
Abstract
Background
Sirolimus has been confirmed to be effective for lymphangioleiomyomatosis (LAM), a rare multisystem neoplastic disease in women. The long-term effects of sirolimus treatment for LAM, however, are largely unknown. We aimed to analyze the long-term efficacy and safety of sirolimus therapy for LAM with 4-year follow-up.
Methods
In total, 142 sporadic LAM patients who took sirolimus for 1–4 years were retrospectively enrolled for this analysis. The variables used for analysis included pulmonary function tests, arterial blood gas analysis, 6-min walking distance (6MWD), St. George’s Respiratory Questionnaires (SGRQ) and serum vascular endothelial growth factor-D (VEGF-D) levels before and after the initiation of sirolimus therapy. The rates of change (slope) in those variables were calculated, and adverse events were also analyzed.
Results
In total, 122, 83, 60 and 32 patients out of 142 were followed for 1, 2, 3 and 4 years respectively. Sirolimus treatment improved the change rate in forced expiratory volume in 1 second (FEV1) and forced vital capacity (FVC) compared with the data before treatment (FEV1, − 10 ± 15 vs. − 178 ± 36 ml/y, P < 0.001 and FVC, 54 ± 22 vs.-72 ± 68 ml/y, P < 0.05). In comparison to the baseline measurements, significant improvements were observed in FEV1 at the first year; FVC at 1–2 years; arterial oxygen levels, 6MWD, and SGRQ at 1–3 years; and VEGF-D at 1–4 years. Overall, all variables stabilized or improved during the 4 years of observation. Adverse events related to sirolimus were mild.
Conclusion
Sirolimus therapy is effective at improving or stabilizing pulmonary function, oxygen levels, exercise capacity, and quality of life in patients with LAM for up to 4 years. VEGF-D is maintained at a lower level for 4 years after treatment. Adverse events related to sirolimus were mild.
Similar content being viewed by others

Background
Lymphangioleiomyomatosis (LAM) is a rare multisystem neoplastic disease that is characterized by cystic lung destruction, angiomyolipoma and lymphangioleiomyomas [1, 2]. LAM may occur sporadically, or in adults with tuberous sclerosis complex [1]. Cystic remodeling in the lungs compromises lung function, resulting in progressive dyspnea, and finally respiratory failure [3].
Sirolimus (rapamycin) has been confirmed to be effective for the treatment of LAM [4, 5]. In our previous report, sirolimus was shown to improve lung function, arterial oxygen levels, 6 min walking distance (6MWD), St George Respiratory questionnaire (SGRQ) scores and vascular endothelial growth factor (VEGF-D) levels [6]. However, the long-term effects of sirolimus are unclear. Several studies included data on sirolimus treatment over a 2-years period [7,8,9,10,11,12]. Taveria-DaSilva et al. [8] reported a study in which 44 patients were treated with sirolimus alone, the changes of predicted values of FEV1 and DLCO were − 1.7% ± 0.1% and − 2.2% ± 0.1% before treatment and + 1.7 ± 0.3% and + 0.7% ± 0.3% after treatment (P < 0.001) during a mean of 2.8 years follow up time. In the recent study, Taveira-DaSilva et al. [9] evaluated the change of pulmonary function of 25 patients with sirolimus treatment, over a period of 4.5 ± 1.6 years, in which annual changes in forced expiratory volume in 1 s (FEV1) and diffusion capacity for carbon monoxide (DLCO) were reduced from − 7.4% ± 1.4% to − 0.3% ± 0.5% (P < 0.001) and − 6.4% ± 0.9% to − 0.4% ± 0.5% (P < 0.001), respectively. Johnson et al. [10, 11] prospectively observed LAM patients treated with sirolimus over 2 years, the mean change in FEV1 ranged from − 7 ± 82 ml/year (n = 23) to 11 ± 75 ml/year(n = 47). The above studies demonstrated that sirolimus effectively improves the lung function in LAM patients. However, it is still unknown whether sirolimus continuously improves or stabilizes lung function over a longer observation period.
Considering sirolimus is used in LAM patients for a long period of time, whether its efficacy can be maintained is a critical question. Safety is another issue for those patients who take sirolimus for many years. In this study, we analyzed the efficacy and safety of sirolimus for up to 4 years.
