
Abstract
Background
Leptin is an hormone that regulates body weight. Studies have shown increasing leptin concentrations according to body mass index (BMI) and intermittent hypoxia.
Our aim is to evaluate the basal leptin levels in OSA patients and its possible relation to OSA severity, independently of confounders and investigate the Autoadjusting-CPAP effect on leptin values.
Methods
In ninety eight male patients with moderate to severe OSA leptin serum levels were evaluated before therapy, 9 days and 6 months after therapy.
Results
In this group mean age was 55.3 years, mean BMI was 33.2 Kg/m2 and mean Apnoea- Hypopnea Index (AHI) was 51.7/h. Mean basal serum leptin value was 12.1 ug/L. Univariate analysis showed a significant correlation between serum leptin values and BMI (R = 0.68; p < 0.001), waist-hip ratio (R = 0.283; p = 0.004) and AHI (R = 0.198; p = 0.048); in stepwise multiple regression analysis only BMI (p < 0.001) was a predictor of serum leptin values.
One week after therapy, mean leptin serum level decreased to 11.0 ug/L and 6 months after it was 11.4 ug/L. (p = 0.56 and p = 0.387, respectively)
Conclusion
Baseline leptin serum levels positively correlate with BMI, fat distributioand OSA severity.
BMI is the only predictor of basal leptin levels.
Treatment with Autoadjusting-CPAP has a small effect on leptin levels.
Similar content being viewed by others


Background
Obstructive Sleep Apnoea (OSA) is a common disorder with a prevalence of 2% to 4% in middle-aged adults [1].
The association between obesity and OSA is strong and well described. Obesity is a major risk factor for OSA, which occurs in up to 50% of obese men [1–6]. In addition, approximately 70% patients with OSA are obese [7]. It is known that every 10-Kg increment in body weight increases OSA risk twofold [8].
Leptin is a hormone with well Known functions concerning body composition, energy homeostasis and feeding behavior in humans [9–11]. It is an 167-amino acids peptide hormone produced predominantly in white adipose tissue [9–11]. Leptin circulates in the plasma in a free-form state or bound to leptin-binding proteins [11]. It acts by binding to specific receptors in the hypothalamus to decrease appetite and increase energy expenditure [9–14]. Leptin inhibits the synthesis of hypotalamic neuropeptide y (NPY), a potent stimulator of food intake, furthermore, downregulation of NPY increases sympathetic nervous system outflow enhancing energy expenditure [9–18].
In fact, leptin informs the brain about the size of adipose stores and has been thought to be the obesity hormone regulator [10].
The dramatic weight reduction observed in ob/ob mice in result to leptin administration, raised expectations that human obesity might also be a leptin deficient state treatable with exogenous leptin administration [19, 20]. However, unlike the tight relationship present between obesity and serum leptin levels in mice, human obesity seems to be associated with more possible derrangements from leptin deficiency to leptin resistance [21, 22].
Leptin levels increase exponentially with increasing body weight [11, 22, 23] and previous studies [22, 24, 25] have reported a significant correlation between measures of body fat and circulating concentrations of leptin in adults.
Under experimental conditions, intermittent hypoxia stimulates leptin production and a number of studies have demonstrated that serum leptin levels are elevated in OSA patients, independently of obesity [18, 26–32] despite some couldn't find that relationship when controlled for body fat [12, 33, 34]. If OSA is truly associated with increased leptin serum levels independent of obesity, the causal link remains unclear. Rodent studies [35, 36] provided evidence for a leptin influence in breathing stability, and thus predisposing individuals to develop OSA. In alternative, OSA may be a cause of elevated leptin serum levels through the effects of hypoxemia, sleep fragmentation or heightened sympathetic activity. Data showing leptin serum levels reduction after CPAP nocturnal usage in OSA patients [32, 34, 37–41] reinforces this idea.
The present study was conducted to evaluate the basal serum leptin levels in OSA patients and its possible relation to OSA severity. This study has also the purpose of understanding the Autoadjusting-CPAP effect on leptin circulating levels after short and long term treatment, as this effect has not been outlined yet, and the automated pressure can play a different role in leptin levels variation than that of fixed CPAP. Thus we try to clarify the relationship between leptin and sleep apneic activity, independently of confounders.
