
Abstract
A portable “diagnostic electronic nose” was used to study the composition of a mixture of volatile compounds emitted by the skin of the forearms in children with obesity and other associated metabolic disorders. Differences and features of the profiles of volatile compounds (primarily organic) of the skin on the left and right forearms in children with obesity and the dependence of the profile on food intake, drugs, concomitant diseases, and body characteristics were evaluated in hospital environment. More than 300 patient profiles were analyzed for 2 years, including the dynamics in profiles during repeated planned hospitalizations. The results suggest that the composition of the gas mixture of compounds emitted by the skin on the forearms can be analyzed and compared without preliminary separation or selection using an array of eight piezoelectric sensors of the “diagnostic electronic nose” device. We measured a correlation between the electronic nose data and the results of standard clinical laboratory tests. The parameters of a sensor array and clinical studies are closely related to each other in the levels of urea, alkaline phosphatase, and glucose. An approach based on scanning a volatile skin profile on the forearm for 3–6 min helps to rank children with obesity into groups associated with the socially significant diseases and conditions: “Normal,” “Obesity with a risk of development of type 2 diabetes mellitus,” and “Type 1 diabetes mellitus.” Using chemometric methods, we optimized the analytical procedure and specified research conditions and control points. The composition of the volatile skin metabolome on the right forearm, scanned on an empty stomach, is the most informative. The accuracy of the difference between the problem groups and the norm is 100%; the accuracy of the rank within pathological groups is 80%. The proportion of false assignments increases in the presence of inflammation in a body of any type. The potentials of the procedure were evaluated in a hospital environment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The World Health Organization (WHO) estimates that more than a billion people in the world are overweight. The problem of obesity is relevant even in countries where a large part of the population is constantly starving, and in industrialized countries, it has long been a serious aspect of public health [1]. The diagnosis of obesity combines hereditary and acquired diseases associated with the excessive accumulation of adipose tissue in a body. Being overweight and obese in children and young adults are major risk factors for chronic disease and are associated with an increased risk of obesity in adults [2] and premature mortality [3, 4]. The World Health Organization recognizes that childhood overweight and obesity have reached epidemic proportions in most industrialized countries [5].
According to a report by the WHO European Childhood Obesity Surveillance Initiative (COSI) group [6] on the trends in the development of overweight and obesity in primary school children, a sedentary lifestyle is the main cause of obesity. However, another reason for obesity lies in the presence of complex metabolic disorders in a body, leading to the accumulation and deposition of excess fat [7]. Many years of research around the world have established that several dangerous diseases can develop against the background of obesity, such as type 2 diabetes, cardiovascular diseases, diseases of the liver, biliary tract, and colon, and esophagus pathology. Since the 1980s, various methods have been developed for assessing the expectation and prediction of obesity in the population, starting from infancy [8]. The last 2 years are distinguished by an objective decrease in the activity of the population and an increased risk of weight gain due to stress and uncertainty about the future. In this regard, the urgency of the rapid identification of risk groups for children with the development of obesity due to metabolic disorders and their differentiation from weight disorders due to reduced mobility increases. It is essential to provide local pediatricians with affordable means and methods for recognizing the causes and risk groups, although such developments are also of interest for endocrinological hospitals for the earlier identification of risk groups with the selection of the right way to treat and prevent the development of socially significant diseases.
The social significance of the problem of obesity is determined by the threat of disability in young patients and a decrease in overall life expectancy due to the frequent and early development of severe complications.
We can distinguish neurogenic, endocrine, and metabolic mechanisms of obesity. Endocrine mechanisms of obesity include leptin, hypothyroid, adrenal, and insulin mechanisms. The insulin mechanism develops as a result of the direct activation of lipogenesis in adipose tissue by insulin [9]. It is believed that the main damage in this type of obesity is at the level of target cells. They are associated with a decrease in the number of insulin receptors, which leads to insulin resistance and compensatory hyperinsulinism [10].
