
Abstract
Background
Air pollution is known to be a leading cause of respiratory symptoms. Many cross-sectional studies reported that air pollution caused respiratory disease in Japanese individuals in the 1960s. Japan has laws regulating air pollution levels and providing compensation for victims of pollution-related respiratory disease. However, long-term changes in respiratory function and symptoms in individuals who were exposed to air pollution in the 1960s have not been well studied. This study aimed to investigate longitudinal respiratory function and symptoms in older, non-smoking, long-term officially-acknowledged victims of pollution-related illness.
Methods
The study included 563 officially-acknowledged victims of pollution-related illness living in Kurashiki, Okayama who were aged ≥ 65 years in 2009. Data were retrospectively collected from yearly respiratory symptom questionnaires and spirometry examinations conducted from 2000 to 2009.
Results
Respiratory function declined significantly from 2000 to 2009 (p < 0.01), but the mean annual changes were relatively small. The change in mean vital capacity was −40.5 ml/year in males and −32.7 ml/year in females, and the change in mean forced expiratory volume in 1 second was −27.6 ml/year in males and −23.9 ml/year in females. Dyspnea was the only symptom that worsened significantly from 2000 to 2009 in both sexes (males: p < 0.05, females: p < 0.01).
Conclusions
Our results suggest that the high concentrations of air pollutants around 1970 resulted in a decrease in respiratory function and an increase in respiratory symptoms in the study population. From 2000 to 2009, the mean annual changes in respiratory function were within the normal range, even though the severity of dyspnea worsened. The changes in respiratory function and symptoms over the study period were probably due to aging. The laws governing air pollution levels and providing compensation for officially-acknowledged victims of pollution-related illness in Japan may be effective for respiratory disease cause by pollution.
Similar content being viewed by others


Background
Air pollution is a serious problem throughout the world. Epidemiological studies have reported that air pollution is associated with adverse respiratory effects [1–7] and increased mortality [8–10]. Some areas of Japan experienced high levels of air pollution during the period of rapid economic growth after World War II and many people who lived in these areas complained about respiratory symptoms. In response, the Japanese government implemented air pollution laws. The Basic Law for Environmental Pollution Control was implemented in 1967, and air pollution has decreased since then. The Pollution-Related Health Damage Special Measures Law was implemented in 1969. Japanese citizens who experience health impairment caused by air pollution are certified by prefectural government committees. These officially-acknowledged victims of pollution-related illness qualify for treatment and compensation.
The air in Kurashiki, Okayama had a high sulfur dioxide (SO2) concentration in the 1960s because of the high concentration of industrial areas. The number of officially-acknowledged victims of pollution-related illness in Kurashiki peaked at 3,838 in 1988, which was equivalent to 0.9% of the population of the city. An assessment in 2009 revealed that this number had fallen to 1,392. Of the 1,807 individuals (1,118 males, 689 females) who died from 1988 to 2009, the cause of death was available for 501. These 501 individuals were 326 males (65.1%) and 175 females (34.9%) with a mean age at death of 75.3 years (range 15–90 years); the mean age at death was 72.3 years in males and 76.3 years in females. The causes of death were respiratory disease (n = 216, 43.1%), malignant neoplasm (n = 151, 30.1%), circulatory disease (n = 77, 15.4%), and other (n = 57, 14.4%). The percentage of people aged ≥ 65 years in Japan increased to 23% in 2009, and a similar pattern of aging occurred in Kurashiki. Of the 1,392 victims of pollution-related illness who were still alive in 2009, 774 (55.6%) were aged ≥ 65 years. The mean age of officially-acknowledged victims of pollution-related illnesses in Kurashiki is increasing, and these individuals are now beginning to develop respiratory illnesses and complications due to aging. These combined health challenges are of major economic and social concern [11].
Many cross-sectional studies have examined the effects of air pollution on respiratory function based on the concentrations or types of pollutants. The Seattle Panel Study [12] reported that the concentration of particulate pollutants was associated with the magnitude of impairment in respiratory function in adults. Almost all studies to date have been cross-sectional, and few longitudinal studies have included measurements of respiratory function. In particular, there is a lack of studies reporting the respiratory symptoms and function of officially-acknowledged victims of pollution-related illness who have received compensation. Furthermore, the effects on respiratory function and symptoms of living in a city that initially had unacceptably high levels of pollution, and later had lower levels of pollution, have not been investigated.
