
Abstract
Background
We aimed to analyze outcomes of early and delayed laparoscopic cholecystectomy in the elderly in our General Surgery Division.
Methods
We analyzed 114 LC performed from the 1st of January 2008 to the 31st of December 2012 in our General Surgery division: 67 LC were performed for gallbladder stones and 47 for acute cholecystitis.
Results and discussion
Comparison between Ordinary and Emergency groups showed that drain placement and post-operative hospital stay were significatively different. There were no significative differences between Early Laparoscopic Emergency Cholecystectomy (E-ELC) and Delayed Laparoscopic Emergency Cholecystectomy (D-ELC). There weren't any differences about Team's evaluation.
Conclusion
We consider LC a safe and effective treatment for cholelitiasis and acute cholecystitis in Ordinary and Emergency setting, also in the elderly. We also demonstrate that, in our experience, LC for AC is feasible as well.
Similar content being viewed by others


Background
Laparoscopic cholecystectomy (LC) represents the gold standard treatment for cholelithiasis.
Its application gradually extended to acute cholecystitis (AC) also in the elderly. We aimed to compare outcomes of the University Section of General Surgery in "San Luigi Gonzaga" Hospital of Orbassano (Turin) with literature, evaluating timing and technique of early or delayed laparoscopic cholecystectomy in the management of acute cholecystitis in elderly patients.
Methods
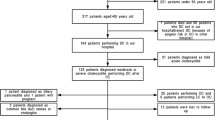
From the 1st of January 2008 to the 31st of December 2012, 114 LC were performed at the University Section of General Surgery in elderly patients (Age > 65 yrs): 67 for gallbladder stones and 47 for acute cholecystitis. The diagnosis of cholecystitis and gallbladder stones was performed basing on general conditions, physical examination, laboratory exams, radiologic findings and sepsis score. For the study we also considered: total hospital stay, time before and after surgery, duration and kind of operation, conversion to open procedure, drain and final pathological results. We excluded 29 patients from the study (17 for choledocolytiasis associated and 12 for hospitalisation > 20 days). We didn't exclude ASA III and ASA IV patients: in these patients (27,4%, 17 ASA III and 4 ASA IV) we used abdominal pressure not superior of 10 mmHg [1]. We included in the study 85 elderly patients (49 M, 36 F): Ordinary Cholecystectomy was peformed in 45 cases (Ordinary Group) and Emergency Cholecystectomy in 40 cases (Emergency Group). This last group was further divided in two groups [2–4]: E-ELC (31 patients with surgery performed before 72 hours from starting of the symptoms) and D-ELC, (9 patients with surgery performed after 72 hours until 9 day). The experience of the first operator was also considered a contributing factor. Basing on this factor, and considering laparoscopic learning curves as described in literature (29-40), we identified three subgroups of surgery teams (Table 1) in order to evaluate our results [5–11].
Statistical proportions related to the analyzed dichotomic variables, for both E-ELC and D-ELC (gender distribution in different patient groups, number of post-operative complications, conversion rate, number of drains, number of other related surgeries, presence of fever, wall thickening, effusion amount, gallbladder distension and calculosis type) were compared using Chi-square test and Fisher's exact test. Continuous variables like age distribution, post-operative hospital stay time, surgery duration and several haematochemical characteristics (WBC, CRP) were expressed as average (range) and analyzed using the Mann-Witney U test. Patient distribution according to different surgical teams was confirmed. All statistical analyses were performed using R software (version 2.6.2), and a p value of less than 0.01 was considered indicative of statistical significance.
Results and discussion
In our experience, the comparison between Ordinary and Emergency Group was no statistically significant about blood test values and ultrasonographic evidence (Table 2).
We analyzed E-ELC and D-ELC data without finding any statistically significant difference in the elderly, except for the full hospital stay duration, which was longer for D-ELC patients (Table 3). Operation time, conversion rate, and complications did not demonstrate any significant difference between the two groups. Comparison of success rates achieved by different surgeons yielded the same results, regardless of their levels of experience (Table 4). Patients can be operated after a time interval of 73 hours and up to 9 days, and receive the same benefits that would have been obtained from an earlier operation.