Biochemical studies recommended for all obese patients include blood lipid profile and enzyme levels (ALT, AST) in combination with the ultrasound examination of the liver. To diagnose lipid metabolism disorders, the levels of total cholesterol, high-density and low-density lipoproteins, and triglycerides in the blood are determined. The determination of liver enzymes (ALT and AST) in combination with liver ultrasound examination is recommended for all obese patients for screening for nonalcoholic fatty liver disease. 25–45% of adolescents with obesity have fatty hepatitis; liver damage can also progress with the duration of obesity, leading to steatohepatitis, fibrosis, or cirrhosis [11]. A study of the prevalence of dyslipidemia in children with insulin-dependent diabetes mellitus (IDDM) and its association with glycemic control showed that circulating lipid abnormalities are common in young people with IDDM but largely disappear when blood glucose levels are reasonably controlled [12].
Thus, the development of affordable and rapid noninvasive methods for diagnosing the condition can significantly narrow the search for problems in the early stages of diagnosis and accelerate the treatment process. One of these methods can be the diagnostics of released compounds, the chemical profile of volatile biomolecules.
The metabolome, or metabolic profile, is a collection of all low-molecular-weight metabolites (<1500 Da) of a biological sample, being a unique chemical “fingerprint” specific to the processes occurring in living cells [13].
Metabolic profile studies are usually performed using a hybrid method of analysis, that is, a combination of gas or liquid chromatography, mass spectrometry, and nuclear magnetic resonance spectrometry. These methods have some limitations: high cost and bulkiness of instrumentation, the need in attracting highly qualified personnel, and the cost of ensuring the working condition. An alternative solution could be the use of the electronic nose as a promising diagnostic tool of the future.
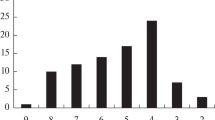
The dynamics of changes in the number of publications on using the electronic nose in diagnostics show a significant increase in the interest in this topic over the past 20 years (Fig. 1a).

(a) Number of publications on the use of electronic nose systems in diagnostics and (b) diseases that can be diagnosed with their help.
Such biosamples as exhaled air, urine, blood, sweat, saliva, and cervical mucus are already analyzed today using an electronic nose [14–18]. Analyzing the sample data, experts mainly diagnose diseases of the gastrointestinal tract, cancerous tumors, respiratory diseases, and other inflammatory diseases (Fig. 1b) [19–22].
Diagnostics of the human condition by volatile compounds are based on the registration of state markers by sensors. Table 1 shows some markers of pathological processes in a body, which can be determined with a high probability when excreted by skin, the largest and constantly functioning excretory organ.
Studying the mixture of gases emitted by the skin can make the diagnosis completely noninvasive and almost instantaneous. Based on all of the above, a new analytical solution is required that can distinguish, in a short time at a specialist’s appointment, whether the patient’s obesity is associated with initial endocrine disorders, or whether it is associated to a greater extent with improper dietary and dynamic behavior. The basis for the development of such an approach can be the use of gas sensors to determine the presence or absence of volatile markers of pathogenic processes in a human body, and detect or record an individual gas profile with the indication of deviations in it associated with metabolic disorders.
The aim of this work is to develop a method for studying the volatile metabolic profile in children with obesity, excreted by the skin, using an array of chemical sensors and assessing its information value.
EXPERIMENTAL
Piezoelectric quartz microweighing. One of highly sensitive and simple methods for studying gas mixtures is piezoelectric quartz microweighing, which enables recording changes in the frequency of mechanical oscillations of a sensitive element, a piezocrystal, caused by minor changes in mass observed during adsorption on a tensosensitive region. This method can be used to detect a wide range of highly volatile biomolecules, for example, alcohols, ketones, organic acids, amino compounds, etc. [38].
The skin gas profile was detected using a Bio-8 portable diagnostic electronic nose (DEN) [39] (Sensorika-Novye tekhnologii (SNT), Russia) (Figs. 2a and 2b). Analytical information of the Bio-8 DEN is presented as chrono-frequency diagrams, “visual fingerprints” of the maximum signals of the piezoelectric sensors (Fig. 2c), and kinetic “visual fingerprints” (Fig. 2d). Before each new measurement, the stabilization of the baseline of each sensor was controlled; the drift should change by no more than ±1 Hz/s.

