Villajoyosa-Benidorm); García Cors, Montserrat (Hospital G. de Catalunya); García de Vinuesa, Soledad (CE. Hosp. G. Marañón); García Fernández, Yolanda (Hospital de Galdakano); García Malpartida, Katherinne Eloise (Hospital Dr. Peset); García Navarro, Maria Dolores (Hospital G. Universitario Alicante); García Pardo, Antonio (Hospital Enf. Tórax Sta. Cruz Tenerife); García Pérez, Héctor (Hospital G. de Castellón); García Sánchez-Gabriel, Juan (Hospital de Cruces); García Torres, Santiago (CExt. Hospital la Plana); Giménez Palop, Olga (Hospital Parc Tauli); Giménez Pérez, Gabriel (Hospital Parc Tauli); Giner Galvañ, Vicente (Hospital Virgen de Los Lirios); Girbes Borrás, Juan (Hospital Arnau de Vilanova); Gómez Campdera, Francisco Javier (CE. Hosp. G. Marañón); Gómez Fernández, Rocío del Carmen (Hospital Ntra. Sra. del Cristal); Gómez García, Luis Antonio (Hospital Universitario Virgen del Rocío); Gómez Segado, Enrique (Hospital de la Marina Baja Villajoyosa-Benidorm); González González, Abel (Hospital G. Mancha Centro); González Igual, Jesús Javier (Hospital Com. de Barbastro); González Pina, Blas Luis (Hospital Com. del Noroeste); González Rodríguez, María Enriqueta (CE. Hospital de Jarrio); González Roncero, Francisco (Hospital Universitario Virgen del Rocío); González Sarmiento, Enrique (Hospital Clínico Universitario Valladolid); Gorostidi Pérez, Manuel (Hospital S. Agustín Avilés); Grande Villoria, Jesús (CE. Hospital G. Virgen de la Concha); Guerediaga Madariaga, Francisco. J (CE. Hospital S. Agustín Avilés); Guerrero González, Jorge (Hospital Virgen Monte Toro); Gurrutxaga Arrillaga, Nicolás (Hospital Com. de Medaro); Gutiérrez Marcos, Fernando (Hospital Príncipe de Asturias); Gutiérrez Martínez, Eduardo (Hospital 12 de Octubre); Hernández Alonso, Enrique (Hospital G. Basic O de defensa); Hernández Criado, Juan Carlos (Hospital Virgen de la Vega); Hernández Hernández, José Alberto (Hospital St. Jaume de Calella); Hernández Rodríguez, José (Hospital Clínic Prov. Barcelona); Herrero Puente, Pablo (Hospital Ntra. Sra. de Covadonga); Herreros Ruiz Valdepeñas, Benjamín (Fundación Hospital Alcorcón); Horcajo Aranda, Pedro (Hospital G. Docente Guadalajara); Hortal Cascón, Luis J (Hospital Universitario Gran Canaria Dr. Negrín); Ibarmia Lahuerta, Joseba (Hospital de Basurto); Ibrahim Basha, Abdul Aziz (Hospital de Jove); Iglesias Alonso, Luis Fernando (Hospital General Yagüe); Inglada Galiana, Luis (Hospital del Rio Hortega); Íñigo Gil, Pablo (Hospital Clínico Universitario Lozano Blesa); Iribarnegaray Valenzuela, Eduardo (CE. Hospital G. de L'hospitalet); Irigoyen Cucalón, Luis (Hospital G. Santiago Apóstol); Jericó Alba, Carlos (Hospital G. Ntra. Sra. del Mar); Junca Creus, Elisabeth (CE. Hospital Josep Trueta); Lalueza Blanco, Antonio (Hospital 12 de Octubre); Lamas Domínguez, Pablo (Hospital Xeral de Vigo); Lasso Olayo, José María (Hospital Com. de Alcañiz); Laynez Cerdeña, Pedro (Hospital Rambla); Lázaro Puente, Francisca (Hospital Clínico Universitario Lozano Blesa); Lecumberri Santamaría, Beatriz (Hospital Puerta de Hierro); León Gómez, Benjamín de (CE. Hospital Virgen Blanca); Lerma Márquez, José Luis (CE. Hospital