
Abstract
Background
The mental health needs of young children in humanitarian contexts often remain unaddressed. The lack of a validated, rapid and simple tool for screening combined with few mental health professionals able to accurately diagnose and provide appropriate care mean that young children remain without care. Here, we present the results of the principle cross-cultural validation of the “Psychological Screening for Young Children aged 3 to 6” (PSYCAa3-6). The PSYCa 3–6 is a simple scale for children 3 to 6 years old administered by non-specialists, to screen young children in crises and thereby refer them to care if needed.
Methods
This study was conducted in Maradi, Niger. The scale was translated into Hausa, using corroboration of independent translations. A cross-cultural validation was implemented using quantitative and qualitative methods. A random sample of 580 mothers or caregivers of children 3 to 6 years old were included. The tool was psychometrically examined and diagnostic properties were assessed comparing the PSYCa 3–6 against a clinical interview as the gold standard.
Results
The PSYCa 3–6 Hausa version demonstrated good concurrent validity, as scores correlated with the gold standard and the Clinical Global Impression Severity Scale (CGI-S) [rho = 0.41, p-value = 0.00]. A reduction procedure was used to reduce the scale from 40 to 22 items. The test-retest reliability of the PSYCa 3–6 was found to be high (ICC 0.81, CI95% [0.68; 0.89]). In our sample, although not the purpose of this study, approximately 54 of 580 children required subsequent follow-up with a psychologist.
Conclusions
To our knowledge, this is the first validation of a screening scale for children 3 to 6 years old with a cross-cultural validation component, for use in humanitarian contexts. The Hausa version of the PSYCa 3–6 is a reliable and a valuable screening tool for psychological distress. Further studies to replicate our findings and additional validations of the PSYCa 3–6 in other populations may help improve the delivery of mental health care to children.
Similar content being viewed by others


Background
The mental health needs of young children in humanitarian contexts often remain unaddressed [1–4]. During the acute phase of a humanitarian emergency, and in humanitarian contexts in general, psychological care of children may come far down on the list of priorities. The limited number of both local and international medical professionals combined with the relative lack of mental health professionals in these settings also hinders the implementation of mental health activities [5]. Further, even when mental health professionals are present, they are rarely specialists in young children. Psychological distress in young children is particularly difficult to evaluate by non-specialists, requiring knowledge of normal child development, as many behaviors are normal at certain ages but not at others. Young children, between 3 and 6 years old, are in a vulnerable psychological period, which can have consequences on the quality of their emotional, cognitive, and physical capacities [6, 7]. Although the psychological response of children depends on their individual, family, and social environments among many other factors, recognizing the diversity of potential psychological responses is essential to provide appropriate interventions [8–10]. The training and infrastructure needs in children’s mental health remain the ultimate goal, but in their absence, tools that help identify children who require further assessment would help to rationalize scare resources and orient children to care in humanitarian contexts.
The lack of cross-culturally valid instruments, and data about child psychological difficulties, is a public health concern in humanitarian contexts [2, 11–14]. Although scales exist for general psychological difficulties, none of them concern children aged 3 to 6 years in humanitarian contexts [15–17]. Further, before use, screening tools should be cross-culturally validated for specific contexts [11, 18–20]. Difficulties with mental health assessment include lack of consistent assessment tools for measuring psychological distress, lack of cross-cultural validation research and variation in methods for validity testing and differences in methods of translation [21]. Typically, examining mental health cross-culturally involves simply transposing Western assessment tools with no examination of their validity [22]. As result, children remain unscreened or evaluated using a scale not designed for either the specificities of childhood psychological distress or the context. The lack of a validated, rapid and simple tool for screening, combined with few mental health professionals able to accurately diagnose and provide appropriate treatment, mean that young children may remain without appropriate care.
In addition, interest in humanitarian settings has focused primarily on trauma rather than other disorders or psychological difficulties [1, 12, 23–25], adding also that most of such studies were implemented in conflict affected settings. This focus is based on the assumption that exposure to violence frequently entails post-traumatic symptoms [12, 26]. This premise has been criticized recently, as well as the use of only a post-traumatic scale for screening [11, 27]. Research addressing the cross-cultural validity of Western diagnostic classification of psychological difficulties in such contexts remains essential to ensure appropriate care is provided [11, 28–31]. Recent research has shown the importance of tools able to detect and orient children in need, but has focused on children older than 6 years with an emphasis on post-traumatic stress disorder [22, 32–35]. In addition to PTSD, recent studies have also shown the importance of addressing depression and anxiety disorders [35].
Our aim was to begin to respond to one of the gaps in addressing the mental health needs of young children in humanitarian contexts. Although there are many valid models of screening, evaluation and care, the need for a simple, rapid screening scale administered by non-specialists would fill one of the many gaps in responding to the mental health needs of young children in humanitarian contexts. We report the results of a study to cross-culturally adapt and assess the reliability, validity and psychometric properties of the Psychological Screening for Young Children aged 3 to 6 (PSYCa 3–6) following cross-cultural validation. Although the PSYCa 3–6 had been validated in several populations [36, 37], it had never undergone but had never undergone a rigorous cross-cultural validation process.
