
Abstract
Background
Lymphangioleiomyomatosis (LAM) is a rare multisystemic disorder with various clinical manifestations. Despite the recognition of several prognostic factors, the long-term clinical course and prognosis of patients with LAM in the era of sirolimus therapy are not established.
Methods
The clinical data of 104 patients with LAM were retrospectively analyzed. Death or lung transplantation was defined as the primary outcome. Disease progression (DP) was defined as a 10% absolute decline in forced expiratory volume in one second (FEV1).
Results
The mean age of all patients was 40.3 years. Over a median follow-up period of 7.1 years, of all patients, 6.7% died and 1.9% underwent lung transplantation, while of 92 patients with serial lung function data, 35.9% experienced DP. The 5-year and 10-year overall survival rates were 93.0% and 90.9%, respectively. The multivariable Cox analysis revealed that older age (hazard ratio [HR]: 1.136, P = 0.025), lower FEV1 (HR: 0.956, P = 0.026) or diffusing capacity for carbon monoxide (HR: 0.914, P = 0.003), and shorter distance during the 6-min walk test (HR: 0.993, P = 0.020) were independent prognostic factors for mortality. A propensity score-matched comparative analysis performed between patients who received sirolimus therapy and those who did not, found no differences in survival, DP, complications, and lung function decline rate.
Conclusions
Over a follow-up period of approximately 7 years, one-tenth of all patients experienced death, while one-third experienced DP. Older age, lower lung function, and reduced exercise capacity were associated with a poor prognosis in patients with LAM.
Similar content being viewed by others


Background
Lymphangioleiomyomatosis (LAM) is a rare multisystemic disorder which mainly affects women of childbearing age [1, 2]. The clinical course of LAM is heterogenous, with a reported 10-year survival rate of 80–90% [3,4,5,6]. A study including 401 patients with LAM showed that the 10-year transplant-free survival rate was 86% [3]. Another study conducted on 217 patients with LAM, also reported 5-year and 10-year transplant-free survival rates of 94% and 85%, respectively [5]. Moreover, the 5-year and 10-year survival rates of 173 Japanese patients with LAM were 91% and 76%, respectively [6]. Patients with LAM experience dyspnea and a progressive decline in lung function, both of which eventually result in the need for lung transplantation. Johnson et al. found that the median time from symptom onset to grade 3 dyspnea according to the Medical Research Council Dyspnea Scale, was 9.3 years in patients from the United Kingdom (UK) with LAM (n = 72) [4].
Several prognostic factors in patients with LAM have been reported in previous studies [3, 5,6,7,8]. In a previous study, lower FEV1 and diffusing lung capacity for carbon monoxide (DLCO) were found to be poor prognostic factors for transplantation-free survival in the age-adjusted Cox analysis [5]. Of a total of 46 Japanese patients with LAM, the non-survivors were found to have a lower forced expiratory volume in one second/forced vital capacity (FEV1/FVC) ratio and a higher total lung capacity (TLC) than the survivors [7]. Moreover, delayed symptom onset and the presence of angiomyolipoma (AML) were associated with better survival in patients with LAM, whereas home oxygen use was associated with poorer survival [3]. However, the long-term clinical course and prognostic factors of LAM in the era of sirolimus therapy which has been recently introduced to the standard treatment, are not well defined. Moreover, the effect of sirolimus on the survival of patients with LAM in a real-world setting has not been investigated. This study aimed to evaluate the long-term clinical course, prognostic factors, and impact of sirolimus on the prognosis of patients with LAM.
Study design and methods
Study population
Of a total of 106 patients who were diagnosed with LAM between July 2001 and February 2020 at Asan Medical Center, Seoul, Republic of Korea, 104 patients whose baseline data were available, were included in this study (Fig. 1). All patients met the diagnostic criteria of definite LAM according to An Official American Thoracic Society/Japanese Respiratory Society Clinical Practice Guideline [1]. Of all the included cases, 60.6% were biopsy-proven through surgical lung biopsy (48.1%), transbronchial lung biopsy (9.6%), or biopsy of other sites including the retroperitoneum and lymph nodes (2.9%). The study protocol was approved by the Institutional Review Board of Asan Medical Center (2016-0480). Informed consent was not deemed necessary owing to the retrospective nature of the study.