Methods
Study design
This trial was designed as a prospective study. All patients gave written informed consent to participate in the trial. The study protocol was approved by the Hospital Ethics Committe and the study was performed in accordance with the guidelines of the Declaration of Helsinki and its current revision.
Subjects
One hundred and two male consecutive patients referred for suspected sleep disordered breathing to our Sleep Disordered Breathing Clinic were included in the study, between February 2005 and March 2006.
All patients presented moderate/severe OSA (AHI > 20/h) confirmed by domiciliary sleep study.
Exclusion criteria were stablished previously: neoplastic diseases, systemic inflammatory chronic diseases, active infectious diseases, systemic long term corticotherapy and female gender.
All but four patients concluded the study (n = 98). Those who failed to conclude the protocol were due to Autoadjusting-CPAP intolerance.
Study procedures
An overnight sleep study was performed using a five-channel recording device (Alphascreen; Vyasis). This device produces a computorized recording of variations in oronasal airflow (measured by nasal cannula), body position, wrist actimetry, pulse rate and arterial oxygen saturation (measured by finger pulse oximetry). The device estimates the total sleep time from the wrist actimetry registry, eliminating those periods with high activity. It automatically calculates the number of apnoeas plus hypopnoeas per hour of estimated sleep time (automatic respiratory disturbance index) and it also provides information of desaturations > 4% per hour of estimated sleep time and the cumulative percentages of sleep time under 90% oxygen saturation. In all cases, sleep technicians carried out a manual analysis of the recordings, by counting apnoea (events of airflow cessation lasting for at least 10 seconds) and hypopnoea episodes (events of airflow reduction to 20 to 50% of the previously observed lasting for at least 10 seconds, joined with a 4% dip in oxygen saturation and/or an arousal), dividing the total number of these episodes by the sleep time in hours, thus obtaining the manual apnoea/hypopnoea index (AHI) according to established criteria [42].
Auto-CPAP therapy was prescribed to all patients with a minimum pressure of 4 and a maximum pressure of 15 cmH20.
24-hour Ambulatory Blood Pressure (Spacelab, Inc 90207 Neural) was performed in all but 3 patients who refused the examination as they considered the arm disconfort intolerable.
Fasting morning venous blood samples were collected between 8–10 a.m. before treatment, one week after and finally 6 months after the treatment initiation.
Blood samples were immediately sent to the laboratory for estimation of glucose and lipids, while a specimen of clotted blood was centrifuged at 4000 g for 20 min for serum, which was stored at -26°C in eppendorfs® until leptin analysis was performed.
Serum leptin concentrations were measured in duplicates with a highly sensitive radioimmunoassay [43] (Linco Res; St. Louis MO). The sensitivity of this assay was 0,5 ng/mL, the specificity was 100% and the interassay coefficient of variation was 4,6%.
Statistical Analysis
Data were analyzed using SPSS, release 14.0, and described as mean values and their respective standard deviation for normally, or as median values and corresponding 25th and 75th centiles for clearly non-normally distributed variables. Counts and proportions are reported for categorical variables. Proportions were compared using Chi-square test or Fisher's exact test whenever appropriate. Means and mean differences of leptin levels between the second and the first period of observations as well as between the third and the first periods of observation were compared by ANOVA or by non-parametric equivalent.
Linear multiple regression models were used to estimate the magnitude of the association between leptin levels and the studied determinants.
Results
Sample Characteristics
Table 1 summarizes the sample characteristics.
Table 2 shows the patients distribution according to Bray's obesity categories [44].
During the 6 months of the study, patients couldn't loose significant weight (mean baseline weight = 94.4 Kg; mean final weight = 94.1 Kg; p = 0.545).
Table 3 summarizes sleep study information.
Habits and Comorbidities
In this population 42.5% patients were non-smokers; 39.6% former- smokers (> 1 year without smoking habits) and 17.9% had active smoking habits.
Arterial Hypertension (AH) was found, according to 24-hour ambulatory blood pressure results, in 47.2% cases, being 2.8% nocturnal AH.
