
Abstract
Background
The short-term cholesterol-lowering efficacy of plant stanol esters has been open to debate, and the data from different clinical studies with hypercholesterolemic subjects are variable, partly due to lack of systematic studies. Therefore, we investigated the time in days needed to obtain the full cholesterol-lowering effect of stanol esters in hypercholesterolemic subjects.
Methods
Eleven mildly to moderately hypercholesterolemic subjects consumed stanol ester margarine (2.0 g/day of stanols) as a part of their habitual diet for 14 days and the changes in serum lipid values were measured three times at 4, 8 and 15 days after the initiation of test margarine consumption (0 day). The returning of serum lipid concentrations to baseline was measured two times after 2 or 3 days and after 7 days of the end of the test margarine consumption.
Results
Serum LDL cholesterol concentrations were reduced from 0 day (4.51 ± 0.66 mmol/l) by 3.5% (P = ns), 9.9% (p < 0.05) and 10.2% (P < 0.05) at 4, 8 and 15 days, respectively. Serum campesterol/total cholesterol ratio, an indirect marker of intestinal cholesterol absorption, was significantly reduced on day 4 already. After ending the stanol ester use serum cholesterol concentrations began to return rapidly and after 7 days serum LDL cholesterol was 5.3% less than the initial value (P = ns).
Conclusion
The specific effect of plant stanol esters on serum LDL cholesterol can fully be obtained within 1–2 weeks of the use of plant stanol ester-enriched margarine.
Similar content being viewed by others


Background
Several clinical studies have shown that plant stanol esters are effective cholesterol-lowering agents [1, 2]. The cholesterol-lowering effect of dietary plant stanol ester has been shown to be sustained for periods up to 12 months [1], but how soon full cholesterol-lowering effect of plant stanol esters can be obtained, is still unclear. In most previous studies [3–5] the vast proportion of reduction in serum cholesterol has been reported to occur within 2–3 weeks, but the effects of plant stanol esters probably appear sooner than that. The results from two clinical studies with normo- or hypercholesterolemic subjects, where the cholesterol measurements have also been done at time point of one week, are conflicting: In one study [6], maximal cholesterol-lowering effect was obtained within a week of dietary plant stanol ester use, whereas in the other [7], no effect on serum cholesterol concentrations was obtained after one week of dietary plant stanol ester use. On the other hand, in a specific patient group, in colectomized patients [8], significant reduction in serum cholesterol was found already after one day of stanol ester use as measured by gas liquid chromatograph (GLC), but a steady state was reached just within one week. However, as far as we know, short-term cholesterol-lowering effects of plant stanol esters have not been studied at several repeated time points within short period of time in a real target group for use of stanol ester-enriched products, i.e. hypercholesterolemic subjects. Therefore, in the present study our aim was to find out the time needed to obtain the full cholesterol-lowering effect of plant stanol esters with a daily dose of 2.0 g stanols in healthy, hypercholesterolemic subjects.
Methods
Subjects
Altogether 11 mildly to moderately hypercholesterolemic (10 men and 1 women) subjects were recruited to the study from subjects participated the former studies carried out at the Department of Clinical Nutrition, University of Kuopio. The main inclusion criteria were as follows: serum total cholesterol 5.0–8.5 mmol/l and total triglycerides below 2.5 mmol/l at screening. Other inclusion criteria were aged 25–65 years, normal liver, kidney and thyroid function, no lipid-lowering medication, no coronary heart disease, no diabetes mellitus, no gastrointestinal diseases, no alcohol abuse (>45 g of ethanol/d) and no irregular eating habits. One subject used postmenopausal estrogen therapy, one used a betablocker for the treatment of hypertension and one used anti-thrombolytic medication. Two subjects were smokers. The subjects were requested to keep their medication, weight, alcohol consumption, smoking habits and physical activity constant during the study. All 11 subjects completed the study. Their mean age was 50.2 ± 8.8 y and mean body mass index (BMI) was 27.0 ± 2.8 kg/m2. Baseline (0 day) total, LDL, HDL and VLDL cholesterol and triglyceride concentrations are shown in Table 2.