Clínico Universitario Salamanca); Lis Muñoz, José María de (Hospital Montecelo); Logroño González, José Manuel (CE. Hospital G. San Jorge); Lombán Villanueva, José Antonio (Hospital Com. de Burela); López de Juan, Mariano (Hospital Clínico Universitario Valladolid); López Guzmán, Antonio Jesús (Hospital Ntra. Sra. de Sonsoles); López Jiménez, Manuel (Hospital G. de Móstoles); López Mesa, Manuel (Hospital Juan Grande); López Paz, José Enrique (Hospital G. y Clínico de Galicia); López Piñeiro, Casiano (Hospital de Calde); Losada González, Patricia (Hospital Son Dureta); Losfablos Callao, Francisco (Hospital Miguel Servet); Lozano Gutiérrez, Francisco (Centro de Salud de Marchena); Lozano Gutiérrez, Francisco (Hospital de Valme); Lozano Rodríguez-Mancheño, Aquiles (Hospital Universitario Reina Sofía Córdoba); Lucena Calvet, Paloma (Hospital Severo Ochoa); Llorente Viñas, Santiago (Hospital Universitario Virgen de la Arrixaca); Magdalena Méndez, Pablo (Hospital de Jove); Marcos Olivares, Santiago (Hospital Prov. Salamanca); Marchan Carranza, Enrique (Hospital G. de Ciudad Real Sescam); Marrero Arencibia, Dunia (Hospital Universitario Insular las Palmas); Martín Arribas, Alberto (Hospital Clínico Universitario Salamanca); Martín Castillo, Fidel (Hospital G. de Móstoles); Martín Hernández, F. Javier (Hospital Ntra. Sra. de la Candelaria); Martín Oterino, José Ángel (Hospital Virgen de la Vega); Martín Serradilla, José Ignacio (Hospital Río Carrión); Martínez Calvo, José Ramón (Hospital de Calde); Martínez González, Julio (Centro de Salud Alameda Perchel)); Martínez López, Vicente (CE. Hospital de la Vega Baja); Martínez Martín, F. Javier (Hospital Universitario Gran Canaria Dr. Negrín); Martínez Puerto, Ana Isabel (Hospital Universitario Virgen Macarena); Martínez Rodés, Pablo (Hospital Royo Villanova); Martínez Uso, Ignacio (Hospital de la Ribera); Martín-Luquero Ibáñez, Miguel (Hospital Com. de Benavente); Martos Pérez, Francisco (Hospital Costa del Sol); Mascaros Torres, Vicente (Clínica Quirón); Mateos Polo, Lourdes (Hospital Virgen de la Vega); Mediavilla García, Juan Diego (Hospital Res. Ruiz de Alda Clínico MQ); Melero Brezo, Manuel (Hospital de Calde); Menacho Miguel, José Antonio (Hospital Clínico Universitario Salamanca); Méndez Pérez, Maria Luisa (Hospital Ntra. Sra. de la Candelaria); Mene Fenor, Enrique (Hospital Com. Rafael Méndez); Mestron Pérez, Antonio (CE. Hosp. Creu Roja); Mico Giner, Maria Luisa (Ciudad. S. la Fe); Michán Doña, Alfredo Luis (Hospital SS. de Jerez); Mira Escartí, José Antonio (Hospital de Valme); Molina Gómez, Fernando (Hospital la Paz); Montes delgado, Rafael (Hospital Universitario Virgen del Rocío); Mora Álvaro, Francisco (CE. Hospital Clínico Universitario Lozano Blesa); Moreno Palomares, Javier (CE. Hospital G. de Segovia); Mulero Conde, Juan Luis (Hospital Com. Rafael Méndez); Navarro González, Juan Francisco (Hospital Ntra. Sra. de la Candelaria); Navarro Herrera, Juan (Hospital Universitario MQ. Jaén); Nieto Iglesias, Javier (Hospital G. de Ciudad Real Sescam); Nogués Solán, Xavier (Hospital G. Ntra. Sra. del Mar); Ojeda Pino, Antonio (Hospital Universitario Insular las