
Abstract
Background
Osteoarthritis is the most common joint damage that leads to cartilage destruction, pain, and disability. The aim of this study is to investigate the effects of resistance exercises and Nano curcumin supplementation on synovial levels of collagenase-2 and NO in patients with knee osteoarthritis.
Methods
Forty women with primary knee osteoarthritis were divided into four groups including control, exercise, supplementation, and supplementation /exercises. The resistance exercise group performed exercises in 16 weeks (three sessions per week). The supplement group consumed one Nano curcumin capsule (1000 mg) per day for 16 weeks. Exercise and supplementation group also performed resistance exercises along with consuming Nano curcumin. Synovial fluid samplings were done in two stages of pre-test (24 h before training and supplementation) and post-test (48 h after the last session of treatment and supplementation). The obtained synovial fluid was used to measure the synovial level of collagenase -II and nitric oxide.
Results
Although, there were not any significant correlations between resistance exercise, nanocurcumum supplementation, and synovial levels of collagenase-2 and NO among women with knee osteoarthritis, we observed interesting reduced levels of both markers following the supplementation.
Conclusions
It can be concluded that the Nano curcumin supplementation can be an effective method to reduce the levels of these inflammatory factors in synovial fluids of cases with knee Osteoarthritis. Longer duration of the protocol may have more promoting results.
Trial registration
The project was registered at Iranian Registry of Clinical Trials (Trial registration number: IRCT20161208031300N1).
Similar content being viewed by others


Background
Osteoarthritis (OA) is a slow and progressive disorder of joints and cartilage [1]. OA is the most common musculoskeletal disorder and causes social and economic disabilities in the elderly population [2]. Various risk factors are associated with OA including age, obesity, occupation, gender (women are more susceptible than men), inheritance, metabolic diseases, knee trauma, and inertia [3,4,5]. The most common symptoms of OA are pain, morning stiffness, mobility limitation of joint, bone and soft tissue sensitivity, swelling, and clicking or cracking sound during joint bending and effusion. Early diagnosis plays a key role in effective treatment and OA management [6, 7]. Collagen fiber is the major collagen of the cartilage [8]. Therefore, the loss of collagen type II leads to loss of cartilage tensile properties [9]. Collagenase-2 is synthesized by connective tissue and is involved in subchondral bone synthesis (type I collagen) and cartilage (type II collagen) [10]. Moreover, increased levels of collagenase-2 have also been observed in synovial fluid during inflammation. It is inhibited by serum proteins and possess pivotal role in cartilage regeneration. Besides, collagenase-2 is secreted by neutrophils through interleukins which results in extracellular matrix (ECM) degradation [11]. Collagenases are released as pro-enzymes and activated outside the cell. It has been shown that the MMP-1, MMP-8 (collagenase-2), and MMP-13 initiate denaturation of fibrillar collagens which results in articular cartilage degradation during OA. Nitric oxide (NO) is a pro-inflammatory factor produced by conversion of L-arginine to L-citrulline [12, 13]. Articular chondrocytes and macrophages might be the main sources of intra-articular NO [12]. It is noteworthy that the NO is contributed in development of cartilage and cartilage matrix synthesis [14, 15]. Inducible NO synthase (iNOS) is the main enzyme involved in NO generation in OA patients [13, 16]. NO causes some damaging events such as apoptosis induction in the cartilage which results in extracellular matrix degradation through preventing proteoglycan secretion from chondrocytes. Several studies have shown that the regular exercise besides medication can be more efficient in attenuation of osteoarthritis symptoms [12, 16]. Resistance exercise has been exerted as the foremost effective exercise which has an efficient impact on attenuation of osteoarthritis complications [17]. Physical activities in the articular cartilage can stimulate lubrication and prevent the contraction of cartilage and prevent the progression of osteoarthritis [18]. Exercise diminishes the destructive effects of aging on musculoskeletal system through improvement of functional capacity, self-efficacy, emotional well-being, and weight control [19]. Besides exercises, medicinal plants supplements may also be effective in improving osteoarthritis. Curcumin is a yellowish pigment that is isolated from Curcuma longa (Turmeric) rhizomes. Curcumin has protective effects on various diseases such as osteoarthritis. It is widely accepted that the curcumin possess efficient antioxidant, anti-inflammation, and anti-cancer properties [20]. Curcumin is effective in maintaining articular flexibility, preserving joints function, and improving the pain in OA patients. It accounts as a potent alternative of non-steroidal anti-inflammatory drugs for cartilage regeneration and articular pain relief [21]. Since, curcumin is sparingly soluble in water and possesses poor gastrointestinal absorption, Nano formulation of curcumin has been approved to increase its cellular uptake, circulation time, and retention [22,23,24]. Considering the role of physical activity and herbal supplements in prevention of OA progression, we aimed to investigate the impact of resistance exercises besides Nano-curcumin supplementation on synovial collagenase-II and nitric oxide levels in patients with knee OA.
