
Abstract
Background
Volume overload in hemodialysis patients is an independent risk factor for cardiovascular event-related mortality. The number of B-lines observed using lung ultrasound is correlated with the severity of pulmonary congestion. The aim of this study was to evaluate the association between the number of B-lines and mortality among hemodialysis patients.
Methods
A total of 61 patients receiving maintenance hemodialysis were enrolled in this study. Clinical data including age, sex, duration of hemodialysis therapy, presence of diabetes mellitus and/or hypertension and/or dyslipidemia complications, the results of biological examinations, and outcome were collected from the patients’ clinical records. We performed echographic examinations at three time points (just after the start, during the middle, and just before the end of hemodialysis therapy). A univariate Cox proportional hazard model was used to identify predictors of the overall outcomes. Furthermore, we divided patients into two groups according to the median number of the B-lines at the end of dialysis and compared the mortality between the two groups.
Results
The mean follow-up period was 507 ± 385 days. During the follow-up period, 24 deaths were recorded. Predictive variables for mortality included age; serum level of albumin, creatinine, and N-terminal pro-brain natriuretic peptide; and body weight (P < 0.001, P < 0.0001, P < 0.001, P = 0.014, and P = 0.019, respectively). The number of B-lines at the start, middle, and end of dialysis therapy was correlated with mortality (hazard ratio (95% confidence interval) 1.20 (1.09–1.32), P = 0.0002; 1.17 (1.07–1.28), P = 0.0008; and 1.23 (1.12–1.37), P = 0.0001; respectively). The mortality was statistically higher in the group with 5 or more B-lines than in the group with less than 5 B-lines (P = 0.013).
Conclusions
The number of B-lines at the start, middle, and end of hemodialysis therapy may be correlated with mortality among hemodialysis patients.
Similar content being viewed by others


Background
Volume overload in hemodialysis patients is an independent risk factor for death from cardiovascular events [1]. Proper evaluation of the intracellular and extracorporeal volumes to set the proper correct dry weight is important for hemodialysis patients. Many methods have been utilized to assess the volume statuses of hemodialysis patients.
Lung ultrasound has recently been shown to be a useful, noninvasive technique for the assessment of extravascular lung water [2]. The most commonly observed finding is a comet tail artifact fanning out from the lung-wall interface and spreading upwards to the edge of the screen, previously named a “B-line” [3]. In patients with heart failure, the number of B-lines is correlated with the degree of extravascular lung water [4, 5]. The pre-dialysis number of B-lines significantly correlated with whole-body bioimpedance spectroscopy device-derived extracellular water in hemodialysis patients [6]. Vitturi et al. investigated lung and bioimpedance spectroscopy results immediately before and after dialysis and reported that a reduction in the number of B-lines was correlated with fluid loss as a result of hemodialysis, conforming that lung ultrasound can identify extravascular lung water. The number of post-dialysis B-lines is correlated with the residual weight assessed using bioimpedance, suggesting a role for ultrasound in the management of hemodialysis patients [7]. Lung ultrasound is also reportedly useful for the accurate evaluation of dry weight and fluid status in hemodialysis patients [2, 8, 9]. The number of B-lines observed using lung ultrasound represents the severity of pulmonary congestion [10].
The relationship between pre-hemodialysis number of B-lines and mortality was already reported [6]. Another investigator reported that the number of B-lines at the end of hemodialysis therapy was related to mortality [11]. There was no report which investigates the relationship between the number of B-lines at the middle of hemodialysis therapy and mortality.
The aim of this study was to evaluate the association between the number of B-lines at three points (at the start, the middle, and the end) and mortality among hemodialysis patients.