The aim of this study was to conduct a longitudinal assessment of respiratory symptoms and function in older long-term officially-acknowledged victims of pollution-related illness in Japan.
Methods
Study design and setting
This study was embedded in a longitudinal study of officially-acknowledged victims of pollution-related illness in Kurashiki from 2000 to 2009. The study protocol was approved by the Ethical Committee of Nagasaki University Graduate School of Biomedical Sciences. The study subjects were drawn from the register of officially-acknowledged victims of pollution-related illness in Kurashiki. Registered victims all met the following conditions as determined by the Public Relief System of Kurashiki City, in accordance with the Pollution-Related Health Damage Special Measures Law (1969) and the Pollution-Related Health Damage Compensation Law (1973): (1) resided or spent time on activities in an area specified as having significant air pollution (Table 1), and (2) were diagnosed with chronic bronchitis, asthma, or emphysema by a doctor. Registered victims were entitled to various forms of compensation including monthly consultation with a doctor, prescriptions for expectorants and bronchodilators, yearly assessment of respiratory symptoms using a detailed questionnaire, and yearly spirometry, in accordance with the Public Nuisance Countermeasures Law. At the time that certification of pollution-related illness ceased in 1988, the population of Kurashiki was 419,203 (204,958 males, 214,245 females), of which 3,838 were officially-acknowledged victims of pollution-related illness (0.9% of the total population). In 2009, the records of these 3,838 victims were reviewed with the authorization of the Kurashiki City Public Office (Figure 1). At that time there were 1,392 registered survivors (634 males and 758 females). The 774 survivors (55.6%) who were aged ≥ 65 years in 2009 (284 males and 490 females) were screened for inclusion in the study. The majority of these victims were diagnosed with chronic bronchitis (n = 528, 68.2%), asthma (n = 242, 31.3%), or emphysema (n = 4, 0.5%) based on their symptom as described in interviews by authorized doctors. Chronic bronchitis was diagnosed if individuals complained of chronic copious sputum production or persistent coughing, asthma was diagnosed if they complained of recurrent episodes of dyspnea and wheezing, and emphysema was diagnosed if the symptoms did not match the criteria for either bronchitis or asthma. Complete spirometry data for the preceding 10 years were available for most victims. To avoid uneven data distribution and selection bias, 44 victims who did not have complete spirometry data for at least 7 of the years from 2000 to 2009 were excluded. A further 167 victims (116 males, 51 females) were excluded because they were former or current smokers. The remaining 563 victims aged ≥ 65 years were included in this study. These victims included 156 males and 407 females who had been certified for 25.9 ± 4.6 years (males: 26.0 ± 4.6 years, females: 25.9 ± 4.6 years). Approximately 60% of these individuals had first been registered as officially- acknowledged victims of pollution- related illness in the 1970s. Date describing spirometry findings and respiratory symptoms were retrospectively collected from the yearly reviews conducted from 2000 to 2009.

Flow chart showing selection of the study subjects. The study included officially-acknowledged victims of pollution-related illness in Kurashiki who were aged 65 years or older in 2009, and for whom the required data for statistical analysis were available.
Air pollution monitoring
The mean daily concentrations of air pollutants were obtained from instruments installed at 21 points in Kurashiki. Measurement of SO2 concentration was started in 1965, and measurement of nitrogen dioxide (NO2) concentration was started in 1971.
Spirometry measurements
Spirometry was performed by trained staff at Mizushima-Kyodo Hospital using an electronic spirometer (FUDAC 70, Fukuda Sangyo Inc., Chiba, Japan). Tests were performed in the sitting position, and were repeated until at least three reproducible forced expiratory curves had been obtained. Forced expiratory volume in 1 second (FEV1), forced vital capacity (FVC), and vital capacity (VC) were measured, and the FEV1/FVC (%) was calculated. Predicted FEV1 was calculated using the equation developed by Berglund et al. [13], predicted FVC was calculated using the equation recommended by the Special Committee of Pulmonary Physiology (Japan Respiratory Society, 1993), and predicted VC was calculated using the equation reported by Baldwin et al. [14].
Respiratory symptoms
Respiratory symptoms (dyspnea, wheeze, cough, and sputum production) were assessed by physicians during the same season each year, using the respiratory symptoms questionnaire provided by the government of Japan. Each symptom was graded using a standardized 5-point scale, as follows.
