
Abstract
Background
Asperger syndrome (AS) is a neurodevelopmental disorder belonging to autism spectrum disorders with prevalence rate of 0,35% in school-age children. It has been most extensively studied in childhood while there is scarcity of reports concerning adulthood of AS subjects despite the lifelong nature of this syndrome. In children with Asperger syndrome the initiation and continuity of sleep is disturbed because of the neuropsychiatric deficits inherent of AS. It is probable that sleep difficulties are present in adulthood as well. Our hypothesis was that adults with AS suffer from difficulty in initiating and maintaining sleep and nonrestorative sleep (insomnia).
Methods
20 AS without medication were compared with 10 healthy controls devoid of neuropsychiatric anamnesis. Clinical examination, blood test battery and head MRI excluded confounding somatic illnesses. Structured psychiatric interview for axis-I and axis-II disorders were given to both groups as well as Beck Depression Inventory and Wechsler adult intelligence scale, revised version.
Sleep quality was assessed with sleep questionnaire, sleep diary during 6 consecutive days and description of possible sleep problems by the participants own words was requested.
Results
compared with controls and with normative values of good sleep, AS adults had frequent insomnia. In sleep questionnaire 90% (18/20), in sleep diary 75% (15/20) and in free description 85% (17/20) displayed insomnia. There was a substantial psychiatric comorbidity with only 4 AS subject devoid of other axis-I or axis-II disorders besides AS. Also these persons displayed insomnia. It can be noted that the distribution of psychiatric diagnoses in AS subjects was virtually similar to that found among patient with chronic insomnia.
Conclusions
the neuropsychiatric deficits inherent of AS predispose both to insomnia and to anxiety and mood disorders. Therefore a careful assessment of sleep quality should be an integral part of the treatment plan in these individuals. Conversely, when assessing adults with chronic insomnia the possibility of autism spectrum disorders as one of the potential causes of this condition should be kept in mind.
Similar content being viewed by others

Background
Asperger syndrome (AS) is a pervasive developmental disorder characterized by altered social interactions, restricted interests and repetitive and stereotyped behaviour as in autism but, contrary to the latter, should not show any significant delay in acquisition of language, psychomotor and cognitive skills [1]. According to epidemiological surveys AS is not uncommon, the prevalence being 0,35% in school-age children [2]. The prevalence of AS in adulthood is unknown but as AS is a continuous and lifelong disorder [1] it is reasonable to assume that it is not significantly lower than in childhood. Most studies on AS concentrate on childhood while there is scarcity of reports about the clinical and neurobiological characteristics of these individuals in adulthood.
Autism, AS and pervasive developmental disorder not otherwise specified (PDD-NOS) are commonly referred as "autistic spectrum disorders" [3]. In children with autism spectrum disorders the initiation and continuity of sleep are disturbed to a greater degree than in children with other developmental disorders [4]. More specifically, AS children reported in a sleep questionnaire study more dyssomnias, particularly difficulty in initiating and maintaining sleep, than age-matched controls [5].
DSM-IV defines insomnia as difficulty in initiating or maintaining sleep, or nonrestorative sleep, lasting at least one month and causing significant dysfunction during daytime [1]. It is further divided into primary and secondary type, depending on whether it is caused by mental disorder, substance abuse, other sleep disorder, a general medical condition.
AS is known to persist into adulthood [1, 6], and it is probable that disorganization of sleep persists as well. Insomnia gives rise to emotional distress, daytime fatigue and loss of productivity [7] and should therefore be taken in consideration when planning rehabilitation of these individuals. As pointed out by Godbout et al 1998 [8], clinical observations suggest that AS subjects may present the same difficulties in initiation and maintaining of sleep as previously described in autism. We are not aware of studies concerning systematic assessment of insomnia in adults with AS.
Comorbid psychiatric disorders occur frequently in adults with AS [9, 10]. They might cause changes in sleep profile and also by themselves lower sleep quality. There is no knowledge of impact of comorbid mood or anxiety disorder on sleep in AS patients.