Methods
A total of 61 patients receiving maintenance hemodialysis at Sekikawa Hospital were enrolled in this study. Clinical data including age, sex, duration of hemodialysis therapy, presence of diabetes mellitus and/or hypertension and/or dyslipidemia complications, the results of biological examinations, and outcome were collected from the patients’ clinical records. Hypertension was defined as a systolic blood pressure of 140 mmHg or higher, a diastolic blood pressure of 90 mmHg or higher, and/or the current use of antihypertensive drugs. Diabetes mellitus was defined as a fasting glucose level ≥ 126 mg/dL, a nonfasting glucose level ≥ 200 mg/dL, or the use of medication. Dyslipidemia was defined as a low-density lipoprotein-cholesterol level ≥ 140 mg/dL, a high-density lipoprotein-cholesterol level < 40 mg/dL, a triglyceride level ≥ 150 mg/dL, or the use of medication. A peripheral blood sample was obtained before hemodialysis during the first session of the week. The serum N-terminal pro-brain natriuretic peptide (NT-proBNP) level in the pre-dialysis blood sample was measured using an electrochemiluminescence immunoassay on an Elecsys platform (Roche, Basel, Switzerland).
A lung ultrasound examination was performed during the first session of the week (at the same time as the peripheral blood sample preparation) using Vscan® (GE Healthcare, Japan), which is a hand-held ultrasound device with a wide-bandwidth phased-array probe (1.7–3.5 MHz) [12, 13]. Bilateral scanning of the anterior and lateral chest walls was performed with the patient in a supine position. An intercostal scan with a maximum extension of the visual pleural line was performed. The chest wall was divided into eight areas (two anterior and two lateral areas per side), and one scan was obtained for each area [14]. The anterior zone of the chest wall was designated as the area from the sternum to the anterior axillary line and was then divided into upper and lower halves (from the clavicle to the third intercostal space and from the third space to the diaphragm). The lateral zone was positioned from the anterior axillary line to the posterior axillary line and was also divided into the upper and lower halves. The investigator attempted to detect comet tail artifacts fanning out from the lung-wall interface and spreading to the edge of the screen, which were previously named B-lines [5, 8]. The total number of B-lines was estimated. Echocardiographic measurements were obtained at the same time, and the inferior vena cava (IVC) dimensions and the peak early mitral inflow wave velocity (peak E-velocity) were estimated using VividS60® (GE Healthcare, Japan). One expert cardiologist, who is blind to the result of blood peripheral blood sample, underwent both lung and cardiac echo examinations. He performed echographic examinations three times (just after the start, during the middle, and just before the end of the hemodialysis therapy). Furthermore, we divided patients into two groups according to the median number of the B-lines at the end of dialysis and compared the mortality between the two groups.
The data were expressed as the means ± S.D. or the median (interquartile range; IQR). To evaluate the association between the number of B-lines and mortality, univariate Cox proportional hazard model was used to examine the predictors of the overall outcomes. The survival curves were estimated using the Kaplan–Meier method. To evaluate the association between the number of B-lines and mortality among hemodialysis patients, a log-rank test was used to compare mortality between the group with a high number of B-lines and the group with a low number of B-lines. All the statistical calculations were performed using JMP 5.1 software. P values less than 0.05 were considered statistically significant. This study was conducted in accordance with the principles of the Declaration of Helsinki and was permitted by the research ethics committee of Sekikawa Hospital (Approved No. H2705).
Results
The patient background characteristics are shown in Table 1. The mean age was 75.2 ± 10.7 years. Diabetic nephropathy was the major cause of end-stage kidney disease (45.9%). Hypertension, diabetes mellitus, and dyslipidemia were present in 86.9%, 45.9%, and 18.0% of the study participants, respectively. The serum albumin level was relatively low (3.1 ± 0.6 g/dL), and the serum NT-proBNP level was relatively high (13,851 [4764–34,279]) pg/mL) among the study participants. The mean ejection fraction was 60.1 ± 13.4%.
The treatment time was 3.7 ± 0.4 h. All participants did not have symptoms of dyspnea and did not undergo oxygen therapy. There was no patient with proteinuria at the nephrotic level. None underwent albumin or blood transfusion during the hemodialysis therapy. Table 2 shows the changes in the echocardiographic indices. The number of B-lines decreased from 11.8 ± 5.5 at the start of the therapy to 9.3 ± 5.3 during the middle and 5.2 ± 4.5 at the end of the therapy. The peak E-velocity also decreased from 78.0 ± 25.8 cm/s at the start of the therapy to 57.5 ± 20.8 cm/s during the middle and 51.4 ± 20.3 cm/s at the end of the therapy. The IVC-exhalation dimensions also decreased from 15.3 ± 3.8 mm at the start of the therapy to 12.0 ± 3.5 mm during the middle and 10.6 ± 3.4 mm at the end of the therapy.