(a) Bio-8 diagnostic electronic nose; (b) scanning technique for volatile skin molecules. Integrated responses of the array of sensors (visual fingerprints) of (c) maximum and (d) kinetic sensor signals.
To ensure the reliability of the detection of volatile skin compounds for a long time of the experiment, two levels of stability control of the array of sensors of the diagnostic electronic nose were used:
(1) The array was internally standardized by standard substances (2-propanol, ethyl acetate) according to the user manual of the instrument. A certain volume of vapors was introduced into the device, and the analytical signal was recorded. The resulting shape of the integral analytical signal for each substance was compared with that presented in the manual. No more than a 15% deviation from the standard value was allowed for the array signal. The mode and periodicity of control are determined and associated with the intensity of measurements and the nature of the test samples;
(2) As the sensors in the array are microbalances, the change in the weight of modifiers on each of them determines the repeatability of measurements and is controlled by the software of the device. Before the operation, the values of the base frequencies of each sensor are introduced into the software with the allowable spread of values for each type of modifier individually (±100–500 Hz). When the allowable set spreads of the base frequency are exceeded, the sensor is subjected to additional regeneration. In case of a critical deviation of the base frequency from the passport one, the sensors are replaced with restandardization according to procedure (1).
The quantitative parameters of microweighing are calculated immediately after the measurement in the instrument software (MAGSoft):
• The maximum analytical signal of the sensor (ΔFmax, Hz), which characterizes the efficiency of the adsorption of organic compounds on adsorbent phases;
• The area under the chrono-frequency diagram of the ith sensor (Si, Hz s) to assess the contribution of the responses of each piezoelectric sensor to the total analytical integral signal of the DEN;
• The area of the visual fingerprint of signals from the DEN sensor array (ΣSv.f., Hz s), which is determined by the total weight of modifiers of volatile organic substances adsorbed by the phases during the measurement time;
• The proportion of the sensor weight in the array (ɷ1–ɷ8), %) characterizes the contribution of the signals of an individual sensor to the total analytical signal of the DEN.
The qualitative parameters of microweighing are the following:
• Adsorption efficiency parameter Ai/j, the ratio of the maximum signals of individual piezoelectric sensors ΔFi/ΔFj (where i, j are different electrode coatings), estimates the concentration ratio of different classes of compounds in the sample. It is identical for diluted vapor mixtures to the selectivity coefficient, that is, the ratio of the sensitivities of the microweighing of substances by two films [40]. The minimax values of individual vapor adsorption efficiency parameters are their qualitative characteristics.
To measure a correlation with standard clinical indicators and build a predictive model, we used a set of informational parameters of the DEN:
Quantitative parameters (25): | Qualitative design parameters (30): |
Signals of all sensors (8 pcs.): ΔFmax (1–8), Hz | Substance adsorption parameters by the sensor array Ai/j (28 pcs.) |
Contribution of individual sensor signals to the total analytical signal (share of weight), ɷ1–ɷ8, % (8 pcs.) | Kinetic parameters of sorption on the sensor with hydroxyapatite phase (2 pcs.): ɑ120/60, ɑ60/80 |
Si, ΣSv.f., Hz s | |
Total 55 parameters | |
The measuring elements are chemical sensors with basic oscillation frequencies of the DEN quartz of 10 ± 1 MHz (Piezo, Russia).
We selected the following phases as piezoelectric sensor modifiers: carboxylated carbon nanotubes (MWCNTCOOH), zirconium oxide nitrate, nanostructured biohydroxyapatite Ca5(PO4)3OH (HA), polyethylene glycol succinate (PEGSc), dicyclohexane-18-crown-6 (DCG18C6) as part of the Bio© commercial kit (SNT, Russia).
We assume that the functioning of all sensors with adsorbents obeys the Sauerbrey model; therefore, the weight of the adsorbate and coating was estimated using the main equation of the model,
where ΔF is the change in the oscillation frequency of the quartz resonator plate during phase deposition or vapor adsorption, Hz; 2.27 × 10–6 is the calibration constant of piezoelectric microbalances Kf at n.c., cm2/g; F0 is the base frequency of oscillations of the quartz plate of the piezoelectric resonator (PCR), MHz; 0.2 is the area of PCR electrodes, cm2.