Our hypothesis was that AS adults display a high grade of insomnia. Our aim was also to study psychiatric comorbidity and its impact on sleep quality in AS adults. The quality of sleep was evaluated using sleep questionnaire, sleep diary and a detailed description of possible sleep problems by participants.
Methods
Diagnosis of Asperger syndrome
AS subjects (n = 20) were, after informed consent, recruited from the Helsinki Asperger Center, a unit to which patients with a tentative diagnosis of AS are referred from all parts of Finland. Prior to inclusion in the present study participants had the following assessment:
The participant himself/herself had a detailed interview by a clinician familiar with autism spectrum disorders focussing on life-history elements essential for the diagnosis of AS. The mother or other significant relative or family member(s) was interviewed on developmental issues relevant for the diagnosis. All available previous medical records were reviewed including data from well baby clinics and school health especially concerning developmental milestones.
Autism spectrum screening questionnaire (ASSQ) is a continuous measure rating scale validated for screening children with tentative autism spectrum disorder [11]. The questionnaire consists of 27 items about patient's behaviour, each scored from 0 to 2 points (score range 0–54). In children a parent rating cut-off of 19 points identifies correctly 82% of AS-patients [11]. In the present study the mothers or other persons in close contact with the subject in childhood filled in ASSQ concerning the subject's childhood behaviour. Each positive score had to be documented with several examples. In one AS subject there was no competent relative to be interviewed and he filled in the ASSQ by himself.
Wechsler Adult Intelligence scale, revised version (WAIS-R) [12] was assessed in all participants by a psychologist familiar with autism spectrum disorders except in one control and in one patient (both having university degree) who refused.
All these data were critically reviewed in corpore by three authors (PT, TN and LvW). All 20 participants fulfilled the ICD-10 and DSM IV-criteria in childhood. Two persons did not meet the full criteria of AS in adulthood but as their problems were essentially similar to those of other subjects they were included in the study group. Exclusion criteria of DSM-IV were followed. Control group (n = 10) consisted of healthy volunteers assessed with same method as the AS group, with no history of neuropsychiatric disorders according to themselves and to anamnesis obtained from parents.
Participants were medication free (with a minimum interval of two weeks for hypnotics, three months for antidepressant medicines and one year for neuroleptics) except of one 44 years old female who had been using thyroxin substitution since childhood.
Associated conditions
Structured Clinical Interview of Diseases (SCID) for DSM III-R [13] was performed for comorbid axis I diagnoses. Because AS-patients are prone to affective disorders [9, 10] their mood was further explored with the Beck Depression Inventory (BDI) [14] in order to quantitate current depressive symptoms potentially affecting sleep quality. Schizophrenia and other chronic psychotic illness in previous medical records or in SCID-interview were used as exclusion criteria. None of the participants had a diagnosis of alcohol misuse or dependency. The controls had no current axis-I diagnoses assessed with SCID-I.
7 AS subjects were devoid of other axis-I diagnoses besides AS. 13 As subjects met the diagnostic criteria of one or more anxiety disorders, the most prevalent being social phobia (n = 8). 5 AS subjects had mild to moderate depressive disorder and none of them had severe MDD.
Also the Structured Clinical Interview of Axis-II disorders for DSM-III-R (SCID-II) [15] was performed to all participants. 5 AS subjects had Cluster A (paranoid, schizoid, schizotypal) personality disorder, and 3 subjects had cluster B (antisocial, borderline, histrionic, narcissistic) disorder. 13 subjects presented Cluster C (avoidant, dependent, obsessive-compulsive, passive-aggressive) personality disorder. 5 subjects had both cluster A and cluster C personality disorder. Obsessive-compulsive personality disorder (12 subjects) or traits of it (7 subjects) were the most common axis-II disorders. Conversely, 6 subjects did not meet the full diagnostic criteria of any axis-II disorders. 4 out of 7 subjects with no axis-I disorder did not have axis II-disorder according to the diagnostic threshold of axis-II although all subjects displayed single or multiple symptoms of some personality disorders. Control subjects did not have axis-II disorders.
Possible confounding comorbid somatic disease was ruled out by means of clinical examination and by a blood test screening for electrolytes, liver and kidney functions, thyroid hormones, calcium metabolism and head MRI (1.5T), the latter in 17 AS subjects and in 9 controls, which all gave normal results.