The entire validation process for the PSYCa 3-6-22 includes three steps, one called principal, including a large sample, and two called secondary, implemented to strengthen the results. The principle validation will be presented here. The overall process including the three steps will be the purpose of another publication. Selection of study sites were based on the political context and the population of children expected to be exposed to conflict to facilitate the evaluation of the post-traumatic component of the screening scale.
Methods
Setting
The principal validation took place in the rural region of Maradi, located in the south of Niger along the Nigerian border. This population is mainly Hausa speakers living in villages interspersed with Fulani and Touareg camps.
Study population
The rationale for the selection of this population included the language itself as well as the prevalence of psychological distress. First, Hausa is one of the principle languages of Sub-Saharan Africa, spoken by an estimated 30 to 50 million people. Although common language does not imply common culture, by selecting a commonly spoken language, the possibility of the use of the scale improved. Second, we expected a lower prevalence of post-trauma in this Hausa population than in other in post-conflict contexts. At the time of the study, the political environment was stable we could consider that young children had not been exposed to countrywide conflict. This was an important factor as the tool should be useful not only in situations of conflict or post-conflict. Niger faces recurrent food insecurity and malnutrition is chronic [38, 39]. Validation of a tool in Hausa, covering multiple registers, could be useful in this context. Finally, existing partnerships with the Ministry of Health of Niger provided the possibility of wide-scale use of the tool within the health system after validation. This was an important consideration providing the possibility of improving the mental health care of children in Niger.
Tool
The “Psychological Screening for Young Children aged 3 to 6” (PSYCa 3–6) is an indicative tool, not designed for diagnosis, but rather to determine a general level of psychological distress in children 3 to 6 years old. It is a hetero-questionnaire completed by the parent or caregiver through an interviewer. Unlike existing generalist tools, the PSYCa 3–6 includes a psycho-traumatic component. Data collected through the PSYCa 3–6 allows for the inferences of psychological difficulties and their main register of expression: depression, phobia, anxiety, regression, psychosomatic complaints, and post-traumatic disorder. The PSYCa 3–6, in its initial version, included 40 items concerning child behavior in the form of easy questions caregivers answer by never/not at all, or sometimes/a few times or often/frequently/always. For example, “Does your child have bad dreams or nightmares often?” Each interviewer, which may be non-specialists, read the questions and score depending to the response. At the end of administration, responses are summed to compute a score ranging from 0 to 80 with higher scores indicating greater distress. Developed in French in 1999 for Albanian and Kosovar child refugees in Macedonia, the tool has been subsequently refined and improved [37, 40]. The results of a preliminary validation in France on 52 children, showed promising results but no formal validation of the scale has been conducted [36] [Table 1.
Adaptation and translation
The adaptability of the tool was discussed with experienced mental health professionals and anthropologists originating from Niger or who had done research in the country. A linguistic and cultural translation of the tool was performed from French to Hausa. Ideally, several bilingual persons (same fluency in the two languages and experience with mental health instruments) are used to obtain translations and blind back translation [41, 42]. Here, two professional translators (Hausa/French) translated the tool independently. The two resulting versions were compared and the few differences were resolved. The translated tool was then administered to a small group of caregivers in a pilot phase for acceptance, adequacy and applicability [43]. A list containing misunderstood items developed and an alternate proposed translation was made. The final version was fixed by the two translator’s consensus taking into account differences between spoken and written Hausa.
Focus group discussions with community key informants, individual interviews and expert meetings were conducted during adaptation and translation phase. Focus groups helped to elucidate understanding of the beliefs and perceptions about child development and expectations of the outcome of treatment [44, 45]. They were also conducted to ensure understanding of each of the scale’s items and enhance the quality of the clinicians’ diagnosis during the validation phase (see methods) [46] and ensure that misclassification was minimized [47–49]. Variations in clinical presentation of psychological distress may lead to misidentification. Cultural variations, social interactions and specific contextual factors vary cross-culturally, and might influence the experience, representation, expression of psychological difficulties [50]. Consultations with psychiatrists and anthropologists and the health care staff of the hospitals in Niamey (the country’s capital) and Maradi to define developmental milestones and child psychopathology were also organized.
Training
All interviewers were selected by meeting the main criteria, experience in questionnaire administration, fluent in Hausa and French and without a background in mental health. They were trained over a three-day period on how to administer the questionnaire. After a general presentation of the tool, items were presented and discussed one by one. Role-plays were used to simulate interviews and training provided on the information and informed consent procedure. Interviewers were also trained on study exclusion criteria. The exclusion criteria for interviewers were based on visible, recognizable difficulties and interviewers were trained on the basics of mental retardation and the severe classifications of the ICD-10. A one-day pilot phase followed the theoretical training to assure standardization of administration and reinforce the theoretical training. The translator participated in the interviewer’s training and also performed an additional day of training on the translation process itself [51]. Interviewers were supervised during the duration of data collection to respond to any difficulties or questions.
Sampling
The study population included a random sample of 580 caregivers recruited between November 2009 and July 2010. A comprehensive information and awareness campaign was organized before study implementation to inform the population about the aims and objectives of the study. Caregivers were selected using cluster-based sampling, with population proportional to size weighting, a standard methodology in populations where population data is either limited or inaccurate [52]. Within the region, 68 villages or city districts were randomly chosen (22 districts in Maradi city, and 23 villages each in the districts of Madarounfa and Guidan Roumdji) [53]. The random sample in the villages followed the traditional method by spinning a pen, as random starting direction from a central location in the cluster. Households lying on this transect from the center to the border of the cluster were counted and then one of them was chosen at random. Proximity selection was then used to select subsequent households as the "next nearest" until the desired sample size was reached [52, 54].