Dyspnea
-
1.
Too breathless to leave the house, or breathless when dressing or undressing.
-
2.
Breathless after walking about 50 m or after a few minutes on level ground.
-
3.
Breathless when walking on level ground and keeping up with people of the same age, but not breathless when walking at own pace.
-
4.
Breathless when walking up a slight hill or the stairs
-
5.
Breathless only during strenuous exercise.
Wheeze
-
1.
Severe episode ≥ 10 days each month during the last year.
-
2.
Severe episode ≥ 5 days each month during the last year, or mild episode ≥ 10 days each month during the last year.
-
3.
Severe episode ≥ 1 day each month during the last year, or mild episode ≥ 5 days each month during the last year.
-
4.
Mild episode ≥ 1 day each month during the last year.
-
5.
No episodes of wheezing.
Cough and sputum
-
1.
Daily cough and sputum, with a large amount of sputum or difficulty clearing sputum.
-
2.
Daily cough and sputum, with a moderate amount of sputum or difficulty clearing sputum.
-
3.
Daily cough and sputum, but not troublesome during daily life.
-
4.
Daily cough and sputum for ≤ 3 months each year.
-
5.
No cough or sputum.
Statistical analysis
The regression coefficients for annual mean changes in FEV1, FEV1% predicted, FVC, VC, VC % predicted, and FEV1/FVC (%) were calculated using simple linear regression analysis. The means and standard deviations were calculated for continuous variables, and a cross-tabulation was constructed for categorical variables. The Kolmogorov-Smirnov test was used to examine the distribution of data. Non-normally distributed data were analyzed using nonparametric tests. Data from the time of certification were compared between males and females using the Mann–Whitney U test and the Kruskal-Wallis test. Data were compared between 2000 and 2009 using the Wilcoxon signed-rank test. Mean annual changes in respiratory function were compared between subjects with and without worsening of dyspnea using the Mann–Whitney U test. All analyses were performed using the PASW software package, version 18. A 2-tailed value of p < 0.05 was considered statistically significant.
Results
Air pollutants
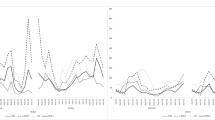
Figure 2 shows the annual mean daily levels of SO2 and NO2 recorded from 1965 to 2009 in Kurashiki. The Air Pollution Control Law was enacted in 1968. The SO2 levels were above the acceptable level for all years from 1968 to 1974, and then decreased to below 40 parts per billion (ppb), which is the acceptable level defined by the Air Pollution Control Law. In 1973, the acceptable NO2 level was changed by the Air Pollution Control Law from 20 ppb to 40 ppb. The NO2 level exceeded the acceptable level only in 1973.

Sulfur dioxide and nitrogen dioxide concentrations from 1965 to 2009 relative to standard values.
Patient characteristics at the time of certification
Table 2 shows the characteristics of subjects at the time of certification. Males were significantly younger than females (p < 0.05). Males had significantly higher FEV1, FVC, and VC than females (p < 0.001). Males had significantly lower FEV1 % predicted (p < 0.001), FVC % predicted (p < 0.01), VC % predicted (p < 0.01), and FEV1/FVC (%) (p < 0.05) than females, but these values were all within the normal range. Many subject reported respiratory symptoms: 96.7% of males and 97.8% of females reported dyspnea when walking on level ground and keeping up with people of the same age (grade 1–3 symptoms on the dyspnea scale), 93.5% of males and 96.3% of females reported at least one episode of severe wheezing each month (grade 1–3 symptoms on the wheeze scale), and 64.1% of males and 61.9% of females reported daily cough and sputum production that was troublesome during their daily life (grade 1–2 symptoms on the cough and sputum). These respiratory symptoms were not significantly different between the sexes.
Respiratory function over time
Table 3 shows spirometry findings in 2000 and 2009 by sex. All measurements of respiratory function declined significantly over time (p < 0.01), except for FEV1/FVC (%) in both sexes, FEV1 % predicted in males, and FVC % predicted in females.
Table 4 shows comparison of the mean annual changes in spirometry data between results in males and females from 2000 to 2009. Only the mean annual change in VC was significantly greater in males than in females (p < 0.05).