Congestive heart failure was present in 9.4% patients, according to clinical symptoms and used medication. History of stroke, acute myocardial infarction (AMI) and angina was present in 15.1%, 7.5% and 1.9% patients, respectively.
Blood analysis showed that 75.5% patients had high serum lipid values (total cholesterol > 2.00 g/L; LDL > 1.30 g/L; triglicerides > 1.50 g/L) and 34.9% showed glucose intolerance (fasting glucose > 1.15 g/L; HgA1c > 6%).
Leptin
Leptin serum levels are showed in table 4.
Sixty percent of patients presented elevated basal leptin levels. The maximum value was 56.0 ug/L. The patients with elevated basal serum leptin levels had a higher BMI than the others (p < 0,001) but did not present a central fat distribution (p = 0.052).
Leptin levels decrease after short and long-term Auto-CPAP therapy were not statistically significant.
Confounders analysis
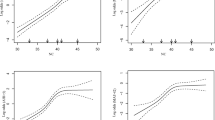
We analyzed whether age, BMI, fat distribution (waist-hip ratio), OSA severity (AHI, dessaturation index, minimum 02 saturation), serum lipids and glucose intolerance could be correlated with basal serum leptin levels or not.
An univariate analysis showed a significant correlation between serum leptin values and BMI (R = 0.68; p < 0.001), waist-hip ratio (R = 0.283; p = 0.004) and AHI (R = 0.198; p = 0.048).
In stepwise multiple regression analysis only BMI (p < 0.001) was a predictor of basal serum leptin values and AHI was not found to be significant.
Auto-CPAP compliance
Compliance with Auto-CPAP was good but it was not related to leptin decrease (table 5). Pressure on 90% nighttime decreased significantly during the study (mean baseline p90 = 10.8 cmH20; mean final p90 = 10.1; p < 0,001) and the mean residual AHI was 2.7/h ± 1.7.
Discussion
Obesity is the major factor regulating circulating leptin [24, 25, 45] which is also influenced by gender and age [23, 46].
In this study, the authors found a strong and highly significant positive correlation between obesity (BMI) and serum leptin levels at baseline (p < 0.001) as others have demonstrated [11, 22–25, 45, 47].
Several previous studies have reported increased plasma leptin levels in patients with OSA [29, 37, 42, 48], however the relationship between leptin and OSA is far from being resolved mainly because the potential confounding role of obesity.
We found that leptin levels are clearly elevated in OSA patients (mean basal value = 12.1 ± 12.2 ug/L; men normal range: 3.8 ± 1.8 ug/L) but these levels do not correlate with OSA severity when considering confounders as obesity and fat distribution. In this study, after performing multiple regression analysis, the BMI was the only predictor of baseline leptin serum levels. Also, some authors could not find correlation between the OSA severity and the leptin values when corrected for obesity [12, 33] but others did [26–30]. The latter studies included lower number of patients when compared to the former and we could speculate about the importance of the sample magnitude to acquire statistical significance in differences encountered.
We found that Auto-CPAP reduced only marginally leptin plasma levels both in short and long term treatment (6 months). This may seem in contrast with previous studies that have generally shown that leptin levels decrease significantly with CPAP [36–41, 48], but these changes were generally small in absolute amount and not very different from those determined here. Furthermore, although clinical and physiological efficacy of Auto-CPAP is equivalent to fixed CPAP [18, 32] and despite the conclusions of numerous studies about Auto-CPAP efficacy [49–55] in controlling respiratory events and hypoxemia that is presumably implicated in plasma leptin levels [18, 32], we cannot exclude that nighttime pressure variation with Auto-CPAP can affect leptin levels in a different way than fixed CPAP does.
In summary, taking all these observations into account our findings suggest that the increased leptin levels described so far in patients with OSA is mostly associated with obesity and not with the disease itself or its severity; accordingly short and long term treatment with CPAP has a small effect on leptin plasma levels and Auto-CPAP therapy compliance is not related with the leptin values decrease.
As our patients didn't demonstrate a significant weight loss, this variable could not be studied as a potential influencing factor in leptin levels.
Some characteristics of our study deserve comment.