In many previous studies on autism spectrum disorders the normality of the control group has been inadequately assessed [16]. In the present study all controls were examined using exactly the same procedures as in the AS group.
Sleep questionnaire
Basic Nordic Sleep Questionnaire (BNSQ) is a quantitative scale for assessment of sleep quality developed by the Scandinavian Sleep Research Society [17] and is widely used in sleep studies published in Nordic countries. It consists of 14 statements assessing the frequency of sleep problems during the past three months with five-point scale. Score range is 14–70; the higher score indicating lower sleep quality. Questions concerning some time values of sleep (e.g. sleep latency) are also included. The items describing frequency and severity of insomnia are reported below. After filling in the BNSQ participants proceeded to follow-up period with sleep diary.
Sleep diary
During the mean period of 6 days (range 5–7 days) participants wrote down the time of retiring to bed in order to sleep, estimated time of falling asleep and awakening in the morning and sleep naps in daytime as well as number and duration of awakenings during night time. Sleep latency was calculated by subtracting the time of falling asleep from time of retiring to bed. Time in bed (TIB) was defined as the time period from retiring to bed in the evening to awakening in the morning, and sleep period as the time from falling asleep to awakening in the morning. Sleep efficiency was defined as a ratio between true sleep (time in bed-sleep latency-duration of awakenings) and time in bed. Subjective quality of each night, sleep was assessed with an arbitrary scale from 4–10 (school grades in Finland) higher numbers indicating better sleep quality. These parameters were calculated for each consecutive night in each participant and then averaged for each subject to enable statistical comparison between individuals. Standard deviation (SD) of each parameter reflects the night-to-night variability and thus the individual SD was pooled up in AS subjects and in controls for comparison. Caffeine, nicotine and alcohol consumption during the study period was registered for each recording day. Participants were advised to lead their normal life at home, work or studies during the study period.
One AS subjects was not able to assess the time of falling asleep and two AS subjects could not assess the quality of sleep in consecutive nights. In one control subject the sleep diary data was entirely lacking.
Sleep naps in daytime were a rare event during the study period; In the AS group four subjects reported one sleep nap each and one subject two sleep naps during the study period. Three of the controls reported one sleep nap each.
During the study period 3 AS subjects and 1 control smoked 5 cigarettes or more per day. 3 AS subjects and 1 control had one or two nights with alcohol use more than 24 g per evening. 2 AS subjects (and none of the controls) had both daily smoking and occasional alcohol use. 1 AS subject and 1 control reported excessive use of coffee (more than three cups per day).
Free description
After filling in the BNSQ and during study period all participants were requested to give a detailed description of possible subjective sleep problems as a short essay.
Definition of insomnia
In BNSQ insomnia was defined as follows: difficulty in falling asleep (initial insomnia) as difficulties in falling asleep on 3–5 days per week or more often and/or sleep latency 30 minutes or more (item 1, grade 4–5, item 2a–2b sleep latency ≥ 30 min), difficulty in staying asleep (middle insomnia) as at least 3 awakenings per night (item 4, grade 4–5) and nonrestorative sleep (terminal insomnia) as excessive sleepiness in the morning after awakening or during daytime on 3–5 days per week or more often (item 8 and 9, grade 4–5).
In sleep diary sleep latency and/or wake after sleep onset ≥ 30 minutes or sleep efficiency below 85% defined insomnia. Both the BNSQ and sleep diary criteria were modified according to previously published operational criteria [18].
In free description participants were encouraged to describe the symptoms of poor sleep, which they found to be most disturbing.
Statistics
In BNSQ the items scored with five-point scale display a rank order quality. Therefore the comparison between AS subjects and controls was performed with Mann-Whitney rank sum test. Variability of items was described with range of 25%-75% percentiles. Time values in BNSQ are continuous measures. Therefore the comparison between AS subjects and controls was performed with Student's t-test except in cases where the items studied had a non-normal distribution. In these cases the Mann-Whitney rank sum test was applied.