In each household, caregivers needed to have at least one child aged 3 to 6 years old, be Hausa speakers, and resident in the study area (Maradi city, Madarounfa, Guidan Roumdji). As mothers were the most knowledgeable of the daily activities and behaviors of children, they were asked to respond to the questionnaire. Children identified by the mother/caregivers as presenting a mental disorder, mental retardation, development disorder, and/or psychosis were excluded. Interviewers also excluded children who met visible, recognizable criteria of mental retardation or grave development disorders. These children were referred immediately for free care. All mothers and caregivers were read an information letter describing the study and asked for written informed consent before enrollment.
Study procedures
The first phase of the study consisted of administration of the tool to 325 mothers and caregivers. The aim of this phase was to collect data to examine the psychometric properties of the tool, reliability and test-retest reliability before proceeding further with the validation (see data analysis). A total of 201 children completed the PSYCa 3–6 once to evaluate internal consistency, 51 completed the PSYCa 3–6 twice for temporal stability, and 51 completed the PSYCa 3–6 twice with two different interviewers for interrater reliability. During the morning, each interviewer included 7 to 8 children meeting the inclusion criteria. At midday, the interviewers met and exchanged children. Each interviewer had to provide all needed information for his colleague to find the children selected. Interrater reliability was measured by re-administering PSYCa3-6 independently on the same day at different times by two interviewers. The timeframe of re-administration was the same. The day started including 7 to 8 children, after administration, caregivers were given an appointment for the same day in the afternoon with the same interviewer.
In the second phase of the study, the interviewer administered the tool and this was followed by a clinical evaluation as the gold standard for 255 children. The psychologist completed the Clinical Global Impression-Severity Scale (CGI-S), a seven-point severity scale, assessing a patient’s current symptom severity, and answered the question “does the child need psychological/psychiatric care?”. The CGI-S is used widely in medical care and clinical research because of its face validity and practicability with the same wording irrespective of the pathology [55, 56]. The clinician also completed a semi-structured clinical interview, and performed a diagnosis based on ICD-10 classification [33, 57].The psychologist was under the supervision of a senior clinical psychologist. In case of psychopathological disorders, specific psychological care consisting of individual based care were provided at home. Mental health care providers in the area were informed of the study and were aware of any referrals for additional care [Figure 1.

Study flow-chart.
Two clinical psychologists carried out the individual interviews (CM, YM), trained in child development and cross-cultural psychology. Each individual interview was a direct and confidential. For each interview, the translator was present. Clinical psychologists were blinded to the score of the tool (administered immediately prior).
Data analysis
First, using data collected in phase I, psychometric properties were analyzed. We performed a descriptive analysis (missing data, scatter-plot of responses, floor and ceiling effects) and redundancy (estimation of Pearson’s correlation coefficient between items two by two).
Internal consistency of the PSYCAa3-6 was evaluated by Cronbach’s alpha for the entire scale. Test-retest and interrater reliability were estimated using intra-class correlation coefficients (ICC). Kappa statistics were used to calculate the degree of interrater agreement for each question.
Second, in phase II, external validity was tested on 255 children by comparing the reported PSYCa 3–6 scores against the clinical psychologists’ evaluation, answering to the question “Does the child need psychological/psychiatric care?”.To strengthen the results, PSYCa 3–6 total scores were correlated with CGI-S scores. Receiver Operating Characteristic (ROC) curve analyses were performed to evaluate the PSYCa 3–6 screening properties and determine an optimal cut-off. Kruskal-Wallis tests were used to assess the association between PSYCa 3–6 scores and each child's socio-demographic characteristics. The cut off for of 17 was based on prior use of the scale prior to its validation.
Third, an expert panel consisting of a child psychiatrist, research psychologists and a statistician reviewed the results and discussed item reduction; which items should remain, be further modified, and those to be removed (item reduction and clarification). Criteria for removal was based on the clinical importance of the item in this population and in others, the number of items covering the same clinical domain, readability, relevance, redundancy, and on psychometric criteria (floor effect, inter-item correlation, reliability and concurrent validity). We used R software (version 2.10.0) for all analyses. Item reduction and the factor analyses will be presented in a forthcoming manuscript.
Ethical considerations
The protocol was submitted for approval to the National Consultative Ethics Committee of Niger, Ministry of Public Health of Niger and the Committee for the Protection of Persons (CPP) Ile de France XI. After informed consent was obtained, caregivers were asked to answer the questionnaire. The consent process included two documents, an information sheet and consent form, both translated in Hausa. Patient data were confidential unless it was deemed necessary to protect the health of the patient. The electronic database contained no names or addresses of patients to ensure their anonymity. Children requiring psychological care received appropriate and free care by a clinical psychologist. The PSYCa 3–6, once validated, will be made available to all health actors who wish in Niger.