In order to get a more homogenous sample in this study, the authors decided not to include women because of gender effect on serum leptin circulating values. Leptin serum levels are significantly higher in pre- and post-menopausal female when compared to male, even after correction for differences in body composition [23, 46]. This sexual dimorphism is apparently due to estrogen and progesterone effects and eventually to an androgen supressive effect on leptin [44].
The authors do not consider the OSA diagnosis based on a domiciliary sleep study a limitation of the present study as this diagnosis tool has already been compared to polysomnography showing to be a viable, accurate, satisfactory, useful and cost effective way of diagnosing OSA [56, 57].
The lack of a control group can be seen as a limitation of this study. Nevertheless we could demonstrate that OSA patients have elevated serum leptin levels and we could establish a significant positive correlation between BMI and leptin levels.
Conclusion
OSA patients show elevated serum plasma levels.
BMI constituted itself as the only predictor of baseline leptin levels.
Short- and long-term Auto-CPAP therapy produces a small and not significant reduction in plasma leptin levels.
References
Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S: The occurrence of Sleep-Disordered Breathing among middle-aged adults. N Engl J Med. 1993, 328: 1230-1235. 10.1056/NEJM199304293281704.
Vgontzas NA, Tan TL, Bixler EO, Martin LF, Shubert D, Kales A: Sleep apnea and sleep disruption in obese patients. Arch Intern Med. 1994, 154: 1705-1711. 10.1001/archinte.154.15.1705.
Young T, Shahar E, Nieto FJ, Redline S, Newman AB, Gottlieb DJ, Walsleben JA, Finn L, Enright P, Samet JM: Predictors of sleep-disordered breathing in community-dwelling adults. Arch Intern Med. 2002, 162 (8): 893-900. 10.1001/archinte.162.8.893.
van Boxem TJM, de Groot GH: Prevalence and severity of sleep disordered breathing in a group of morbidly obese patients. Neth J Med. 1999, 54 (5): 202-206. 10.1016/S0300-2977(98)00139-9.
Richman RM, Elliott LM, Burns CM, Bearpark HM, Steinbeck KS, Caterson ID: The prevalence of obstructive sleep apnoea in an obese female population. Int J Obes Relat Metab Disord. 1994, 18 (3): 173-177.
Resta O, Foschino-Barbaro MP, Legari G, Talamo S, Bonfitto P, Palumbo A, Minenna A, Giorgino R, Pergola GD: Sleep-related breathing disorders, loud snoring and excessive daytime sleepiness in obese subjects. Int J Obes Relat Metab Disord. 2001, 25 (5): 669-675. 10.1038/sj.ijo.0801603.
Malhotra Atul, White David: Obstructive sleep apnoea. Lancet. 2002, 360 (9328): 237-245. 10.1016/S0140-6736(02)09464-3.
Gami AS, Caples SM, Somers VK: Obesity and obstructive sleep apnea. Endocrinol Metab Clin N Am. 2003, 32: 869-894. 10.1016/S0889-8529(03)00069-0.
Haynes WG, Morgan DA, Walsh SA, Mark AL, Sivitz WI: Receptor-mediated regional sympathetic nerve activation by leptin. J Clin Invest. 1997, 100: 270-278. 10.1172/JCI119532.
Lima J: Leptin and neuroendocrinology. Arqui Med. 2002, 16 (2): 115-120.
Marik PE: Leptin, obesity, and obstructive sleep apnea. Chest. 2000, 118 (3): 569-571. 10.1378/chest.118.3.569.
Patel SR, Palmer LJ, Larkin EK, Jenny NS, White DP, Redline SMD: Relationship between obstructive sleep apnea and diurnal leptin rhythms. Sleep. 2004, 27 (2): 235-239.
Hakansson ML, Brown H, Ghilardi N, Skoda RC, Meister B: Leptin receptor immunoreactivity in chemically defined target neurons of the hypothalamus. J Neurosci. 1998, 1881: 559-572.
Auwerx J, Staels B: Leptin. The Lancet. 1998, 351: 737-742. 10.1016/S0140-6736(97)06348-4.
Stephens TW, Basinski M, Bristow PK, Bue-Valleskey JM, Burgett SG, Craft L, Hale J, Hoffmann J, Hsiung HM, Kriauciunas A, Mackellar W, Rosteck PR, Schoner B, Smith D, Tinsley FC, Zhang XY, Heiman M: The role of neuropeptide Y in the antiobesity action of the obese gene product. Nature. 1995, 377: 530-532. 10.1038/377530a0.