The subjects gave their informed consent for the study and study protocol was approved by the Ethics Committee of the Kuopio University Hospital.
Study design
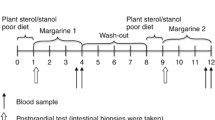
The study was carried out at the Department of Clinical Nutrition, University of Kuopio with the open and uncontrolled study design. The study lasted three weeks including six visits to the study unit. Subjects started the study in two batches so that one started a week later than the other batch. For 14 days the subjects consumed the test margarine daily and during this period the fasting blood samples were taken at the beginning of the experimental period (0 day) and at days 4, 8 and 15 (meaning 3, 7 and 14 days after the initiation of test margarine consumption, respectively). The returning of the serum lipid concentration was followed two times after 2 or 3 days (17 or 18 days) and after 7 days (22 days) from the end of the test spread consumption.
At the first visit of the study (0 day) routine laboratory measurements were taken to ensure normal health status. In addition, medical history, use of drugs and nutrient supplements, alcohol consumption, smoking habits and physical activity were interviewed using a structured questionnaire. The possible changes in dietary habits, health status and physical activity were asked to record in the follow-up diary during the trial. The possible adverse effects and symptoms were enquired based on a structured questionnaire at the end of the experimental period (15 days).
Diet
The subjects followed their habitual diet except replacing 25 g of their normal fat spread with rapeseed oil-based stanol ester margarine daily (Benecol-80®, Raisio Group Plc, Raisio, Finland). The fat content of test margarine was 72.5 %. Plant stanol esters were prepared from wood and vegetable sterols (DRT, Les Derives Resiniques & Terpeniques Granel S.A. Dax Cedex, France and Archer Daniels Midland Co, Decatur, IL, respectively) by recrystallization, hydrogenation to form plant stanols, and esterification with low-erucic acid rapeseed oil-based fatty acids to produce fatty acid esters of plant stanols. The margarine contained 8.0 weight-% total stanols including 6.1 weight-% sitostanol and 1.9 weight-% campestanol. Thus the targeted daily intake of total stanols based on the actual amount of stanols in test spread was 2.0 g (1.52 g sitostanol and 0.47 g campestanol).
The subjects received the tubs of test margarine when visiting the study unit. They were given detailed instructions on how to use the test spread. Furthermore, the subjects were asked to record the use of test spread daily and to return the empty and partly empty tubs and the extra tub of test spread to the study unit at the end of experimental period. The packages and the test spread left over were weighed and the result recorded.
The background diet of the subjects was monitored by seven-day food record (five weekdays and two weekend days) and nutrient intake was calculated from the records by using the Micro-Nutrica® dietary analysis program (version 2.0, Finnish Social Insurance Institute, Turku, Finland). The subjects kept the food record after the third study visit.
Laboratory measurements
All measurements were done and venous blood samples were obtained after 12-h overnight fast by using standardized methods. Body weight was measured with a digital scale.
Lipoproteins were separated by ultrasentrifugation for 18 h at density 1.006 to remove very low density lipoprotein (VLDL). HDL in the infranatant was separated from LDL by precipitation of LDL with dextran sulfate and magnesium chloride [9]. LDL cholesterol was calculated as the difference between the mass of cholesterol in the infranatant and HDL, and VLDL cholesterol was calculated as difference between the whole serum and the infranatant. Enzymatic photometric methods were used for the determination of cholesterol and triglycerides from whole serum and separated lipoproteins using commercial kits (Monotest® Cholesterol and Triglyceride GPO-PAP, Boehringer Mannheim GmbH Diagnostica, Mannheim, Germany) with a Kone Specific Clinical Analyser (Kone Ltd., Espoo, Finland). The coefficients of variation between measurements for serum total cholesterol were 1.4–1.7%, for triglycerides were 2.1–2.2%, for HDL cholesterol were 0.4–1.4% and for HDL triglycerides was 0.8%.