Palmas); Oliván Ballabriga, Antonio (Hospital de Navarra); Olivas García, Emilio (CE. Hospital G. Albacete); Ortega López, Nicolás (Hospital Universitario Virgen de la Arrixaca); Ortiz Librero, Milagros (Hospital Severo Ochoa); Pablos Velasco, Pedro de (Hospital Universitario Gran Canaria Dr. Negrín); Paco Moya, Miguel de (Hospital Com. del Noroeste); Palacios-García Cervigón, Gregorio (Fundación Hospital Alcorcón); Palomares Ortega, Rafael (Hospital Universitario Reina Sofía Córdoba); Palomo Gil, Salvador (Hospital de Riotinto); Palos Ortega, Miguel Ángel (CE. Ctro. Hospital Cardiológico); Parra Barahona, Juan (Hospital G. SS. Mérida); Parra Zurutuza, Aitor (Hospital Com. Ntra. Sra. la Antigua); Pastor Gómez-Cornejo, Luis (CE. Hosp. G. Marañón); Pastor Mourón, Lorenzo (Hospital Miguel Servet); Paytubi Gari, Carlos (Centro Medico Teknon); Pelegrí Santos, Antonio Luis (Hospital Sagrado Corazón Alianza); Penades Cervera, Gema (Hospital G. Universitario Elche); Peña Jiménez, Daniel (Hospital Carlos Haya); Peña Somovilla, José Luis (Hospital S. Millán); Peñafiel Martínez, Francisco Javier (CE. Hospital Torrecárdenas); Pérez Castrillón, José Luis (Hospital del Río Hortega); Pérez Marín, Juan Carlos (Hospital Universitario Insular las Palmas); Pérez Tamajón, María Lourdes (Hospital Universitario de Canarias); Plana Gil, Nuria (CE. Hospital S. Juan de Reus); Portoles Suso, Antonio (Hospital Miguel Servet); Pozo Pico, Carlos del (Mutua de Terrassa); Prada Álvarez, Francisco José de la (Hospital Son Dureta); Prieta López, Ramiro de la (Hospital de Cruces); Prieto Velasco, Mario (CE. Hospital Virgen Blanca); Puñal Castellanos, Pedro (Hospital Prov. de Toledo); Quintana San José, Begoña (Hospital de Cruces); Ramírez Duque, Nieves (CE. Hospital Universitario Virgen del Roció); Ramos Salado, Juan Lucio (Hospital Perpetuo Socorro); Ramos Sánchez, Rosa (Hospital Com. Sant Antoni Abat); Reinares García, Leonardo (Hospital Clínico Universitario San Carlos Madrid); Riesgo García, Alba (Hospital Ntra. Sra. de Covadonga); Rivera Gallego, Alberto (Hospital Xeral de Vigo); Rodrigo Parra, Antonio (Hospital del Río Hortega); Rodríguez Álvarez, Sergio (Hospital G. de Ciudad Real Sescam); Rodríguez Fernández, Marta (Hospital Prov. Santiago Clínico); Rodríguez Jiménez, Celestino (Hospital 12 de Octubre); Rodríguez Pérez, José Carlos (Hospital Universitario Gran Canaria Dr. Negrín); Roldán Suárez, Cecilia (Hospital 12 de Octubre); Román Sánchez, Pilar (Hospital de Requena); Romero Bobillo, Enrique (Hospital Clínico Universitario Valladolid); Romero Jiménez, Manuel Jesús (Hospital Infanta Elena); Rosich Font, Esther (Hospital Clínic Prov. Barcelona); Rossique Delmas, Pilar (Hospital Universitario Insular las Palmas); Rovira Rovira, Josep Maria (Hospital S. Bernabé); Rubio García, José Antonio (Ambulatorio Veredillas); Saban Ruiz, José (Hospital Ramón y Cajal); Sáez-Royuela Villanueva, Alfonso (Hospital la Magdalena); San José Alonso, Javier (Hospital Río Carrión); Sánchez Casajús, Ángel Antonio (Hospital S. Millán); Sánchez Fuentes, Demetrio (Hospital Ntra. Sra. de Sonsoles); Sánchez Haya, Eloy (Hospital Donostia); Sánchez Llinares, Juan Ramón (Hospital