Methods
Study design and samples
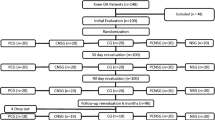
The present study was a semi-experimental and double-blind clinical trial. Forty women who referred to Imam Ali hospital in Bojnourd (Iran) were enrolled in present study. Patients were women aged 50–65 years, at grade 2 to 4 of osteoarthritis with low regular physical activity. The cases with nanocurcumin (turmeric) allergy, smoking, lower extremities fractures, use of analgesics, endocrine and metabolic diseases, cardiovascular disease, mental illness, epilepsy, anemia, and cancer were excluded from the study. All the cases have completed informed consent forms which were approved by the ethic committee. The participants were categorized in four groups of interventions including exercise and supplementation, exercise and placebo, supplementation, and control. The height, weight, and body mass index were measured. Localized questionnaire for pain measurements such as WOMAC index and VAS were also filled for each subject before intervention initiation and at the end of study.
Randomization and allocation
The participants were randomly allocated into supplementation, resistance exercise, supplementation plus resistance exercise, and control groups using a block randomization method. Sequentially numbered, opaque sealed envelopes (SNOSE) method was used to conceal the random sequence [25]. The participants and research assistants were blinded to group allocation. SNOSE were also kept by an independent researcher not involved in evaluation of participants or data analysis. The envelopes were opened following the baseline assessment of participants.
Resistance exercises and Nano curcumin supplementation
The resistance exercise group performed exercises in 16 weeks (three sessions per week). Each exercise session included warming for 10 min with a fixed-gear bicycle prior the main resistance exercise program. The subjects of each group performed knee and thigh resistance exercises including knee extension, pelvic abduction, and plantar flexion in three sets with an intensity of 50–75% 1RM for 3 days per week for 16 weeks [26]. Afterwards the cooling was performed for 5 to 10 min. The 1RM values of different movements were measured every 2 weeks, based on which the intensity of the exercises increased. The supplement group consumed one Nano curcumin capsule (1000 mg) per day for 16 weeks. Participants of control group also received one daily soft gelatin capsule as placebo to attenuate the psychiatric effects of supplementation.
Sampling and enzyme-linked immunosorbent assay (ELISA)
Synovial fluid samples were obtained 24 h prior to exercises and supplement use and 48 h after exercises and supplementation. The volume of aspirated synovial fluid samples was different according to disease grade and progression. The samples transferred to the laboratory and kept at − 70 °C. Collagenase II and nitric oxide levels of the synovial fluid were measured using human-specific ELISA kit (collagenase II, Zelbio, Germany and nitric oxide, Sib-zist, Iran) according to the manufactures protocol.
Nitric oxide assay
Nitric Oxide (NO) is extremely unstable and undergoes rapid oxidative degradation to stable nitrite (NO2-) and nitrate (NO3-), which react with the colorant and produce azo-pink composition and is quantified spectrophotometrically [27]. Serum levels of metabolites were measured by colorimetric Griess assay. During the colorimetric assay, the nitrite concentration was determined by measuring the absorbance at 450 nm.