Results
In total, 580 children participated in the study. From December 2009 to February 2010, 325 children (160 males (49.2%) and 165 females (50.8%), mean age 52 months) were included. A total of 201 children completed the PSYCa 3–6 once to evaluate internal consistency, 51 completed the PSYCa 3–6 twice for temporal stability, and 51 completed the PSYCa 3–6 twice with two different interviewers for interrater reliability. From May 2010 to July 2010, 255 children were included for the evaluation of diagnostic properties (123 males (48.2%) and 132 girls (51.8%), mean age 52 months) [Table 2]. The item reduction procedure yielded a 22-item instrument (scores 0–44) and results are presented as follows.
In the population of 580 children, the proportion of missing data or “I don’t know” response per item was low (average 1.6%, <5% for all but 4 items) suggesting good acceptability and that it was easy to complete. With the exception of item 21 (“moves constantly”), the distribution of answers was left-skewed with a higher floor rather than ceiling effect reflecting the low traumatic exposition of this sample. The mean PSYCa 3–6 scores were 7.13 (SD = 3.95, interquartile range 4–9, min 0 max 27). There was no significant difference between the PSYCa 3–6 scores of boys and girls (p = .16), or between children 36, 48, or 60 months of age (p = 0.5) but scores on the PSYCa 3–6 were significantly higher for children who were detected by their own family as having difficulties such as fears, outbursts, sleep disorders, recurrent nightmares problem and were oriented to a traditional practitioner (p = 0.0002).
The test-retest reliability of the PSYCa 3–6 was found to be high (ICC 0.81, CI9% [0.68; 0.89]). Interrater reliability was satisfactory (ICC of 0.69, CI 95% [0.45; 0.80]). The tool demonstrated acceptable internal consistency (Cronbach’s alpha 0.61, CI 95% [0.54; 0.65] for a screening tool validation including several dimension (depression, anxiety, post traumatic component) [20, 58].
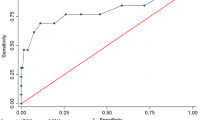
During the second phase, psychologists identified 31 children in need of psychological orientation and 224 children not requiring care. Concerning the CGI-S scale among these 255 children, 187 (73.3%) were rated as 1 “normal, not at all ill”, 29 (11.4%) with borderline CGI, 23 (9%) mildly ill, 12 (4.7%) moderately ill, 4 (1.6%) markedly ill. None were rated as severely or extremely ill. Overall, the 255 children evaluated by psychologist had a mean CGI-S of 1 [1; 3] for the children without orientation and 4 [2; 5] for children oriented towards additional assessment (p < 0.001). The PSYCa 3–6 exhibited significant positive correlations with CGI severity scale (rho = 0.41, p-value = 0.0001). Mean PSYCa 3–6 scores were significantly higher among the 31 children requiring care than those that did not (p-value = 0.0001 [Table 3). The frequency of positive responses to twenty-two items in children requiring care and in other children is shown Figure 2. The ROC analysis resulted in an area under the curve of 0.81 (CI 95% [0.73, 0.89]) [Figures 2, 3 and 4. When the cut-off value of PSYCa 3–6 was nine according to the point closest to the upper left-hand corner of the graph, the sensitivity and specificity were 0.77 and 0.71, respectively [59].

Frequency of positive responses (sometimes, often) between children needing care and others.

Histograms for PSYCa 3–6 score.

Receiver operating characteristics (ROC) curve of the PSYCa 3–6.
Discussion
To our knowledge, this is the first validation of a screening scale for children aged 3 to 6 years old, with a cross-cultural validation component, for use in humanitarian contexts. The PSYCa 3–6 enables the rapid screening of children and can be administered by non-specialists. The results of this study suggest that the Hausa version of the PSYCa 3–6 is a reliable and a valuable tool for screening psychological distress in children 3 to 6 years old. The tool was acceptable to caregivers and interviewers (after training and piloting). The sample of patients for this validation was large compared to other validation studies further strengthening our results [13, 37, 42, 60].
Screening tools provide an important means to facilitate addressing the mental health needs of children in humanitarian emergencies and contexts. Difficulties of young children may remain unnoticed or undetected by both local and international health actors [61] and may have short and/or long term developmental consequences [8, 45, 62, 63]. Screening children provides a means to identify those in need of additional evaluation and eventual care as well as recognizing the limited resources available in these contexts. The reduction from a 40 to 22-item scale also provides additional encouragement that the scale could be administered to an often large number of children in a relatively short period of time. The simple administration of the screening scale also provides additional awareness and understanding of the overall status of the population for health care workers addressing the situations. In humanitarian contexts, a part from the acute phase of an emergency, the tool could also be used to identify difficult to reach children (due to either distance or isolation for example) and refer only those in need of additional evaluation to health structures. However, it is important to highlight that this tool allows for the identification of children requiring further evaluation, but the lack of mental health professionals remains. As with all public health interventions, identification of children in need does not unfortunately always follow with their receipt of appropriate care. Greater investments are needed to ensure that children mental health needs are addressed, and certainly that they are only screened if appropriate care is available [64, 65].
We would like to highlight two key points for discussion, especially relevant for future validation studies. First, the translation process was long and involved a linguistic specialist, anthropologist, psychiatrist and psychologist. We first attempted a classical translation/back translation procedure [13, 42, 66–70], but due to significantly differences concerning written and spoken Hausa, we used independent translations resolved by discussion and pilot testing.
