
Abstract
Background
Data on encephalitis in Thailand have not been completely described. Etiologies remain largely unknown. We prospectively analyzed 103 Thai patients from 27 provinces for the causes of encephalitis using clinical, microbiological and neuroimaging indices; caseswithout a diagnosis were evaluated for autoimmune causes of encephalitis.
Methods
Patients with encephalitis and/or myelitis were prospectively studied between October 2010 and August 2012. Cases associated with bacterial, rickettsial and mycobacterial diseases were excluded. Herpes viruses 1-6 and enteroviruses infection was diagnosed using PCR evaluation of CSF; dengue and JE viruses infection, by serology. The serum of test-negative patients was evaluated for the presence of autoantibodies.
Results
103 patients were recruited. Fifty-three patients (52%) had no etiologies identified. Twenty-five patients (24%) were associated with infections. Immune encephalitis was found in 25 (24%); neuropsychiatric lupus erythematosus (4), demyelinating diseases (3), Behcet’s disease (1) and the remaining had antibodies to NMDAR (5), ANNA-2 (6), Yo (2), AMPA (1), GABA (1), VGKC (1) and NMDA coexisting with ANNA-2 (1). Presenting symptoms in the autoimmune group included behavioral changes in 6/25 (versus 12/25 in infectious and 13/53 in unknown group) and as psychosis in 6/25 (versus 0/25 infectious and 2/53 unknown). Seizures were found in 6/25 autoimmune, 4/25 infectious and 19/53 unknown group. Two patients with anti-ANNA-2 and one anti-Yo had temporal lobe involvement by magnetic resonance imaging. Two immune encephalitis patients with antibodies to NMDAR and ANNA-2 had ovarian tumors.
Conclusions
Autoantibody-associated encephalitis should be considered in the differential diagnosis and management algorithm regardless of clinical and neuroimaging features.
Similar content being viewed by others

Background
The priority in managing encephalitis is to first exclude infectious causes, many of which are effectively treated using antimicrobial agents. Non-infectious causes of encephalitis due to autoimmune and paraneoplastic etiologies, are also a diagnostic priority as these syndromes may be life-threatening, are often associated with an underlying malignancy or systemic disease, and may be treatable if diagnosed early. Despite dramatic advances in identifying the protean causes of encephalitis, a significant proportion of cases still defy diagnostic work-up. Recent international studies reported greater than 50% of encephalitis patients as have no etiology identified, despite extensive evaluation [1, 2]. The California Encephalitis Project (CEP) initiated in 1998 [3] reported that 25% of 334 patients had confirmed or possible infectious etiologies, whereas 208 cases (62%) lacked a diagnosis. Although patients with lymphocytic and normal glucose cerebrospinal fluid (CSF) profile are usually suspected to have a viral meningoencephalitis, there is growing evidence of another entity capable of producing an aseptic CSF profile autoantibody-associated encephalitis.
In 2004, Thieben et al published a series of 7 patients with potentially reversible autoimmune limbic encephalitis associated with neuronal potassium channel antibody [4]. Vincent et al reported another 10 cases with limbic encephalitis associated with low plasma sodium that were identified as potassium channel antibody-associated encephalopathy [5]. These publications are among the earliest studies to emphasize the significance of neuronal autoantibodies in aseptic encephalitis. After the discovery of antibody to N-methyl-D-aspartate receptor (NMDAR) in 2007 [6], there have been additional reports of immune-mediated encephalitis. The first case series of anti-NMDAR limbic encephalitis included 12 women with prominent psychiatric symptoms [6]. Ten of 20 encephalitis patients with unidentified etiologies in CEP (The California Encephalitis Project) were later found to have anti-NMDAR antibody [7]. These patients (6 females and 4 males) were young adults (mean age 18.5 year) who primarily presented with dyskinesia and psychiatric manifestations [7]. Subsequent CEP study (2007-2010) demonstrated that encephalitis associated with anti-NMDAR antibody (32 of 761) was nearly as common as viral causes (47 of 761) in patients less than 30 years of age [8]. Seizures, language and autonomic dysfunctions, movement disorder and psychoses were predominating clinical features in these patients [9].