Flow chart of the patient selection. LAM lymphangioleiomyomatosis, PS propensity score
Clinical data
The clinical and survival data of all patients were retrospectively collected from medical records, telephone interviews, and records from the National Health Insurance of South Korea. Spirometry and measurement of DLCO and TLC were performed according to the recommendations of the ATS and European Respiratory Society [9,10,11]; and the results are expressed as a percentage of the normal predicted values. The 6-min walk test (6MWT) was performed based on the ATS guidelines [12].
Records of follow-up visits which took place every 3–6 months, and hospitalization were reviewed to identify the development of complications such as disease progression (DP) and extrapulmonary involvement. DP was defined as a 10% absolute decline in FEV1 from baseline values.
Statistical analysis
Continuous variables are expressed as mean ± standard deviation, while categorical variables are expressed as percentages. The student’s t-test or the Mann–Whitney U test was used to analyze continuous data, whereas the Pearson’s chi-square test or Fisher’s exact test was used to analyze categorical data. Death was defined as the primary outcome, and lung transplantation was considered an equivalent outcome to death. The Cox regression model was used to identify the prognostic factors for survival and variables with P < 0.1 in the unadjusted analysis were incorporated in the multivariable model using backward elimination. Survival was evaluated using the Kaplan–Meier survival analysis and the log-rank test. The availability of serial lung function data (≥ 3 measurements) in 92 patients enabled the calculation of the annual rate (slope) of decline in lung function using a linear regression model.
All patients were divided into two (sirolimus and non-sirolimus) groups according to whether or not they received sirolimus therapy, to evaluate its effect on the clinical outcome of patients with LAM. The index date was set as the date of the first prescription of sirolimus in the sirolimus group and the date of LAM diagnosis in the non-sirolimus group. Patients were observed from the index date until the occurrence of the study outcome or until the end of the observation period (April 30, 2020), whichever took place earlier. Propensity score matching (1:1) to adjust for the differences in baseline characteristics between the sirolomus and non-sirolimus groups, yielded 22 matched pairs (Fig. 1). The matched variables consisted of age, history of smoking, FEV1, and DLCO; propensity scores were calculated using the multiple logistic regression analysis to estimate the probability of receiving sirolimus therapy in each patient. All statistical analyses were performed using the SPSS software version 23.0 (IBM Inc., Chicago, IL, USA). All P-values were two-tailed, and P-values < 0.05 were considered statistically significant.
Results
Baseline characteristics at diagnosis
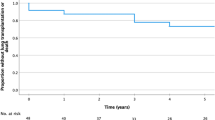
Among all patients, the mean age was 40.3 years, 9.6% were ever-smokers, and 12.5% were diagnosed with tuberous sclerosis complex (TSC) (Table 1). During follow-up (median: 7.1 years, interquartile range: 2.8–9.9 years), seven (6.7%) patients died, and two patients (1.9%) underwent lung transplantation. The 5-year and 10-year survival rates were 93.0% and 90.9%, respectively (Fig. 2A). The non-survivors had lower lung function as manifested by FEV1, DLCO and FEV1/FVC, higher values of residual volume (RV), and poorer exercise capacity as shown by the distance and the lowest oxygen saturation (SpO2) during the 6MWT, than the survivors (Table 1). However, there were no significant differences in the incidence of pneumothorax and extrapulmonary manifestations. Sirolimus was administered to 59.6% of patients, and no significant difference in the treatment received was observed between the non-survivors and survivors.