Characteristics of the test samples. The study took place at the Voronezh Children’s Clinical Hospital, Burdenko State Medical University, from September 1, 2020, to June 26, 2021.
Using the Bio-8 diagnostic electronic nose and a selected array of sensors, we measured concentrations of 380 volatile compounds emitted by the skin in the forearm area in children in various conditions with various diseases during their inpatient examinations and treatment in the endocrinology department.
Each measurement lasted 200 s; the loading of the device by bringing it to the patient’s skin in the forearm area on the inner side took 80 s; after this time, spontaneous desorption of volatile biomolecules from the open cell was observed with continued recording of their responses (Fig. 2b).
For the proper assessment of the condition and labeling of the profile of volatile molecules of the patient’s skin, we used the doctor’s diagnosis and the results of medical laboratory examinations. For each patient, the volatile profile was measured on the left and right forearms on an empty stomach, after eating, and after taking medication. The metabolic profiles of 35 patients aged 5 to 17 years with various endocrine disorders, including 14 obese and 20 volunteers aged 7 to 17 years without disorders, were studied. A total of 380 measurements were carried out in a group of test subjects with abnormalities in the work of the endocrine system, while from 10 to 20 volatile body condition profiles were obtained for each patient at controlled time points at the time of inpatient treatment. For three patients, studies were performed at intervals of 1 year (2019, 2020, and 2021). For each person from the group of volunteers without health problems, the volatile profile was measured on each arm with a triple repetition in different conditions (before and after eating).
A commercial set of Bio© sensors was previously trained using individual substances that may indicate violations (Table 1), and the sensitivity and selectivity characteristics previously found for other bioassays were also taken into account [41].
The research was supported by the ethical committee of the Burdenko State Medical University, Voronezh, and parents of children during their hospitalization in written consent to Voronezh Children’s Clinical Hospital. Volunteers also signed an agreement on voluntary participation in the experiment.
Standard clinical laboratory tests. All test subjects passed through standard studies at the clinical laboratory of the Voronezh Children’s Clinical Hospital, Burdenko State Medical University. Biochemical blood parameters were measured using a BS-120 analyzer; a general urinalysis, a general blood test, and a glucose tolerance test were performed, and sex hormones and hormones produced by the thyroid gland were determined.
RESULTS AND DISCUSSION
At the first stage of the experiment, we examined the data of the diagnostic electronic nose on the volatile profile of the skin compounds of obese children for possible correlation with the results of standard clinical tests. To do this, we created a database for 14 obese children studied for 2 years during planned hospitalizations. The database included various parameters of the electronic nose, characterizing the adsorption on an array of eight sensors, and the results of laboratory studies. The gas profile of the skin of children was studied on the left and right forearms, which are associated with the cardiovascular system and organs on the left side of the body (left arm) and organs located on the right, in particular, the gallbladder, liver, intestines, and duodenum. The correlation between DEN parameters and the results of clinical studies was assessed considering these features by 52 parameters of the diagnostic nose and 23 different indicators of clinical studies. As new parameters reflecting the peculiarity of the nature of volatile molecules, we proposed kinetic parameters of the adsorption and desorption process for a specific sensor in a set, one with a hydroxyapatite phase (ɑ120/60, ɑ60/80) [42]. From a physical point of view, the parameters show how many times adsorption rate changes for a load for 60 and 80 s and spontaneous desorption after 120 s from the start of the study.