A report from Malaysia [10] revealed that 8 of 16 adult encephalitis patients (14-29 years of age) and 2 children (both 9 years old) with dominant psychiatric features had anti-NMDAR antibody yet lacked evidence of underlying tumor. Autoantibody-associated encephalitis other than anti-NMDAR is now increasingly reported [7, 8]. These patients can present with a wide range of manifestations unrelated to solid tumors and are distributed across a wider age group. These reports have confirmed the incidence and severity of immune-mediated encephalitis in non-infectious cases of encephalitis.
We prospectively studied 103 Thai patients between 2 and 85 years of age, presenting with clinically non-bacterial, non-rickettsial, non-TB, non-fungal and non-parasitic encephalitis and/or myelitis with normal or lymphocytic CSF profile who were evaluated by the Neurology service of King Chulalongkorn Memorial Hospital (KCMH) between October 2010 and August 2012. Eleven pediatric patients aged one to fourteen years seen over the same period were included in this study.
Methods
Study design
This prospective study of patients with clinical evidence of encephalitis was conducted at KCMH, a tertiary referral hospital. Seventeen hospitals in Bangkok, Chonburi, Nakhonpatom and Ayutthaya provinces recruited patients. The study was approved by the KCMH ethics committee (reference number 015/2011). Informed consent was obtained from all patients in written form; when patients were impaired or underage, consent was obtained from a family member, parent or guardian. Only patients with clinical evidence of encephalitis and/or myelitis with or without peripheral nerve involvement were included. Patients with laboratory evidence of infectious encephalitis, e.g. viral, bacteria, mycobacterium tuberculosis (TB), parasite or rickettsia were excluded. Only patients who were normocellular or showed lymphocytosis with normal or slightly decreased glucose in CSF were enrolled. Patients with low CSF glucose and who had no evidence of viral, bacterial, TB, fungal, or parasitic infection and patients without evidence of malignant cells after cytocentrifugation were included. Magnetic resonance imaging (MRI) of the brain and/or spinal cord was performed within 48-72 hours of admission. In patients with unstable clinical conditions, computed tomography (CT) scan was performed instead of MRI.
Definition
Encephalitis was defined as a clinical syndrome comprising of headache, impaired cognitive function or consciousness, seizures or other focal deficits in the presence of an imaging study consistent with brain dysfunction. Myelitis was also included since it may be a sole manifestation or presenting feature subsequently followed by involvement of other structures. Myelitis was defined as fever and/or evidence of spinal cord dysfunction manifesting as sensori-motor deficits or pure motor deficit with or without sphincter involvement. Onset of the disease was defined as acute when neurological symptoms appeared at onset of any symptoms or within 7 days of a prodrome. They were subacute when appearing 8-30 days after prodrome and chronic if the interval was longer than 30 days.
All suspected cases of central nervous system infection with bacteria, fungi, parasites or mycobacteria were excluded as well as encephalopathy secondary to sepsis or systemic inflammatory response syndrome.
Investigations
Investigations included routine CBC, BUN, Cr, serum electrolytes, HIV antibody, chest X-Ray and liver function studies. Blood cultures were performed in all febrile case. Immunofluorescence assays for rickettsia were performed on serum when appropriate. All CSF was examined using cytology, glucose and protein levels, and cryptococcal antigen determination. PCR was used to evaluate CSF for herpes simplex virus (HSV) varicella zoster virus (VZV), Epstein Barr virus (EBV), cytomegalovirus (CMV), human herpes virus 6 (HHV-6) and enteroviruses. Patients with a history of animal bites and/or those with signs or symptoms suggesting rabies, had saliva, urine, CSF and extracted hair follicles tested for rabies viral RNA. Serologies for Japanese Encephalitis virus (JEV) and dengue virus were performed using IgM capture methods [11]. When indicated by MRI and by initial-negative serology studies, patients were evaluated for Nipah, Hendra and West Nile Virus (WNV) by PCR and paired acute and convalescent serology studies. MRI was performed for all cases unless the patient was unstable. MR studies were performed with a 3-T MR imager (Phillip MR systems Achieva Release 2.6.3.7) at Phyathai 2 Hospital and a 3-T Horizon MR imager (GE Medical systems) at KCMH. Contrast-enhanced studies were obtained using intravenous gadopentetate dimeglumine.