Statistical analysis
Shapirowilk statistical test was used to evaluate the distribution of data. One-way analysis of variance and Bonferroni post hoc were used for the data with normal distribution (P ≤ 0.05). Leven test was used to compare the intra-group variables from the correlated t-test for normal variables. Wilcoxon test was also used for abnormal variables. Bonferron’s post hoc test was also used for paired comparison.
Results
Descriptive results of the research variables are presented in three sections: anthropometric characteristics, health status, and blood variables. The findings included mean values and standard deviations of variables. The anthropometric characteristics are presented in Table 1. The t-test and one-way ANOVA demonstrated that there were not any significant correlation between resistance exercise, supplement intake, exercise/supplementation, and synovial collagenase II levels (Table 2). However, we interestingly observed that the synovial collagenase II levels were decreased 4.67% in supplemented group (0.102 ± 0.019 vs. 0.107 ± 0.053, ng/ml). Whereas the supplementation/ exercise neutralizes the inhibitory role of supplementation and notably increased (7.55%) the levels of collagenase II among the cases (0.114 ± 0.048 vs. 0.106 ± 0.020, ng/ml) (Table 3). Regarding the NO, our data showed that there were not also any significant correlation between resistance exercise, supplement intake, exercise/supplementation, and synovial levels of nitric oxide (Table 4). However, we also observed that the supplementation interestingly reduced (26.67%) the NO synovial levels (0.11 ± 0.026 vs. 0.15 ± 0.074, ng/ml). In contrast with the collagenase II which was increased in supplementation/ exercise, the NO levels was notably decreased (13.3%) following the exercise and supplementation (0.10 ± 0.019 vs. 0.12 ± 0.03, ng/ml). Although the NO synovial levels were reduced following the exercise/supplementation, the exercise also neutralized the inhibitory role of supplementation from 26.67 to 13.3%. In the case of exercise without supplementation we also observed that the levels of collagenase II and NO were increased in post-test groups (Table 3). Moreover, we observed that the participant’s health and satisfaction were significantly increased following the supplementation and supplementation/exercises (p < 0.05).
Discussion
Pain and disability are common complications in patients with osteoarthritis which lead to various physical limitations [28]. Considering the fact that one of the goals of osteoarthritis treatment is to minimize pain and disability and improve the function in patients [29], the present study assessed the probable effect of resistance exercise and nano-curcumin supplementation on synovial levels of collagenase -II and nitric oxide in patients with knee osteoarthritis. It has been reported that the fixed-gear bicycle exercises in water decrease knee pain and swelling and increase aerobic capacity, respectively in knee osteoarthritis patients [30]. The exercise with sodium diclofenac has been reported to significantly reduce synovial TNF-α, hs-CRP, and MMP- 3 levels in osteoarthritis patients with knee [31]. The results of present study revealed that there were not any significant differences in synovial levels of collagenase-II and NO between four groups. However, it was shown that the supplementation notably reduced the synovial levels of collagenase II and NO among cases. The pain assessment of patients with VAS pain score and WOMAC index also showed that the resistance exercises and supplementation with nano-curcumin significantly decreased pain and stiffness of joints. Moreover, patient satisfaction confirmed the efficiency of our therapeutic method to improve and manage knee osteoarthritis complications. According to our results, it seems that the most effective state will be observed after supplementation without resistance exercises. It has been reported that the 12-week exercise protocol significantly decreased the IL-6 inflammatory marker [31]. Another group showed that the regular and moderate physical activity (cycling in 70% VO2max), significantly increased NO production in elderly women which was not in line with the present study [32]. The participants of the abovementioned study were normal and healthy woman but in the present study the participants were women with osteoarthritis. Type of exercise program, intensity, duration and number of sessions were different with the present study. Moreover, they assessed serum levels, whereas we evaluated the synovial levels of NO. The evaluation of synovial levels can be strength