In the averaged sleep diary items (with continuous measures) the comparison between AS subjects and controls was performed either with Student's t-test or with Mann-Whitney rank sum test depending on whether the parameter studied displayed a normal or non-normal distribution. Fisher exact test was used when comparing the number of subjects with or without insomnia studied with different methods.
Statistical analyses were calculated with commercial computer software (Sigma Stat 2.03, SPSS Inc. 1995).
Ethics
The local ethical committee approved the study and principles of declaration of Helsinki were adequately followed.
Results
General
As indicated in Table 1, AS subjects did not differ from controls in regard of age, education, intelligence and body mass index (BMI). In ASSQ AS subjects displayed significantly higher scores compared with controls in accordance to anamnesis of Asperger syndrome in childhood. BDI-score was also significantly higher in AS subjects although only two subjects reached the threshold of moderate depression, as described in previous section.
Sleep questionnaire (BNSQ)
The selected BNSQ items (see Additional file: 1) of AS subjects and controls are given in Table 2 and Table 3, respectively. 18 out of 20 AS subjects had insomnia, including those 4 subjects with no axis-I or axis-II psychiatric comorbidity. Initial insomnia was expressed by 11 AS subjects, middle insomnia by 2 AS subjects and terminal insomnia by 14 AS subjects. 7 AS subjects had both initial and terminal insomnia. 5 AS subjects rated low sleep quality (item 6, grade 4–5)
With same criteria 3 controls displayed insomnia with no daytime consequences and no experience of poor sleep quality.
As indicated in Table 4, AS subjects had, compared with controls, higher total score, more frequent difficulties in falling asleep (item 1), longer sleep latency in working days (item 2a) and tendency to prolonged sleep latency also during freetime (item 2b). Also more frequent sleepiness in the morning after awakening (item 8) and during daytime (item 9) was found. The general sense of sleep quality was worse (item 6). For statistics, see Table 4.
Sleep diary
In Table 6 the sleep diary items of AS subjects concerning poor sleep quality are given.13 AS subjects had prolonged sleep latency, 6 had prolonged wake after sleep onset and 9 had low sleep efficiency. In controls (Table 7) the corresponding figures were 3, zero and 1 subject. Altogether 15 AS subjects and 3 controls were poor sleepers. Of the 4 AS subjects with no comorbid axis-I or axis-II disorders, 3 displayed poor sleep and one was not able to assess the estimated time of falling asleep or sleep quality.
In Table 8 the results of comparison between averaged sleep diary parameters between AS subjects and controls are given. AS subjects had low sleep quality, tendency to prolonged wake after sleep onset and significantly lower sleep efficiency as compared with controls. All the parameters studied displayed a tendency to increased night-to-night variability reaching statistical significance in case of time of awakening in the morning and sleep efficiency.
Free description
In description of possible sleep problems 17 AS subjects, and none of the controls, described a variable degree of chronic problems in initiation and continuity of sleep.
Discussion
The main finding of the present study, obtained by using three different methods, is that adults with Asperger syndrome display frequent complaints of impaired initiation and continuity of sleep. According to sleep diaries, AS subjects showed a tendency to a greater night-to-night variability of sleep parameters, a feature typical of insomnia [19]. Also AS subjects without psychiatric axis-I or axis-II comorbidity had insomnia.
There are several possible explanations for these findings. First, comorbid axis-I disorders, anxiety disorders in particular, seem to be associated with insomnia. According to sleep questionnaire studies, patients with social phobia display poor sleep quality, long sleep latency and frequent sleep disturbances [20]. In the present study 8 AS subjects had social phobia, and altogether 13 subjects reached the threshold for clinical anxiety disorder.
Secondly, 14 AS subjects had personality disorder, especially in cluster C. In a study where 100 patients with chronic insomnia where assessed with structured psychiatric interview, SCID-III, 95% of subjects had multiple psychiatric diagnoses, the most prevalent being anxiety disorders and dysthymia as well as substance use disorders on axis-I, and obsessive compulsive personality disorder or traits of it on axis-II [21]. Insomnia was ascribed to internalisation of emotions leading to heightened arousal. Results in the present, smaller sample are virtually identical to those except that diagnosis of alcohol abuse was absent. In longitudinal analysis insomnia includes a risk for development of new psychiatric illness [22].