Kaplan–Meier curves for overall survival and disease progression in patients with LAM. A Survival curve for overall survival. B Survival curve for disease progression. LAM lymphangioleiomyomatosis
Clinical course
During follow-up, 33 patients (35.9% of the patients with serial lung function data [≥ 3 measurements; n = 92]) experienced DP (Table 2). The 5-year and 10-year progression-free survival rates were 61.2% and 56.2%, respectively (Fig. 2B). Among the complications detected after the diagnosis of LAM, pneumothorax and angiomyolipoma (AML) were the most common (in each 2.9%), followed by chylothorax (1.9%) (Table 2). Analysis of the serial lung function data (n = 92), revealed a mean annual decline rate in FEV1, FVC, and DLCO of − 0.7 ± 4.2% predicted/year, 0.3 ± 3.2% predicted/year, and 1.5 ± 4.0% predicted/year, respectively (Table 2).
No significant differences in the development of complications (pneumothorax, chylothorax, and extrapulmonary manifestations) after the diagnosis of LAM, DP, and lung function decline rate were noted between the non-survivors and survivors (Table 2).
Risk factors for mortality
The unadjusted Cox analysis demonstrated that lower lung function (FEV1, FVC, DLCO, TLC, FEV1/FVC, and FEF25–75% [forced expiratory flow between 25 and 75% of FVC]) and poorer exercise capacity (distance and the lowest SpO2 during the 6MWT) were associated with mortality in patients with LAM (Table 3). Due to the close correlation between FEV1 and DLCO (r = 0.705), we developed two multivariable models with each including either FEV1 or DLCO. The multivariable model including age, FEV1, 6-min walk distance (6MWD), and lowest SpO2 during the 6MWT showed that older age (hazard ratio [HR]: 1.136, 95% confidence interval [CI]: 1.016–1.269, P = 0.025), lower FEV1 (HR: 0.956, 95% CI: 0.919–0.995, P = 0.026), and shorter 6MWD (HR: 0.993, 95% CI: 0.987–0.999, P = 0.020) were independent prognostic factors for mortality in patients with LAM. The other multivariable model including age, DLCO, 6WMD, and lowest SpO2 during the 6MWT showed that older age (HR: 1.167, 95% CI: 1.036–1.314, P = 0.011), and lower DLCO (HR: 0.914, 95% CI: 0.861–0.969, P = 0.003) were also risk factors for mortality.
Effects of sirolimus therapy
In the unmatched analysis, patients treated with sirolimus were younger, had a higher incidence of lymphangioleiomyoma, lower lung function (FEV1, DLCO, FEV1/FVC, and FEF25-75%), and poorer exercise capacity (distance and lowest SpO2 during the 6MWT) than those who did not receive sirolimus therapy (Additional file 1: Table S1). Propensity score matching that was performed to adjust for these differences generated 22 matched pairs (Table 4). The baseline characteristics of the patients in the matched cohort and those in the unmatched one are displayed in Additional file 1: Table S2. The unmatched patients had a higher incidence of lymphangioleiomyoma and a shorter distance during the 6MWT. Additionally, the lowest SpO2 during the 6MWT was inferior in the unmatched patients compared with the matched ones.
Among the matched patients, the mean age was 40.7 years and TSC was diagnosed in 11.4% patients. The median follow-up duration was 7.1 years (8.5 years in the sirolimus group versus 6.1 years in the non-sirolimus group, P = 0.213). Additionally, the median time from diagnosis to the start of sirolimus therapy was 1.8 (interquartile range: 0.2–3.8) years, and the median duration of sirolimus therapy was 4.5 (interquartile range: 1.5–6.0) years. Although the sirolimus group showed lower the minimum SpO2 during the 6MWT than the non-sirolimus group (Table 4), there were no differences in survival, DP, and lung function decline rate between the two groups (Table 5). Moreover, in the Kaplan–Meier survival analysis, there was a tendency of better survival in the sirolimus group than that in the no-sirolimus group (P = 0.073) (Additional file 1: Fig. S1).
Discussion
This study reported the long-term clinical course and prognostic factors of patients with LAM. The 10-year survival and progression-free survival rates were 90.9% and 56.2%, respectively. Older age, lower FEV1 and DLCO, and shorter 6MWD were independent prognostic factors for overall survival in patients with LAM.