Conclusions
In agreement with literature [8–10], we consider LC a safe and effective treatment for AC also in the elderly. This study demonstrates that in our experience LC for AC is feasible as well. The learning curve of this procedure is feasible [11, 12]. We also believe that, whenever possible, early LC is to be preferred, above all for the significantly shortened total hospital stay. Nevertheless, the retrospective analysis of our case study, even with a smaller sample for delayed LC patients, showed that elderly patients can be operated with delayed approach and still benefit from the same advantages that would be obtained with an early operation [12–19]. In our experience, according to literature, laparoscopic cholecystectomy is a secure procedure to be performed [20–24]. We consider surgery approach more difficult in the elderly in some cases [25] but we also considered laparoscopic approach is, in general, a safe and feasible technique in acute pathology and a safe approach also in the elderly [26].
References
Catani M, Modini C: Laparoscopic cholecystectomy in acute cholecystitis: a proposal of safe and effective technique. Hepatogastroenterology. 2007, 54: 2186-91.
Chung-Mau Lo, Chi-Leung Liu, Sheung-Tat Fan, Edward Lai CS, John Wong: Prospective Randomized Study of Early Versus Delayed Laparoscopic Cholecystectomy for Acute Cholecystitis. Ann Surg. 2008, 227: 461-467.
Litwin DE, Cahan MA: Laparoscopic cholecystectomy. Surg Clin North Am. 2008, 88: 1295-313. 10.1016/j.suc.2008.07.005.
Wilson E, Gurusamy K, Gluud C, Davidson BR: Cost-utility and value-of-information analysis of early versus delayed laparoscopic cholecystectomy for acute cholecystitis. Br J Surg. 2010, 97: 210-219. 10.1002/bjs.6872.
Dàvila D, Manzanares C, Picho ML, Albors P, Cardenas F, Fuster E: Experience in the treatment (early vs. delayed) of acute cholecystitis via laparoscopy. Cirugia Espanola. 1999, 66: 233-235.
Bohacek L, David MD, Pace E: Advanced laparoscopic training and outcomes in laparoscopic cholecystectomy. Can J Surg. 2009, 52: 223-224.
Ballantyne GH, Ewing D, Capella RF: The learning curve measured by operating times for laparoscopic and open gastric bypass: roles of surgeon's experience, institutional experience, body mass index and fellowship training. Obes Surg. 2005, 15: 172-82. 10.1381/0960892053268507.
Gill J, Booth MI, Stratford J, Dehn TC: The extended learning curve for laparoscopic fundoplication: a cohort analysis of 400 consecutive cases. J Gastrointest Surg. 2007, 11: 487-92. 10.1007/s11605-007-0132-0.
Avital S, Hermon H, Greenberg R, Karin E, Skornick Y: Learning curve in laparoscopic colorectal surgery: our first 100 patients. Isr Med Assoc J. 2006, 683-6. 8
Rispoli C, Rocco N, Iannone L, Amato B: Developing guidelines in geriatric surgery: role of the grade system. BMC Geriatrics. 2009, 9 (SUPPL.1): A99-
Li GX, Yan HT, Yu J, Lei ST, Xue Q, Cheng X: Learning curve of laparoscopic resection for rectal cancer. 2006, 26: 535-8.
Kauvar DS, Brown BD, Braswell AW, Harnisch MJ: Laparoscopic cholecystectomy in the elderly: increased operative complications and conversions to laparotomy. Laparoendosc Adv Surg Tech A. 2005, 15: 379-82. 10.1089/lap.2005.15.379.
Moyson J, Thill V, Simoens Ch, Smets D, Debergh N, Mendes da Costa P: Laparoscopic cholecystectomy for acute cholecystitis in the elderly: a retrospective study of 100 patients. Hepatogastroenterology. 2008, 55: 1975-80.
Polychronidis A, Botaitis S, Tsaroucha A, Tripsianis G, Bounovas A, Pitiakoudis M, Simopoulos C: Laparoscopic cholecystectomy in elderly patients. J Gastrointestin Liver Dis. 2008, 309-13. 17
Kirshtein B, Bayme M, Bolotin A, Mizrahi S, Lantsberg L: Laparoscopic cholecystectomy for acute cholecystitis in the elderly: is it safe?. Surg Laparosc Endosc Percutan Tech. 2008, 18: 334-9. 10.1097/SLE.0b013e318171525d.