The correlation was evaluated using The Unscrambler X software (version 10.4) (Table 2). Upon detecting a volatile skin profile on the left hand, the most significant correlation was observed between the kinetic parameters of adsorption on the piezoelectric sensor modifier with a sensitive layer of HA ɑ120/60, ɑ60/80 and the level of urea in the blood obtained by the biochemical method of analysis. In detecting a volatile skin profile on the right arm of patients, the maximum correlation was found between the qualitative parameters of adsorption A1/2, A1/6, which were calculated from the maximum signals of sensors with MWCNTCOOH of different weights (sensors 1 and 7), zirconium oxide nitrate (sensor 2), PEGSc (sensor 6), and the level of alkaline phosphatase (inverse strong correlation). A correlation was also observed between the parameters A5/6, A5/7 (the responses of the sensor with HA (sensor 5) were taken into account) and the blood glucose level obtained by a biochemical blood test (direct strong correlation). This allowed a judgement of the qualitative relationship between the information of the diagnostic electronic nose and some standard clinical laboratory tests. It was impossible to quantify the level of urea, alkaline phosphatase, or glucose in the blood by the signals of the electronic nose, because the found correlation coefficient did not meet the criteria for quantitative analysis, only a qualitative dependence could be proved. Such relationships are significant for obtaining primary information about changes in these indicators in a hospital during the day, while the calculation of all indicators is carried out by one or two measurements within 5 min without blood sampling.
The second stage of the study included the data simulation and the assessment of a possibility of ranking samples (patients) into classes of diagnoses according to the information of the electronic nose with a set of Bio© sensors.
To classify the samples by diagnosis, they were divided into two groups: a training sample (197 measurements) and a test sample (77 measurements), which included data on scanning volatile compounds of the skin of patients without obesity, with diagnoses of obesity, and with types 1 and 2 diabetes mellitus (DM) of the endocrinological department.
Samples of the training set were divided into three groups: “Normal,” “Obesity with a risk of development of type 2 DM,” and “Type 1 DM.” The sample did not include data on the extreme response of a body at the time of measurement, for example, when the person was hot or when he experienced excitement or stress.
A PCA model was built for all 34 parameters of the diagnostic electronic nose (Fig. 3). The score plot suggests that the samples are divided into two groups: samples of the gas profile of patients in the first half of inpatient treatment and samples in the second half of treatment (Fig. 3). For diagnostic purposes, the first half of inpatient treatment is essential; therefore, a PCA model was built specifically for this part of the sample, and the most informative parameters of the electronic nose were determined, which can rank the samples into previously set classes.

Score plot of samples for the entire training set (132 samples) without taking into account the time of eating or the measurement point (left/right forearm).
In optimizing the PCA model for a clearer division of samples into groups according to similar features, we found that the following parameters calculated from all sensor signals in the Bio© array had the greatest influence on the ranking of samples: A1/5, A1/8, A2/5, A2/6, A2/8, A3/5, A4/5, A6/8, A7/8, ɷ3, ɷ4, ɷ5, and ɷ8.
According to the main diagnostic rule, to exclude the effect of food on the results of analysis, biosamples are usually taken on an empty stomach. Therefore, the results of scanning the gas profile of the skin obtained after eating were excluded from the sample of all data. The ranking was also taken into account separately for the left and right forearms, considering their connection with the internal organs and systems of the body (Figs. 4a and 4b).

Score plots for the parameters of the diagnostic electronic nose when scanning volatile skin compounds on (a) the left and (b) right forearm, performed on an empty stomach.
The score plots obtained in ranking the results into groups on an empty stomach show that the division into groups occurs better according to the profile of the compounds of the right forearm (Fig. 4b). The groups “Normal,” “Type 1 DM,” and “Obesity with a risk of the development of type 2 DM” are separated with high reliability.
Similar models for other states of patients (after eating and taking medications) do not allow a reliable ranking of the results into groups. Samples fall into the “Normal” group because before the measurement, patients received medications (tablets, droppers) that compensated for their condition, metabolic failures, and brought them closer to the conditional norm; the other group combined the results for patients with type 1 DM and a patient with a hormonal disorder. The selection of the scanning side (left/right) did not improve the situation. Thus, the best ranking of samples into groups occurs when studying the gas composition of a mixture of molecules secreted by the skin on the right forearm, on an empty stomach or 2–3 h after a meal.