Erickson JC, Hollopeter G, Palmiter RD: Attenuation of the obesity syndrome of the ob/ob mice by the loss of neuropeptide Y. Science. 1996, 274: 1704-1707. 10.1126/science.274.5293.1704.
Collins S, Kuhn CM, Petro AE, Swick AG, Chrunyk BA, Surwit RS: Role of leptin in fat regulation. Nature. 1996, 380: 677-10.1038/380677a0.
Rubinsztajn R, Kumor M, Byskiniewicz K, Bielicki P, Chazan R: Serum leptin concentration and sympathetic activation estimated on the adrenalin and noradrenalin serum concentration in patients with obstructive sleep apnea. Pol Arch Med Wewn. 2005, 113 (6): 544-551.
Pelleymounter MA, Cullen MJ, Baker MB, Hecht R, Winters D, Boone T, Collins F: Effects of the obese gene product on body weight regulation in ob/ob mice. Science. 1995, 269: 540-543. 10.1126/science.7624776.
Haalas JL, Gajiwala KS, Maffei M, Cohen SL, Chait BT, Rabinowitz D, Lallone RL, Burley SK, Friedman JM: Weight-reducing effectsof the plasma protein encoded by the obese gene. Science. 1995, 269: 543-546. 10.1126/science.7624777.
O'Donnell CP, Tankersley CG, Polotsky VP, Schwartz AR, Smith PL: Leptin, obesity, and respiratory function. Respir Physiol. 2000, 119 (2–3): 163-170. 10.1016/S0034-5687(99)00111-5.
Friedman JM, Halaas JL: Leptin and the regulation of body weight in mammals. Nature. 1998, 395: 763-770. 10.1038/27376.
Ostlund RE, Yang JW, Klein S, Gingerich R: Relation between plasma leptin concentration and body fat, gender, diet, age, and metabolic covariates. J Clin Endocrinol Metab. 2005, 81 (11): 3909-3913. 10.1210/jc.81.11.3909.
Maffei M, Halaas J, Ravussin E, Pratley RE, Lee GH, Zhang Y, Fei H, Kin S, Lallone R, Ranganathan S, Kern PA, Friedman JM: Leptin levels in human and rodent: measurement of plasma leptin and ob RNA in obese and weight-reduced subjects. Nature Medicine. 1995, 1: 1155-1161. 10.1038/nm1195-1155.
Considine RV, Sinha MK, Heiman ML, Kriauciunas A, Stephens TW, Nyce MR, Ohanneslan JP, Marco CC, Mkee LJ, Bauer TL, Caro JF: Serum immunoreactive-leptin concentrations in normal-weight and obese humans. N Engl J Med. 1996, 334: 292-295. 10.1056/NEJM199602013340503.
Jin G, Wang W, Kang J, Wu Y, Hou X, Yu R: Study of serum leptin level in patients with obstructive sleep apnea. Zhonghua Jie He He Hu Xi Za Zhi. 2002, 25 (4): 204-206.
Manzella D, Parillo M, Razzino T, Gnasso P, Buonanno S, Gargiulo A, Caputi M, Paolisso G: Soluble leptin receptor and insulin resistance as determinant of sleep apnea. Int J Obes Relat Metab Disord. 2002, 26 (3): 370-5. 10.1038/sj.ijo.0801939.
Ozturk L, Ünal M, Tamer L, Celikoglu F: The association of the severity of obstructive sleep apnea with plasma leptin levels. Arch Otolaryngol Head Neck Surg. 2003, 129 (5): 538-540. 10.1001/archotol.129.5.538.
Phillips BG, Kato M, Narkiewicz K, Choe I, Somers VK: Increases in leptin levels, sympathetic drive, and weight gain in obstructive sleep apnea. Am J Physiol Heart Circ Physiol. 2000, 279 (1): H234-237.
Ciftci TU, Kokturk O, Bukan N, Bilgihan A: Leptin and ghrelin levels in patients with obstructive sleep apnea syndrome. Respiration. 2005, 72 (4): 395-401. 10.1159/000086254.