The mean follow-up period was 507 ± 385 days. During the follow-up period, 24 deaths (including 12 from infection, 8 from heart failure, 2 from malignant tumors, and 2 from other causes) were recorded.
Table 3 shows a Cox proportional hazards analysis of the covariates for predicting mortality. In the univariate regression analysis, predictive variables for mortality included age; serum level of albumin, creatinine, and NT-proBNP; and body weight (P < 0.001, P < 0.0001, P < 0.001, P = 0.014, and P = 0.019, respectively). Ultrafiltration rate (UFR), UFR/body weight, and ΔB-lines/B-lines at the start also associated with mortality (P = 0.004, P = 0.042, and P = 0.027, respectively). Elder, low serum level of albumin and creatinine, high serum level of NT-proBNP, and low level of UFR, UFR/body weight, and ΔB-lines/B-lines at the start were risk factors for mortality.
Table 4 shows the results of the same Cox proportional hazards analysis focusing on the echocardiographic changes during hemodialysis therapy. Significant factors related to mortality were the number of B-lines at the start (hazard ratio (95% confidence interval); 1.20 (1.09–1.32), P = 0.0002), middle (1.17 (1.07–1.28), P = 0.0008), and end (1.23 (1.12–1.37), P = 0.0001) of dialysis therapy. A large number of B-lines at any point resulted in poor outcome. The number of B-lines at the end of hemodialysis therapy was the most significant factor associated with mortality.
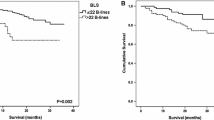
The medium number of B-lines at the end of hemodialysis therapy was 4, so we divided patients into two groups, the “5 or more” group (n = 30) and the “less than 5” group (n = 31). Figure 1 shows the comparison of survival curves between the 5 or more group and less than 5 group. One-year survival was 55.4% in the 5 or more group whereas it was 89.8% in less than 5 group. The mortality was statistically higher in the 5 or more group than the less than 5 group (P = 0.013).

The comparison of survival curves between the group with 5 or more B-lines (n = 30) and the group with less than 5 B-lines (n = 31) at the end of hemodialysis therapy. One-year survival was 55.4% in the 5 or more group whereas it was 89.8% in the less than 5 group. The mortality was statistically high in the more than 5 group than the less than 5 group (P = 0.013)
Discussion
We found that the number of B-lines at the start, middle, and end of hemodialysis therapy was a risk factor for mortality. Among them, the number of B-lines at the end of hemodialysis therapy was the most significant factor. Furthermore, we divided the patients according to the number of B-lines at the end of hemodialysis therapy and found the mortality was statistically higher in the 5 or more group than the less than 5 group.
Lung ultrasound is a novel, well-validated technique that allows reliable clinical estimates of lung water [5]. B-lines can be evaluated anywhere (including extreme environmental conditions using pocket-sized instruments to detect high-altitude pulmonary edema), anytime (during dialysis), by anyone (even a novice sonographer after 1 h of training), and on anybody (since the chest acoustic window usually remains patent even when an echocardiography is not feasible) [10].
In this study, the IVC dimensions and peak E-velocity were not associated with mortality. Both the IVC dimensions and the peak E-velocity are related to the intravascular volume; the IVC dimensions represent the right ventricular preload [15], whereas the peak E-velocity represents the left ventricular preload [16, 17]. On the other hand, B-lines represent extravascular lung water. We previously reported that the IVC dimensions and the peak E-velocity were reduced mainly during the first half of the dialysis period, while the number of B-lines, which represents lung congestion, decreased significantly mainly during the last half of the dialysis period [18]. This finding may be largely dependent on the time lag in plasma refilling. Thus, even if the IVC dimensions are sufficiently reduced, lung congestion may still exist and should be treated.