Detection of autoantibodies
Examination for autoantibodies was performed on archived serum of all patients admitted between October 2010 and June 2011 who presented with a negative work-up for infectious etiologies. Routine autoantibody testing was initiated in June 2011 after infection had been ruled out by laboratory studies and extended culture. Testing for autoantibodies was completed within 7-14 days. Twenty autoimmune and paraneoplastic neurological syndrome (PNS) related antibodies consisting of anti-NMDAR, anti-AMPA (2-amino-3-(5-methyl-3-oxo-1,2- oxazol-4-yl) propanoic acid)-1 and 2 receptor, anti-CASPR2 (contactin-associated protein 2), anti-LGI-1(Leucine-rich, glioma inactivated 1), anti-GABA (gamma-aminobutyric acid)-A and B receptor, anti-Hu (ANNA-1), anti-Ri (ANNA-2), anti-Yo (PCA-1), PCA-2, anti-Tr, anti-MAG, anti-myelin, anti-GAD, anti-CV2 (CRMP5), anti-ampiphysin, anti-neuroendothelium, anti-GFAP, anti-synaptophysin and AGNA/anti-SOX1 were determined by indirect immunofluorescence (IIF) assay in sera using EUROIMMUN® (Germany). Briefly, serum was diluted 10-fold and incubated on slides containing either individual antigens expressed in HEK cells or specific tissues (cerebellum, pancreas, intestine and nerve cell) followed by the second antibody conjugated with fluorescence isothiocyanate (FITC). Immunofluorescence was assessed using an inverted fluorescence microscope (Olympus®, model IX81). Assay for neuromyelitis optica (NMO) antibody was performed using standard IIF technique [12]. The diagnosis was confirmed using immunoblot analysis against five autoantibodies (antibodies against anti-amphiphysin, anti CV2, anti-Ri, anti-Yo and anti-Hu). Patient’s serum was diluted 1:100 and incubated with coated test strips followed by co-incubation of enzyme conjugate with alkaline phosphatase labeled anti-human IgG and substrate. The incubated test strips were evaluated using the EUROLineScan® software provided by the manufacturer.
Results
One-hundred eleven patients with encephalitis and/or myelitis were enrolled between October 2010 and August 2012. Sixty-six patients were admitted to KCMH and 45 represented referrals from 17 hospitals, primarily central Thailand. Eight patients were excluded after investigation showed alternative diagnoses (cerebral infarction, metabolic encephalopathy, cerebral venous thrombosis and subarachnoid hemorrhage). Of 103 patients, presentations included encephalitis (82,79.6%), myelitis (11,10.7%), encephalomyelitis (4,3.9%), meningoencephalitis (3,2.9%), encephalomyeloradiculitis (2, 1.9%) and myeloradiculitis (1,1%). Demographic data are summarized in Table 1.
Patients were categorized into infectious, immune-mediated and unidentified groups. There were 25 patients (24.3% of 103) in the infectious group; HSV-1 (6,24%), VZV (4,16%), JEV (3,12%), fungi (2,8%), mycobacterium tuberculosis (2,8%), EBV (2,8%), Clostridium tetani (2,8%), bacteria (1,4%), dengue (1,4%), rabies (1,4%), and dual infections with HSV-1 and dengue virus (1,4%). Four cases of TB (2) and fungi (2) were included in this study because they all had atypical presentations that we could not distinguish initially from other viral encephalitis cases. As for TB cases, one presented with acute onset of fever, headache and prominent behavioral changes resembling viral encephalitis. The other patient with TB presented with acute fever, drowsiness accompanied by hemiparesis shortly after onset which was not common in TB cases. None had abnormal chest X-Rays or meningeal enhancement particularly at basal cisterns on CT scan of the brain. The CSF white blood cell counts were 1,050 and 162 cells/mm3 respectively with predominant mononuclear cells and both had CSF protein <200 mg/dl with a sugar level of 12 and 40 mg/dl respectively. PCR for TB in CSF was positive in both cases. Two patients with fungal infections also had atypical manifestations. They presented with acute alterations of behavior in one case and brainstem encephalitis with cranial nerve palsies in another. CSF findings showed white blood cells of 9 and 327 cells/mm3, sugar levels of 52 and 33 mg/dl, protein levels of 106 and 61 mg/dl respectively. CSF India Ink preparations were negative.
