
Abstract
Background
Dengue, a mosquito-borne flavivirus infection, is endemic in Southeast Asia. Currently, the incidence has been increasing among adults.
Case presentation
A 26-year-old Thai woman, G1P0 31 weeks pregnancy, presented with epigastric pain for 1 day. She also had a high-grade fever for 4 days. The physical examination, complete blood counts as well as serology confirmed dengue fever. The patient was under conservative treatment despite severe thrombocytopenia. She was well at the 3rd day of discharge and 1-week follow-up. The pregnancy continued until term without any complication and she delivered vaginally a healthy female baby.
Conclusions
More cases of dengue infection in pregnancy can be found due to the increasing incidence during adulthood. It should be suspected when a pregnant woman presents with symptoms and signs like in a non-pregnant. Conservative treatment should be conducted unless there are any complications.
Similar content being viewed by others


Introduction
Dengue is a mosquito-borne flavivirus infection, is endemic in Southeast Asia, including Thailand [1, 2]. Currently, the incidence of dengue infection has been increasing among adults [1, 3]. Then, the more cases of dengue infection occurring in pregnancy are found. Herein, I report an additional case of dengue fever (DF) in pregnancy which ended with a favorable outcome.
Case presentation
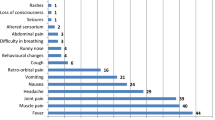
A 26-year-old, gravida 1,31 weeks pregnant woman, presented to the hospital with complaints of epigastric pain, bleeding per gum and petechiae hemorrhage for 1 day. She had a high-grade fever for 5 days prior to admission. She was first seen at antenatal clinic at 12 weeks pregnancy, and there was no abnormality detected until this presentation. Her past medical and family history were unremarkable.
On admission, her body temperature was 37°c, blood pressure was 110/80 mmHg, pulse rate was 80/mim and respiratory rate was 20/min. She had mild dehydration, normal breathing sound and heart sound. Her liver was enlarged 1 cm below the right costal margin with mild tenderness. The fundal height was compatible with 31 weeks' gestation and fetal heart rate was 144 beats/min. Petechiae sized 1–2 mm in diameter were found around her face, forearms and both pretibial areas.
Laboratory analysis on admission gave the following results: hemoglobin 11.9 g/dl, hematocrit 35%, white blood cells count 7,440/mm3 with 50% neutrophil, 45% lymphocytes and 3% atypical lymphocytes; platelet count was 10,100 /mm3
She was diagnosed as dengue fever in pregnancy and was treated with intravenous fluid replacement. She was put under close observation for vital signs and bleeding precaution. Twenty-four hours later, the epigastric pain disappeared and the vital sings were within normal limits. The hematocrit was 30% and the platelet count was 6,320 /mm3. Platelet concentration was prepared but it was not used because the patient had no clinical bleeding. On the third day, she gradually recovered and had an itching convalescent rash on both pretibial areas. The hematocrit was 31% with platelet count 15,000 /mm3. She was discharged on the fourth day. On 1 week follow-up, she was healthy and hematocrit was 32% with platelet count 354,000 /mm3. Serologic study of paired serum detecting IgG antibody titer by the haemagglutination inhibition test indicated secondary dengue serotype 2 infection. After that, she had an uneventful antenatal care. At the 39 weeks' gestation, she delivered a healthy female baby weighing 2,630 grams by vaginal route with APGAR scores 9 and 10 at 1 and 5 minutes, respectively. No abnormality in newborn was detected.
Discussion
Dengue is an Aedes aegypti mosquito-borne infection, caused by dengue virus serotypes 1,2,3 and 4. It is a major public health problem in tropical countries [4]. There are few reports of DF and DHF in pregnancy from literature review. Nowadays, the incidence has been increasing among adults [1, 3], more cases of DF and DHF in pregnancy like this present case can be found.