Serum cholesterol precursors, cholestanol and plant sterols were measured by GLC (HP 5890 Series II, Hewlett Packard, Delaware, Little Falls, USA) from nonsaponifiable serum material [10, 11] equipped with a 50-m long Ultra 1 capillary column (Methyl-polysiloxane) (Hewlett Packard, Delaware, Little Falls, USA) for cholestanol, desmosterol, squalene, 8Δ-cholestenol, 7Δ-lathosterol, campesterol and sitosterol, and equipped with a 50-m long Ultra 2 capillary column (5 % Phenyl-methyl siloxane) (Hewlett Packard, Delaware, Little Falls, USA) for sitostanol and campestanol. 5α-cholestanol for cholesterol and epi-coprostanol for cholesterol precursors, plant sterols and cholestanol were used as internal standards. Serum cholesterol precursors, cholestanol and plant sterols were determined twice and the mean value of two measurements was used in the statistical analysis. To eliminate the effects of the impact of changes in the amount of sterol transporting lipoprotein particles, values of above-mentioned variables are presented in terms of 10-2mg/mg of cholesterol (GLC), which express ratio to total cholesterol.
Plasma glucose was analyzed by enzymatic photometric method using reagent Granutest 100 (Merck, Damstadt, Germany) with a Kone Specific Clinical Analyser (Kone Ltd., Espoo, Finland).
Statistical analyses
All statistical analyses were performed with SPSS for windows 6.0.1 statistics program (SPSS, Chicago, IL, USA) [12]. The results are given as means ± SDs and in some cases also as range. Normal distribution of variables was checked with Shapiro Wilks test before the further analyses. If a variable was not normally distributed statistical analysis was made after logarithmic transformation. Simple factorial analysis of variance (ANOVA) was used to test whether there were differences in the initial measurements of each period (0 day and 15 days) between two starting batches. Analysis of variance for repeated measurements (MANOVA) was used to compare the overall changes in continuous variables among different dose periods. Two-tailed comparisons with paired t-test were used in the further analyses. For variables which were not normally distributed not even after logarithmic transformation Friedman Two-tailed ANOVA test or Wilcoxon matched-paired signed rank test or Mann-Whitney test was used. To control the overall level Bonferroni adjustment was used.
Results
Baseline Characteristics
During the experimental period BMI decreased <1%, from 27.0 ± 2.8 to 26.7 ± 2.7 kg/m2 (P < 0.01), whereas during the follow-up period BMI remained unchanged. Because the change of BMI was significant during the experimental period, the analyses of that period were made both with and without BMI as covariate. Medication, physical activity and smoking habits remained stable. No side effects were found during the experimental period.
Feasibility of the diet
The intake of nutrients of background diet during the experimental period are presented in Table 1. The mean daily consumption of margarine according to the weighed returned tubs was 25.4 ± 0.8 g (24.4–27.5 g). Thus the actual daily intake of stanol was 2.03 ± 0.06 g (1.54 ± 0.05 g sitostanol and 0.48 ± 0.02 g campestanol).
Serum lipids and lipoproteins
Serum lipid and lipoprotein concentrations are presented in Table 2.
No significant differences were found in the mean values of serum lipids and lipoproteins at 0 and 15 days between the two starting batches. Furthermore, though the first follow-up blood sample was taken from first batch the day before (17 day) than from the second batch (18 day), no significant differences were found in serum lipids and lipoprotein concentrations in the first follow-up sample between the two starting batches.
During the experimental period serum LDL cholesterol concentration decreased slightly already at 4 days, but the decrease was not significant until at 8 days (Table 2). In addition, no further decrease in serum LDL cholesterol concentration was found from the 8 to 15 days. At the time points 8 and 15 days the decrease of serum LDL cholesterol was significant even when the changes in BMI were taken into account in the analysis as covariate (P = 0.012–0.051). The reductions in serum total cholesterol paralleled the reductions in serum LDL cholesterol except at 15 days due to the significant increase of VLDL cholesterol. There were no significant changes in serum HDL cholesterol and triglyceride concentrations during the experimental period (Table 2).