Respiratory symptoms over time
Table 5 shows respiratory symptoms in 2000 and 2009 by sex. There was a significant worsening of dyspnea over this time period (males: p < 0.05, females: p < 0.01). In females, there was also a significant worsening of wheeze over this time period (p < 0.01). There was no significant difference between 2000 and 2009 in cough and sputum production. We examined the relationships between worsening of dyspnea and mean annual changes in spirometry measurements (Table 6). In males, the mean annual changes in spirometry measurements were greater in those with worsening dyspnea than those without worsening dyspnea, but the differences were not significant. In females, however, the mean annual changes in all spirometry measurements except FEV1/FVC (%) were significantly greater in those with worsening dyspnea than those without worsening dyspnea (all p < 0.05). For the group overall, the mean annual changes in all spirometry measurements, including FEV1/FVC (%), were significantly greater in subjects with worsening dyspnea than those without worsening dyspnea (all p < 0.05, data not shown).
Discussion
This paper presents the first longitudinal study of respiratory function and symptoms in officially-acknowledged victims of pollution-related illness who were exposed to air pollution at least 40 years previously, and continued to receive various forms of compensation from the government. Spirometry data at the time of certification, revealed low FEV1, FEV1 % predicted, and FEV1/FVC (%). In addition, a high proportion of victims complained of respiratory symptoms. Many victims were diagnosed with chronic bronchitis or asthma. We consider that the respiratory disease in this group was caused mainly by the high environmental levels of SO2 and NO2 during 1965 to 1974, because approximately 60% of the victims were first registered during the 1970s. Our results are consistent with those of past reports indicating that high environmental levels of SO2 (40–60 ppb) and NO2 (17.4 ppb) can affect the bronchi and bronchioles, resulting in respiratory symptoms such as a cough, sputum, wheeze, and breathlessness [1–7, 15–17]. Our results show significant differences in respiratory function between males and females at the time of certification, with FEV1 % predicted, FVC % predicted, VC % predicted, and FEV1/FVC (%) significantly lower in males than in females. These differences are thought to result from the anatomical differences between the sexes. Many studies have shown that lung volumes are smaller in females than in age-matched males [18, 19]. Although, FEV1 % predicted, FVC % predicted, VC % predicted, and FEV1/FVC (%) were significantly lower in males than in females, respiratory symptoms were not significantly different between males and females. This differs from previous reports that females appear to be more significantly affected by air pollution than males [20–22]. It is unknown whether sex affects the defense mechanisms and responses to air pollution in this study. In the current study, most of the males were working or had worked in a factory, whereas about 40% of females were housewives during the 1960s and 1970s [23, 24]. The level of exposure therefore differed by sex, with males exposed to more air pollution than females, which would be expected to result in greater impairment of lung function in males [11]. However, we could not definitively determine the reasons for the differences between males and females observed in this study.
Our longitudinal analysis showed a significant decline in respiratory function from 2000 to 2009. The mean annual change in FEV1 in this study was −27.6 ml/year in male and −23.9 ml/year in females. The mean annual change in FEV1 reported for healthy, non-smoking males and females aged > 65 years is −31 to −22 ml/year [25–27]. The results of the current study were within this range. Furthermore, a previous study [28] reported that patients with chronic obstructive pulmonary disease had a mean annual change in FEV1 of 30–80 ml/year, which is 2 or 3 times the mean annual change in of healthy subjects, and higher than the mean annual change of the subjects in this study. The mean annual change in FVC in this study was −33.4 ml/year. The mean annual change in FVC reported for healthy, non-smoking males and females aged > 65 years is −38 to −11 ml/year [25–27, 29–31]. The mean annual change in VC in this study was −40.6 ml/year in males and −32.7 ml/year in females. The mean annual change in VC reported for healthy, non-smoking males and females aged > 65 years is −35 to –10 ml/year [25–27, 29, 31, 32]. The mean annual changes in FVC and VC in this study were therefore within the previously reported ranges for healthy, non-smoking males and females aged > 65 years. We considered that aging is the main cause of the decline in respiratory function observed from 2000 to 2009, with almost no additional effect cause by exposure to air pollutions. There are several possible reasons for the preservation of respiratory function in our study population. The level of air pollution in Kurashiki exceeded environmental standards until 1973, after which it declined as a result of the establishment of environmental standards and the introduction of antipollution laws. The NO2 level did not exceed the environmental standard from 2000 to 2009, and continued to decrease during this time. The SO2 level also did not exceed the environmental standard from 2000 to 2009. Downs et al. [33] reported that a reduction in air pollution may slow the annual rate of decline of respiratory function in adults. Another study showed that pollutant related delay in lung development in children can be attenuated if the children move to cleaner geographic areas [34]. In Switzerland, residence in more polluted areas has been associated with reduced respiratory function in adults [35]. We therefore consider that the study population may not have had a significant pollution- related decline in respiratory function from 2000 to 2009 because the concentrations of air pollutants continued to decrease. Another possible explanation is that medical treatment may have prevented deterioration of symptoms in officially-acknowledged victims of pollution-related illness. Reduced decline in respiratory function has been reported following treatment with bronchodilators such as inhaled corticosteroids, long-acting bronchial anticholinergic agents, and long-acting β2 agonists [30, 36–38]. It is possible that non-smoking individuals with pollution-related illness also sought medical treatment at other healthcare institutions, because continuous medical care is guaranteed by the national government. However, this study did not collect detailed data regarding treatment regimen, and we were therefore unable to evaluate the effects of treatment on respiratory function.