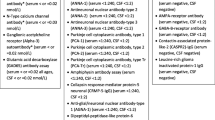
The immune-mediated group comprised of 25 cases (24.3% of 103) consisting of anti-Ri (ANNA2) (6,24%), anti-NMDAR (5,20%), neuropsychiatric lupus erythematosus (NPLE) (4,16%), demyelinating disease (3,12%), anti-Yo (PCA-1) (2,8%), neuro-Behcet’s disease (1,4%), anti-AMPAR (1,4%), anti-GABAR (1,4%), anti-VGKC (1,4%), and co-existence of anti-NMDAR with anti-Ri (1,4%). Three demyelinating cases were newly diagnosed with first attacks of multiple sclerosis or neuromyelitis optica. All presented with encephalitis syndrome. We could not differentiate them clinically from other viral or autoimmune causes.
Comparison of clinical course, neuroimaging studies and results of the workup for immune-mediated and unidentified etiologies are summarized in Table 2.
Clinical profiles, course and investigation of patients with immune-mediated causes
Onset of the disease was defined as acute in 17 cases (58%), subacute 4 cases (21%) and chronic in 4 cases (21%). Common prodromal symptoms included fever alone (7, 28%) and fever with associated symptoms (3, 12%). Time between prodrome and onset of neurological symptoms varied (Table 2). Psychosis was more notable in the immune group (6, 24%). Behavioral changes were evident in all groups and seizures were found less commonly in groups lacking a confirmed etiology (only 6%).
Although fever appeared at different time points within each groups, only half of the patients (13 of 25) in the infectious group reported fever as prodromal symptom. Interestingly, fever was also found to persist despite recovery of consciousness and respiratory function in two patients in the immune-mediated group (1 anti-NMDAR and 1 anti-Yo).
CSF pleocytosis was presnt in roughly half of the patients in immune and unidentified groups and up to 80% in the infectious etiology group (Tables 2 and 3). MRI of the brain was done in all but one patient: a young male with an unstable clinical condition; CT scan of the brain was performed in this unstable patient who had anti-NMDAR antibody and the study result was normal. Abnormalities confined to temporal lobe and hippocampus suggesting limbic encephalitis were noted in one case with anti-Yo and two cases with anti-Ri antibodies.
Table 3 summarized clinical characteristics, course of disease and results of investigations and outcome of 25 cases associated with autoimmune markers. An underlying tumor was found in 3 cases with antibodies to NMDAR (ovarian teratoma), anti-Yo (germ cell tumor) and ANNA-2 (ovarian cancer). However, another patient with anti-Yo encephalitis also had a high serum level of CA-125 despite a normal CT study of the abdomen. The clinical outcomes of immune-mediated CNS diseases varied from complete recovery in 1 case (treated with IVIG and concurrent corticosteroid), partial recovery in 10 (4 treated with immune-modulating therapy), and 12 cases who remained severely disabled (5 treated) and death in 2 cases (untreated). The following treatments were used in this series: corticosteroids were given to patients with NPLE (2), demyelinating disease (1), neuro-Behcet’s disease (1), and NMO (1); plasmapheresis was used to treat one NMDAR antibody-positive patient and IVIG with concurrent corticosteroids were used to treat 4 cases with anti-NMDAR (2) and anti-Yo (2).
Co-existence of anti-NMDAR and –Ri antibodies was found in one patient: an 18- year-old male who initially developed hemophagocytic syndrome after salmonella sepsis and was admitted to the ICU where he had seizures without focal neurological deficits. His CSF profiles were within normal limit and MRI demonstrated diffuse cerebral atrophy. The patient received intravenous antibiotics (cephalosporin) and improved over the next six weeks with partial minor disability. Result of anti-Ri and anti-NMDAR became available 3 weeks after his discharge and no immunotherapy was ever initiated. The relationship between salmonella septicemia and auto-antibodies may be coincidental. Interestingly, this case also demonstrated moderately severe cortical atrophy for his age.