During the follow-up period serum total and LDL cholesterol concentrations began to return immediately after termination of test spread consumption, but the changes were significant neither at 17/18 days nor at 22 days. At 22 days serum LDL cholesterol concentration was still 5.3 ± 10.0 % lower than the initial value (0 day).
Plant sterols and cholesterol precursors
The results of serum plant sterols, cholestanol and cholesterol precursors are shown in Table 3. There were significant differences in the mean values of serum sitosterol at the 0 and 15 days between the two starting batches, therefore the initial values were taken into account in the analyses as a covariate.
Serum plant sterols, and in particular serum campesterol/total cholesterol ratio, which reflects cholesterol absorption efficacy [13–15], reduced significantly already at 4 days (Table 3). In contrast, the ratios of serum campestanol and sitostanol to total cholesterol increased significantly during the experimental period and the significant increase was reached in 4 days. However, after termination of test spread consumption serum campestanol and sitostanol decreased rapidly and the reduction was significant already at 17/18 days. At 22 days serum campestanol/total cholesterol ratio had almost returned to baseline (P = 0.614), but sitostanol/total cholesterol ratio was slightly, but still significantly, greater than baseline (P = 0.033).
Serum 7Δ-lathosterol/total cholesterol ratio, which reflects cholesterol synthesis [13, 14, 16], increased during the experimental period and the increase was statistically significant at 15 days compared with the initial value (Table 3).
Discussion
The main results of the present study with hypercholesterolemic subjects were that the significant decrease in serum LDL cholesterol concentrations was achieved already after one week of the initiation of stanol ester margarine consumption, and that no additional cholesterol-lowering effect was obtained between the 8th and 15th days (-9.9% and -10.2%, respectively). Our findings agree with the findings of Mensink et al. [6] in which full cholesterol-lowering effect was reached within one week with stanol ester use. These results are also in line with the values of two weeks of our dose-response study, where serum LDL cholesterol was reduced significantly by 10.5%, 11.2%, 17.4% and 17.4% versus control with the daily stanol dose of 0.8 g, 1.6 g, 2.4 g and 3.2 g, respectively [17]. In contrast to the above findings, Jones et al. [7] did not find any effect on serum cholesterol concentrations after one week with stanol ester use. It can be speculated that some background factors, such as changes in diet, might have confounded their results. In fact, the actual composition of the diet has not been reported in that study. Our study can be criticized because of the lack of the control group. It is clear that the fatty acid modification contributes to the serum cholesterol reduction, but this takes place after a few week consumption. Therefore, the changes in serum cholesterol concentrations in the present study can be ascribed to plant stanol ester use despite the lack of the control group. Furthermore, these results can be ascribed to plant stanol ester use, since the compliance of subjects was good according to the follow-up diaries and weighted returned tubs. In addition, the changes in serum plant sterol and stanol concentrations reveal the good compliance. Moreover, our results are supported by results from the studies of Mensink et al. [6] and Miettinen et al.[8].
In a specific patient group, in colectomized patients [8], significant reduction in serum cholesterol concentrations was reported already after one day of stanol ester consumption. However, in the present study with hypercholesterolemic subjects we found non-significant reduction in serum cholesterol at 4 days. The different results could be explained by different cholesterol metabolism between the healthy subjects and colectomized patients. In colectomized patients transit time is very short, on an average 4–6 hours, and removal of cholesterol is slightly increased [18, 19]. Our result in noncolectomized hypercholesterolemic subjects is not unexpected, since under normal circumstances the half-life of disappearance of LDL apo B-100 from the circulation is about 2½ days, therefore serum LDL cholesterol concentration can be expected to decrease significantly only after some days of stanol ester use [20].
Serum VLDL cholesterol concentration was significantly higher at 15 days compared with the initial value. However, this finding was likely occasional and due to temporary increased alcohol consumption – about 2% higher than recorded in other studies – since plant stanols have generally not been reported to affect serum VLDL cholesterol [21–26].