Dyspnea worsened significantly in both sexes during from 200 to 2009. The mean annual changes in respiratory function measurements were greater in subjects with worsening dyspnea than in those whose symptoms remained unchanged. However, the mean annual changes in respiratory function measurements in subjects with worsening dyspnea were within the range reported for healthy, non-smoking males and females aged > 65 years. We therefore think that these changes were due to aging. Previous studies [39, 40] reported that exacerbation of dyspnea is associated with age-related decline in respiratory function in normal elderly people. In this study, the mean annual changes in respiratory function measurements were greater in those with worsening dyspnea than those without worsening dyspnea in females but not in males. A previous study showed a stronger association between exposure to air pollution and decline in respiratory function in young females than young males [20]. Several studies have also shown that females are more likely to notice a worsening of respiratory function than males [41–44]. This may be because males have a greater tolerance to change in respiratory function [44] In addition, dyspnea which is the subjective perception of respiratory discomfort, is a result of complex and multifocal mechanisms [45]. These include abnormalities in the respiratory control system, neurochemical receptors, ventilation, respiratory muscles, gas exchange, and so on [45]. Therefore, we were not able to determine the reasons for the different relationships between worsening dyspnea and mean annual changes in spirometry findings males and females in this study. Appropriate medical treatment may have prevented the worsening of wheezing (in males) and cough and sputum (in both sexes), but the effects of medical treatment on these symptoms could not be determined in the current study.
In our population of officially-acknowledged victims of pollution-related illness who were living in an area where the level of air pollutants did not exceed the environmental standards and were receiving compensation set by the Air Pollution Control Law and the revised Public Nuisance Countermeasures Law of Japan, treatment measures were considered to be effective, and decreases in respiratory function over time were mild. However, dyspnea worsened significantly in both sexes from 2000 to 2009, and further intervention for dyspnea is required.
This study has some limitations. First, we evaluated only non-smoking officially-acknowledged victims of pollution-related illness, and did not include a control group of subjects who lived in the same area. Second, our study population included more females than males. This may be partly explained by a higher death rate in males, as 65% of the deceased individuals for whom records were available were male. The population of Kurashiki also had a higher proportion of females than males, and more males than females were excluded because they were smokers. Third, spirometry testing was conducted during various seasons. Fourth, differences in social background, employment and lifestyle, which could have resulted in differences in exposure to environmental pollutants, and differences in treatment were not taken into account.
Conclusion
The results of this study suggest that the high concentrations of air pollutants during the 1970s affected respiratory function. However, the mean annual changes in respiratory function in officially-acknowledged victims of pollution-related illness were within the range of healthy, non-smoking males and females aged > 65 years, even though the severity of dyspnea worsened over time. These results suggest that the changes were limited to the effects of aging. The reduction air pollution levels and the laws regarding pollution-related compensation and treatment in Japan may therefore be effective for reducing respiratory disease cause by pollution.
Abbreviations
- FEV1:
-
Forced expiratory volume in 1 second
- FVC:
-
Forced vital capacity
- NO2:
-
Nitrogen dioxide
- SO2:
-
Sulfur dioxide
- VC:
-
Vital capacity.
References
Groneberg-Kloft B, Kraus T, Mark A, Wagner U, Fischer A: Analysing the causes of chronic cough: relation to diesel exhaust, ozone, nitrogen oxides, sulphur oxides and other environmental factors. J Occup Med Toxicol. 2006, 1: 6-10.1186/1745-6673-1-6.