Method
Study populations
Subjects were from the LAM registry in Peking Union Medical College Hospital (PUMCH), Beijing, China. The diagnosis of LAM was re-evaluated and confirmed according to the recent diagnosis criteria of American Thoracic Society and Japanese Respiratory Society published in 2017 [13]. Subjects were included if the following criteria were met: (1) sirolimus therapy with follow-up data after treatment, and (2) sirolimus therapy with baseline evaluation (within 3 months of sirolimus initiation). The exclusion criteria included the following: (1) patients with tuberous sclerosis complex, and (2) patients with other malignant tumors, and (3) patients who had undergone lung transplantation. Patients with tuberous sclerosis complex were not included because of limited data of this group of patients.
The protocol of this study was approved by the Ethical Committee of PUMCH (S-K709). All subjects included in this study signed informed consent documents.
The indication of sirolimus was primarily based on reduced lung function (FEV1 less than 70% predicted value) or rapidly declining lung function (FEV1 loss over 90 ml per year) [5]. Other indications included chylothorax, chylous ascites, angiomyolipomas or repeated pneumothorax, etc. Dosage and dosage adjustment of sirolimus were based on the judgement of the physicians who treated the patient, which have been described in our previous study [6]. Generally, patients took sirolimus 1 or 2 mg orally once daily. A serum level of 5 to 10 ng/ml sirolimus was considered optimal concentration range. For patients with a serum level > 10 ng/ml or < 5 ng/ml, the dose of sirolimus was adjusted according to the clinical symptoms and adverse events.
Study design
We carefully collected the annual follow-up records of the enrolled subjects for this retrospective analysis. The follow-up visit data comprised pulmonary function tests, arterial blood gas analysis at rest (on room air), 6MWD, Borg dyspnea index, SGRQ, and VEGF-D. The baseline data were defined as those collected within 3 months of sirolimus initiation. The additional data were categorized as pretreatment and posttreatment data, defined as 1 year (± 3 months) or 2 years (± 3 months) before sirolimus initiation and 1 year (± 3 months), 2 years (± 3 months), 3 years (± 3 months), and 4 years (± 3 months) after sirolimus initiation.
Pulmonary function was measured according to the American Thoracic Society/European Respiratory Society (ATS/ERS) Task Force Standardization of Lung Function Testing [14]. The 6MWD was performed based on ATS guidelines [15]. Borg dyspnea index was assessed at the end of the 6MWD test. Patients completed the SGRQ according to the provided instructions. The pneumothorax and chylothorax were evaluated by chest X-ray or CT. Degree of pulmonary cystic lesions and renal angiomyolipoma size was evaluated by CT. Adverse events were assessed according to the Common Terminology Criteria for Adverse Events (version 3.0). Serum VEGF-D levels were measured with an enzyme-linked immunosorbent assay (Quantikinine Human VEGF-D Immunoassay, R&D Systems).
Statistical analysis
Normally distributed data are reported as the mean ± SD; data that were not normally distributed are reported as the medians and interquartile ranges (median [25, 75%]). The normality of the data was analyzed by the Kolmogorov-Smirnov test. The unpaired t-test or Mann-Whitney U-test was used to compare continuous variables. The paired t-test was used to compare the baseline data with post-treatment data. All reported P values are two-sided. P values less than 0.05 were considered statistically significant. We used R language V3.5.3 (Microsoft, Washington, USA) to build linearmix-effect model in order to assess the effects of sirolimus therapy. Data analyses were also performed in GraphPad Prism V.7.03 (Graphpad, California, USA) and SPSS V.24 (IBM, New York, USA).
Results
Demographics
The baseline characteristics and clinical features of the study participants (n = 142) are shown in Table 1. Of 142 subjects enrolled, 122, 83, 60 and 32 patients were followed-up for 1, 2, 3 and 4 years respectively.