Hypocholesterolemic effect of plant stanol esters is based on their ability to inhibit cholesterol absorption effectively from small intestine [27]. Serum campesterol/total cholesterol ratio has been found to be an indirect marker of cholesterol absorption [13–15]. In the present study, serum campesterol/total cholesterol ratio decreased significantly already within 4 days indicating that intestinal cholesterol absorption reduces rapidly after the initiation of the stanol ester consumption. This support the finding that cholesterol-lowering effect of stanol esters appears very soon after the initiation of their consumption. On the other hand, during the experimental period serum 7Δ-lathosterol/cholesterol ratio [13, 14, 16] increased significantly reflecting the enhanced endogenous cholesterol synthesis as a feedback reaction to the reduced cholesterol absorption. Also in previous studies the synthesis of Δ7-lathosterol has been found to be stimulated by plant stanol esters [22, 23, 28–31]. In fact, Relas et al. [32] suggested that effectively increased endogenous cholesterol synthesis was a reason for the inconsistent decrease in serum total and LDL cholesterol after 2 weeks with stanol ester use in their study.
Similar to recent stanol ester studies [3, 8, 26, 31, 33–35], in the present study sitostanol and campestanol from stanol ester margarine seemed to be absorbed to some extent. However, the rapid reduction in serum plant stanol concentration after termination of the test margarine consumption, indicates that biliary elimination of plant stanols is rapid and that they are not stored in the human body.
During the follow-up period the returning of serum cholesterol to the initial values began rapidly after termination of the consumption of plant stanol esters. However, after one week serum LDL cholesterol value was still 5% lower than the initial value indicating that full return to the initial values after use of the plant stanol ester enriched-margarine does not take place within one week. This finding supports the finding of previous studies [1, 3, 6] in which the returning to baseline has been found to occur after two to three weeks of the termination. Therefore, consumption of products enriched with stanol esters should be regular in order to receive sustainable cholesterol-lowering effect. In addition to that it should be taken into account that although clinically significant benefit can be reached already within one week with the plant stanol ester use, a steady state in serum cholesterol concentrations is usually attained within 3–4 weeks. Therefore, serum cholesterol values are reasonable to follow at least that time, especially if there is need to match cholesterol-lowering drug therapy with the use of dietary plant stanol esters.
Conclusions
In conclusion, effect of plant stanol esters on serum LDL cholesterol concentrations can fully be obtained within 1–2 weeks of the use of plant stanol ester-enriched margarine in hypercholesterolemic subjects.
References
Miettinen TA, Puska P, Gylling H, Vanhanen H, Vartiainen E: Reduction of serum cholesterol with sitostanol-ester margarine in a mildly hypercholesterolemic population. N Engl J Med. 1995, 333: 1308-1312. 10.1056/NEJM199511163332002.
Moghadasian MH, Frohlich JJ: Effects of dietary phytosterols on cholesterol metabolism and atherosclerosis: clinical and experimental evidence. Am J Med. 1999, 107: 588-594. 10.1016/S0002-9343(99)00285-5.
Nguyen TT, Dale LC, von Bergmann K, Croghan IT: Cholesterol-lowering effect of stanol ester in a US population of mildly hypercholesterolemic men and women: a randomized controlled trial. Mayo Clin Proc. 1999, 74: 1198-1206.
Hallikainen MA, Uusitupa MIJ: Effects of 2 low-fat stanol ester-containing margarines on serum cholesterol concentrations as part of a low-fat diet in hypercholesterolemic subjects. Am J Clin Nutr. 1999, 69: 403-410.
Williams CL, Bollella MC, Strobino BA, Boccia L, Campanaro L: Plant stanol ester and bran fiber in childhood: effects on lipids, stool weight and stool frequency in preschool children. J Am Coll Nutr. 1999, 18: 572-581.