Forbes LJ, Kapetanakis V, Rudnicka AR, Cook DG, Bush T, Stedman JR, Whincup PH, Strachan DP, Anderson HR: Chronic exposure to outdoor air pollution and lung function in adults. Thorax. 2009, 64 (8): 657-663. 10.1136/thx.2008.109389.
Gotschi T, Sunyer J, Chinn S, de Marco R, Forsberg B, Gauderman JW, Garcia-Esteban R, Heinrich J, Jacquemin B, Jarvis D, et al: Air pollution and lung function in the European Community Respiratory Health Survey. Int J Epidemiol. 2008, 37 (6): 1349-1358. 10.1093/ije/dyn136.
Goldberg MS, Burnett RT, Stieb D: A review of time-series studies used to evaluate the short-term effects of air pollution on human health. Rev Environ Health. 2003, 18 (4): 269-303.
Brauer M, Ebelt ST, Fisher TV, Brumm J, Petkau AJ, Vedal S: Exposure of chronic obstructive pulmonary disease patients to particles: respiratory and cardiovascular health effects. J Expo Anal Environ Epidemiol. 2001, 11 (6): 490-500. 10.1038/sj.jea.7500195.
Penttinen P, Timonen KL, Tiittanen P, Mirme A, Ruuskanen J, Pekkanen J: Number concentration and size of particles in urban air: effects on spirometric lung function in adult asthmatic subjects. Environ Health Perspect. 2001, 109 (4): 319-323. 10.1289/ehp.01109319.
Detels R, Tashkin DP, Sayre JW, Rokaw SN, Massey FJ, Coulson AH, Wegman DH: The UCLA population studies of CORD: X. A cohort study of changes in respiratory function associated with chronic exposure to SOx, NOx, and hydrocarbons. Am J Public Health. 1991, 81 (3): 350-359. 10.2105/AJPH.81.3.350.
Dockery DW, Pope CA, Xu X, Spengler JD, Ware JH, Fay ME, Ferris BG, Speizer FE: An association between air pollution and mortality in six U.S. cities. N Engl J Med. 1993, 329 (24): 1753-1759. 10.1056/NEJM199312093292401.
Abbey DE, Nishino N, McDonnell WF, Burchette RJ, Knutsen SF, Lawrence Beeson W, Yang JX: Long-term inhalable particles and other air pollutants related to mortality in nonsmokers. Am J Respir Crit Care Med. 1999, 159 (2): 373-382. 10.1164/ajrccm.159.2.9806020.
Nafstad P, Haheim LL, Wisloff T, Gram F, Oftedal B, Holme I, Hjermann I, Leren P: Urban air pollution and mortality in a cohort of Norwegian men. Environ Health Perspect. 2004, 112 (5): 610-615. 10.1289/ehp.6684.
Asano S, Matsuoka K, Fukuda H, Satomi K, Michibata T, Hatano T: A summary of the analysis of the deseased victims of air pollution. Reseach on the deceased victims of air pollution. 2005, 17-27.
Trenga CA, Sullivan JH, Schildcrout JS, Shepherd KP, Shapiro GG, Liu LJ, Kaufman JD, Koenig JQ: Effect of particulate air pollution on lung function in adult and pediatric subjects in a Seattle panel study. Chest. 2006, 129 (6): 1614-1622. 10.1378/chest.129.6.1614.
Berglund E, Birath G, Bjure J, Grimby G, Kjellmer I, Sandqvist L, Soderholm B: Spirometric studies in normal subjects. I. Forced expirograms in subjects between 7 and 70 years of age. Acta Med Scand. 1963, 173: 185-192.
Baldwin ED, Cournand A, Richards DW: Pulmonary insufficiency; physiological classification, clinical methods of analysis, standard values in normal subjects. Medicine (Baltimore). 1948, 27 (3): 243-278.
Osterman JW, Greaves IA, Smith TJ, Hammond SK, Robins JM, Theriault G: Respiratory symptoms associated with low level sulphur dioxide exposure in silicon carbide production workers. Br J Ind Med. 1989, 46 (9): 629-635.
van Strien RT, Gent JF, Belanger K, Triche E, Bracken MB, Leaderer BP: Exposure to NO2 and nitrous acid and respiratory symptoms in the first year of life. Epidemiology. 2004, 15 (4): 471-478. 10.1097/01.ede.0000129511.61698.d8.