Second, due to the lack of previously cross-cultural validated scales in Hausa, we chose to use a classic individual interview by a psychologist as our gold standard [47, 69, 70]. Two major types of assessment of mental disorders are used in epidemiological studies: semi structured clinical interviews and lay-administered structure diagnostic questionnaires [71]. To date, there has not been agreement the most appropriate validation method for global mental health research with children [22, 42, 72, 73]. Although use of a clinical interview appeared here the most rigorous choice in this context as opposed to using another tool. The psychologist, trained in cross-cultural psychology and mental health care in children based their diagnosis on ICD-10 classification. To strengthen the clinical interviews, qualitative research concerning child development, child rearing, psychological difficulties in Hausa culture was conducted [35]. Concordance between the clinical interview and the PSYCa 3–6 suggest that use of the ICD-10 did not influence the results presented here.
An apparent limitation is that we do not present a traditional psychometric validation. The traditional validation process (item analysis, factor analysis, etc.) of a psychometric tool was developed in the absence of a gold standard [74]. The objective of the PSYCa 3–6 is to screen subjects who need further evaluation for psychiatric/psychological care. In an ideal situation, the clinician decides, after an interview, if such a care is required. Our gold standard was the clinician’s answer to the question: “does the child need psychological/psychiatric care?”. For this reason, we validated the PSYCa 3–6 as compared with the above question and classical statistics. Most other screening tools in medicine are based on the same methodology; this is the case for example for scores of gravity in intensive care units such as the APACHE score [75], validated against mortality rather than with psychometric tools. After secondary evaluations have been completed, the factor structure of the PSYCa 3–6, corresponding to different clinical conditions should be investigated. The internal consistency may be viewed as a limitation from a psychometric perspective. However, as the PSYCa 3–6 is a screening tool for psychological difficulties, the scale is not one-dimensional to ensure the detection of psychological difficulties in several area of psychopathology. As the PSYCa 3–6 includes several domains, this is not unexpected.
An additional limitation concerns the test-retest and interrater reliability. Both were estimated from interviews performed on the same day. Time between the different interviews is problematic since short interval are prone to recall bias, while long intervals risk being associated with the clinical evolution of the subject evaluated.
Finally, we used initially a cut-off of 17, based on the results of previous use of the scale [36, 40]. This number was calculated on 40 items, the initial version, scoring up to 80 (2 points per item). As previously documented, cut-off scores established with Western child populations are not necessarily comparable in others settings [27, 43]. After reduction of the scale and analysis, we refined the cut-off to 8/9. The cut-off requires further analysis in subsequent validations to assure stability in other cross-cultural contexts.
Conclusions
The results of this first validation show promising results, suggesting that the PSYCa 3–6 should be validated in other contexts, to test the post-traumatic component of the tool and to simplify further the instrument. From a public health standpoint, the ability to identify potential psychological difficulties in young children represents a significant advancement for the possibility of addressing children’s’ mental health needs in difficult contexts [76]. Additional efforts to adapt and validate simple screening scales for use in humanitarian contexts should be encouraged.
Author contributions
CM coordinated the implementation of the study, participated in the interpretation of the results and drafted the manuscript. CB performed the statistical analysis and. YM participated in the design of the study and in revising the manuscript. SH participated in the design of the study and revised the final manuscript. MDD and MML participated in the design of the study and revising the manuscript. BF participated in the design of the study, statistical analysis, interpretation of the results and revising the manuscript. ARL provided interpretation of the results and revised the manuscript. RFG and MRM conceived the study and the protocol, participated in its design and implementation and revised the manuscript. All authors read and approved the final manuscript.
Funding
This study was funded by Medecins sans Frontieres.
References
Jones L, Rrustemi A, Shahini M, Uka A: Mental health services for war-affected children: Report of a survey in Kosovo. Br J Psychiatry. 2012, 540-546.
Jordans MJD, Komproe IH, Tol WA, Susanty D, Vallipuram A, Ntamatumba P, Lasuba AC, De Jong JTVM: Practice-driven evaluation of a multi-layered psychosocial care package for children in areas of armed conflict. Community Ment Health J. 2011, 47 (3): 267-277. 10.1007/s10597-010-9301-9.
Omigbodun O: Developing child mental health services in resource-poor countries. Int Rev Psychiatr (Abingdon, England). 2008, 20 (3): 225-
Shatkin JP, Belfer ML: The Global Absence of Child and Adolescent Mental Health Policy. Child Adolesc Ment Health. 2004, 9 (3): 104-108. 10.1111/j.1475-3588.2004.00090.x.
Vostanis P: Child mental health services across the world: opportunities for shared learning. Child Adolesc Ment Health. 2007, 12 (3): 113-114. 10.1111/j.1475-3588.2007.00464.x.
Larsson AS, Granhag PA: Interviewing children with the cognitive interview: assessing the reliability of statements based on observed and imagined events. Scand J Psychol. 2005, 46 (1): 49-57. 10.1111/j.1467-9450.2005.00434.x.
Marans S, Adelman A: Experiencing Violence in a Developmental Context. Children in a violent society. Children in a violent society. 1997, The Guilford Press, Ososfsky, 202-222.
Zeanah CH: Handbook of Infant Mental Health. 1993, The Guildford Press, New York
Petot D: Evaluation clinique en psychopathologie de l’enfant. 2006, Dunod, Paris
Wallon H: L’évolution psychologique de l'enfant. 2002, Colin, Paris
Mollica RF, Cardozo BL, Osofsky HJ, Raphael B, Ager A, Salama P: Mental health in complex emergencies. Lancet. 2004, 364 (Issue 9450): 2058-2067.