Anti-Ri (ANNA2) antibody, directed against neuron oncological ventral antigens (NOVA-1 and NOVA-2) [13, 14], was the most common autoantibody identified in this study (24% of immune-mediated cases). These markers were previously reported in patients presenting with opsoclonus, cerebellar ataxia, limbic encephalitis, brainstem encephalitis, myelopathy and dementia [15–17], nearly all cases in our study presented with seizures, and underlying malignancy was found in one case (ovarian cancer).
Anti-Yo (PCA-1) targeted CDR2 [18] peptides that are involved in DNA transcription. The inflammatory process against this 52 kDa antigen mediated by CD8 cytotoxic T lymphocytes [18, 19] was identified in the cerebellum, brainstem, spinal cord and spinal nerve roots [20, 21]. Such patients usually presented with cerebellar ataxia and associated malignancies such as ovary, breast or small cell lung cancer [15, 16]. However, none of our patients presented with ataxia.
Anti-GABABR-antibody has been reported in patients with limbic encephalitis (LE) associated with small-cell lung cancer (SCLC). These patients usually present with intractable seizures [22]. This antibody has been demonstrated to target the B1 subunit extracellular domain of GABA receptor [23]. This syndrome most commonly presents with subacute onset among patients in their sixth decade of life. Our case presented at 70 years of age, and with behavioral changes and seizures.
AMPAR is a subtype of glutamate receptor implicated in excitatory neurotransmission of the brain. This receptor consists of 4 subunits, but only antibodies to GluR1 and GluR2 subunits are associated with limbic encephalitis in patients with thymoma, breast cancer and lung carcinoma[24]. Most of the cases previously reported with anti-AMPAR antibody were females over 50 years of age [25], however our single patient with anti-AMPAR was a 2-year-old girl who presented with stiff-person syndrome. Anti-GAD and anti-ampiphysin antibodies in this case were negative. However, we have not tested anti-glycine receptor antibody, which has also been reported in stiff person syndrome. It is also possible that anti-AMPAR antibody in this case could be associated with viral infection suggested by the history of antecedent skin rashes.
There are 2 main targets of autoantibodies to VGKC; one at LGI1 protein and another at CASPR2 [26]. Antibodies against VGKC complexes are rarely associated with malignancies [27]. CASPR2 is largely found at the juxtaparanodal region of myelin [28]. This may explain why circulating antibody of CASPR2 can be associated with neuromyotonia, for example, as part of Morvan’s disease [29]. However, one case with anti-CASPR2 in our series manifested with solitary encephalitis instead of peripheral nervous system symptoms.
Discussion
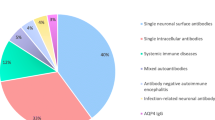
The results of our study confirm that autoantibody-associated encephalitis was as common as infectious encephalitis in our Thai cohort. These results are similar to the CEP result [8] and encephalitis studies from other regions [9, 10, 30]. However, in our study we found that this entity was not confined to young adults less than 18 years of age as previously reported [8]. The average ages of our patients with anti-NMDAR- and ANNA-2 antibodies were different; 39 and 67 years respectively. The presence of autoantibodies other than anti-NMDAR strongly support that the search for immune-mediated causes of encephalitis should not be limited to anti-NMDAR antibody alone.
Clinically, it is extremely difficult to distinguish between immune-mediated and infectious encephalitis. Immune mediated diseases such as NPLE, disease of white matter such as acute post-infectious encephalitis, NMO and neuro-Behcet’s disease should also be considered in patients with encephalomyelitis. This includes CNS vasculitis of both immune and infectious origin and mitochondrial encephalopathy, the latter of which can have MRI disturbances similar to herpes simplex encephalitis [30]. Furthermore, several autoantibodies, including those unrelated to malignancy, can be associated with this syndrome. We also could not exclude the presence of prior undetected viral, bacterial or parasitic infections that might actually have incited the aberrant immune response.