There may be several possible pathophysiologies about the relationship between the number of B-lines and mortality. Lung congestion is a direct consequence of either overall overhydration and/or cardiac dysfunction which may affect poor outcome. At the same time, there is a direct pathophysiological link between overall hydration and left ventricular function. As we previously reported, the number of B-lines negatively related to body weight and serum level of albumin and creatinine [8]. Two mechanisms have been proposed to explain the relationship between hypoalbuminemia and congestion. On the one hand, an increase in vascular permeability mediated by an increase in hydrostatic venous pressure may increase the transcapillary escape rate of albumin from the intravascular to the extravascular space [19]; on the other hand, it is possible that intestinal congestion favors albumin enteric losses [20]. The decrease in oncotic pressure due to low serum level of albumin causes the movement of water from intravascular to lung interstitial. The malnutrition-inflammation-atherosclerosis syndrome affects mortality and hydration mechanics [18], which may be another cause of the relation between number of B-lines and mortality.
The relationship between the number of B-lines and mortality has been reported by investigators in several countries. From Italy, the number of B-lines before hemodialysis was reported to be a strong, independent predictor of death and cardiac events [21]. From Romania, the pre-hemodialysis number of B-lines was shown to have a significant independent discriminating power for survival [6]. The latter authors also reported that the post-dialysis number of B-lines also had a significant impact on survival when examined using a crude Cox analysis, but the statistical significance was lost after adjusting for other factors [6]. In our study, the number of B-lines at the end of the hemodialysis therapy was more strongly associated with mortality than the number of B-lines at the start of the hemodialysis therapy. The mortality was statistically higher in the 5 or more group than in the less than 5 group at the end of hemodialysis therapy. This difference may be caused, in part, by the difference in the backgrounds of the hemodialysis patients. Nishihira et al. measured the B-line score of Japanese hemodialysis patients using a method similar to that used in the Italian study. The B-line score has been reported to be lower at both pre-hemodialysis (8.9 vs. 33.5) and post-hemodialysis (4.7 vs. 16.1) in Japan compared with that in Italy [22]. Gargani investigated patients who were admitted because of acute heart failure and found that the number of B-lines at the time of hospital discharge, but not at admission, strongly predicted rehospitalization [23]. Another investigator also reported that residual pulmonary congestion at discharge, as assessed using a B-line count ≥ 30, was a strong predictor of all-cause death or heart failure hospitalization [24]. Treatment-resistant pulmonary congestion appears to be a poor prognostic factor among patients with heart failure. We found low level of UFR/body weight which also resulted in a poor outcome. UFR/body weight represents the plasma refilling rate. Condition of low level of plasma refilling rate, which results in refractory lung congestion, might affect mortality. Indeed, we revealed low level of ΔB-lines/B-lines at the start resulted in a poor outcome.
Pulmonary congestion, which can remain after hemodialysis therapy, may also be correlated with a poor outcome. In a recent American study, a multivariate Cox regression analysis showed that the number of B-lines at the end of hemodialysis therapy was an independent predictor of mortality [11]. Thorough removal of the water and the prevention of lung congestion at the end of hemodialysis seem to be important for a better prognosis. We reported that the patient heart rate and the serum log (NT-proBNP) level were positively correlated and the body weight and the serum albumin and creatinine level were negatively correlated with the number of B-lines [8]. Improving conditions that can easily cause pulmonary congestion might also be useful for improving patient outcome.
Our study had some limitations. The sample size was relatively small, and the study was performed at a single institution. B-line echo findings contribute to the dry weight setting [2, 8, 9], but in our study, nephrologists determined each dry weight using conventional markers such as change of blood pressure, X-ray finding, or serum level of biomarkers. We could not find a statistically significant relationship between number of B-lines at any point and deaths from heart failure. That may be because of the small number of studied participants. We enrolled not only out patients but also hospitalized patients in this study, so the mortality was high and serum level of albumin was low. Therefore, caution must be exercised when generalizing our current results to different hemodialysis patients. Measurement of B-line in lung echogram is an operation-dependent examination. But Bedetti et al. compared lung ultrasound information obtained by experienced echocardiologists and by an inexperienced echocardiographer with very limited (30′) dedicated training on B-line assessment and reveal there was a significant, tight correlation (r = 0.958, p < 0.001) between the two observations in the same patient [25]. We generally use chest X-ray for evaluation of pulmonary congestions. But we could not estimate chest X-ray at the same time as echo examinations. Several groups have shown how B-lines correlate reasonably well with the imperfect gold standards of chest X-ray [26, 27] and radiological score. The correlation is stronger when intra-patient variations are considered [26]. Another limitation of this study was that the investigator that performed ultrasound was not blind for clinical information of the patients such as age, gender, or clinical diagnosis. In addition, the limitations of lung ultrasound are essentially patient-dependent. Obese patients may be more difficult to examine because of the thickness of their ribcages and soft tissues.