In our study, the prognosis of patients with LAM was better than that reported previously [3, 4, 13, 14]. The studies published in the 2000s (n = 57–105) demonstrated a mortality rate of 10–20% after symptom onset during median follow-up period of 4.5–12.6 years [4, 14]. Oprescu et al. reported a 10-year transplantation-free survival of 86% in 410 patients with LAM who were followed up over a median time period of 10.4 years until 2007 [3]. Gupta et al., who observed 217 patients with LAM until 2014, also demonstrated 5-year and 10-year transplantation-free survival rates of 94% and 85%, respectively [5]. Having followed up patients with LAM until April 2020, we found a higher 10-year transplantation-free survival rate of 90.9%. The better survival of patients in our study might be attributed to improved management of patients with LAM, and more widespread access to chest computed tomography imaging for screening purposes in South Korea, which could have led to earlier diagnosis of LAM.
Our study revealed that older age and lower lung function (FEV1 or DLCO) were independent prognostic factors for mortality in patients with LAM. The prognostic factors in patients with LAM have been previously reported [3, 5,6,7]. The age-adjusted multivariable Cox analysis performed by Gupta et al. revealed that lower FEV1 (HR: 0.97, 95% CI: 0.96–0.99, P = 0.008) and DLCO (HR: 0.97, 95% CI: 0.95–0.99, P = 0.001) were independent risk factors for transplantation-free survival [5]. The multivariable Cox analysis conducted by Oprescu et al., also showed that late symptom onset after diagnosis (HR: 0.80, 95% CI: 0.64–0.99, P = 0.043), and the presence of AML (HR: 0.49, 95% CI: 0.30–0.79, P = 0.004) were associated with a lower risk of death or transplantation, while home oxygen use (HR: 3.13, 95% CI: 1.90–5.18, P < 0.001) was associated with poor prognosis [3]. These findings support our results which have shown an association between higher disease severity and poor prognosis. On the other hand, Kitaichi et al. revealed that a lower FEV1/FVC ratio and a higher TLC were associated with poor prognosis in a study performed on 46 patients with LAM [7]. These findings are also consistent with our results; lower FEV1/FVC and increased TLC were associated with a higher risk of mortality in the unadjusted analysis. The lower FEV1/FVC ratio reflects airflow limitation [15], while an increase in TLC indicates hyperinflation of the lungs due to air trapping [16] in obstructive lung disease.
After propensity score matching for age, smoking status, and lung function, no significant differences in clinical outcome and lung function decline rate were found between the sirolimus and non-sirolimus groups. However, these results actually suggest the presence of clinical benefits with sirolimus therapy in patients with LAM, since the sirolimus group included patients with more advanced disease (lower the minimum SpO2 during 6MWT). The efficacy of sirolimus in the stabilization of lung function has been demonstrated by real-world studies [17,18,19,20]. In a study performed on 98 Chinese patients with LAM, Zhan et al., showed an improvement in FEV1 decline (n = 18; − 31.1 ± 30.8 [pre-sirolimus] versus 16.1 ± 36.0 mL/month [post-sirolimus], P = 0.002), 6MWD (n = 46; 358.8 ± 114.4 versus 415.6 ± 118.6 m, P = 0.004), and arterial blood oxygen tension (n = 17; − 0.55 ± 0.60 versus 0.30 ± 1.19 mmHg/month, P = 0.018) [17]. Bee et al. also demonstrated an improvement in FEV1 after sirolimus therapy (− 150 versus 35 mL/year, n = 21, P < 0.001) in a prospective national cohort study conducted on 47 patients with LAM in the UK [18]. Through the Multicenter International Lymphangioleiomyomatosis Efficacy of Sirolimus trial, Gupta et al. demonstrated that sirolimus therapy stabilized FEV1 decline regardless of clinical features including menopausal status, baseline FEV1, and co-existing TSC [20]. Despite the lack of statistical significance, the rate of FEV1 decline in the sirolimus group was numerically lower (0.5 versus − 0.3% predicted/year) than that in the non-sirolimus group in our study.