Johns DO, Svendsgaard D, Linn WS: Analysis of the concentration-respiratory response among asthmatics following controlled short-term exposures to sulfur dioxide. Inhalation toxicology. 2010, 22 (14): 1184-1193. 10.3109/08958378.2010.535220.
McClaran SR, Harms CA, Pegelow DF, Dempsey JA: Smaller lungs in women affect exercise hyperpnea. J Appl Physiol. 1998, 84 (6): 1872-1881.
Harms CA: Does gender affect pulmonary function and exercise capacity?. Respir Physiol Neurobiol. 2006, 151 (2–3): 124-131.
Brunekreef B, Janssen NA, de Hartog J, Harssema H, Knape M, van Vliet P: Air pollution from truck traffic and lung function in children living near motorways. Epidemiology. 1997, 8 (3): 298-303. 10.1097/00001648-199705000-00012.
Dockery DW, Berkey CS, Ware JH, Speizer FE, Ferris BG: Distribution of forced vital capacity and forced expiratory volume in one second in children 6 to 11 years of age. Am Rev Respir Dis. 1983, 128 (3): 405-412.
Peters JM, Avol E, Gauderman WJ, Linn WS, Navidi W, London SJ, Margolis H, Rappaport E, Vora H, Gong H, et al: A study of twelve Southern California communities with differing levels and types of air pollution. II. Effects on pulmonary function. Am J Respir Crit Care Med. 1999, 159 (3): 768-775. 10.1164/ajrccm.159.3.9804144.
Japan. Keizai Kikakucho: Annual reports on national life. 1978, Tokyo: Economic Planning Agency, Japanese Government
Japan. Keizai Kikakuch: White paper on the national lifestyle (summary). 1995, Tokyo: Printing Bureau, Ministry of Finance
Yokoyama T, Mitsulfuji M: Statistical representation of the ventilatory capacity of 2,247 healthy Japanese adults. Chest. 1972, 61 (7): 655-661. 10.1378/chest.61.7.655.
Japan Respiratory Society, committee of Pulmonary Physiology: Japanese clinical pulmonary function test standard value: The healthy person pulmonary function test in 14 area (in Japanese). Nihon Kyobu Shikkan Gakkai Zasshi. 1993
Nakadate T: [Age-related decline in forced expiratory volume in one second and forced vital capacity based on a longitudinal observation of Japanese males]. Nihon Kyobu Shikkan Gakkai Zasshi. 1997, 35 (9): 954-959.
Fletcher C, Peto R: The natural history of chronic airflow obstruction. Br Med J. 1977, 1 (6077): 1645-1648. 10.1136/bmj.1.6077.1645.
Nakadate T, Sato T, Kagawa J: Longitudinal changes in time domain spirogram indices and their variability. Eur Respir J. 1994, 7 (6): 1062-1069.
Yamagata T, Hirano T, Sugiura H, Yanagisawa S, Ichikawa T, Ueshima K, Akamatsu K, Nakanishi M, Matsunaga K, Minakata Y, et al: Comparison of bronchodilatory properties of transdermal and inhaled long-acting beta 2-agonists. Pulm Pharmacol Ther. 2008, 21 (1): 160-165. 10.1016/j.pupt.2007.05.004.
Japan Respiratory Society JR: The predicted values of pulmonary function testing in Japananese. Jpn J Thorac Dis. 1993, 31 (3): Appendex
Feraudi M, Harm K, Schmidt H: [Statistical analysis on the question of normal values and physiological variability of serum creatine phosphokinase]. Enzymol Biol Clin (Basel). 1968, 9 (5): 338-354.
Downs SH, Schindler C, Liu LJ, Keidel D, Bayer-Oglesby L, Brutsche MH, Gerbase MW, Keller R, Kunzli N, Leuenberger P, et al: Reduced exposure to PM10 and attenuated age-related decline in lung function. N Engl J Med. 2007, 357 (23): 2338-2347. 10.1056/NEJMoa073625.
Avol EL, Gauderman WJ, Tan SM, London SJ, Peters JM: Respiratory effects of relocating to areas of differing air pollution levels. Am J Respir Crit Care Med. 2001, 164 (11): 2067-2072. 10.1164/ajrccm.164.11.2102005.