The clinical pictures of this case were the same as found in non-pregnant patients and previous reports [2, 5, 6]. She had acute dengue viral hepatitis with bleeding tendencies. However, she had no other associated features that might fulfill the criteria as described by the World Health Organization [7], such as rise in the hematocrit (≥ 20%) and clinical evidence of increased vascular permeability, manifested by generalized edema, pleural effusion and ascites. These presentations might be confused with other obstetrics complications, such as HELLP syndrome (hemolysis, elevated liver enzyme and low platelet counts) and other medical disease. A high index of suspicion is therefore required for the diagnosis, especially in areas of endemicity. Detailed history taking is helpful in diagnosis. The others hematologic signs, such as thrombocytopenia and atypical lymphocytosis, similarly detected in this case are also helpful for the diagnosis [8]. Serologic test is used to confirm the diagnosis and detect the specific serotype. Serologic diagnosis depends on the presence of IgM antibody or a rise in IgG antibody titer in paired acute and convalescent phase serum. Currently, the most widely used IgM assay is a capture ELISA (enzyme-linked immunosorbent assay). If sample positive for IgM capture ELISA, it should be reported as a probable dengue, not a confirmed dengue, since IgM antibody may persist at detectable levels for two or more months after infection. For a diagnosis of confirmed dengue, dengue virus should be identified by isolation, immuohistochemistry in necrosy tissue, or there should be a four-fold rise in antibody titer using a type-specific plaque reduction neutralization test [9]. This case was confirmed secondary dengue infection by four-fold rise in IgG antibody using the haemagglutination inhibition test.
Regarding the effect of DF and DHF in pregnancy, it hardly caused any infant abnormality, but DHF might be responsible for fetal death [4]. Fortunately, in this case, the baby appeared normal. Although rare, there had been reports about vertical transmission of dengue virus [2, 5]. Those cases occurred at or near the time of delivery. Those infants had common clinical features of thrombocytopenia, fever, hepatomegaly and varying degrees of circulatory insufficiency [5]. However, this case occurred remote from term pregnancy, and these clinical features were not found in newborn infant.
Another possible effect of DF and DHF in pregnancy is bleeding due to severe thrombocytopenia especially in high risk cases, such as placenta previa [4]. In this case, although the patient had very low platelet counts, no hemorrhagic complication was occurred. Platelet concentration was not given. This suggests that platelet concentration may not be given even severe thrombocytopenia regardless of clinical bleeding.
Management of this case was conservative, with intravenous fluid replacement and close observation of vital signs and bleeding, as practiced in the non-pregnant cases and previous reports [2, 5, 6]. Blood component should be prepared but given only in bleeding cases.
Conclusions
More cases of dengue infection in pregnancy can be found because of the increasing incidence of dengue infection among adults. The infection should be suspected when a pregnant woman presents with the similar pattern of symptoms and signs like in a non-pregnant case. Conservative treatment should be given unless there are complications.
References
Goh KT: Dengue – a re-emerging infectious disease in Singapore. Ann Acad Med Singapore. 1997, 26: 664-670.
Thaithumyanon P, Thisyakorn U, Deerojnawong J, Innis BL: Dengue infection complicated by severe hemorrhage and vertical transmission in a parturient woman. Clin Infect Dis. 1994, 18: 248-249.
Teeraratkul A, Limpakarnjanaral K: Three decades of dengue hemorrhagic fever surveillance in Thailand 1958–1987. Southeast Asian J Trop Med Public Health. 1990, 21: 684-
Carles G, Peiffer H, Talarmin A: Effects of dengue fever during pregnancy in French Guiana. Clin Infect Dis. 1999, 28: 637-640.
Chye JK, Lim CT, Ng KB, Lim JM, George R, Lam SK: Vertical transmission of dengue. Clin Infect Dis. 1997, 25: 1374-1377.
Bunyavejchevin S, Tanawattanacharoen S, Taechakraichana N, Thisyakorn U, Tannirandorn Y, Limpaphayom K: Dengue hemorrhagic fever during pregnancy: antepartum, intrapartum and postpartum management. J Obstet Gynaecol Res. 1997, 23: 445-448.
World Health Organization: Dengue hemorrhagic fever: diagnosis, treatment and control. Geneva, World Health Organization. 1986
Thisyakorn U, Nimmannitya S, Ningsanond V, Soogarun S: Atypical lymphocyte in dengue hemorrhagic fever: its value in diagnosis. Southeast Asian J Trop Med Public Health. 1984, 15: 32-36.
Rigau-Perez JG, Clark GG, Gubler DJ, Reiter P, Sanders EJ, Vorndam AV: Dengue and dengue haemorrhagic fever. Lancet. 1998, 352: 971-977. 10.1016/S0140-6736(97)12483-7.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2393/1/7/prepub
Acknowledgements
Written consent was obtained from the patient or their relative for publication of the patient's details.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
None declared
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Phupong, V. Dengue fever in pregnancy: a case report. BMC Pregnancy Childbirth 1, 7 (2001). https://doi.org/10.1186/1471-2393-1-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2393-1-7