Mensink RP, Ebbing S, Lindhout M, Plat J, van Heugten MM: Effects of plant stanol esters supplied in low-fat yoghurt on serum lipids and lipoproteins, non-cholesterol sterols and fat soluble antioxidant concentrations. Atherosclerosis. 2002, 160: 205-213. 10.1016/S0021-9150(01)00562-7.
Jones PJ, Raeini-Sarjaz M, Ntanios FY, Vanstone CA, Feng JY, Parsons WE: Modulation of plasma lipid levels and cholesterol kinetics by phytosterol versus phytostanol esters. J Lipid Res. 2000, 41: 697-705.
Miettinen TA, Vuoristo M, Nissinen M, Järvinen HJ, Gylling H: Serum, biliary, and fecal cholesterol and plant sterols in colectomized patients before and during consumption of stanol ester margarine. Am J Clin Nutr. 2000, 71: 1095-1102.
Penttilä IM, Voutilainen E, Laitinen O, Juutilainen P: Comparison of different analytical and precipitation methods for the direct estimation of high-density lipoprotein cholesterol. Scand J Clin Lab Invest. 1981, 41: 353-360.
Miettinen TA, Koivisto P: Non-cholesterol sterols and bile acid production in hypercholesterolaemic patients with ileal bypass. In: Bile acid and cholesterol in health and disease. Edited by: Paumgartner G, Stiehl A, Gerok W. 1983, Lancaster, MTP Press, 183-187.
Miettinen TA: Cholesterol metabolism during ketoconazole treatment in man. J Lipid Res. 1988, 29: 43-51.
Norusis MJ: SPSS for Windows Base System User's Guide. Release 6.0. Chicago IL SPSS. 1993
Miettinen TA, Tilvis RS, Kesäniemi YA: Serum plant sterols and cholesterol precursors reflect cholesterol absorption and synthesis in volunteers of a randomly selected male population. Am J Epidemiol. 1990, 131: 20-31.
Tilvis RS, Miettinen TA: Serum plant sterols and their relation to cholesterol absorption. Am J Clin Nutr. 1986, 43: 92-97.
Miettinen TA, Tilvis RS, Kesäniemi YA: Serum cholestanol and plant sterol levels in relation to cholesterol metabolism in middle-aged men. Metabolism. 1989, 38: 136-140.
Björkhem I, Miettinen T, Reihnér E, Ewerth S, Angelin B, Einarsson K: Correlation between serum levels of some cholesterol precursors and activity of HMG-CoA reductase in human liver. J Lipid Res. 1987, 28: 1137-1143.
Hallikainen M, Uusitupa M, Sarkkinen E, Wester I: Short term cholesterol-lowering efficacy of plant stanol esters. Experimental Biology 2002 congress. New Orleans, Lousiana. April 20–24, 2002. FASEB Journal. 2002, 16: A609-
Luukkonen P: Restoperative proctocolectomy for ulcerative colitis. Second Department of Surgery, Helsinki University Central Hospital. Helsinki, University of Helsinki,. 1989
Fozio VW: Ulcerative colitis. Surgical management. In: Bockus Gastroenterogy. Edited by: Haubrich SW, Schaffner F. 1995, Philadelphia, Saunders, 1382-1393. 2
Malloy MJ: Disorders of lipoprotein metabolism. In: Basic and clinical endocrinology. Edited by: Greenspan FS, Gardner DG. 2001, New York, Lange Medical Books/McGraw-Hill, 716-744.
Blomqvist SM, Jauhiainen M, van Tol A, Hyvönen M, Torstila I, Vanhanen HT, Miettinen TA, Ehnholm C: Effect of sitostanol ester on composition and size distribution of low- and high-density lipoprotein. Nutr Metab Cardiovasc Dis. 1993, 3: 158-164.
Gylling H, Siimes M, Miettinen TA: Sitostanol ester margarine in dietary treatment of children with familial hypercholesterolemia. J Lipid Res. 1995, 36: 1807-1812.
Gylling H, Radhakrishnan R, Miettinen TA: Reduction of serum cholesterol in postmenopausal women with previous myocardial infarction and cholesterol malabsorption induced by dietary sitostanol ester margarine. Women and dietary sitostanol. Circulation. 1997, 96: 4226-4231.