An additional mechanism in AS adults may also play a role in generation of insomnia. As pointed out by Söderström et al [23] " the theoretical boundaries between uneven and deficient neuropsychiatric functioning and maladaptive personality traits are not sharply defined", it is unclear, whether AS originating in childhood predisposes to, or even causes the symptoms of personality disorder in adulthood. In Temperament and Character Inventory (TCI) AS adults score high on harm avoidance and low on self-directedness and novelty seeking [23] resulting in anxiety prone, socially detached character with reluctance to accept changes. Moreover, similarity of obsessive-compulsive personality disorder to AS has been previously noted by Gillberg et al [9]. Further studies will clarify this issue, but when assessing adults with chronic insomnia the possibility of autism spectrum disorders should be kept in mind.
The same applies to clinical anxiety disorders as well. Clinicians with substantial experience in AS have noticed that anticipatory anxiety is a nearly universal feature of AS [6, 9] as a result of the developmental deficit in intersubjectivity and excessive adherence to routines inherent in AS. Both the temperament and character of AS adults predispose to anxiety [23], which might be difficult to classify in terms of present clinical anxiety disorders. Most AS subjects in the present study had one or more anxiety disorders but also the remaining ones displayed subthreshold anxiety symptoms. This is in accordance with the observation that those few AS subjects without axis-I and axis-II comorbidity also had symptoms of insomnia.
The impact of AS symptom severity on sleep is difficult to evaluate. In children with autism even a minor disruption of stereotypic rituals before going to bed may prevent them from falling asleep [4]. Our patients did not describe this type of behaviour (which is often less conspicuous in AS as compared to autism) but complained more of hypersensitivity to external noise, forgetting oneself in front of computer, ruminating things passed in previous days, or, most often, diffuse difficulty in falling asleep.
Previously published studies in this field rely mostly on categorical classifications like DSM-IV and ICD-10 criteria. ASSQ score in the present study reflects the mothers' perception and recall of patients' symptoms in childhood. Some AS subjects had very low ASSQ-scores in spite of clear anamnesis and status of AS. If spouses or colleagues had been interviewed instead of mothers the results might had been different in accordance to the notion [11] that in children teachers report more autistic symptoms than parents. To our knowledge there is presently no validated instrument available for assessing the severity of adult AS.
Only few subjects in AS group and in controls used alcohol, nicotine and caffeine, and excessive use of these substances seemed to cluster in 2–3 AS subjects.
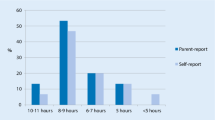
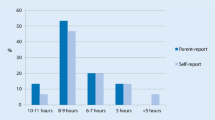
Paavonen et al [5] compared 50 AS children with 43 age-matched controls with two sleep questionnaires, one filled in by parents and the other by participants themselves. The most significant difference between AS children and controls was in increased prevalence of disorders in initiating and maintaining sleep. The same result was obtained in the present study with considerably smaller material suggesting that sleep difficulties inherent of AS are preserved, together with other symptoms, in adulthood.
The term insomnia refers essentially to subjective experience of low sleep quality [7], which might have multiple causes beyond and besides psychiatric morbidity. For example, the decreased continuity of sleep in AS subjects together with frequent daytime sleepiness might be caused by specific sleep disorders. We have previously reported that AS adults have increased movements in legs during controlled rest in daytime, measured with three channel actometry [24] and therefore the possibility of RLS/PLMS should be explored as a possible cause of decreased continuity of sleep. In a polysomnographic study of sleep AS subjects (with the mean age of 22.5 years) showed decreased sleep time in the first two-thirds of the night, signs of REM sleep disruption and three of them had periodic leg movements in sleep [25]. All these features predispose to low sleep quality and to the subjective complaint of insomnia. They also give support to the possibility of defective sleep control system in AS [25] that might play a role in symptoms of low sleep quality in these subjects.