Com. del Noroeste); Sanchís Salvador, Vicente (Hospital Lluis Alcanyis); Santamaría Olmo, Rafael (Hospital Universitario Reina Sofía Córdoba); Sanz Parras, Marisol (Hospital Son Llatzer); Saura Lujan, Isabel Ma (Hospital Universitario Virgen de la Arrixaca); Segarra Medrano, Alfonso (Hospital G. Vall Hebrón); Segura de la Morena, Julián (Hospital 12 de Octubre); Selva O'callagham, Francisco (Hospital'G. Vall Hebrón); Serrano Fernández, Cristóbal (Hospital de San Vicente); Serrato Llamas, Maria Teresa (Hospital de la Serranía); Simal Blanco, Fernando (Hospital Com. del Bierzo); Sola Aznár, Joan (Hospital Parc Tauli); Soláns Laque, Roser (Hospital G. Vall Hebrón); Sorli Redo, Luisa (CE. Hospital Ntra. Sra. del Mar); Soto Mas, José Antonio (Hospital Universitario San Cecilio); Suárez Dono, Francisco Javier (Hospital Prov. Santiago Clínico); Suárez Ortega, Saturnino (Hospital Universitario Gran Canaria Dr. Negrín); Teijo Núñez, Cristian (Comp. Hospital Virgen Blanca); Tiberio López, Gregorio (Centro de Salud Olite); Tirado Miranda, Raimundo (Hospital Com. Infanta Margarita); Tornero Molina, Fernando (Hospital Virgen de la Luz); Torralba Cabeza, Miguel Ángel (Hospital Clínico Universitario Lozano Blesa); Torregrosa Maicas, Isidro Antonio (CE. Hospital Clínico Universitario Valencia); Troya García, Jesús (Hospital Virgen de la Salud); Uriol Ribera, Miguel (Hospital Son Dureta); Valera Cortes, Alfonso (Hospital Clínico Universitario Virgen de la Victoria); Valero Díaz Lamadrid, Carmen (Hospital Marques de Valdecilla); Vázquez Álvarez, Joaquín (Hospital Ntra. Sra. de Covadonga); Verdú Berenguer, Alicia (Hospital G. Universitario Elche); Vicente Casanova, Antonio José (CE. Hospital Clínico Universitario Valencia); Vicente Más, Josép (Hospital G. Universitario Valencia); Vidal López, Fco. Javier (Hospital de Calde); Vigil Medina, Luis (Hospital G. de Móstoles); Villa Bautista, Mariano (Hospital G. de Móstoles); Villar Gómez, Irama (Hospital de Cruces); Villarreal Balza-Vallejo, Juan José (Hospital Com. de Medaro); Villarroel Bajo, África (Ambulatorio José Marva); Vinuesa García, David (Hospital Universitario San Cecilio); Vivanco Martínez, Fco. Javier (Hospital Donostia)
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Competing interests
LC is a full-time employee at the Clinic Research Department of Merk Sharp & Dohme, Spain. PC and PG have received fees from Merck Sharp & Dohme, Spain for lectures during the past five years. CF has received fees from Merck Sharp & Dohme, Spain as a consultant in statistics. FA does not declare any competing interest.
Authors' contributions
LC, PC, PG anf FA conceived the study, and participated in its design. CF designed and made the statistical analysis. LC drafted the manuscript, and all authors reviewed and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Cea-Calvo, L., Conthe, P., Gómez-Fernández, P. et al. Target organ damage and cardiovascular complications in patients with hypertension and type 2 diabetes in Spain: a cross-sectional study. Cardiovasc Diabetol 5, 23 (2006). https://doi.org/10.1186/1475-2840-5-23
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1475-2840-5-23