Andersson A, Karlström B, Mohsen R, Vessby B: Cholesterol-lowering effects of a stanol ester-containing low-fat margarine used in conjunction with a strict lipid-lowering diet. Eur Heart J Supplements. 1999, 1 (Suppl S): S80-S90.
Miettinen TA, Vanhanen HT: Dietary sitostanol related to absorption, synthesis and serum level of cholesterol in different apolipoprotein E phenotypes. Atherosclerosis. 1994, 105: 217-226.
Hallikainen MA, Sarkkinen ES, Gylling H, Erkkilä AT, Uusitupa MI: Comparison of the effects of plant sterol ester and plant stanol ester-enriched margarines in lowering serum cholesterol concentrations in hypercholesterolaemic subjects on a low-fat diet. Eur J Clin Nutr. 2000, 54: 715-725. 10.1038/sj.ejcn.1601083.
Ling WH, Jones PJH: Dietary phytosterols: a review of metabolism, benefits and side effects. Life Sci. 1995, 57: 195-206. 10.1016/0024-3205(95)00263-6.
Vanhanen HT, Blomqvist S, Ehnholm C, Hyvönen M, Jauhiainen M, Torstila I, Miettinen TA: Serum cholesterol, cholesterol precursors, and plant sterols in hypercholesterolemic subjects with different apoE phenotypes during dietary sitostanol ester treatment. J Lipid Res. 1993, 34: 1535-1544.
Gylling H, Miettinen TA: Serum cholesterol and cholesterol and lipoprotein metabolism in hypercholesterolaemic NIDDM patients before and during sitostanol ester-margarine treatment. Diabetologia. 1994, 37: 773-780. 10.1007/s001250050178.
Gylling H, Miettinen TA: Effects of inhibiting cholesterol absorption and synthesis on cholesterol and lipoprotein metabolism in hypercholesterolemic non-insulin-dependent diabetic men. J Lipid Res. 1996, 37: 1776-1785.
Gylling H, Puska P, Vartiainen E, Miettinen TA: Serum sterols during stanol ester feeding in a mildly hypercholesterolemic population. J Lipid Res. 1999, 40: 593-600.
Relas H, Gylling H, Miettinen TA: Effect of stanol ester on postabsorptive squalene and retinyl palmitate. Metabolism. 2000, 49: 473-478.
Tammi A, Rönnemaa T, Gylling H, Rask-Nissilä L, Viikari J, Tuominen J, Pulkki K, Simell O: Plant stanol ester margarine lowers serum total and low-density lipoprotein cholesterol concentrations of healthy children: the STRIP project. Special Turku Coronary Risk Factors Intervention Project. J Pediatr. 2000, 136: 503-510.
Gylling H, Miettinen T: Cholesterol reduction by different plant stanol mixtures and with variable fat intake. Metabolism. 1999, 48: 575-580.
Hallikainen MA, Sarkkinen ES, Uusitupa MIJ: Plant stanol esters affect serum cholesterol concentrations of hypercholesterolemic men and women in a dose-dependent manner. J Nutr. 2000, 130: 767-776.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2261/2/14/prepub
Acknowledgements
The authors will thank Niina Tapola, M.Sc., for nutritional counselling.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The study was granted by Raisio Benecol Ltd., Finland.
Authors' contributions
MH was responsible for the study design, gave nutrition counselling, analyzed and interpreted the data and wrote the manuscript. ES and MU contributed to the planning of study design and diet, interpreting the data and writing the manuscript. IW contributed to the planning of study design and diet, interpreting the data and reviewing the manuscript. All authors read and approved the final manuscript.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Hallikainen, M., Sarkkinen, E., Wester, I. et al. Short-term LDL cholesterol-lowering efficacy of plant stanol esters. BMC Cardiovasc Disord 2, 14 (2002). https://doi.org/10.1186/1471-2261-2-14
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2261-2-14