Majeski J: Laparoscopic cholecystectomy in geriatric patients. Am J Surg. 2004, 187: 747-50. 10.1016/j.amjsurg.2003.11.031.
Stanisić V, Bakić M, Magdelinić M, Kolasinac H, Miladinović M: Laparoscopic cholecystectomy in elderly patients. Acta Chir Iugosl. 2009, 56: 87-91. 10.2298/ACI0902087S.
Tambyraja AL, Kumar S, Nixon SJ: Outcome of laparoscopic cholecystectomy in patients 80 years and older. World J Surg. 2004, 28: 745-8. 10.1007/s00268-004-7378-4.
Aprea G, Canfora A, Ferronetti A, Giugliano A, Guida F, Braun A, Battaglini Ciciriello M, Tovecci F, Mastrobuoni G, Cardin F, Amato B: Morpho-functional gastric pre-and post-operative changes in elderly patients undergoing laparoscopic cholecystectomy for gallstone related disease. BMC Surgery. 2012, 12 (Suppl 1): S1-10.1186/1471-2482-12-S1-S1.
Lau H, Lo CY, Patil NG, Yuen WK: Early versus delayed-interval laparoscopic cholecystectomy for acute cholecystitis: a metaanalysis. Surg Endosc. 2006, 20: 82-7. 10.1007/s00464-005-0100-2.
Johansson M, Thune A, Blomqvist A, Nelvin L, Lundell L: Management of acute cholecystitis in the laparoscopic era: results of a prospective, randomized clinical trial. J Gastrointest Surg. 2003, 7: 642-645. 10.1016/S1091-255X(03)00065-9.
Lo C, Liu C, Fan ST, Lai EC, Wong J: Prospective randomized study of early versus delayed laparoscopic cholecystectomy for acute cholecystitis. Ann Surg. 1998, 227: 461-467. 10.1097/00000658-199804000-00001.
Solej M, Martino V, Mao P, Enrico S, Rosa R, Fornari M, Destefano I, Ferrarese AG, Gibin E, Bindi F, Falcone A, Ala U, Nano M: Early versus delayed laparoscopic cholecystectomy for acute cholecystitis. Minerva Chirurgica. 2012, 67 (5): 381-387.
Ferrarese A, Martino V, Nano M: Elective and emergency laparoscopic cholecystectomy in the elderly: early or delayed approach. BMC Geriatrics. 2011, 11 (Suppl 1): A14-10.1186/1471-2318-11-S1-A14.
Ferrarese A, Martino V, Falcone A, Solej M, Destefano I: Perforated duodenal diverticulum: case report and short review of the literature. su Chirurgia,
Ferrarese A, Martino V, Nano M: Wound defects in the elderly: our experience. BMC Geriatrics. 2011, 11 (Suppl 1): A15-10.1186/1471-2318-11-S1-A15.
Declarations
Funding for this article came from personal funds.
This article has been published as part of BMC Surgery Volume 13 Supplement 2, 2013: Proceedings from the 26th National Congress of the Italian Society of Geriatric Surgery. The full contents of the supplement are available online at http://www.biomedcentral.com/bmcsurg/supplements/13/S2
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
AGF: conception and design, interpretration of data, given final approval of the version to be published.
SE: conception and design, interpretration of data, given final approval of the version to be published.
MS: acquisition of data, drafting the manuscript, given final approval of the version to be published.
AF: acquisition of data, drafting the manuscript, given final approval of the version to be published.
SC: acquisition of data, drafting the manuscript, given the final approval of the version to be published.
GP: acquisition of data, drafting the manuscript, given the final approval of the version to be published.
SM: critical revision, interpretation of data, given final approval of the version to be published
VM: critical revision, interpretation of data, given final approval of the version to be published
Mario Solej, Stefano Enrico, Alessandro Falcone, Silvia Catalano, Giada Pozzi, Silvia Marola and Valter Martino contributed equally to this work.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an open access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Ferrarese, A.G., Solej, M., Enrico, S. et al. Elective and emergency laparoscopic cholecystectomy in the elderly: our experience. BMC Surg 13 (Suppl 2), S21 (2013). https://doi.org/10.1186/1471-2482-13-S2-S21
Published:
DOI: https://doi.org/10.1186/1471-2482-13-S2-S21