Our study had a few limitations. First, the generalizability of our results could be limited by the single-centered and retrospective nature of the study. Nonetheless, the baseline characteristics of our patients were similar to those of previous studies [21]. Second, the small number of patients analyzed (the non-survivors and the matched patients) could account for the lack of statistical significance. However, our analyses suggested prognostic factors consistent with previous studies [3, 5,6,7]. Third, the patients were enrolled over a long period of time. Standards of care for patients with LAM might have evolved over time. However, despite these limitations, the strengths of our study include its long-term follow-up period and the determination of prognostic factors based on various clinical variables.
Conclusion
During long-term follow-up of about 7 years, a tenth, and a third of patients with LAM experienced death or DP. Our results suggest that older age, lower lung function, and poorer exercise capacity mean poor prognosis in patients with LAM.
Availability of data and materials
Any data generated and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- DLCO:
-
Diffusing capacity of the lung for carbon monoxide
- DP:
-
Disease progression
- FEV1 :
-
Forced expiratory volume in one second
- FVC:
-
Forced vital capacity
- LAM:
-
Lymphangioleiomyomatosis
- SpO2 :
-
Oxygen saturation
- TLC:
-
Total lung capacity
- TSC:
-
Tuberous sclerosis complex
- 6MWD:
-
6-Minute walk distance
- 6MWT:
-
6-Minute walk test
References
Gupta N, Finlay GA, Kotloff RM, Strange C, Wilson KC, Young LR, Taveira-DaSilva AM, Johnson SR, Cottin V, Sahn SA, et al. Lymphangioleiomyomatosis Diagnosis and Management: High-Resolution Chest Computed Tomography, Transbronchial Lung Biopsy, and Pleural Disease Management. An Official American Thoracic Society/Japanese Respiratory Society Clinical Practice Guideline. Am J Respir Crit Care Med. 2017;196:1337–48.
Harari S, Torre O, Moss J. Lymphangioleiomyomatosis: what do we know and what are we looking for? Eur Respir Rev. 2011;20:34–44.
Oprescu N, McCormack FX, Byrnes S, Kinder BW. Clinical predictors of mortality and cause of death in lymphangioleiomyomatosis: a population-based registry. Lung. 2013;191:35–42.
Johnson SR, Whale CI, Hubbard RB, Lewis SA, Tattersfield AE. Survival and disease progression in UK patients with lymphangioleiomyomatosis. Thorax. 2004;59:800–3.
Gupta N, Lee HS, Ryu JH, Taveira-DaSilva AM, Beck GJ, Lee JC, McCarthy K, Finlay GA, Brown KK, Ruoss SJ, et al. The NHLBI LAM registry: prognostic physiologic and radiologic biomarkers emerge from a 15-year prospective longitudinal analysis. Chest. 2019;155:288–96.
Hayashida M, Seyama K, Inoue Y, Fujimoto K, Kubo K. The epidemiology of lymphangioleiomyomatosis in Japan: a nationwide cross-sectional study of presenting features and prognostic factors. Respirology. 2007;12:523–30.
Kitaichi M, Nishimura K, Itoh H, Izumi T. Pulmonary lymphangioleiomyomatosis: a report of 46 patients including a clinicopathologic study of prognostic factors. Am J Respir Crit Care Med. 1995;151:527–33.
Taveira-DaSilva AM, Stylianou MP, Hedin CJ, Hathaway O, Moss J. Decline in lung function in patients with lymphangioleiomyomatosis treated with or without progesterone. Chest. 2004;126:1867–74.
Wanger J, Clausen JL, Coates A, Pedersen OF, Brusasco V, Burgos F, Casaburi R, Crapo R, Enright P, van der Grinten CP, et al. Standardisation of the measurement of lung volumes. Eur Respir J. 2005;26:511–22.
Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, Crapo R, Enright P, van der Grinten CP, Gustafsson P, et al. Standardisation of spirometry. Eur Respir J. 2005;26:319–38.
Macintyre N, Crapo RO, Viegi G, Johnson DC, van der Grinten CP, Brusasco V, Burgos F, Casaburi R, Coates A, Enright P, et al. Standardisation of the single-breath determination of carbon monoxide uptake in the lung. Eur Respir J. 2005;26:720–35.