To test the resulting model, another data sample was used. A PCA model was created for each ranking group, and a possible diagnosis in patients was predicted using the SIMCA method (Table 3). The verification of the developed model demonstrated that all patients with deviations in the metabolic processes of a body did not fall into the “Normal” group. There are no false negative results, which is essential for diagnostic methods, since such errors can lead to severe consequences and late detection of a problem, when it is already more difficult to help a person. At the same time, the problem of diagnosing deviations as early as possible (preventive diagnostics) has not been solved. The proportion of false positive ranking results is 20%. The error is associated with a small test sample and is caused by a strong influence of the inflammatory process in a body of two patients from the sample on the classification. Moreover, the “Type 1 DM” group includes profiles of patients without this diagnosis but with a complex metabolic disorder (grade 3 obesity, risk of the development of type 2 diabetes). Strictly speaking, this is not an error in terms of determining functional disorders and their severity and can be explained by the presence of the same volatile biomolecules released by the skin (nonspecific markers) in the samples.
Volatile compounds were determined, that is, state markers that can be released during various deviations in the work of a body. To do this, the data on the adsorption of vapors of test substances were projected onto the constructed PCA model of the training and test samples (Fig. 5). We determined reliably that ethanedial (glyoxal) is secreted in patient B6. Ethanedial is recorded at almost all test points and more often than in other patients, which is consistent with the diagnosis of patient B6 and the results of standard clinical studies: type 1 diabetes mellitus was diagnosed, the marker of which is, among other things, ethanedial (glyoxal).

Score plot with the ranking of bioassays into groups and possible volatile organic compounds emitted by the skin of patients.
Table 4 presents qualitative parameters for marker substances and the gas profile of people belonging to different groups: type 1 diabetes mellitus, class 3 obesity and risk of the development of type 2 diabetes mellitus, and conditional norm. Glyoxal and lactic acid, markers of carbohydrate metabolism disorders, are most often and with high probability isolated in patient B6, who has been diagnosed with type 1 diabetes mellitus; these markers release less often and less reliably in patient B7 with grade 3 obesity and with a risk of the development of type 2 diabetes mellitus. In the conditional norm group, the presence of these markers was not reliably detected.
CONCLUSIONS
We confirmed that the gas mixture of compounds emitted by the skin on the forearm of the hands can be qualitatively analyzed without preliminary separation or selection using an array of eight piezoelectric sensors of the diagnostic electronic nose (portable model). Correlations between DEN information and results of standard clinical laboratory tests were assessed. Correlating parameters of an array of sensors and clinical studies, closely related to each other, were found: ɑ120/60, ɑ60/80 and the level of urea, A1/2, A1/6 and the level of alkaline phosphatase, A5/6, A5/7 and the level of glucose. An approach based on scanning a volatile skin profile on the forearm for 3–6 min helps to rank children with obesity into groups associated with the socially significant diseases and conditions: “Normal,” “Obesity with a risk of the development of type 2 diabetes mellitus,” and “Type 1 diabetes mellitus.” Using chemometric methods, we optimized the analysis procedure and specified the research conditions and control points. An essential task in a hospital environment is noninvasive and painless, rapid monitoring of changes. For this, a volatile skin profile can be used, which is the subject of our next article.
Change history
13 February 2023
An Erratum to this paper has been published: https://doi.org/10.1134/S1061934822370055
REFERENCES
World Health Organization. www.euro.who.int/ru/health-topics. Accessed January 31, 2022.
Branca, F., Nikogosian, H., and Lobstein, T., The challenge of obesity in the WHO European Region and the strategies for response, Copenhagen: WHO Regional Office for Europe, 2007, p. 76.
Dietz, W.H., Pediatrics, 1998, vol. 101, p. 518.
Elgar, F.J., J. Adolesc. Health, 2005, vol. 37, p. 371.
Eisenberg, M.E., Ncumark-Sztainer, D., and Story, M., Arch. Pediatr. Adolesc. Med., 2003, vol. 157, p. 733.
Adolescent obesity and associated behaviors: trends and social inequalities in the WHO European Region, 2002–2014: Observations from the WHO collaborative cross-country study on health behavior in school-age children. https://apps.who.int/iris/handle/10665/ 329418. Accessed February 14, 2022.