The AS subjects of the present study were patients from a tertiary clinic that is specialized for assessment of AS. The subjects using sedatives or other psychoactive medicines were excluded from the study, presumably excluding those subjects that had severe sleep problems. Even in this population, with relatively mild AS symptoms, almost all had subjective sleep complains. Although the generalizability of our results to all adults with AS remains open it is obvious that a substantial proportion of AS adults display similar type of sleep difficulties than previously described in children with autism spectrum disorders.
The clinical relevance of our results is emphasised by the notion that the human prefrontal cortex functions are particularly prone to the deficits induced by sleep deprivation [26, 27]. In subjects like AS, who already have compromised function of the prefrontal cortex [28], the poor sleep quality-induced sleep deprivation may impair daytime functioning more severely than in the general population.
Conclusions
Adults with AS display a high grade of insomnia. Sleep patterns of AS adults have similarity to those described in AS children but to date it is unclear whether insomnia in this population is due to comorbid psychiatric disorders or of the AS itself or a combination of both factors.
References
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders. 2000, Washington DC: American Psychiatric Press, 4
Ehlers S, Gillberg C: The epidemiology of Asperger syndrome. A total population study. J Child Psychol Psychiatr. 1993, 34: 1327-1350.
Wing L: The relationship between Asperger's syndrome and Kanner's autism. In Autism and Asperger syndrome. Edited by: Uta Frith. 1999, Cambridge University Press
Richdale AL: Sleep problems in autism: prevalence, cause, and intervention. Dev Med Child Neurol. 1999, 41: 60-66. 10.1017/S0012162299000122.
Paavonen J, Nieminen T, Vanhala R, Aronen E, von Wendt L: Sleep problems in Asperger children. [abstract]. Int J Circumpolar Health. 2001, 60 (suppl 1): 71-
Tantam D: Adolescence and Adulthood of Individuals with Asperger Syndrome. In Asperger Syndrome. Edited by: Klin A, Volkmar FR, Sparrow SS. 2000, The Guilford Press New York
Sateia MJ, Doghramji K, Hauri PJ, Morin CM: Evaluation of Chronic Insomnia. Sleep. 2000, 23 (2): 243-308.
Godbout R, Bergeron C, Stip E, Mottron L: A Laboratory Study of Sleep and Dreaming in a Case of Asperger's Syndrome. Dreaming. 1998, 8 (2): 75-88. 10.1023/B:DREM.0000005898.95212.58.
Gillberg C, Billstedt E: Autism and Asperger syndrome: coexistence with other clinical disorders. Acta Psychiatr Scand. 2000, 102 (5): 321-330. 10.1034/j.1600-0447.2000.102005321.x.
Ghaziuddin M, Ghaziuddin N, Greden J: Depression in persons with Autism; Implications for Research and Clinical Care. J Autism Dev Disord. 2002, 32 (4): 299-306. 10.1023/A:1016330802348.
Ehlers S, Gillberg C, Wing L: A Screening Questionnaire for Asperger Syndrome and Other High-Functioning Autism Spectrum Disorders in School Age Children. Journal Autism Dev Disord. 1999, 29 (2): 129-141. 10.1023/A:1023040610384.
Wechsler D: Wechsler Adult Intelligence Scale-Revised Manual. 1981, Cleveland: Psychological Corporation
Spitzer RL, Williams JBW, Gibbon M, First MB: Structured clinical Interview for DSM-III-R, Patient edition. 1990, Washington D.C.: American Psychiatric Press, Inc
Beck AT, Steer RA, Garbin MG: Psychometric Properties of the Beck Depression Inventory. Twenty-five years of evaluation. Clin Psychol Rev. 1988, 8: 77-100. 10.1016/0272-7358(88)90050-5.
Spitzer RL, Williams JBW, Gibbon M, First MB: Structured Clinical Interview for DSM-III-R Axis II Disorders. 1990, Washington D.C.: American Psychiatric Press, Inc
Schulz RT, Romanski LM, Tsatsanis K: Neurofunctional Models of Autistic Disorder and Asperger Syndrome: Clues from neuroimaging. In Asperger Syndrome. Edited by: Klin A, Volkmar F and Sparrow SS. 2000, The Guilford Press, New York London
Partinen M, Gislason T: Basic Nordic Sleep Questionnaire (BNSQ): a quantitated measure of subjective sleep complaints. J Sleep Res. 1995, 4 (suppl 1): 150-155.