Sirolimus improves pulmonary function, oxygen levels, exercise capacity and quality of life
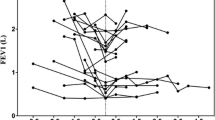
Not surprisingly, in comparison to the pretreatment data, the posttreatment data showed that sirolimus significantly improved pulmonary function (FEV1, FEV1%predicted, FVC, FVC%predicted, FEV1/FVC, DLCO), oxygen levels (PaO2, P(A-a)O2), 6MWD, SGRQ and VEGF-D levels (Table 2). Over a mean duration of 1.4 ± 0.5 years before the beginning of sirolimus therapy, the FEV1 decreased by 178 ± 36 ml per year (7.71% ± 1.20% predicted, P < 0.001), and the FVC decreased by − 72 ± 68 ml per year (− 4.11% ± 1.15% predicted, P < 0.001). In contrast, over a mean of 2.2 ± 1.1 years of sirolimus therapy, the FEV1 changed by − 10 ± 15 ml per year (0.29% ± 0.48%predicted, P > 0.05), and the FVC increased by 54 ± 22 ml per year (2.78% ± 0.72%predicted, P < 0.001).
Pulmonary function changes in patients with chylothorax and those without chylothorax
Forty-eight patients were with chylothorax, and 94 patients were without chylothorax. Pulmonary function data were only available in patients with small amount of pleural effusion. Our data showed that baseline VEGF-D levels were higher in patients with chylothorax, however no significant differences were observed in changes of VEGF-D levels and pulmonary functions in patients with and without chylothorax over 4 years treatment (data not shown). The yearly changes of FEV1 in patients with and without chylothorax were 0.46% ± 0.76% predicted and 0.10% ± 0.60 predicted (P = 0.95), respectively. The yearly change of DLco were − 0.06% ± 0.69% and − 0.45% ± 0.43% predicted (P = 0.92).
Long-term effects of sirolimus at 1, 2, 3 and 4 years
The main aim of the study was to investigate the long-term effects of sirolimus. Using paired comparison, we were able to detect the differences of the measurements from the baseline to 1, 2, 3 and 4 years after the initiation of treatment. As shown in Table 3, the FEV1 improved significantly in the first year, and the FVC improved in the first and second year; then, the significance disappeared during the subsequent follow-up. There were no changes in the diffusion capacity after treatment. Overall, pulmonary function was maintained after the initiation of sirolimus therapy. Sirolimus could potentially stabilize pulmonary function for up to 4 years. The improvements in PaO2, P(A-a)O2, 6MWD, and SGRQ were maintained for 3 years and disappeared in the fourth year (Table 3). No worsening was observed except for in FEV1/FVC during the follow-up period. The decrease in VEGF-D level was maintained for up to 4 years (Table 3). For chylothorax, one patient accepted thoracic duct surgery and sirolimus treatment at the same time and rapidly achieved a complete remission. Among the patients receiving sirolimus treatment without surgery, 35 patients got complete remission, and 12 patients improved.
Dosage of sirolimus
The mean dosage of sirolimus was 1.59 ± 0.50 mg/d (range, 1 to 2 mg/d) at the beginning, and it was 1.27 ± 0.47 mg/d (range, 0.5 to 2 mg/d) after an adjustment period of 1–6 months. Ninety patients accepted the tests of the serum concentration of sirolimus in the first year. The average blood sirolimus level was 7.2 ± 2.6 ng/ml (range, 1.5 to 18.6 ng/ml).
Frequencies of adverse events
The adverse events that occurred in our study during the observation period are listed in Table 4. In the first year, the most frequent adverse events were mouth ulcer (68.2%), menstrual abnormality (57.9%), acne (34.6%), weakness (11%), diarrhea (6%), and peripheral edema (5.6%). During the next 3 years, the common adverse events were mouth ulcer, menstrual abnormality and acne. However, the incidence rate of mouth ulcer, menstrual abnormality and acne reduced to 23.3, 26.7 and 10% in the fourth year. Occurrence of adverse events could reduce over time (Table 4). We did not observe severe adverse events in our follow-up periods. Three patients required the temporary discontinuation of sirolimus therapy due to menstrual abnormalities, and then restarted the therapy after 3 to 6 months. No other patients had to discontinue sirolimus therapy because of adverse events.
Discussion
Whether the efficacy of sirolimus can be maintained during long-term treatment is a critical question. We partially answered this question in the present study. We found improvements of sirolimus in the following parameters in patients after beginning sirolimus treatment: the FEV1 in the first year; the FVC in the first and second year; arterial oxygen levels, exercise capacity and quality of life in the first, second and third year; and the VEGF-D levels in all 4 years. An encouraging finding was that most measurements improved or stabilized during 4-year observations after sirolimus treatment.