Rakov, A.L., Nov. Apteka. Aptechnyi Assortiment, 2008, no. 6, p. 11.
Wilkinson, P.W. and Parkin, J.M., Lancet, 1974, p. 1522. https://doi.org/10.1016/s0140-6736(74)90266-9
Litvitskii, P.F., Patofiziologiya: Uchebnoe posobie (Pathophysiology: Textbook), Moscow: GEOTAR-MED, 2003.
Zaiko, N.N., Byts’, Yu.V., and Ataman, A.V., Patologicheskaya fiziologiya: Uchebnoe posobie (Pathological Physiology: Textbook), Zaiko, N.N. and Byts’, Yu.V., Eds., Moscow: MEDpress-Inform, 2002, p. 644.
Giorgio, V., Graziano, F., and Nobili, V., BMC Pediatr., 2013, vol. 13, p. 40.
Azad, K., Parkin, J.M., Court, S., Laker, M.F., and Alberti, K.G., Arch. Dis. Child., 1994, vol. 71, p. 108.
Daviss, B., Scientist, 2005, vol. 19, no. 8, p. 25.
Maksimova, E.N., Markov, V.F., Bezdetnova, A.E., Shashmurin, Yu.G., Maskaeva, L.N., and D’yakov, V.F., Butlerovskie Soobshch., 2019, vol. 60, no. 12, p. 25.
Protoshchak, V.V., Andreev, E.A., Karpushchen-ko, E.G., Sleptsov, A.V., Ovchinnikov, D.V., Alent’ev, S.A., Lazutkin, M.V., Mamaenko, A.V., and Mamaenko, T.V., Urologiya, 2019, no. 5, p. 22.
Balashova, L.M., Kolesnichenko, I.I., Kantarzhi, E.P., Korobkova, N.O., and Cherkashina, E.L., in Proliferativnyi Sindrom v biologii i meditsine (Proliferative Syndrome in Biology and Medicine), Moscow, 2016, p. 95.
Karpishchenko, S.A., Dzhagatspanyan, I.E., Lavrenova, G.V., Malai, O.P., Malysheva, M.I., Duikova, M.V., Khudyakov, E.S., Semenova, A.I., and Volchek, A.O., Folia ORL PR, 2020, vol. 26, no. 4, p. 74.
Arsen’ev, A.V., Nefedov, A.O., Ganeev, A.A., Novikov, S.N., Nefedova, A.V., Barchuk, A.A., Gagua, K.E., Tarkov, S.A., and Aristidov, N.Yu., Issled. Prakt. Med., 2019, vol. 6, p. 50.
Ageikin, A.V., Kolesova, E.V., Pronin, I.A., and Temnikov, V.A., Molodoi Uchenyi, 2015, no. 23, p. 308.
Obkhodskii, A.V., Popov, A.S., Sachkov, V.I., and Obkhodskaya, E.V., in Sbornik trudov XVII Mezhdunarodnoi nauchno-prakticheskoi konferentsii studentov, aspirantov i molodykh uchenykh (Proc. XVII Int. Scientific and Practical Conference of Students, Postgraduates, and Young Scientists), Tomsk: Nats. Issled. Tomsk. Politekh. Univ., 2020, p. 174.
Rodionov, E.O., Tuzikov, S.A., Miller, S.V., Kul’bakin, D.E., and Chernov, V.I., Sib. Onkol. Zh., 2020, vol. 19, no. 4, p. 112.
Sinitsyna, O.V., Meshkov, G.B., and Yaminskii, I.V., Med. Vys. Tekhnol., 2016, no. 2, p. 40.
Wishart, D.S., Tzur, D., and Knox, C., Nucleic Acids Res., 2007, vol. 35, p. 521.
Dhananjayan, K., Irrgang, F., and Muncha, G., Anal. Biochem., 2019, vol. 8, p. 241.
Raman, M., Ahmed, I., Gillevet, P.M., Probert, C.S., Ratcliffe, N.M., Smith, S., and Greenwood, R., Clin. Gastroenterol. Hepatol., 2013, vol. 11, p. 868.