Ackermann-Liebrich U, Leuenberger P, Schwartz J, Schindler C, Monn C, Bolognini G, Bongard JP, Brandli O, Domenighetti G, Elsasser S, et al: Lung function and long term exposure to air pollutants in Switzerland. Study on Air Pollution and Lung Diseases in Adults (SAPALDIA) Team. Am J Respir Crit Care Med. 1997, 155 (1): 122-129. 10.1164/ajrccm.155.1.9001300.
Celli BR, Thomas NE, Anderson JA, Ferguson GT, Jenkins CR, Jones PW, Vestbo J, Knobil K, Yates JC, Calverley PM: Effect of pharmacotherapy on rate of decline of lung function in chronic obstructive pulmonary disease: results from the TORCH study. Am J Respir Crit Care Med. 2008, 178 (4): 332-338. 10.1164/rccm.200712-1869OC.
Mahler DA, Wire P, Horstman D, Chang CN, Yates J, Fischer T, Shah T: Effectiveness of fluticasone propionate and salmeterol combination delivered via the Diskus device in the treatment of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2002, 166 (8): 1084-1091. 10.1164/rccm.2112055.
Donohue JF, van Noord JA, Bateman ED, Langley SJ, Lee A, Witek TJ, Kesten S, Towse L: A 6-month, placebo-controlled study comparing lung function and health status changes in COPD patients treated with tiotropium or salmeterol. Chest. 2002, 122 (1): 47-55. 10.1378/chest.122.1.47.
Yamada K, Kida K, Takasaki Y, Kudoh S: [A clinical study of the usefulness of assessing dyspnea in healthy elderly subjects]. J Nihon Med Sch. 2001, 68 (3): 246-252. 10.1272/jnms.68.246.
Berglund DJ, Abbey DE, Lebowitz MD, Knutsen SF, McDonnell WF: Respiratory symptoms and pulmonary function in an elderly nonsmoking population. Chest. 1999, 115 (1): 49-59. 10.1378/chest.115.1.49.
Chhabra SK, Chhabra P: Gender differences in perception of dyspnea, assessment of control, and quality of life in asthma. J Asthma. 2011, 48 (6): 609-615. 10.3109/02770903.2011.587577.
Singh AK, Cydulka RK, Stahmer SA, Woodruff PG, Camargo CA: Sex differences among adults presenting to the emergency department with acute asthma. Multicenter Asthma Research Collaboration Investigators. Arch Intern Med. 1999, 159 (11): 1237-1243. 10.1001/archinte.159.11.1237.
Wijnhoven HA, Kriegsman DM, Snoek FJ, Hesselink AE, de Haan M: Gender differences in health-related quality of life among asthma patients. J Asthma. 2003, 40 (2): 189-199. 10.1081/JAS-120017990.
Cydulka RK, Emerman CL, Rowe BH, Clark S, Woodruff PG, Singh AK, Camargo CA: Differences between men and women in reporting of symptoms during an asthma exacerbation. Ann Emerg Med. 2001, 38 (2): 123-128. 10.1067/mem.2001.114305.
Dyspnea: Mechanisms, assessment, and management: a consensus statement. American Thoracic Society. Am J Respir Crit Care Med. 1999, 159 (1): 321-340.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2458/13/766/prepub
Acknowledgments
We thank the study participants, technical staff, administrative support team, and our coworkers for their help. In addition, we are grateful to Sue Jenkins, PhD, Associate Professor at the School of Physiotherapy, Curtin University for help in reviewing this manuscript. This study was supported by the Environmental Restoration and Conservation Agency and Mizushima-Kyodo Hospital.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
HS was the principal investigator, contributed to the design of the study, handled funding and supervision, and made critical revisions to the manuscript for important intellectual content. TT designed the study, collected the data, analyzed and interpreted the data, and prepared the manuscript. SH interpreted the data, analyzed the data, handled supervision, and made critical revisions to the manuscript for important intellectual content. RK made critical revisions to the manuscript for important intellectual content. MA collected d and interpreted the data, drafted the manuscript and made critical revisions to the manuscript for important intellectual content. YY, TN, NM, KK, and YY collected, analyzed, and interpreted the data. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Tanaka, T., Asai, M., Yanagita, Y. et al. Longitudinal study of respiratory function and symptoms in a non-smoking group of long-term officially-acknowledged victims of pollution-related illness. BMC Public Health 13, 766 (2013). https://doi.org/10.1186/1471-2458-13-766
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2458-13-766