Conclusions
The number of B-lines at the start, middle, and end of hemodialysis therapy may be correlated with mortality among hemodialysis patients.
Availability of data and materials
The datasets during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Change history
06 August 2019
An error occurred during the publication of a number of articles in Renal Replacement Therapy. Several articles were published in volume 5 with a duplicate citation number.
Abbreviations
- IVC:
-
Inferior vena cava
- NT-proBNP:
-
N-terminal pro-brain natriuretic peptide
- peak E-velocity:
-
Peak early mitral inflow wave velocity
- UFR:
-
Ultrafiltration rate
References
Wang AY, Sanderson JE. Current perspectives on diagnosis of heart failure in long-term dialysis patients. Am J Kidney Dis. 2011;57:308–19.
Alexiadis G, Panagoutsos S, Roumeliotis S, Stibiris I, Markos A, Kantartzi K, et al. Comparison of multiple fluid status assessment methods in patients on chronic hemodialysis. Int Urol Nephrol. 2017;49:525–32.
Lichtenstein D. Pneumothorax and introduction to ultrasound signs in the lung. In: Heilmann U, Wilbertz H, Gosling A, editors. editors General ultrasound in the critically ill. 1st ed. Heidelberg: Springer-Verlag; 2005. p. 105–15.
Agricola E, Bove T, Oppizzi M, Marino G, Zangrillo A, Margonato A, et al. “Ultrasound comet-tail images”: a marker of pulmonary edema: a comparative study with wedge pressure and extravascular lung water. Chest. 2005;127:1690–5.
Kajimoto K, Madeen K, Nakayama T, Tsudo H, Kuroda T, Abe T. Rapid evaluation by lung-cardiac-inferior vena cava (LCI) integrated ultrasound for differentiating heart failure from pulmonary disease as the cause of acute dyspnea in the emergency setting. Cardiovasc Ultrasound. 2012;10:49–51.
Siriopol D, Hogas S, Voroneanu L, Onofriescu M, Apetrii M, Oleniuc M, et al. Predicting mortality in haemodialysis patients: a comparison between lung ultrasonography, bioimpedance data and echocardiography parameters. Nephrol Dial Transplant. 2013;28:2851–9.
Vitturi N, Dugo M, Soattin M, Simoni F, Maresca L, Zagatti R, et al. Lung ultrasound during hemodialysis: the role in the assessment of volume status. Int Urol Nephrol. 2014;46:169–74.
Kuzuhara S, Otsubo S, Kajimoto K, Akiba T, Nitta K. Association between B-lines detected during lung ultrasound and various factors in hemodialysis patients. Ren Replace Ther. 2017;3:17.
Noble VE, Murray AF, Capp R, Sylvia-Reardon MH, Steele DJ, Liteplo A. Ultrasound assessment for extravascular lung water in patients undergoing hemodialysis: time course for resolution. Chest. 2009;135:1433–9.
Picano E, Pellikka PA. Ultrasound of extravascular lung water: a new standard for pulmonary congestion. Eur Heart J. 2016;37:2097–104.
Saad MM, Kamal J, Moussaly E, Karam B, Mansour W, Gobran E, et al. Relevance of B-lines on lung ultrasound in volume overload and pulmonary congestion: clinical correlations and outcomes in patients on hemodialysis. Cardiorenal Med. 2018;8:83–91.
Cardim N, Fernandez Golfin C, Ferreira D, Aubele A, Toste J, Cobos MA, et al. Usefulness of a new miniaturized echocardiographic system in outpatient cardiology consultations as an extension of physical examination. J Am Soc Echocardiogr. 2011;24:117–24.
Liebo MJ, Israel RL, Lillie EO, Smith MR, Rubenson DS, Topol EJ. Is pocket mobile echocardiography the next-generation stethoscope? A cross-sectional comparison of rapidly acquired images with standard transthoracic echocardiography. Ann Intern Med. 2011;155:33–8.