Brown, D.G., Rao, S., Weir, T.L., O’Malia, J., Bazan, M., Brown, R.J., and Ryan, E.P., Cancer Metab., 2016, vol. 6, p. 4.
Sinha, R., Ahn, J., Sampson, J.N., Shi, J., Yu, G., Xiong, X., Hayes, R.B., and Goedert, J.J., PLoS One, 2016, vol. 25, p. 1.
Goedert, J.J., Sampson, J.N., Moore, S.C., Xiao, Q., Xiong, X., Hayes, R.B., Ahn, J., and Shi, J., Carcinogenesis, 2014, vol. 35, p. 2089.
Sugimoto, M., Wong, D.T., Hirayama, A., Soga, T., and Tomita, M., Metabolomics, 2010, vol. 6, p. 78.
Liebich, H.M. and Woll, J., J. Chromatogr., 1977, vol. 11, no. 142, p. 505.
Garner, C.E., Smith, S., de Lacy, CostelloB., White, P., Spencer, R., Probert, C.S., and Ratcliffe, N.M., FASEB J., 2007, vol. 21, p. 1675.
Ahmed, I., Greenwood, R., Costello, B., Ratcliffe, N., and Probert, C.S., Aliment. Pharmacol. Ther., 2016, vol. 43, p. 596.
Marchesi, J.R., Holmes, E., Khan, F., Kochhar, S., Scanlan, P., Shanahan, F., Wilson, I.D., and Wang, Y., J. Proteome Res., 2007, vol. 6, p. 546.
Walton, C., Fowler, D.P., Turner, C., Jia, W., Whitehead, R.N., Griffiths, L., Dawson, C., Waring, R.H., Ramsden, D.B., Cole, J.A., Cauchi, M., Bessant, C., and Hunter, J.O., Inflamm. Bowel Dis., 2013, vol. 19, p. 2069.
Bjerrum, J.T., Wang, Y., Hao, F., Coskun, M., Ludwig, C., Gunther, U., and Nielsen, O., Metabolomics, 2015, vol. 11, p. 122.
Bain, M.A., Faull, R., Milne, R.W., and Evans, A.M., Curr. Drug Metab., 2006, vol. 7, p. 811.
Azario, I., Pievani, A., Del Priore, F., Antolini, L., Santi, L., Corsi, A., and Cardinale, L., Sci. Rep., 2017, vol. 25, no. 7, p. 73.
Lvova, L.B., Chemosensors, 2019, vol. 7, no. 3, p. 39.
Kuchmenko, T.A., Dorovskaya, E.S., Menzhuli-na, D.A., and Umarkhanov, R.U., RF Patent 2764964, 2022.
Kuchmenko, T.A., Shuba, A.A., Umarkhanov, R.U., and Chernitskii, A.E., Anal. Kontrol’, 2019, vol. 23, no. 4, p. 557.
Kuchmenko, T.A., Dorovskaya, E.S., Bosikova, Y.N., Smetankina, A.V., and Bityukova, V.V., J. Anal. Chem., 2021, vol. 76, no. 7, p. 868.
Kuchmenko, T.A., Umarkhanov, R.U., and Menzhulina, D.A., Sorbtsionnye Khromatogr. Protsessy, 2021, vol. 21, no. 2, p. 216.
Funding
The work was partially supported within the framework of the UMNIK-2019 program, grant no. 15477GU/2020 of July 4, 2020.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest. The authors declare that they have no conflicts of interest.
Statement of compliance with standards of research involving humans as subjects. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants involved in the study.
Additional information
Translated by O. Zhukova
The original online version of this article was revised: Due to a retrospective Open Access order.
Rights and permissions
Open Access. This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kuchmenko, T.A., Dorovskaya, E.S., Menzhulina, D.A. et al. Estimating the Potential of the Electronic Nose System for Monitoring Disturbances in the Functional Obesity of Children in a Hospital: Noninvasive Diagnosis without Biosampling. J Anal Chem 77, 1595–1606 (2022). https://doi.org/10.1134/S1061934822120073
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1134/S1061934822120073