Immune-mediated encephalitis in our series was found in both sexes and in young and old patient alike (range 1-82 years of age). The majority of cases presented with an acute to subacute course. Fever was present in both immune and infectious cases of encephalitis. Psychosis was the single parameter more likely to be found in the immune mediated (24%) rather than infectious groups where there were none. Psychosis was found in 3 of 5 patients with antibody to NMDAR, 2 of 6 ANNA-2 and 1 of 4 NPLE. Seizures were found in both groups. Headache was slightly more prominent in the infectious group (20% versus 8%).
Although normocellular CSF (0-5 cells/mm3) can be found in 60% of immune cases (versus 20% of patients with infection), it should not be used as a solitary criteria for diagnosis because as many as 8 of 28 patients (29%) with PCR-confirmed HSV encephalitis had no CSF pleocytosis (Saraya, et al. manuscript in preparation).
Neuroimaging failed to aid in the diagnosis of immune encephalitis. Results varied and abnormalities were usually confined to the cortical and subcortical regions, whereas those associated with infection tended to involve midline and posterior fossa structures (data not shown). MRI presentation of limbic involvement, previously reported in association with antibodies against synaptic or neuronal surface proteins or intracellular antigens, was found in only 2 cases in this series.
An underlying tumor or malignancy was documented in only 3 patients. However, search for malignancy was not conducted in all cases since laboratory results were known after discharge and the patients were too disabled or the patient or families’ refused to participate in additional investigations.
Conclusion
The results from this study should encourage physicians to aggressively screen for immune causes of encephalitis in all patients with a negative work-up for infectious encephalitis. Efforts should be made to expedite identification of autoantibodies as soon as possible, as delays in treatment may allow patients to progress to coma and/or require intensive medical care including mechanical ventilation. Ventilator associated infection or other iatrogenic complications will likely be minimized if appropriate treatment is applied in a timely manner. The high prevalence and significant morbidity of autoimmune encephalitis (24% in our study and 21% in a recent study from England) coupled to the successful treatment experience using immune-modulating therapy, make the diagnosis of immune encephalitis a priority in all patients presenting with suspected non-infectious encephalitis.
References
Granerod J, Ambrose HE, Davies NW, Clewley JP, Walsh AL, Morgan D, Cunningham R, Zuckerman M, Mutton KJ, Solomon T, et al: Causes of encephalitis and differences in their clinical presentations in England: a multicentre, population-based prospective study. Lancet Infect Dis. 2010, 10: 835-844. 10.1016/S1473-3099(10)70222-X.
Fowler A, Stodberg T, Eriksson M, Wickstrom R: Childhood encephalitis in Sweden: etiology, clinical presentation and outcome. Eur J Paediatr Neurol. 2008, 12: 484-490. 10.1016/j.ejpn.2007.12.009.
Glaser CA, Gilliam S, Schnurr D, Forghani B, Honarmand S, Khetsuriani N, Fischer M, Cossen CK, Anderson LJ: In search of encephalitis etiologies: diagnostic challenges in the California Encephalitis Project, 1998-2000. Clin Infect Dis. 2003, 36: 731-742. 10.1086/367841.
Thieben MJ, Lennon VA, Boeve BF, Aksamit AJ, Keegan M, Vernino S: Potentially reversible autoimmune limbic encephalitis with neuronal potassium channel antibody. Neurology. 2004, 62: 1177-1182. 10.1212/01.WNL.0000122648.19196.02.
Vincent A, Buckley C, Schott JM, Baker I, Dewar BK, Detert N, Clover L, Parkinson A, Bien CG, Omer S, et al: Potassium channel antibody-associated encephalopathy: a potentially immunotherapy-responsive form of limbic encephalitis. Brain. 2004, 127: 701-712.
Dalmau J, Tuzun E, Wu HY, Masjuan J, Rossi JE, Voloschin A, Baehring JM, Shimazaki H, Koide R, King D, et al: Paraneoplastic anti-N-methyl-D-aspartate receptor encephalitis associated with ovarian teratoma. Ann Neurol. 2007, 61: 25-36. 10.1002/ana.21050.
Gable MS, Gavali S, Radner A, Tilley DH, Lee B, Dyner L, Collins A, Dengel A, Dalmau J, Glaser CA: Anti-NMDA receptor encephalitis: report of ten cases and comparison with viral encephalitis. Eur J Clin Microbiol Infect Dis. 2009, 28: 1421-1429. 10.1007/s10096-009-0799-0.