point of our study, because the factors involved in OA, firstly increase or decrease in synovial fluid and after that in plasma. NO is mainly produced by the chondrocytes through stimulating inflammatory cytokines [33]. Cartilage also produces NO in osteoarthritis condition [34]. In the present study in spite of insignificant decrease in inflammatory markers, pain attenuation was considered as a result of decreased levels of inflammatory factors. It has been showed that the curcumin and diclofenac intake decreased pain and improved quality of daily life [35]. Non-steroidal anti-inflammatory drugs (NSAIDs) are one of the commonly used medications for treatment of knee osteoarthritis which play analgesic and anti-inflammatory roles by inhibiting the synthesis of prostaglandin with COX-1 and COX-2 isoenzymes. However, the main side effect of NSAIDs is that their long-term use affects the kidneys, liver, and digestive system. In contrast, curcumin as an herbal compound has not any noticeable side effect and attenuates anti-inflammatory activity by regulation of NF-κB, TNF-α, IL-1, IL-8, and NO. These cytokines could have negative effects on knee in patient with OA. Another group has also observed that the Flexofitol (biocompatible curcumin) intake (two capsules per day) for 3 months also significantly reduced Coll-2-1 and CRP [36]. Their results are not in line with the present investigation of nano-curcumin effects on collagenase-II levels. The difference in the results can be related to the differences in disease severity, supplementation dosage, intake duration, or chemical composition of the abovementioned supplementation with nano-curcumim. It has been shown that the rat chondrocytes induction with IL-1β resulted in increased and decreased levels of MMP-3 and collagen II, respectively. Subsequently, treatment of the induced chondrocytes by curcumin decreased MMP-3 levels and increased collagen-2 levels [37]. The results of the present study are not consistent with the aforementioned study which can be associated with type of subjects (animal sample), intake duration, and curcumin dose.. It has also been observed that the oral and injectable curcumin methods significantly reduced NO concentration in mice [38]. Anti-inflammatory and anti-oxidant potentials are the most important biological effects of curcuminoid compounds. Curcuminoids can effectively decline the levels of inflammatory cytokines such as TNF-α, IL-1β, IL-6, and prostaglandin E2. Curcuminoids aggregate in ECM and prevent cartilage damage. They improve the chondrocytes survival by apoptosis inhibition. They are strong antioxidants that regulate oxidative stress through various mechanisms. Moreover, they are able to decline the free radicals’ production through COX-II and induce nitric oxide synthase. All of these properties might be efficient for improving joint health and pain relief by curcuminoid supplementation [39]. There were several limitations in present study such as; the rate and type of physical activities of participants, lack of knee synovial fluid during aspiration, knee joint movement restriction, and disability in doing exercises. Therefore, it is recommended to change the type, length, and intensity of resistance exercise programs, and intervals between training sessions and use of combined exercises and supplementation with nano-curcumin. Considering the positive effects of regular physical activities, herbal medicine, and medical treatment on pain reduction and improving the quality of life, the co-ordination of specialists in these three groups is useful and necessary for optimal treatment of these patients.
Conclusions
The present study suggested that the resistance exercises for 16 weeks with nanocurcumin supplementation had not any significant effect on synovial fluid levels of selected biomarkers in healthy menopause women.. Moreover, Nano curcumin supplementation or resistance exercise/supplementation effectively attenuated the pain and stiffness of joints in osteoarthritis patients and improved their quality of life. Therefore, curcumin supplementation can be used as an efficient herbal therapy without side effects in knee osteoarthritis management.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ECM:
-
Extracellular matrix
- iNOS:
-
Inducible NO synthase
- NO:
-
Nitric oxide
- NSAIDs:
-
Non-steroidal anti-inflammatory drugs
- OA:
-
Osteoarthritis
References
Casper Denise LDL, G.L., Foucault Anthony, Husser Stephen, Husser Joseph (2005), Harrison Rhymathology internal medicine book. Translators: Masood Khodaee, Ali Khalat. Editing 19. Arjmand Publishing 384 pages.