Jordans MJD, Komproe IH, Tol WA, De Jong JTVM: Screening for psychosocial distress amongst war-affected children: cross-cultural construct validity of the CPDS. J Child Psychol Psychiatry. 2009, 50 (4): 514-523. 10.1111/j.1469-7610.2008.02028.x.
Jordans MJD, Komproe IH, Ventevogel P, Tol WA, De Jong JTVM: Development and validation of the child psychosocial distress screener in Burundi. Am J Orthopsychiatry. 2008, 78 (3): 290-299.
Flaherty JA, Gaviria M, Pathak D, Mitchelle T, Wintrob R, Richman JA, Birz S: Developing instruments for cross-cultural psychiatric research. J Nerv Ment Dis. 1988, 176 (5): 257-263.
Goodman R, Ford T, Simmons H, Gatward R, Ord TF, Ward RGAT: Using the Strengths and Difficulties Questionnaire ( SDQ ) to screen for child psychiatric disorders in a community sample. Br J Psychiatry. 2000, 177: 534-539. 10.1192/bjp.177.6.534.
Goodman R: The strengths and difficulties questionnaire: a research note. J Child Psychol Psychiatry. 1997, 38: 581-586. 10.1111/j.1469-7610.1997.tb01545.x.
Goodman R, Scott S: Comparing the strengths and difficulties questionnaire and the child behavior checklist: is small beautiful?. J Abnorm Child Psychol. 1999, 27 (1): 17-24. 10.1023/A:1022658222914.
Van Ommeren M: Validity issues in transcultural epidemiology. Br J Psychiatry. 2003, 182: 376-378. 10.1192/bjp.182.5.376.
Kirmayer LJ: Clinical presentation of depression and anxiety: implications for diagnosis and treatment. J Clin Psychiatr. 2001, 62 (13): 22-28.
Ghanizadeh A: Scale validation of the strengths and difficulties questionnaire in Iranian children. Iranian Journal of Psychiatry. 2007, 2 (2): 65-71.
Cha ES, Kim KH, Erlen JA: Translation of scales in cross-cultural research: issues and techniques. J Adv Nurs. 2007, 58 (4): 386-395. 10.1111/j.1365-2648.2007.04242.x.
Murray LK, Bass J, Chomba E, Imasiku M, Thea D, Semrau K, Cohen JA, Lam C, Bolton P: Validation of the UCLA Child Post Traumatic Stress Disorder-reaction Index in Zambia. Int J Ment Heal Syst. 2011, 5: 5-24. 10.1186/1752-4458-5-5.
Folmar S, Palmes GK: Cross-cultural psychiatry in the field: collaborating with anthropology. J Am Acad Child Adolesc Psychiatr. 2009, 48 (9): 873-876. 10.1097/CHI.0b013e3181ae09b6.
Thabet AAM, Abed Y, Vostanis P: Comorbidity of PTSD and depression among refugee children during war conflict. J Child Psychol Psychiatry. 2004, 45 (3): 533-542. 10.1111/j.1469-7610.2004.00243.x.
Qouta S, Punamaki RL, El Sarraj E: Prevalence and determinants of PTSD among Palestinian children exposed to military violence. Eur Child Adolesc Psychiatr. 2003, 12 (6): 265-272. 10.1007/s00787-003-0328-0.
Jordans JDM, Ventevogel P, Komproe HI, Tol AW, De Jong JTVM: Development and validation of the child psychosocial distress screener in Burundi. Am J Orthopsychiatry. 2008, 78 (3): 290-299.
Silove D, Ekblad S, Mollica R: The rights of the severely mentally ill in post-conflict societies. Lancet. 2000, 355: 1548-1549. 10.1016/S0140-6736(00)02177-2.
Barenbaum J, Ruchkin V, Schwab-Stone M: The psychosocial aspects of children exposed to war: practice and policy initiatives. J Child Psychol Psychiatry. 2004, 45 (1): 41-62. 10.1046/j.0021-9630.2003.00304.x.
Betancourt TS, Williams T: Building an evidence base on mental health interventions for children affected by armed conflict. Intervention. 2009, 6 (1): 39-56.
Lustig SL, Kia-Keating M, Knight WG, Geltman P, Ellis H, Kinzie JD, Keane T, Saxe GN: Review of child and adolescent refugee mental health. J Am Acad Child Adolesc Psychiatr. 2004, 43 (1): 24-36. 10.1097/00004583-200401000-00012.
Tol WA, Komproe IH, Susanty D, Jordans MJD, Macy RD, De Jong JTVM: School-based mental health intervention for children affected by political violence in Indonesia: a cluster randomized trial. JAMA. 2008, 300 (6): 655-662. 10.1001/jama.300.6.655.
Catani C, Kohiladevy M, Ruf M, Schauer E, Elbert T, Neuner F: Treating children traumatized by war and Tsunami: a comparison between exposure therapy and meditation-relaxation in North-East Sri Lanka. BMC Psychiatry. 2009, 9: 22-10.1186/1471-244X-9-22.
Elbert T, Schauer M, Schauer E, Huschka B, Hirth M, Neuner F: Trauma-related impairment in children–a survey in Sri Lankan provinces affected by armed conflict. Child Abuse Negl. 2009, 33 (4): 238-246. 10.1016/j.chiabu.2008.02.008.