Current clinical trials usually observed 12–24 months of sirolimus treatment. Several studies included observations over 2 years. In studies with 2–4 years observation, the increase in the FEV1 varied from 11 ml/year to 50 ml/year after starting sirolimus treatment [6, 7, 10,11,12]. In a 4-year prospective study, the mean change in the FEV1 in patients not receiving sirolimus was -70 ml /year (n = 66), while the mean change in patients receiving sirolimus was 7 ml/year (n = 23) [10]. Taveira-DaSilva et al. [9] observed 25 patients for 4.5 years, and the FEV1 and DLCO changed slightly. The change of FEV1 was − 10 ml/year (P = 0.53) and the FVC increased by 54 ml/year (P = 0.016) in our study. In the paired comparison analysis, we found that the FEV1 benefited most from sirolimus in the first year, and the FVC benefited in the first 2 years. No significant reduction in pulmonary function was observed over the 4 years. The efficacy of sirolimus can be maintained for at least 4 years.
Higher VEGF-D levels were observed more frequently in patients with lymphatic disease who presented with chylous pleural effusion or ascites than in patients without lymphatic involvement [17]. Several studies reported that compared with patients without lymphatic disease, patients with lymphatic involvement may experience a great improvement in pulmonary function after starting sirolimus therapy [7, 9]. Taveira-DaSilva et al. [9] observed that the effects of sirolimus on VEGF-D levels and DLCO were especially marked in patients with LAM with lymphatic involvement than those without lymphatic involvement. For patients with or without limited small amount of chylothorax, improvement of pulmonary function was similar.
The safety profile is satisfactory. Patients tolerated sirolimus treatment very well. The rate of adverse effects decreased during the follow-up. We also analyzed the group of patients who were followed up for 3 and 4 years, the rate of adverse effects were decreased over time (data not shown).
Anyway, we still need to be cautious in observing long-term adverse effects from the treatment. LAM patients use sirolimus for many years, and it is important to monitor their progress and safety data regularly, at least once a year. Novel therapies for LAM are urgently needed for use when sirolimus cannot be used because of insensitivity or resistance of sirolimus.
The limitations of this study include its retrospective nature and the limited sample size during observation, as only 32 patients had data for all 4 years. Beginning in 2016, a national LAM registry in China was planned that will recruit 800 LAM patients and conduct yearly follow-up. We hope that some unanswered questions will be clarified in future studies.
In conclusion, sirolimus therapy is effective at improving or stabilizing pulmonary function, oxygen levels, exercise capacity, and quality of life in patients with LAM for up to 4 years. VEGF-D maintained at lower level for 4 years after the initiation of treatment. Adverse events related to sirolimus was mild during the follow-up period.
Availability of data and materials
The datasets used and analysed during the current study area available from the corresponding author.
Abbreviations
- %pred:
-
% predicted
- 6MWD:
-
6-min walking distance
- ATS:
-
American Thoracic Society
- DLCO:
-
Diffusion capacity for carbon monoxide
- ERS:
-
European Respiratory Society
- FEV1 :
-
Forced expiratory volume in 1 s
- FVC:
-
Forced vital capacity
- LAM:
-
Lymphangioleiomyomatosis
- P(A-a)O2 :
-
Alveolar-arterial oxygen gradient
- PaO2 :
-
Partial pressure of oxygen in arterial blood
- RV:
-
Residual volume
- SGRQ:
-
St. George’s Respiratory Questionnaire
- TLC:
-
Total lung capacity
- VEGF-D:
-
Vascular endothelial growth factor-D
References
Johnson SR, Taveira-DaSilva AM, Moss J. Lymphangioleiomyomatosis. Clin Chest Med. 2016;37(3):389–403.
Harari S, Torre O, Cassandro R, Moss J. The changing face of a rare disease: lymphangioleiomyomatosis. Eur Respir J. 2015;46(5):1471–85.
Henske EP, McCormack FX. Lymphangioleiomyomatosis - a wolf in sheep’s clothing. J Clin Invest. 2012;122(11):3807–16.
McCormack FX, Inoue Y, Moss J, Singer LG, Strange C, Nakata K, et al. Efficacy and safety of sirolimus in lymphangioleiomyomatosis. N Engl J Med. 2011;364(17):1595–606.
McCormack FX, Gupta N, Finlay GR, Young LR, Taveira-DaSilva AM, Glasgow CG, et al. Official American Thoracic Society/Japanese respiratory society clinical practice guidelines: Lymphangioleiomyomatosis diagnosis and management. Am J Respir Crit Care Med. 2016;194(6):748–61.