Jeong H, et al. Comorbidities and health-related quality of life in Koreans with knee osteoarthritis: data from the Korean National Health and nutrition examination survey (KNHANES). PLoS One. 2017;12(10):e0186141.
Langu Dan Louise GL, F.A.., Husser Stephen, Lawcalso Joseph, Casper Dennis (2012). Internal medicine book. Rheumatic diseases and immune system. Translators: Nafiseh Abdollahi and Fahimeh Abdollahi. Boshr Resources.
Yegane A, Mottaghi A, Moghimi J. Correlation of quantified MRI, physical exam and knee radiography in patients with knee osteoarthritis. Tehran Univ Med J. 2011;69(3):185–90.
Ganji R, et al. Prevalence of osteoporosis and osteopenia in men and premenopausal women with celiac disease: a systematic review. Nutr J. 2019;18(1):9.
Stolz M, et al. Early detection of aging cartilage and osteoarthritis in mice and patient samples using atomic force microscopy. Nat Nanotechnol. 2009;4(3):186.
Mortazavi H, et al. The effect of self-management education program on disability of elderly patients with knee osteoarthritis referring to elderly care clinic of imam Reza (AS) treatment center in shiraz, 2015-2106. J North Khorasan Univ Med Sci. 2017;8(3):461–70.
Smith GN Jr. The role of collagenolytic matrix metalloproteinases in the loss of articular cartilage in osteoarthritis. Front Biosci. 2006;11(3081):95.
Stone AV, et al. Osteoarthritic changes in vervet monkey knees correlate with meniscus degradation and increased matrix metalloproteinase and cytokine secretion. Osteoarthr Cartil. 2015;23(10):1780–9.
Giessen, E., The role of joint homeostasis in equine articular cartilage repair. 2019.
Harris ED, DiBona DR, Krane SM. Collagenases in human synovial fluid. J Clin Invest. 1969;48(11):2104–13.
Abramson SB. Nitric oxide in inflammation and pain associated with osteoarthritis. Arthritis Res Ther. 2008;10(2):S2.
Melchiorri C, et al. Enhanced and coordinated in vivo expression of inflammatory cytokines and nitric oxide synthase by chondrocytes from patients with osteoarthritis. Arthritis Rheum. 1998;41(12):2165–74.
Studer R, et al. Nitric oxide in osteoarthritis. Osteoarthr Cartil. 1999;7(4):377–9.
McInnes IB, et al. Production of nitric oxide in the synovial membrane of rheumatoid and osteoarthritis patients. J Exp Med. 1996;184(4):1519–24.
Wei Y, et al. Resveratrol ameliorates inflammatory damage and protects against osteoarthritis in a rat model of osteoarthritis. Mol Med Rep. 2018;17(1):1493–8.
Coudeyre E, et al. Isokinetic muscle strengthening for knee osteoarthritis: a systematic review of randomized controlled trials with meta-analysis. Ann Phys Rehabil Med. 2016;59(3):207–15.
Szychlinska M, et al. Altered joint tribology in osteoarthritis: reduced lubricin synthesis due to the inflammatory process. New horizons for therapeutic approaches. Ann Phys Rehabil Med. 2016;59(3):149–56.
Muñoz-López M, et al. Load-, force-, and power-velocity relationships in the prone pull-up exercise. Int J Sports Physiol Perform. 2017;12(9):1249–55.
Keshavarz R, et al. Dendrosomal nanocurcumin and p53 overexpression synergistically trigger apoptosis in glioblastoma cells. Iran J Basic Med Sci. 2016;19(12):1353.
Appelboom T, Maes N, Albert A. A new curcuma extract (Flexofytol®) in osteoarthritis: results from a Belgian real-life experience. Open Rheumatol J. 2014;8:77.
Sun Y, et al. Curcumin prevents osteoarthritis by inhibiting the activation of Inflammasome NLRP3. J Interf Cytokine Res. 2017;37(10):449–55.
Pant MK, et al. Curcumin: a wonder therapeutical drug. World J Pharm and Pharm Sci. 2014;3(6):374–96.