Espie C: Insomnia: Conceptual Issues in the Development, Persistence, and Treatment of Sleep Disorder in Adults. Annu Rev Psychol. 2002, 53: 215-243. 10.1146/annurev.psych.53.100901.135243.
Coates TJ, Killen JD, George J, Marchini E, Silverman S, Thoresen C: Estimated sleep parameters: a multitrait-multimethod analysis. J Consult Clin Psychol. 1982, 50: 345-352. 10.1037//0022-006X.50.3.345.
Stein MB, Kroft CDL, Walker JR: Sleep Impairment in Patients With Social Phobia. Psychiatry Res. 1993, 49: 251-256. 10.1016/0165-1781(93)90065-O.
Tan TL, Kales JD, Kales A, Soldatos CR, Bixler EO: Biopsychobehavioral correlates of Insomnia, IV: Diagnosis Based on DSM-III. Am J Psychiatry. 1984, 141: 357-362.
Weissman MM, Greenwald S, Nino-Murcia G, Dement WC: The morbidity of insomnia uncomplicated by psychiatric disorders. Gen Hosp Psychiatry. 1997, 19 (4): 245-50. 10.1016/S0163-8343(97)00056-X.
Soderstrom H, Rastam M, Gillberg C: Temperament and character in adults with Asperger syndrome. Autism. 2002, 6 (3): 287-297. 10.1177/1362361302006003006.
Tuisku K, Tani P, Nieminen-von Wendt T, von Wendt L, Holi M, Porkka-Heiskanen T, Lauerma H, Lindberg N, Appelberg B, Wahlbeck K: Lower-limb motor restlessness in Asperger's disorder, measured using actometry. Psychiatry Res. 2002
Godbout R, Bergeron C, Limoges E, Stip E, Mottron L: A laboratory study of sleep in Aspergers syndrome. Neuroreport. 2000, 11: 127-130.
Horne JA: Human sleep loss and behaviour implications for the prefrontal cortex and psychiatric disorder. Br J Psychiatry. 1993, 162: 413-419.
Dahl RE: The regulation of sleep and arousal: Development and psychopathology. Devt Psychopathol. 1996, 8: 3-27.
Ozonoff S, McMahon Griffith E: Neuropsychological Function and the External Validity of Asperger Syndrome. In Asperger Syndrome. Edited by: Klin A, Volkmar F, Sparrow SS. 2000, The Guilford Press New York London
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-244X/3/12/prepub
Acknowledgements
We wish to thank Miss Anna-Maarit Penttilä for excellent technical assistance, Professor Dag Stenberg for useful advice in the course of the work, Tuula Kulomäki M.Sc, Anne Avellan M.Sc, and Jan-Henry Stenberg M.Sc for psychological assessment of the participants. The Research was funded by the Helsinki University Hospital (EVO: TYH 9233). Yrjö Jahnsson Foundation and The Finnish Psychiatric Association, provided additional funding.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
None declared.
Authors' contributions
This manuscript was prepared by a multidisciplinary team consisting of:
PT, generated the idea for this study, interviewed all subjects and carried out statistical analyses and prepared the manuscript together with the team
NL, had a substantial contribution in theoretical background and processing of the present study as well as in carrying out statistical analyses
TNvW and LvW, recruited AS subjects and participated in the processing of this manuscript as experts in autism spectrum disorders
LA, participated in planning and processing of this manuscript and solved crucial statistical problems
BA, allocated financial resources to this project and helped solving many theoretical problems
TP-H, supervised and participated with great impact in all stages of preparation of this manuscript.
Electronic supplementary material
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Tani, P., Lindberg, N., Nieminen-von Wendt, T. et al. Insomnia is a frequent finding in adults with Asperger syndrome. BMC Psychiatry 3, 12 (2003). https://doi.org/10.1186/1471-244X-3-12
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-244X-3-12