Volpicelli G, Elbarbary M, Blaivas M, Lichtenstein DA, Mathis G, Kirkpatrick AW, et al. International Liaison Committee on Lung Ultrasound (ILC-LUS) for International Consensus Conference on Lung Ultrasound (ICC-LUS). International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012;38:577–91.
Simonson JS, Schiller NB. Sonospirometry: a new method for noninvasive estimation of mean right atrial pressure based on two-dimensional echographic measurements of the inferior vena cava during measured inspiration. J Am Coll Cardiol. 1988;11:557–64.
Triulzi MO, Castini D, Ornaghi M, Vitolo E. Effects of preload reduction on mitral flow velocity pattern in normal subjects. Am J Cardiol. 1990;66:995–1001.
Sztajzel J, Ruedin P, Monin C, Stoermann C, Leski M, Rutishauser W, Lerch R, et al. Effect of altered loading conditions during haemodialysis on left ventricular filling pattern. Eur Heart J. 1993;14:655–61.
Kimura K, Kajimoto K, Otsubo S, Akiba T, Nitta K. Associations between fluid removal and number of B-lines, peak early mitral inflow wave velocity, and inferior vena cava dimensions in hemodialysis patients. Ren Replace Ther. 2017;3:54.
Hesse B, Parving HH, Lund-Jacobsen H, Noer I. Transcapillary escape rate of albumin and right atrial pressure in chronic congestive heart failure before and after treatment. Circ Res. 1976;39:358–62.
Battin DL, Ali S, Shahbaz AU, Massie JD, Munir A, Davis RC Jr. Hypoalbuminemia and lymphocytopenia in patients with decompensated biventricular failure. Am J Med Sci. 2010;339:31–5.
Zoccali C, Torino C, Tripepi R, Tripepi G, D'Arrigo G, Postorino M, et al. Pulmonary congestion predicts cardiac events and mortality in ESRD. J Am Soc Nephrol. 2013;24:639–46.
Nishihira M, Shimoji K, Oroku M, Nagayama K, Adachi T, Kikumura T, et al. Lower US B line score in Japanese hemodialysis patients. Nephrol Dial Transplant. 2017;32(suppl 3):iii 652.
Gargani L, Pang PS, Frassi F, Miglioranza MH, Dini FL, Landi P, et al. Persistent pulmonary congestion before discharge predicts rehospitalization in heart failure: a lung ultrasound study. Cardiovasc Ultrasound. 2015;13:40.
Coiro S, Rossignol P, Ambrosio G, Carluccio E, Alunni G, Murrone A, et al. Prognostic value of residual pulmonary congestion at discharge assessed by lung ultrasound imaging in heart failure. Eur J Heart Fail. 2015;17:1172–81.
Bedetti G, Gargani L, Corbisiero A, Frassi F, Poggianti E, Mottola G. Evaluation of ultrasound lung comets by hand-held echocardiography. Cardiovasc Ultrasound. 2006;31(4):34.
Picano E, Frassi F, Agricola E, Gligorova S, Gargani L, Mottola G. Ultrasound lung comets: a clinically useful sign of extravascular lung water. J Am Soc Echocardiogr. 2006;19:356–63.
Volpicelli G, Caramello V, Cardinale L, Mussa A, Bar F, Frascisco MF. Bedside ultrasound of the lung for the monitoring of acute decompensated heart failure. Am J Emerg Med. 2008;28:585–91.
Acknowledgments
The authors are very grateful to dialysis staff who understood the clinical importance of this study and who provided high-quality data in Sekikawa Hospital.
Funding
This study was not supported by any grants or funding.
Author information
Authors and Affiliations
Contributions
KK planned the study, searched the literature, assessed studies, extracted the data, analyzed the data, and prepared the article. KK and SO searched the literature, assessed the studies, and assisted in the article preparation. KK performed the lung echo. KN assisted in the article preparation. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the research ethics committee of Sekikawa Hospital (Approved No. H2705) and was conducted under the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Kawachi, K., Kajimoto, K., Otsubo, S. et al. Associations between pulmonary congestion on chest ultrasound and survival in hemodialysis patients. Ren Replace Ther 5, 27 (2019). https://doi.org/10.1186/s41100-019-0223-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41100-019-0223-x