Gable MS, Sheriff H, Dalmau J, Tilley DH, Glaser CA: The frequency of autoimmune N-methyl-d-aspartate receptor encephalitis surpasses that of individual viral etiologies in young individuals enrolled in the california encephalitis project. Clin Infect Dis. 2012, 54: 899-904. 10.1093/cid/cir1038.
Titulaer MJ, McCracken L, Gabilondo I, Armangue T, Glaser C, Iizuka T, Honig LS, Benseler SM, Kawachi I, Martinez-Hernandez E, et al: Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study. Lancet Neurol. 2013, 12: 157-165. 10.1016/S1474-4422(12)70310-1.
Abdullah S, Lim S-Y, Goh KJ, Lum LC, Tan CT: Anti-N-methyl-D-aspartate receptor (NMDAR) encephalitis: A series of ten cases from a university hospital in Malaysia. Neurol Asia. 2011, 16: 241-246.
Innis BL, Nisalak A, Nimmannitya S, Kusalerdchariya S, Chongswasdi V, Suntayakorn S, Puttisri P, Hoke CH: An enzyme-linked immunosorbent assay to characterize dengue infections where dengue and Japanese encephalitis co-circulate. Am J Trop Med Hyg. 1989, 40: 418-427.
Jarius S, Probst C, Borowski K, Franciotta D, Wildemann B, Stoecker W, Wandinger KP: Standardized method for the detection of antibodies to aquaporin-4 based on a highly sensitive immunofluorescence assay employing recombinant target antigen. J Neurol Sci. 2010, 291: 52-56. 10.1016/j.jns.2010.01.002.
Yang YY, Yin GL, Darnell RB: The neuronal RNA-binding protein Nova-2 is implicated as the autoantigen targeted in POMA patients with dementia. Proc Natl Acad Sci USA. 1998, 95: 13254-13259. 10.1073/pnas.95.22.13254.
Ueki K, Ramaswamy S, Billings SJ, Mohrenweiser HW, Louis DN: ANOVA, a putative astrocytic RNA-binding protein gene that maps to chromosome 19q13.3. Neurogenetics. 1997, 1: 31-36. 10.1007/s100480050005.
McKeon A, Pittock SJ: Paraneoplastic encephalomyelopathies: pathology and mechanisms. Acta Neuropathol. 2011, 122: 381-400. 10.1007/s00401-011-0876-1.
Didelot A, Honnorat J: Update on paraneoplastic neurological syndromes. Curr Opin Oncol. 2009, 21: 566-572. 10.1097/CCO.0b013e3283306647.
Darnell RB: Onconeural antigens and the paraneoplastic neurologic disorders: at the intersection of cancer, immunity, and the brain. Proc Natl Acad Sci USA. 1996, 93: 4529-4536. 10.1073/pnas.93.10.4529.
Corradi JP, Yang C, Darnell JC, Dalmau J, Darnell RB: A post-transcriptional regulatory mechanism restricts expression of the paraneoplastic cerebellar degeneration antigen cdr2 to immune privileged tissues. J Neurosci. 1997, 17: 1406-1415.
Okano HJ, Park WY, Corradi JP, Darnell RB: The cytoplasmic Purkinje onconeural antigen cdr2 down-regulates c-Myc function: implications for neuronal and tumor cell survival. Genes Dev. 1999, 13: 2087-2097. 10.1101/gad.13.16.2087.
Storstein A, Krossnes BK, Vedeler CA: Morphological and immunohistochemical characterization of paraneoplastic cerebellar degeneration associated with Yo antibodies. Acta Neurol Scand. 2009, 120: 64-67. 10.1111/j.1600-0404.2008.01138.x.
McKeon A, Tracy JA, Pittock SJ, Parisi JE, Klein CJ, Lennon VA: Purkinje cell cytoplasmic autoantibody type 1 accompaniments: the cerebellum and beyond. Arch Neurol. 2011, 68: 1282-1289. 10.1001/archneurol.2011.128.