Neuner F, Schauer E, Catani C, Ruf M, Elbert T: Post-tsunami Stress: A Study of Posttraumatic Stress Disorder in Children Living in Three Severely Affected Regions in Sri Lanka. J Trauma Stress. 2007, 19 (3): 339-347.
Klasen F, Oettingen G, Daniels J, Post M, Hoyer C, Adam H: Posttraumatic resilience in former Ugandan child soldiers. Child Dev. 2010, 81 (4): 1096-1113. 10.1111/j.1467-8624.2010.01456.x.
Mouchenik Y, Gaboulaud V, Pérouse de Montclos MO, Monge S, Baubet T, Taïeb OMM: Questionnaire Guide d’Evaluation des difficultés psychologiques de jeunes enfants pris en charge par la Protection de l'Enfance. Enfance. 2010, 02: 143-166.
Mouchenik YE: Evaluer les troubles psychologiques post-traumatiques chez les enfants de moins de six ans. A propos d’une étude réalisée à Débar (Macédoine). L’autre, Cliniques, cultures et sociétés. 2001, 2: 359-366.
Wuehler SE, Biga HA: Situational analysis of infant and young child nutrition policies and programmatic activities in Niger. Matern Child Nutr. 2011, 7 (1): 133-156.
Isanaka S, Nombela N, Djibo A, Poupard M, VanBeckhoven D, Gaboulaud , Guerin PJ, Grai RF: Effect of preventive supplementation with ready-to-usetherapeutic food on the nutritional status, mortality and morbidity of children 6 to 60 months in Niger: a cluster randomized trial. JAMA. 2009, 301 (3): 277-285. 10.1001/jama.2008.1018.
Mouchenik Y, de Pérouse de Montclos MO, Monge S, Gaboulaud V: Difficultés psychologiques des enfants de 3 à 6 ans placés en urgence: Research report. 2007, Direction de l'action sociale et de la Santé, cahier de Chaligny, Paris
Baubet T, Moro MR: Psychopathologie transculturelle. 2009, Edition Masson, Paris
Kohrt BA, Jordans MJD, Tol WA, Luitel NP, Maharjan SM, Upadhaya N: Validation of cross-cultural child mental health and psychosocial research instruments: adapting the Depression Self-Rating Scale and Child PTSD Symptom Scale in Nepal. BMC Psychiatry. 2011, 11 (1): 127-10.1186/1471-244X-11-127.
Achenbach TM, Becker A, Dopfner M, Heiervang E, Roessner V, Steinhausen HC, Rothenberger A: Multicultural assessment of child and adolescent psychopathology with ASEBA and SDQ instruments: Research findings, applications, and future directions. J Child Psychol Psychiatr. 2008, 49 (3): 251-275. 10.1111/j.1469-7610.2007.01867.x.
Verhoef MJ, Casebeer AL HR: Assessing Efficacy of Complementary Medicine: Adding Qualitative Research Methods to the “Gold Standard. J Alternative Compl Med. 2002, 8 (3): 275-281. 10.1089/10755530260127961.
Osofsky JD: The impact of violence on children. Future Child. 1999, 9 (3): 33-49. 10.2307/1602780.
Canino G, Alegria M: Psychiatric diagnosis–is it universal or relative to culture?. J Child Psychol Psychiatry. 2008, 49 (3): 237-250. 10.1111/j.1469-7610.2007.01854.x.
Draguns JG, Tanaka-Matsumi J: Assessment of psychopathology across and within cultures: issues and findings. Behav Res Ther. 2003, 41: 755-776. 10.1016/S0005-7967(02)00190-0.
Bhui K, Mohamud S, Warfa N, Craig TJ, Stansfeld S: Cultural adaptation of mental health measures: improving the quality of clinical practice and research. Br J Psychiatry. 2003, 183: 184-186. 10.1192/bjp.183.3.184.
Daley TC: The need for cross-cultural research on the pervasive developmental disorders. Transcult Psychiatr. 2002, 39 (4): 531-550.
Moro MR, Heidenreich F: Children all over the world. The International Association of Child and Adolescent Psychiatry bulletin (IACAPAP). 2004, 1: 8-19.
Rousseau C, Measham T, Moro M-R: Working with interpreters in child mental health. Child Adolesc Ment Health. 2011, 16 (12): 55-59.
Hoshaw-woodard WS: Description and comparison of the methods of cluster sampling and lot quality assurance sampling to assess immunization coverage. 2001, World Health Organization, Geneva
Niger: Le Niger en chiffres. Institut National de la Statistique. www.stat-niger.org/statistique
The World Health Survey: Sampling Guidelines for Participating Countries. http://www.who.int/entity/healthinfo/survey/whssam
Guy W: Clinical Global Impressions. ECDEU Assessment Manual for Psychopharmacology. 1976, DHEW publication, Rockville, 218-222.
Kadouri A, Corruble E, Falissard B: The improved Clinical Global Impression Scale (iCGI): development and validation in depression. BMC Psychiatry. 2007, 7: 7-10.1186/1471-244X-7-7.
Janca A, Hiller W: ICD-10 checklists–a tool for clinicians’ use of the ICD-10 classification of mental and behavioral disorders. Compr Psychiatry. 1996, 37 (3): 180-187. 10.1016/S0010-440X(96)90034-6.