Vgontzas AN, Papanicolaou DA, Bixler EO, Hopper K, Lotsikas A, Lin HM, Kales A, Chrousos GP: Sleep apnea and daytime sleepiness and fatigue: relation to visceral obesity, insulin resistance, and hypercytokinemia. J Clin Endocrinol Metab. 2000, 85: 1151-1158. 10.1210/jc.85.3.1151.
Ip MS, Lam KS, Ho C, Tsang KW, Lam W: Serum leptin and vascular risk factors in obstructive sleep apnea. Chest. 2000, 118: 580-586. 10.1378/chest.118.3.580.
Schafer H, Pauleit D, Sudhop T, Gouni-Berthold I, Ewig S, Berthold HK: Body fat distribution, serum leptin, and cardiovascular risk factors in men with obstructive sleep apnea. Chest. 2002, 122 (3): 829-839. 10.1378/chest.122.3.829.
Barceló A, Barbé F, Llompart E, de la Peña M, Durán-Cantolla J, Ladaria A, Bosch M, Guerra L, Agustí AG: Neuropeptide Y and leptin in patients with obstructive sleep apnea syndrome. Am J respir Crit Care Med. 2005, 171 (2): 183-187. 10.1164/rccm.200405-579OC.
Tankersley CG, O'Donnell C, Daood MJ, Watchko JF, Mitzner W, Schwartz A, Smith P: Leptin attenuates respiratory complications associated with the obese phenotype. J Appl Physiol. 1998, 85: 2261-2269.
O'Donnell CP, Schaub CD, Haines AS, Berkowitz DE, Tankersley CG, Schwartz AR, Smith PL: Leptin prevents respiratory depression in obesity. Am J respir Crit Care Med. 1999, 159: 1477-1484.
Harsch I, Konturek PC, Koebnick C, Kuehnlein PP, Fuchs FS, Pour Schahin S, Wiest GH, Hahn EG, Lohmann T, Ficker JH: Leptin and ghrelin levels in patients with obstructive seep apnoea: effect of CPAP treatment. Eur Respir J. 2003, 22 (2): 251-257. 10.1183/09031936.03.00010103.
Huang R, Huang XZ, Wang HG, Li M, Xiao Y: Effects of nasal continuous positive airway pressure on serum leptin concentration and the metabolic parameters in obstructive sleep apnea hypopnea syndrome. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2004, 26 (2): 168-171.
Sanner BM, Kollhosser P, Buechner N, Zidek W, Tepel M: Influence of treatment on leptin levels in patients with obstructive sleep apnoea. Eur Respir. 2004, 23 (4): 601-604. 10.1183/09031936.04.00067804.
Shimizu K, Chin K, Nakamura T, Masuzaki H, Ogawa Y, Hosokawa R, Niimi A, Hattori N, Nohara R, Sasayama S, Nakao K, Mishima M, Nakamura T, Ohi M: Plasma leptin levels and cardiac sympathetic function in patients with obstructive sleep apnoea-hypopnoea syndrome. Thorax. 2002, 57 (5): 429-434. 10.1136/thorax.57.5.429.
Tharaux PL: Effect of sleep apnea syndrome on the vascular endothelium. Rev Neurol. 2003, 159 (11): 6s102-106.
The report of an American Academy of Sleep Medicine Task Force: Sleep- related breathing disorders in adults: recommendations for syndrome definition and measurement techniques in clinical research. Sleep. 1999, 22 (5): 667-689.
Ma Z, Gingerich RL, Santiago JV, Klein S, Smith CH, Landt M: Radioimmunoassay of leptin in human plasma. Clin Chem. 1996, 42: 942-946.
Bray GA: Pathophysiology of obesity. Am J Clin Nutr. 1992, 55: 4883-4943.
Mantzoros CS: The role of leptin in human obesity and disease: a review of current evidence. Ann Intern Med. 1999, 130: 671-680.
Rosenbaum M, Nicolson M, Hirsch J, Heymsfield SB, Gallagher D, Chu F, Leibel RL: Effects of gender, body composition, and menopause on plasma concenrations of leptin. J Clin Endocrinol Metab. 1996, 81: 3424-3427. 10.1210/jc.81.9.3424.