Zhan Y, Shen L, Xu W, Wu X, Zhang W, Wang J, et al. Functional improvements in patients with lymphangioleiomyomatosis after sirolimus: an observational study. Orphanet J Rare Dis. 2018;13(1):34.
Taveira-DaSilva AM, Hathaway O, Stylianou M, Moss J. Changes in lung function and chylous effusions in patients with lymphangioleiomyomatosis treated with sirolimus. Ann Intern Med. 2011;154(12):797–805 W-292-3.
Taveira-DaSilva AM, Jones AM, Julien-Williams PA, Stylianou M, Moss J. Retrospective review of combined sirolimus and simvastatin therapy in lymphangioleiomyomatosis. Chest. 2015;147(1):180–7.
Taveira-DaSilva AM, Jones AM, Julien-Williams P, Stylianou M, Moss J. Long-term effect of Sirolimus on serum vascular endothelial growth factor D levels in patients with Lymphangioleiomyomatosis. Chest. 2018;153(1):124–32.
Bee J, Bhatt R, McCafferty I, Johnson SR. A 4-year prospective evaluation of protocols to improve clinical outcomes for patients with lymphangioleiomyomatosis in a national clinical Centre. Thorax. 2015;70(12):1202–4.
Bee J, Fuller S, Miller S, Johnson SR. Lung function response and side effects to rapamycin for lymphangioleiomyomatosis: a prospective national cohort study. Thorax. 2018;73(4):369–75.
Yao J, Taveira-DaSilva AM, Jones AM, Julien-Williams P, Stylianou M, Moss J. Sustained effects of sirolimus on lung function and cystic lung lesions in lymphangioleiomyomatosis. Am J Respir Crit Care Med. 2014;190(11):1273–82.
Gupta N, Finlay GA, Kotloff RM, Strange C, Wilson KC, Young LR, et al. Lymphangioleiomyomatosis diagnosis and management: high-resolution chest computed tomography, Transbronchial lung biopsy, and pleural disease management. An official American Thoracic Society/Japanese respiratory society clinical practice guideline. Am J Respir Crit Care Med. 2017;196(10):1337–48.
Wanger J, Clausen JL, Coates A, Pedersen OF, Brusasco V, Burgos F, et al. Standardisation of the measurement of lung volumes. Eur Respir J. 2005;26(3):511–22.
ATS Committee on Profiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111–7.
Avila NA, Dwyer AJ, Rabel A, Moss J. Sporadic lymphangioleiomyomatosis and tuberous sclerosis complex with lymphangioleiomyomatosis: comparison of CT features. Radiology. 2007;242(1):277–85.
Glasgow CG, Avila NA, Lin JP, Stylianou MP, Moss J. Serum vascular endothelial growth factor-D levels in patients with lymphangioleiomyomatosis reflect lymphatic involvement. Chest. 2009;135(5):1293–300.
Acknowledgements
We thank Professor Feng Chen and Dr. Lijuan Lin from Nanjing Medical University for statistical assistance.
Funding
This work was supported by the National Nature Science Foundation of China (81570061), the National Key Research and Development Program of China (2016YFC0901502), and Chinese Academy of Medical Sciences (CAMS) Initiative for Innovative Medicine (2017-12 M-2-001).
Author information
Authors and Affiliations
Contributions
SH: study design, data analysis and manuscript writing. XW: study design, data analysis. WX: study design, data analysis. XT: clinical evaluation of the patients. YY: clinical evaluation of the patients. STW: clinical evaluation of the patients. SL: data analysis. XX: data analysis. KFX: design, clinical evaluation of the patients, data analysis, and manuscript writing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was part of LAM registry study of Peking Union Medical College Hospital (S-379). The protocol of this study was approved by the Ethical Committee of Peking Union Medical College Hospital (S-K709). All subjects included in this study signed informed consent documents.
Consent for publication
Consent for publication was obtained from all participants.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Hu, S., Wu, X., Xu, W. et al. Long-term efficacy and safety of sirolimus therapy in patients with lymphangioleiomyomatosis. Orphanet J Rare Dis 14, 206 (2019). https://doi.org/10.1186/s13023-019-1178-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13023-019-1178-2