Beusenberg M, Orley J: A user’s guide to the self reporting questionnaire (SRQ). 1994, WHO Division of mental health, Geneva
Zweig MH, Campbell G: Receiver–operating characteristics (ROC) plots: a fundamental evaluation tool in clinical medicine. Clin Chem. 1993, 39 (4): 561-577.
Foa EB, Johnson KM, Feeny NCTK: The Child PTSD Symptom Scale: A Preliminary Examination of its Psychometric Properties. J Clin Child Psychol. 2001, 30 (3): 376-384. 10.1207/S15374424JCCP3003_9.
Tareen A, Elena Garralda M, Hodes M: Post-traumatic stress disorder in childhood. Arch Dis Child Educ Pract. 2007, 92 (1): 1-6.
Espié E, Gaboulaud V, Baubet T, Casas G, Mouchenik Y, Yun O, Grais FG, Moro MR: Trauma-related psychological disorders among Palestinian children and adults in Gaza and West Bank, 2005–2008. Int J Ment Heal Syst. 2009, 3 (1): 21-10.1186/1752-4458-3-21.
Espié E, Ouss L, Gaboulaud V, Candilis D, Ahmed K, Cohuet S, Baubet T, Grais FG, Moro MR: Against the Odds: Psychomotor Development of Children Under 2 years in a Sudanese Orphanage. J Trop Pediatr. 2011, 57 (6): 412-417. 10.1093/tropej/fmq117.
Onyut LP, Neuner F, Schauer E, Ertl V, Odenwald M, Schauer M, Elbert T: The nakivale camp mental health project: building local competency for psychological assistance to traumatised refugees. Intervention. 2004, 2 (2): 90-107.
Schauer E, Neuner F, Elbert T, Ertl V, Onyut LP, Odenwald M, Schauer M: Narrative exposure therapy in children: a case study. Intervention. 2004, 2 (1): 18-32.
Omoro SAO, Fann JR, Weymuller EA, Macharia IM, Yueh B: Swahili translation and validation of the Patient Health - 9 depression scale in the kenyan head and neck cancer patient population. Int J Psychiatr Med. 2006, 36 (3): 367-381. 10.2190/8W7Y-0TPM-JVGV-QW6M.
Fountoulakis KN, Iacovides A, Kleanthous S, Samolis S, Gougoulias K, St Kaprinis G, Bech Per : The Greek translation of the symptoms rating scale for depression and anxiety: preliminary results of the validation study. BMC Psychiatry. 2003, 3: 21-10.1186/1471-244X-3-21.
Montazeri A, Torkan B, Omidvari S: The Edinburgh Postnatal Depression Scale (EPDS): translation and validation study of the Iranian version. BMC Psychiatry. 2007, 6: 4-9.
Chibanda D, Mangezi W, Tshimanga M, Woelk G, Rusakaniko P, Stranix-Chibanda L, Midzi S, Maldonado Y, Shetty AK: Validation of the Edinburgh Postnatal Depression Scale among women in a high HIV prevalence area in urban Zimbabwe. Arch Wom Ment Health. 2010, 13 (3): 201-206. 10.1007/s00737-009-0073-6.
Adewuya AO, Ola BA, Dada AO, Fasoto OO: Validation of the Edinburgh Postnatal Depression Scale as a screening tool for depression in late pregnancy among Nigerian women. Psychosom Obstet Gyneco. 2006, 27 (4): 267-272. 10.1080/01674820600915478.
Brugha TS, Bebbington PE, Jenkins R, Meltzer H, Taub NA, Janas M, Vernon J: Cross validation of a general population survey diagnostic interview: a comparison of CIS-R with SCAN ICD-10 diagnostic categories. Psychol Med. 1999, 29 (5): 1029-1042. 10.1017/S0033291799008892.
Bolton P, Tang AM: Using Ethnographic methods in the selection of post-disaster. Prehosp Disaster Med. 2004, 19 (1): 97-101.
Bolton PA, Weiss WM: Communicating across cultures: improving translation to improve complex emergency program effectiveness. Prehosp Disaster Med. 2001, 16 (4): 252-256.
Nunnally JC, Bernstein IH: Psychometric Theory. 1994, McGraw-Hill, New York
Wagner DP, Knaus WA, Draper EA: Statistical validation of a severity of illness measure. Am J Public Health. 1983, 73 (8): 878-884. 10.2105/AJPH.73.8.878.
Patel V, Flisher AJ, Nikapota A, Malhotra S: Promoting child and adolescent mental health in low and middle income countries. J Child Psychol Psychiatry. 2008, 49 (3): 313-334. 10.1111/j.1469-7610.2007.01824.x.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-244X/12/170/prepub
Acknowledgements
The authors wish to thank all of the participants in this study. We also wish to thank our collaborators at the Ministry of Health in Niamey and Maradi, the psychiatric ward of the General Hospital of Niamey. Mrs. Hadiza Moussa graciously provided her anthropological expertise.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Marquer, C., Barry, C., Mouchenik, Y. et al. A rapid screening tool for psychological distress in children 3–6years old: results of a validation study. BMC Psychiatry 12, 170 (2012). https://doi.org/10.1186/1471-244X-12-170
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-244X-12-170