Tatsumi K, Kasahara Y, Kurosu K, Tanabe N, Takiguchi Y, Kuriyama T: Sleep oxygen desaturation and circulating leptin in obstructive sleep apnea-hypopnea syndrome. Chest. 2005, 127: 716-721. 10.1378/chest.127.3.716.
Chin K, Shimizu K, Nakamura T, Narai N, Masuzaki H, Ogawa Y, Mishima M, Nakamura T, Nakao K, Ohi M: Changes in intra-abdominal visceral fat and serum leptin levels in patients with obstructive sleep apnea sydrome following nasal continuous positive airway pressure therapy. Circulation. 1999, 100: 706-712.
Massie CA, McArdle N, Hart RW, Schmidt-Nowara WW, Lankford A, Hudgel DW, Gordon N, Douglas NJ: Comparison between automatic and fixed positive airway pressure therapy in the home. Am J Respir Crit Care Med. 2003, 167: 20-23. 10.1164/rccm.200201-022OC.
Ayas NT, Patel SR, Malhotra A, Schulzer M, Malhotra M, Jung D, Fleetham J, White DP: Auto-titrating versus standard continuous positive airway pressure for the treatment of obstructive sleep apnea: Results of a meta-analysis. Sleep. 2004, 27: 249-253.
Behbehani K, Yen FC, Lucas EA, Burk JR: A sleep laboratory evaluation of an automatic positive airway pressure system for treatment of obstructive sleep apnea. Sleep. 1998, 21: 485-491.
Teschler H, Wessendorf TE, Farhat AA, Konietzko N, Berthon-Jones M: Two months auto-adjusting versus conventional nCPAP for obstructive sleep apnoea syndrome. Eur Respir J. 2000, 15: 990-995. 10.1034/j.1399-3003.2000.01503.x.
d'Ortho MP, Grillier-Lanoir V, Levy P, Goldenberg F, Corriger E, Harf A, Lofaso F: Constant vs automatic continuous positive airway pressure therapy: home evaluation. Chest. 2000, 118: 1010-1017. 10.1378/chest.118.4.1010.
Noseda A, Kempenaers C, Kerkhofs M, Braun S, Linkowski P, Jann E: Constant vs auto-continuous positive airway pressure in patients with sleep apnea hypopnea syndrome and a high variability in pressure requirement. Chest. 2004, 126: 31-37. 10.1378/chest.126.1.31.
Marrone O, Insalaco G, Bonsignore MR, Romano S, Salvaggio A, Bonsignore G: Sleep structure correlates of continuous positive airway pressure variations during application of an autotitrating continuous positive airway pressure machine in patients with obstructive sleep apnea syndrome. Chest. 2002, 121: 759-767. 10.1378/chest.121.3.759.
Golpe R, Jiménez A, Carpizo R: Home sleep studies in the assessment of sleep apnea/hypopnea syndrome. Chest. 2002, 122: 1156-1161. 10.1378/chest.122.4.1156.
Dingli K, Coleman EL, Nennelle M, Finch SP, Wraith PK, Mackay TW, Douglas NJ: Evaluation of a portable device for diagnosing the sleep apnea/hypopnoea syndrome. Eur respir J. 2003, 21: 253-259. 10.1183/09031936.03.00298103.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2466/8/21/prepub
Acknowledgements
The authors would like to sincerely thank nurses Emília Araújo, Paula Martins and Edgar Mateus for their colaboration on blood sample collections and Dr. Conceição Gonçalves for the laboratory analysis performance as to all Sleep Technicians who manually reviewed all sleep studies.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
MD conceived the study, participated in its design, data acquisition, coordination and drafted the manuscript. JCW conceived the study, participated in its design and data acquisition. JTG coordinated the chemical analysis. ACS performed the statistical analysis. JA participated in data acquisition. JAM conceived the study and participated in its design. All the authors read and approved the final manuscript.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Drummond, M., Winck, J.C., Guimarães, J.T. et al. Autoadjusting-CPAP effect on serum Leptin concentrations in Obstructive Sleep Apnoea patients. BMC Pulm Med 8, 21 (2008). https://doi.org/10.1186/1471-2466-8-21
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2466-8-21