Holland AE, Spruit MA, Troosters T, Puhan MA, Pepin V, Saey D, McCormack MC, Carlin BW, Sciurba FC, Pitta F, et al. An official European Respiratory Society/American Thoracic Society technical standard: field walking tests in chronic respiratory disease. Eur Respir J. 2014;44:1428–46.
Carrington CB, Cugell DW, Gaensler EA, Marks A, Redding RA, Schaaf JT, Tomasian A. Lymphangioleiomyomatosis: physiologic-pathologic-radiologic correlations. Am Rev Respir Dis. 1977;116:977–95.
Matsui K, Beasley MB, Nelson WK, Barnes PM, Bechtle J, Falk R, Ferrans VJ, Moss J, Travis WD. Prognostic significance of pulmonary lymphangioleiomyomatosis histologic score. Am J Surg Pathol. 2001;25:479–84.
Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. Am J Respir Crit Care Med. 2001;163:1256–76.
O’Donnell DE, Laveneziana P. Physiology and consequences of lung hyperinflation in COPD. Eur Respir Rev. 2006;15:61–7.
Zhan Y, Shen L, Xu W, Wu X, Zhang W, Wang J, Li X, Yang Y, Tian X, Xu KF. Functional improvements in patients with lymphangioleiomyomatosis after sirolimus: an observational study. Orphanet J Rare Dis. 2018;13:34.
Bee J, Fuller S, Miller S, Johnson SR. Lung function response and side effects to rapamycin for lymphangioleiomyomatosis: a prospective national cohort study. Thorax. 2018;73:369–75.
Taveira-DaSilva AM, Hathaway O, Stylianou M, Moss J. Changes in lung function and chylous effusions in patients with lymphangioleiomyomatosis treated with sirolimus. Ann Intern Med. 2011;154:797–805.
Gupta N, Lee HS, Young LR, Strange C, Moss J, Singer LG, Nakata K, Barker AF, Chapman JT, Brantly ML, et al. Analysis of the MILES cohort reveals determinants of disease progression and treatment response in lymphangioleiomyomatosis. Eur Respir J. 2019; 53.
Harknett EC, Chang WY, Byrnes S, Johnson J, Lazor R, Cohen MM, Gray B, Geiling S, Telford H, Tattersfield AE, et al. Use of variability in national and regional data to estimate the prevalence of lymphangioleiomyomatosis. QJM. 2011;104:971–9.
Acknowledgements
We would like to express our deep gratitude to Mynkyu Han (statistician, Asan Medical Center) for his valuable advice on the statistical analysis.
Funding
This study was supported by a Grant from the Basic Science Research Program (NRF-2019R1A2C2008541, NRF-2022R1A2B5B02001602) and the Bio & Medical Technology Development Program (NRF-2022M3A9E4082647) of the National Research Foundation of Korea (NRF) funded by the Ministry of Science & ICT, Republic of Korea.
Author information
Authors and Affiliations
Contributions
JWS takes full responsibility for the content of this manuscript, including its data and analysis. JWS made substantial contributions to the conception and design of the study. HYY, HK and JWS made substantial contributions to the analysis and interpretation of the data. HYY, HK and JWS drafted the initial manuscript. All authors discussed the results and reviewed the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Institutional Review Board of Asan Medical Center (2016-0480). Informed consent was not deemed necessary owing to the retrospective nature of the study.
Consent for publications
Not applicable.
Competing interests
The authors declare that they have no conflicts of interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1.
Comparison of baseline characteristics between the sirolimus and non-sirolimus groups among patients with LAM. Table S2. Comparison of baseline characteristics between propensity score-matched and unmatched groups among patients with LAM. Figure S1. Comparison of survival curves between the sirolimus and non-sirolimus groups among the matched patients with LAM.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yoon, HY., Kim, H.J. & Song, J.W. Long-term clinical course and outcomes in patients with lymphangioleiomyomatosis. Respir Res 23, 158 (2022). https://doi.org/10.1186/s12931-022-02079-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12931-022-02079-6