Lancaster E, Lai M, Peng X, Hughes E, Constantinescu R, Raizer J, Friedman D, Skeen MB, Grisold W, Kimura A, et al: Antibodies to the GABA(B) receptor in limbic encephalitis with seizures: case series and characterisation of the antigen. Lancet Neurol. 2010, 9: 67-76. 10.1016/S1474-4422(09)70324-2.
Huang ZJ: GABAB receptor isoforms caught in action at the scene. Neuron. 2006, 50: 521-524. 10.1016/j.neuron.2006.05.005.
Traynelis SF, Wollmuth LP, McBain CJ, Menniti FS, Vance KM, Ogden KK, Hansen KB, Yuan H, Myers SJ, Dingledine R: Glutamate receptor ion channels: structure, regulation, and function. Pharmacol Rev. 2010, 62: 405-496. 10.1124/pr.109.002451.
Lai M, Hughes EG, Peng X, Zhou L, Gleichman AJ, Shu H, Mata S, Kremens D, Vitaliani R, Geschwind MD, et al: AMPA receptor antibodies in limbic encephalitis alter synaptic receptor location. Ann Neurol. 2009, 65: 424-434. 10.1002/ana.21589.
Ogawa Y, Oses-Prieto J, Kim MY, Horresh I, Peles E, Burlingame AL, Trimmer JS, Meijer D, Rasband MN: ADAM22, a Kv1 channel-interacting protein, recruits membrane-associated guanylate kinases to juxtaparanodes of myelinated axons. J Neurosci. 2010, 30: 1038-1048. 10.1523/JNEUROSCI.4661-09.2010.
Tan KM, Lennon VA, Klein CJ, Boeve BF, Pittock SJ: Clinical spectrum of voltage-gated potassium channel autoimmunity. Neurology. 2008, 70: 1883-1890. 10.1212/01.wnl.0000312275.04260.a0.
Poliak S, Gollan L, Salomon D, Berglund EO, Ohara R, Ranscht B, Peles E: Localization of Caspr2 in myelinated nerves depends on axon-glia interactions and the generation of barriers along the axon. J Neurosci. 2001, 21: 7568-7575.
Hart IK, Maddison P, Newsom-Davis J, Vincent A, Mills KR: Phenotypic variants of autoimmune peripheral nerve hyperexcitability. Brain. 2002, 125: 1887-1895. 10.1093/brain/awf178.
Sureka J, Jakkani RK: Clinico-radiological spectrum of bilateral temporal lobe hyperintensity: a retrospective review. Br J Radiol. 2012, 85 (1017): e782-e792. 10.1259/bjr/30039090. doi:10.1259/bjr/30039090. Epub 2012 Mar 14
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2377/13/150/prepub
Acknowledgement
This work was part of the encephalitis project in Thailand supported by grants from a Broad Agency Agreement with the Naval Health Research Center under Cooperative Agreement Number W911NF-11-2-0041 Advanced Diagnostic Imaging Center (AIMC) and Thai Brain Mapping Project, Faculty of Medicine Ramathibodi Hospital, Mahidol University and sponsored by the Defense Advanced Research Projects Agency (DARPA) Prophecy Program, and by the Higher Education Research Promotion and National Research University Project of Thailand, Office of the Higher Education Commission HR1160A and Thai government fund. The views and conclusions contained in this document are those of the authors and should not be interpreted as representing the official policies, either expressed or implied, of the Army Research Laboratory, DARPA or other branches of the U.S. Government. The U.S. Government is authorized to reproduce and distribute reprints for Government purposes notwithstanding any copyright notation herein.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
TH and SW participated in design. AS and TH participated in adult patient management. TD participated in pediatric patient management. AM and NS performed the IF laboratory assay. AS and AM participated in data collection, interpretation of the data and prepared the manuscript. TH, SS, NS, MC participated in interpretation of the data and prepared and reviewed the manuscript to final version. HW and MC contributed to and edited the manuscript. All authors read and approved the final manuscript.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an open access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Saraya, A., Mahavihakanont, A., Shuangshoti, S. et al. Autoimmune causes of encephalitis syndrome in Thailand: prospective study of 103 patients. BMC Neurol 13, 150 (2013). https://doi.org/10.1186/1471-2377-13-150
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2377-13-150