Yadav A, Flora S, Kushwaha P. Nanocurcumin prevents oxidative stress induced following arsenic and fluoride co-exposure in rats. Def Life Sci J. 2016;1(1):69–77.
Schulz KF, Grimes DA. Allocation concealment in randomised trials: defending against deciphering. Lancet. 2002;359(9306):614–8.
Vincent KR, Vincent HK. Resistance exercise for knee osteoarthritis. PM&R. 2012;4(5):S45–52.
Rewald S, et al. Effect of aqua-cycling on pain and physical functioning compared with usual care in patients with knee osteoarthritis: study protocol of a randomised controlled trial. BMC Musculoskelet Disord. 2016;17:88.
Neogi T. The epidemiology and impact of pain in osteoarthritis. Osteoarthr Cartil. 2013;21(9):1145–53.
Alshami AM. Knee osteoarthritis related pain: a narrative review of diagnosis and treatment. Int J Health Sci (Qassim). 2014;8(1):85–104.
Pereira Nunes Pinto, Ana Carolina, et al., Acute effect of a resistance exercise session on markers of cartilage breakdown and inflammation in women with rheumatoid arthritis. International journal of rheumatic diseases, 2017. 20(11): p. 1704–1713.
Aguiar GC, et al. Effects of an exercise therapy protocol on inflammatory markers, perception of pain, and physical performance in individuals with knee osteoarthritis. Rheumatol Int. 2015;35(3):525–31.
Maeda S, et al. Moderate regular exercise increases basal production of nitric oxide in elderly women. Hypertens Res. 2004;27(12):947–53.
Hashimoto S, et al. Nitric oxide production and apoptosis in cells of the meniscus during experimental osteoarthritis. Arthritis Rheum. 1999;42(10):2123–31.
McInnes IB, et al. The role of interleukin-15 in T-cell migration and activation in rheumatoid arthritis. Nat Med. 1996;2(2):175–82.
Pinsornsak P, Niempoog S. The efficacy of Curcuma longa L. extract as an adjuvant therapy in primary knee osteoarthritis: a randomized control trial. J Med Assoc Thail. 2012;95(Suppl 1):S51–8.
Henrotin Y, Priem F, Mobasheri A. Curcumin: a new paradigm and therapeutic opportunity for the treatment of osteoarthritis: curcumin for osteoarthritis management. Springerplus. 2013;2(1):56.
Wang J, et al. Regulation of type II collagen, matrix metalloproteinase-13 and cell proliferation by interleukin-1beta is mediated by curcumin via inhibition of NF-kappaB signaling in rat chondrocytes. Mol Med Rep. 2017;16(2):1837–45.
Chan MM, et al. In vivo inhibition of nitric oxide synthase gene expression by curcumin, a cancer preventive natural product with anti-inflammatory properties. Biochem Pharmacol. 1998;55(12):1955–62.
Panahi Y, et al. Curcuminoid treatment for knee osteoarthritis: a randomized double-blind placebo-controlled trial. Phytother Res. 2014;28(11):1625–31.
Acknowledgements
Not applicable.
Funding
None.
Author information
Authors and Affiliations
Contributions
SCB, MB, FH, AA, and MRS were involved in experiments and sample gathering. MM was involved in drafting and edition. RG supervised the project. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This work was approved by the Ethics Committee of North Khorasan University of Medical Sciences (No. ir. Nkums.rec.1396.77). The research project was also registered at Iranian Registry of Clinical Trials (Trial registration number: IRCT20161208031300N1). All the participants filled informed consent forms which were approved by the ethic committee of North Khorasan University of Medical Sciences.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Cheragh-Birjandi, S., Moghbeli, M., Haghighi, F. et al. Impact of resistance exercises and nano-curcumin on synovial levels of collagenase and nitric oxide in women with knee osteoarthritis. transl med commun 5, 3 (2020). https://doi.org/10.1186/s41231-020-00055-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41231-020-00055-0